1. Introduction
Laparoscopic sleeve gastrectomy (LSG) has effectively been popularized due to its effectiveness in achieving high percentages of excess weight loss (EWL), combined with its favorable safety profile mainly compared to Roux-en-Y gastric bypass (RYGB). Currently, it is the most frequently performed bariatric procedure, accounting for 58% of all such procedures worldwide [
1,
2,
3]. The American Society for Metabolic and Bariatric Surgery (ASMBS) has recognized the significant impact of LSG, and utilizing long-term outcome data from large studies, has officially classified it as a primary bariatric operation for the management of morbid obesity [
4]. Indications to undergo sleeve gastrectomy remain the same as with other types of bariatric surgery and include BMI equal or greater than 35 kg/m
2, BMI of 30 to 35 kg/m
2 with the presence of serious metabolic disease as a comorbidity, especially regarding poorly controlled diabetes mellitus or metabolic syndrome [
5,
6,
7].
In addition, SG has been the operation of choice for a wide array of high-risk patients, and experts recommend it over other procedures such as RYGB. The expert consensus statement on SG states that SG is a safe and effective choice for patients awaiting transplant, the elderly, adolescents, and super obese patients [
8], as well as patients requiring revision from another type of weight loss operation, mainly adjustable gastric banding [
9,
10,
11,
12,
13]. Despite many years of experience and continuous reproducible results in successfully treating obesity-caused morbidity, as well as an evidently favorable safety profile, SG continues to display certain postoperative complications in approximately 2.2% of the patients [
14] with reports from some centers mentioning percentages of up to 5.8% [
15]. Among these, postoperative leakage is a major cause of mortality and extended hospital stays associated with LSG. It is estimated that anastomotic leakage occurs in approximately 1–3% of the patients with preoperative BMI being an effector for slightly higher rates of leakage occurrence [
16]. Currently, there is an identifiable gap in the surgical literature, regarding several aspects of post-LSG leaks, evidenced by a lack of definitive guidelines for their management strategies. Outstanding issues that need to be further explored, include correlations with the timing of postoperative leaks, identification of patient risk factors associated with the development of leaks, and appropriate ranking of management options within the tertiary hospital environment.
Our retrospective, single-center study aims to evaluate the prevalence of postoperative staple line leakage after LSG and identify risk factors for its development, with a focus on acute (before the 7th postoperative day) leaks. As secondary aims of this study, we also describe patient symptomatology, the correlation of patient characteristics with a postoperative day of leakage diagnosis, and the management options of anastomotic leaks, through our practice.
3. Results
During the study period, data from a total of 402 patients were enrolled. Within this patient cohort, 26 patients (6.46%) developed a postoperative staple line leak. The entirety of the reported leaks were reported in the cardio-esophageal junction area. The demographic characteristics of leak vs. non-leak patients can be seen in
Table 1. There were no statistically significant differences in patient age, mean weight at time of operation, and mean BMI (
Table 1). Average hospital stay differed significantly between the two groups, with patients complicated by postoperative leaks, being hospitalized for a total of 44.2 (SD 27.24) days on average, as opposed to 7.78 (SD 7) days for the uncomplicated patients.
Regarding presenting symptoms of patients with postoperative leaks, developing a high or low-grade fever was the hallmark of diagnosing a postoperative leak, found in 96.2% of the patients. Other symptoms included acute abdominal pain in 38.5% of the patients, positive Kehr sign in 38.5%, respiratory distress in 19.2% of the patients, and vomiting in 15.4% of the patients (
Table 2). Hemodynamic instability requiring aggressive resuscitation on presentation was found in only one (4.2%) patient of our cohort. The most common symptom constellation was that of fever with acute abdominal pain and positive Kehr sign, found in 11 (42.3%) patients. Two patients developed subclinical leaks with no reported symptoms. One was diagnosed after routine radiographical upper GI series with no change in drain biochemistry (Type B leak) and the other had solely increased amylase drain levels with no radiographic evidence of a leak (Type A leak).
