1. Introduction
Exposure to potentially traumatic events (PTE) has been associated with the development of several psychopathologies with the number and intensity of these events being risk factors [
1]. Firefighters are considered a high-risk group for developing stress-related psychopathologies, such as post-traumatic stress disorder (PTSD), due to repeated exposure to traumatic events [
1,
2]. PTSD is a condition that may follow exposure to a traumatic event and is characterized by intrusive symptoms, avoidance behaviors, negative alterations in mood and cognitions, as well as in arousal and reactivity associated with the traumatic event. In order to differentiate normal from pathological reactions after exposure to traumatic events, one of the diagnostic criteria concerns the duration of symptoms, which must exceed one month. In addition, the symptoms significantly impair the person’s ability to function socially or occupationally [
2].
“Although not distinguished in the DSM-5, PTSD can be further differentiated into Primary and Secondary PTSD. The differentiation between Primary and Secondary PTSD is determined depending on the type of exposure to the trauma. Direct exposure as a victim to the traumatic event results in Primary PTSD; while indirect exposure, as an observer of a trauma or close family member/friend of a trauma victim, results in Secondary PTSD. The concept of Secondary PTSD is based on the concept of secondary stress, that is, the stress resulting from indirectly experiencing a traumatizing event experienced by a significant other or the stress resulting from helping or wanting to help a person who has been traumatized”
Studies have shown that the exposure to traumatic events is also associated with the development of Somatic Symptom Disorder (SSD) [
3], being the diagnosis of PTSD associated with a considerable increase in somatic symptoms among firefighters [
4]. SSD is characterized by persistent physical symptoms that lead individuals to recurrently seek health care services, being seen by several medical specialties that do not find an organic pathology that explains such symptoms.
It is known that the female gender is associated with higher rates of somatic symptoms [
5]. A study conducted in Portugal [
5] showed that gender had the greatest influence on the severity of somatic symptoms, explaining 11.6% of the variation in the symptom severity. On the other hand, in a study on the amplification of common somatic symptoms by PTSD in firefighters [
4], gender and age were not significant in the variation of somatic symptom levels. The results indicated that the presence of PTSD was associated with more somatic symptom complaints, with the presence of such symptoms accounting for 9.8% of the variance in somatic symptom severity.
“The somatization of emotions accounts for a large proportion of family practice visits. Twenty percent of new presentations in primary care and 20–40% of medical outpatient referrals present with high rates of somatization into bodily systems including the respiratory, cardiovascular, gastrointestinal, musculoskeletal, neurological and dermatological systems”
The World Health Organization carried out a study in 14 countries (N = 1146) and found that somatic symptoms were the main reasons for consultation in 69% of patients with major depression, demonstrating that the clinical presentation of a somatic idiom can hide, or marginalize, concomitant changes in emotional state [
7]. The high costs for health care services, in addition to the evident frustration of doctors and patients, have stimulated psychiatric research, mainly due to the difficulty of diagnosing individuals with this condition. The underestimation of the severity of mental health problems and the resistance to reporting emotional issues are among the main factors that hinder the diagnostic process, delaying the referral of these patients to appropriate treatments [
5].
SSD is considered a consequence of the avoidance of strong emotions, especially trauma-related emotions [
6]. While avoidance is a symptom of PTSD, it is also a maladaptive coping strategy that may contribute for the development of this condition, as well as other psychopathologies [
1]. Since mental health stigma is a common problem within Fire Departments, where seeking mental health help may be seen as a sign of weakness, firefighters become susceptible to the emergence of psychological and physical health problems [
1,
8]. As stated by Milligan–Saville et al. [
4] (p. 4), “PTSD and its associated physical health problems cause substantial impairments in daily functioning, though only a small proportion of individuals with PTSD obtain psychiatric treatment”.
Although there are many studies on the prevalence of PTSD among firefighters, the results are divergent. A previous systematic review [
1] (p. 76) found that “while some studies reported PTSD rates of 26.6% [
9] and 31.8% [
10], others indicated 13% [
11], or even 2.7% [
12]”. This systematic review focused on studies on the risk and protective factors for the development of stress-related diseases in firefighters and proposed a relational model, showing how a set of factors may influence the perception of stress and then the development of these conditions in this population. The first factor proposed by this model is exposure to a PTE, a precondition for the development of stress-related symptoms. According to this study, professional factors highly influence the subjective appraisal of the PTE, as indicated by the different reactions of professional and volunteer firefighters. Studies showed that volunteer firefighters have a higher risk for developing depression, anxiety and PTSD symptoms compared to professional firefighters, as they generally receive less formal training and have less work experience [
1].