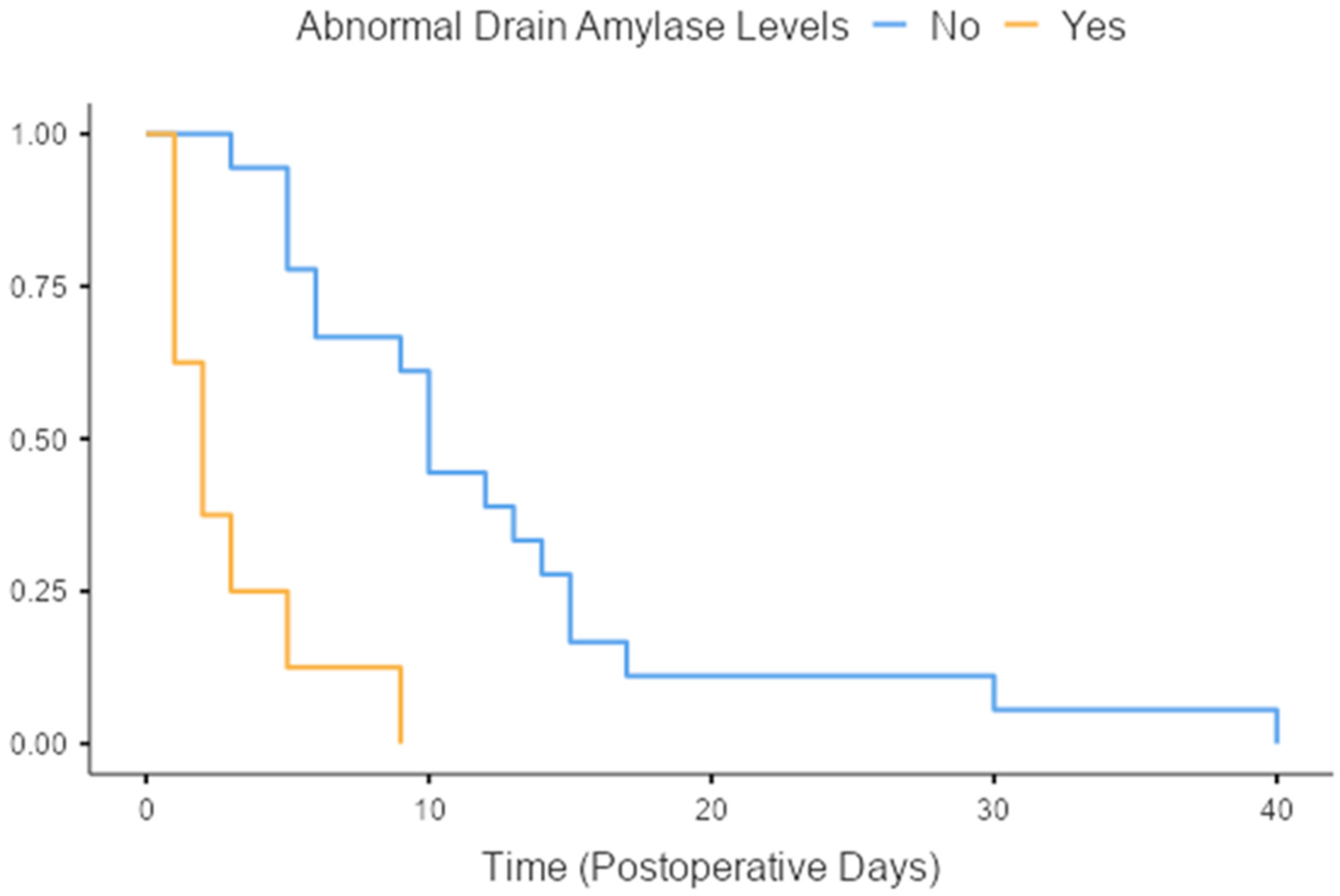
Drain amylase levels area relatively controversial indicator of postoperative leakage in sleeve gastrectomy patients. The definition of abnormal amylase drain levels in our study was amylase levels higher than three times the value of patient serum amylase. In our cohort, abnormal amylase levels were detected in eight out of the twenty-six patients (30.6%) that were diagnosed with a staple line leak. Time-to-event analysis revealed that patients with abnormal amylase drain levels were diagnosed with staple line leak earlier when compared to those that had normal amylase drain levels (3 days vs. 12.5 days on average,
p < 0.001,
Figure 1).
Treatment options within our unit included conservative management with percutaneous drainage, endoscopic placement of intraluminal stents, and endoscopic clipping of the defect. In total, nineteen(73.3%) patients underwent percutaneous drainage, fourteen patients (53.8%) were treated with intraluminal endoscopic stenting, with two of them requiring a second attempt, and one requiring three attempts. Finally, five patients (19.2%) were treated with endoscopic clipping of the defect. Operative management was required in only one patient, who underwent conversion to a Roux-en-Y gastric bypass. Nutritional support was needed in 21 patients (80.8%), 11 of which received enteral feeding via NJ tube (42.3%), and 10 (38.5%) received TPN.
Readmissions due to persisting gastric leak (fistula) were deemed necessary for 15 (57.7%) patients. The number of readmissions varied from one (seven patients—26.9%) up to ten readmissions for two of our patients.
Early leaks were present in eleven patients (42.3%), intermediate leaks in four patients (15.38%), and late leaks in eleven patients (42.3%), between which subgroup analyses were conducted. Hospital stay did not differ significantly between the three subgroups in the univariate and multivariate analyses.
Choice of modality for the successful management of postoperative leaks differed significantly between the three chronological subgroups. Early leaks were successfully managed with most available modalities, drainage followed by clipping (36.36%), drainage followed by endoscopic stenting (45.45%), and conservative management (18.18%). Intermediate leaks were managed by drainage alone (50%), drainage followed by endoscopic stenting (25%), and conservatively in 25%. Late leaks were managed with drainage alone (36.36%) and drainage followed by stenting (63%) (
p = 0.038) (
Table 3).
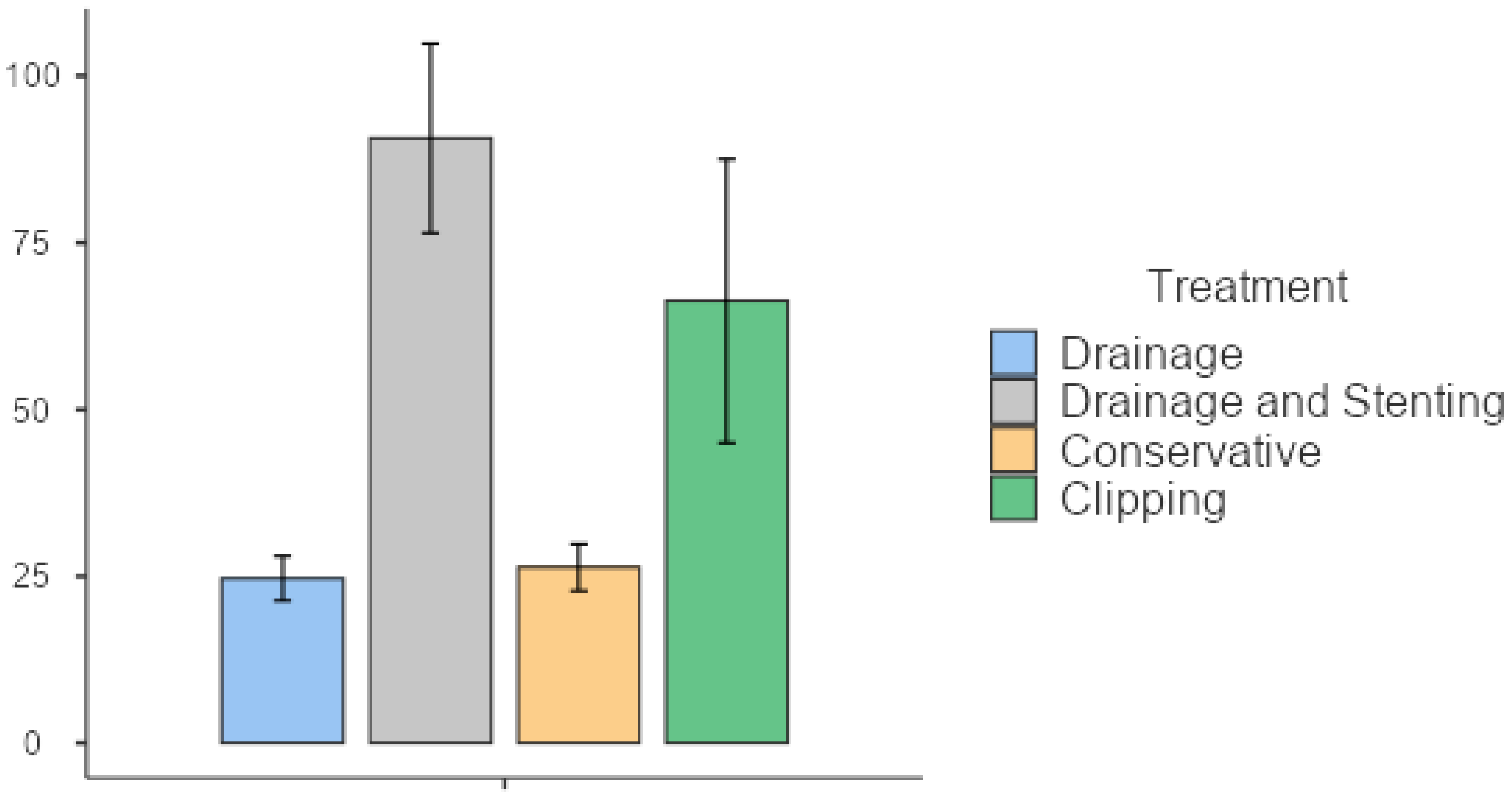
Hospital stays differed significantly among treatment groups, with patients undergoing endoscopic clipping staying for 63.7 (SD 35.2) days, those treated with drainage and stenting being hospitalized for an average of 57.7 (SD 19.39) days, conservatively treated patients staying for 26.3 (SD 6.11) days, and those treated by drainage alone staying for 21.5 (SD 7.82) days (
Table 4) (