Although there is a great interest in the factors that contribute to the development of PTSD in firefighters, there are few studies exploring the relationship between exposure to PTE and other psychopathological symptoms, such as SSD, anxiety and depressive symptoms, with this population. Considering that, the present study started from the analysis of the correlations between psychopathological symptoms and the risk factors identified in previous studies [
1,
5], namely gender, age, educational level, experience (years of service as a firefighter) and firefighter status (volunteer or professional). Then, it aimed to assess the relationships between PTE and PTSD, and the relationship between PTE and SSD. Since there is evidence that the diagnosis of PTSD is associated with an increase in somatic symptoms [
4], and that SSD is associated with the exposure to PTE [
3], we were interested in the potential effect SSD could have on PTSD symptoms. Thus, this study aimed to assess the mediating role of SSD in the relationship between PTE and PTSD within Portuguese firefighters. We have also included a mediation analysis with a variable extracted in the principal component analysis, psychopathologies, in order to assess its mediating role in the relationship between PTE and PTSD. It is known that there is a higher prevalence of depression and anxiety among firefighters, as well as that these psychopathologies are considered common PTSD comorbidities [
1].
Considering studies in this field, we hypothesized that PTSD, SSD and psychopathologies would be highly correlated. Regarding the sociodemographic characteristics, we hypothesized that less experience and being a volunteer firefighter would be associated with PTSD, as well as being female associated with SSD. Finally, we also hypothesized that SSD would mediate the relationship between PTE and PTSD, since the co-occurrence of psychopathologies is common after traumatic exposure.