p = 0.008). The overall time-to-resolution was correspondingly different for the treatment groups, with drainage and stenting patients being admitted for a total of 90.6 (SD 51.2) days, endoscopic clipping patients for 66.3 (SD 42.5) days, and image-guided drainage patients for 24.7 (SD 8.24) days (
p = 0.012) (
Figure 2 and
Figure 3,
Table 4). Patients requiring stenting or clipping in addition to percutaneous drainage had longer hospital stays. Patients managed conservatively were not readmitted and therefore did not have a longer time-to-resolution than that of their initial hospitalization. Readmission rates also differed significantly between the three subgroups. Patients with late leaks were readmitted in 90.9% of the cases, those with intermediate leaks in 50% of the cases, followed by patients with early leaks in 27.3% of the cases (
p = 0.001) (
Table 3).
Hospital stay was also found to differ significantly when type of nutritional support was evaluated. Patients requiring no enteral or parenteral nutritional support (TPN) had an average hospitalization length of 25 days (SD 8.2), with those being supported by enteral nutrition via NJ tube having a length of stay of 44.2 (SD 22.5) days, and finally TPN-requiring patients being hospitalized for an average of 60.1 (SD 28.14) days (p = 0.004).
Multivariable analysis on the correlation between time-to-resolution of gastric leak, and studied parameters, revealed that neither the treatment choice, nor the need for nutritional support or the timing of gastric leak occurrence were independent predictors of hospitalization length until full resolution of the gastric leak (
Table 5).
The occurrence of gastric leaks was found to be independently associated with several of the studied risk factors for leaks. Among studied patient parameters that influence the occurrence or not of gastric leaks, smoking was revealed to be an independent risk factor, with an OR of 1.43 (95 CI 1.27–1.58) (
Table 6). Preoperative diagnosis of diabetes was also identified as a prognostic factor for leak occurrence with an OR of 1.13 (95 CI 1.04–1.42) as well as the presence of sleep apnea with an OR of 1.24 (95 CI 1.09–1.58). Crude preoperative BMI and BMI of more than 50 were not found to be positively related to the occurrence of postoperative leaks in our patient group (
Table 6).
4. Discussion
Leakage is the most frequent postoperative complication of SG with occurrence rates of 2.1% on average, reaching up to 5.5% in some studies [
21]. Despite the fact that SG does not involve any kind of anastomosis, it seems more susceptible to postoperative leaks than RYGB. In addition to its high prevalence rate, postoperative leakage has been found to be the second leading cause of mortality after bariatric surgery, with reported mortality rates of 1.4% [
22]. No mortality that was definitively attributable to a staple line leak was recorded at our institution. Our incidence of postoperative staple line leaks is on the upper limits of that reported in the literature. One possible explanation for this difference is the fact that many of the cases included in our study are from the 2000s, when our and international experience was limited and the surgical technique was not sufficiently standardized. Another possible explanation for this difference is our election of a smaller diameter bougie tube for the creation of the gastric tube. A smaller bougie tube results in a narrower gastric pouch, which naturally produces higher intraluminal pressures that might contribute to a small increase in postoperative leaks. A few studies have looked into the correlation of bougie sizes and postoperative staple line leaks, failing to produce definitive results, yet indicating a trend towards a trade-off of increased leak incidence with better weight loss outcomes [
23,
24,
25]. Single-institution studies are consistently producing contradictory results either in favor of or indifferent towards increased leak rates with narrower bougie sizes [
25,
26]. There are two meta-analyses available on the subject, with equally contradictory conclusions regarding bougie sizes and the risk of postoperative staple line leaks [
27]. The analysis by Parikh et al. [
27] treated bougie size as a binomial variable (greater or smaller than 40 Fr) as opposed to a continuous spectrum including all sizes which always seems to lead to no correlation between bougie size and leak. This meta-analysis managed to showcase a significant difference in postoperative leak rates for patients with bougie tubes under 40 Fr, as is also the case for our patients. Bougie size in sleeve gastrectomy is also implicated in the occurrence of chronic dehydration of the bariatric patients, with narrower gastric pouches being associated with fewer admissions for dehydration in post-SG patients [
28]. At our institution, we continue to use a 32 Fr bougie. Based on our previously published results [
29], we believe that a 32 Fr boogie is a key factor for successful long-term weight loss in the majority of patients. Postoperative leakage after SG is commonly classified based on time of occurrence post-surgery. According to the ASMBS, acute leaks are considered those within 7 days of surgery, early leaks are between 1 and 6 weeks postoperatively, late leaks after 6 weeks, and chronic leaks are considered those after 12 weeks [
30]. Our study focused on acute and early leaks, with a few reports on late and chronic leaks that are largely thought to be governed by different pathophysiological principles. Authors have also classified leaks according to their clinical presentation, with Type I leaks being the subclinical, localized leaks without dissemination in the abdominal cavity, and Type II leaks being those with severe clinical manifestations caused by their dissemination in the peritoneal cavity [
31].
The mechanics of staple line leakage, include a long stapling line being present, as well as the conversion of the stomach itself into a narrow, high-pressure tube due to the presence of both esophageal and pyloric sphincters. In our case, election of a smaller diameter bougie that results in a narrow gastric tube, also predisposes to higher intraluminal pressures that might contribute to a small increase in staple line leak rates. It must be noted however, that further morbidity rates and mortality were not increased in our cohort, compared to previous studies. Therefore, the true impact of a narrower, high-pressure tube seems to be limited in minor leaks with little to no physiological derailment of the patient. Although not leading to patient mortality, morbidity rates attributed to postoperative leaks are a significant burden for the patient and healthcare systems alike, often requiring multiple hospital admissions, as well as endoscopic and image-guided interventions. Stapler misfiring, shearing forces during surgery, and tissue creeping are also factors that contribute to early leakage, and can be combated by allowing adequate compression time before each stapler firing [
31], as is our practice. As mentioned earlier, studies on staple line reinforcement do not seem to reach clear conclusions on their utility, and there while some report a trend in bleeding reduction, no clear effect on leakage rates can be inferred [
32,
33,
34]. A meta-analysis on the subject failed to demonstrate any significant reduction in leakage rates with any of the methods studied, although postoperative bleeding and reoperation rates were significantly lower when reinforcement was applied
21, and therefore we did not perform staple line reinforcement routinely which was abandoned post 2010, whereas negative pressure drains were placed routinely. One such study concluded that the only clear effectors on leakage rates were surgical technique, experience of the surgeon, and complexity of the patient’s anatomy [
35]. In addition, our multivariate analysis determined no additional significant independent predictors for the occurrence of postoperative staple line leaks in SG patients, with the exception of smoking as a risk factor.