3. Results
The sample consists predominantly of men (75%) with a mean age of 34.75 years old and 12.34 years of schooling. The main PTE reported by the sample were work accident requiring medical care (n = 55; 47.4%), death of family member (n = 50; 43.1%), death of a friend (n = 43; 37.1%), and accident or illness of a friend or family member (n = 40; 34.5%). According to the assessment instruments, 12.7% of the sample scored for PTSD (PCL-5: M = 9; SD = 12.68), and 3.9% scored for SSD (PHQ-15: M = 3; SD = 3.87).
The Pearson correlation test (
Table S3) shows that experience (years of service as a firefighter) and firefighter status (volunteer or professional) were not related to PTSD, SSD and the variable psychopathologies (
p > 0.05). Female gender was associated with somatic symptoms (
r = −0.344,
p < 0.001) and psychopathologies (
r = −0.290,
p < 0.001).
We ran Pearson correlations to examine the strength of association between PTSD, SSD and psychopathologies. Results show that PTSD were correlated with SDD (r = 0.606, p < 0.001) and psychopathologies (r = 0.76, p < 0.001). Psychopathologies and SDD were also correlated (r = 0.63, p < 0.001). All had large effect sizes.
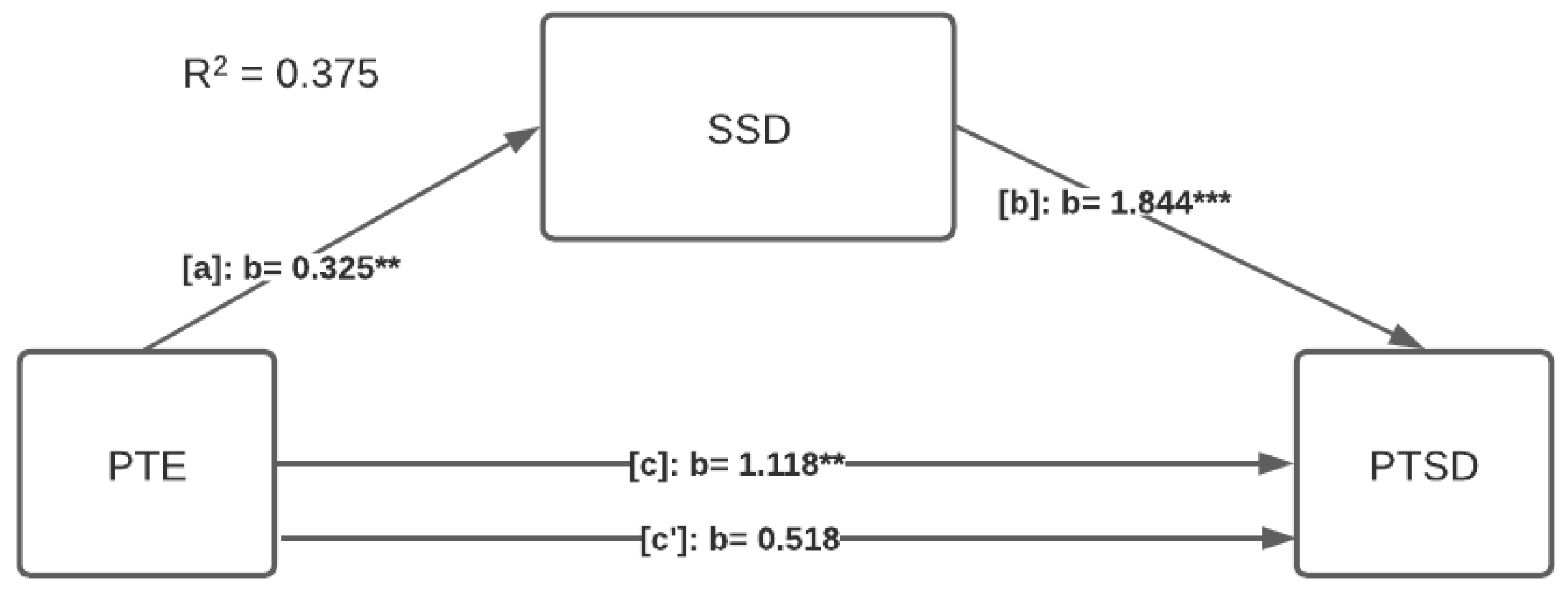
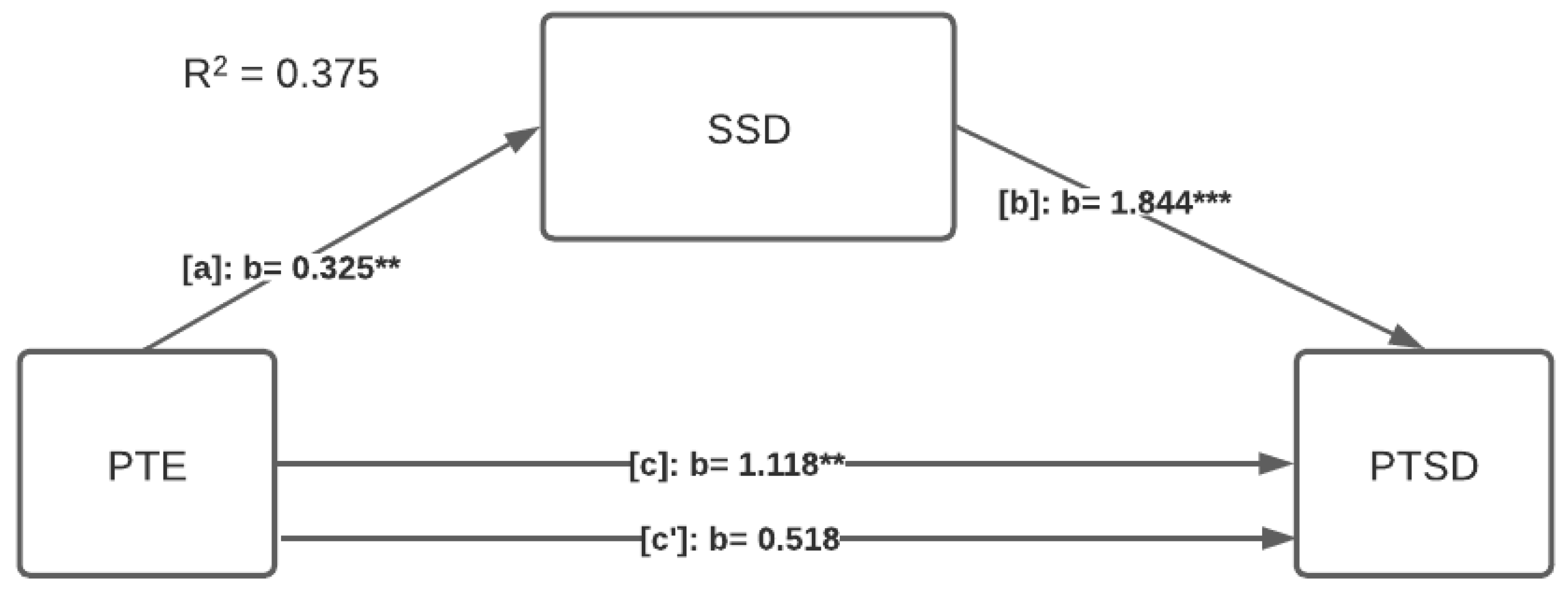
We tested the mediating role of SSD in the relationship between PTE and PTSD. Results show that SSD mediates the PTE—PTSD relationship. The model explains 37.5% of the variance (F (2, 113) = 33.94
p < 0.001), and the indirect effect of this relation is significant (indirect effect: 0.60, SE = 0.22, 95% CI [0.18–1.06]), meaning that SSD fully mediates in the relationship between PTE and PTSD since the direct effect is no longer significant (direct effect: 0.52, SE = 0.30, 95% CI [−0.08–1.12]).