Experienced surgeons also seem to agree that another cause of postoperative leaks is the creation of an ischemic environment on the staple line, particularly close to and around the angle of His. Maintaining a distance of 1–2 cm from the gastro-esophageal junction, has been recommended in order to reduce tissue ischemia in this area [
17,
31]. Bougie size was also identified in a number of studies to be a predictor of leak occurrence [
27], although as already discussed, the overall results are not definitively conclusive, largely due to the lack of homogeneity in establishing a bougie size cutoff, between the studies. In this aspect, using bougies of sizes of 40 Fr or greater seem to be associated with fewer instances of leakage [
13,
16,
27], most likely due to the resulting wider tube that lowers the intraluminal pressure. As already mentioned, our utilization of a narrower gastric tube could be the cause behind an increased incidence rate of staple line leaks within our cohort. Patient risk factors that are found in the literature to significantly contribute to leakage rates, include male sex, BMI of more than 50 kg/m
2, use of SG as a revision procedure, and presence of sleep apnea [
36,
37,
38]. Interestingly, within our cohort, BMI, crude weight, gender, and ideal preoperative weight were not associated with the occurrence of staple line leaks. On the contrary, preoperative diagnosis of diabetes and sleep apnea were confirmed as independent factors contributing to leak occurrence in the multivariate analysis, which confirms previous findings from large patient cohorts [
39]. This is possibly attributed to microvascular damage in diabetic patients leading to micro ischemic damage along the staple line, causing leakages to occur. Obstructive sleep apnea is also associated with increased odds for postoperative staple line leaks with two physiological mechanisms; anemia and poor tissue oxygenation are both implicated in postoperative leaks [
40,
41]. Revision procedures were not included in our patient cohort.
Gastric leakage can be the cause of significant mortality and morbidity of patients, leading to sepsis, hemodynamic instability, and MODS. Clinical presentation of this complication can vary from asymptomatic (Type I), to mild pain, to full-blown presentation of peritonitis with septic shock (Type II). Tachycardia, sudden postoperative abdominal pain, and fever should alert the clinician to the possibility of a developing leak [
42,
43,
44]. Postoperative pain and fever were the most common symptom combination within our cohort, and fever developed in 96% of the patients, indicating a series of clinically significant leaks. There were no asymptomatic postoperative leaks within our cohort of patients, which raises the question of the utility of classification according to presentation.
High-quality data from RCTs have shown no statistically significant difference in anastomotic dehiscence in patients with and without intra-abdominal drains, as the current trend recommends the use of intra-abdominal drains only in complicated or revisional cases. Our study showed that the use of drains can provide early identification of PSLLs after SG, and at our institution, we continue to use them routinely. In uncomplicated cases, the intra-abdominal drain is removed on the 4th postoperative day, and only if there are alarming clinical and laboratory findings for PSLL, it remains for a longer period. We believe that early detection of a PSLL is important and may modify clinical decision-making, although we cannot be certain whether such knowledge affects patient prognosis and outcome.
Treating the postoperative leaks after SG remains a field lacking a standard algorithm, despite many surgical teams having developed several individual ones. While timely diagnosis and treatment is considered ideal and contributes to postoperative outcomes, still most patients are diagnosed with gastric leaks after they have been discharged from the hospital [
22,
31]. These patients contribute to late and chronic leak rates, and are the cause behind more advanced diagnosis in postoperative days. Patients presenting acutely, with fulminant sepsis and hemodynamic instability should be taken to the operating room immediately for emergency surgical intervention, rather than using any of the conservative or endoscopic methods of treatment. Managing source control of the sepsis via peritoneal lavage and drainage, is of the utmost importance in such cases, and should not be delayed in order to attempt conservative management [
30,
42,
44]. Patients that ultimately undergo emergency surgery as a measure of leakage treatment, ultimately exhibit larger mortality rates; however, it must be noted that these are the most critically ill patients, and none of the studies measuring mortality rates have done so while adjusting for well-known mortality factors, such as organ dysfunction, presence of shock, etc. [
44]. Fortunately, such cases are scarce, and in our cohort that represents a single-center experience over multiple years, there was only one such case. When considering patients without such a catastrophic presentation, a variety of management options have been described in the literature. Authors advocate attempting nonoperative management in stable patients whether the leak is early or late. Administration of broad-spectrum antibiotics for coverage of intra-abdominal infections, as well as nutrition and hydration support, are key in the conservative management of such patients [
45,
46,
47,
48]. Within the minimally invasive spectrum of treatments, percutaneous drainage of any recognized and accessible fluid collection should also be performed. In our study, percutaneous drainage with or without intraluminal stenting was the most commonly followed management strategy and resulted in significantly faster leak resolution rates and shorter hospitalization length.
Utilization of endoscopic methods in the treatment of SG leaks is also widely described in the literature. Endoluminal stenting in select patients can allow for nonoperative management of leaks, without the need for surgery, while at the same time the patients maintain nutritional support of themselves with oral feeding. Patients treated with endoluminal stents achieve high success rates of up to 100% in several studies [
49,
50,
51,
52,
53], including our own. Endoscopic stenting was used in 53.8% of our patients with a perfect success rate. It must be noted however, that endoscopic stenting required additional attempts in a few of our patients, and thus, resulted in an increased average hospitalization length. Additionally, endoscopic stenting required a longer period until the confirmation of biochemical and clinical resolution of the staple line leak. Instead of primary closure (that is not recommended), covered stents manage to endoluminally seal the leaks, acting as a physical barrier that promotes healing. Shortcomings of this approach include migration of covered stents that is reported in 17–58% of the patients, requiring repetition of the endoscopy procedure [
54,
55]. Partially covered stents have been used to achieve better anchoring; however, in 9% of the patients, removal is unsuccessful and can require further manipulation [
54,
55,
56,
57,
58]. Endoscopic clip placement can also be used to approximate the defect causing the leak and was utilized in five of our patients with no reported adverse events. This is a more technically demanding approach and requires experienced endoscopists in order to achieve good visualization and complete closure of the defect. Despite lacking large-scale trials, the literature suggests high success rates with minimal to no adverse effects [
50,
59,
60]. In the event of failure of effective management with any of the aforementioned methods, surgical management should be the next logical step, since the time interval will likely be such, that the leak will now be considered chronic [
61]. Revision options include fistulojejunostomy, RYGB conversion, and total or near total gastrectomy, or the described rendezvous procedure, a technically challenging undertaking that has yet to prove palpable advantages [
62,
63,
64,
65].
In light of a postoperative complication that can cause a great morbidity and mortality burden, to bariatric patients, novel and innovative approaches to address the postoperative leak are continuously emerging. Perhaps one of the most commonly discussed is the use of biological glue (commonly fibrin or cyanoacrylate). Fibrin glue has been studied in the closure of small leaking defects in various bariatric operations including sleeve gastrectomy. Reported success rates range from 92.8% up to 100%; however, these are reported usually in small cohorts, and after multiple application sessions. Fibrin glue increases the cellular response to damage and promotes fibroblast proliferation. Ease of application and lack of debilitating complications are the main advantages of the technique [
63,
64,
65]. A group of researchers successfully utilized mesenchymal stem cells derived from each patient to endoscopically assist in sealing identified orifices after SG by submucosal injection with no reported complications. Open-pore suction devices can be placed endoscopically at the endoluminal fistula opening [
66]. Addition of laparoscopic assistance forms the rendezvous procedure, during which the laparoscopic surgeon assists in accurate identification of the defect and placement of the suction device which is guided at the same time by the endoscopist [
67]. This procedure is thought to be reserved for treatment-resistant leaks, or large leaks requiring laparoscopic washout in addition to attempts for sealing. Advanced surgical options after conservative, endoscopic, or minimally invasive approaches have failed are also being performed in experienced bariatric centers. One such approach is the complex laparoscopic Roux-en-Y fistulojejunostomy formation usually performed for complex, chronic fistulas after a SG leak [
67].
Study Limitations
Our study is not immune to certain shortcomings, as with any original report. First of all, there is an inherent difficulty in the generalization and external validity of our findings, since our study is a retrospective, single-institution cohort study. As such, our patient population was somewhat limited in a specific geographical area, and intraoperative techniques limited to those of our institution. Second, our study did not include certain proposed management strategies of staple line leaks (e.g., biological glue), due to lack of availability. Third, the retrospective nature is also a setback, since without randomization, our results while significant, are of lower quality than an RCT looking into the comparison of different management strategies for staple line leaks. Fourth, our study includes patients who underwent SG during a long time period of 17 years. This implies a lower level of experience during the first years that we performed the surgery. In addition, the indications and decisions for the various therapeutic interventions for PSLLs changed slightly or more over time. Fifth, the subgroup statistical analysis included subgroups with a small number of patients, which may not be representative. Finally, given the retrospective nature of this study design, there were several parameters that could not be evaluated and were related to the patients (e.g., clinical and laboratory findings at the time of PSLL), to PSLL (e.g., location, size, presence of abscess or fistula), and to the therapeutic methods applied (e.g., availability, indications).



 ,
, 


{kind=link}
{kind=link}
{kind=link}