Figure 1 shows the coefficient results in the mediation model.
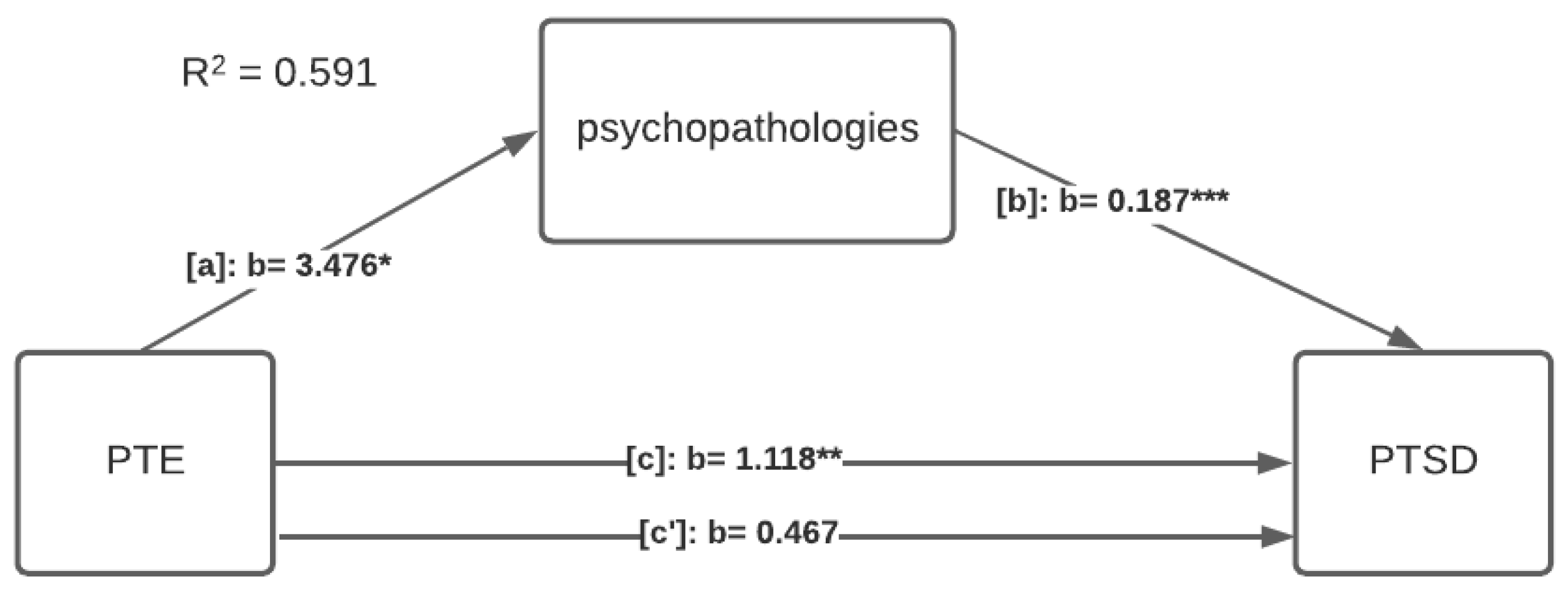
We then tested the mediating role of psychopathologies in the relationship between PTE and PTSD. Results show that the psychopathologies mediate the PTE—PTSD relationship. The model explains 59.1% of the variance (F (2, 113) = 81.77
p < 0.001), and the indirect effect of this relation is significant (indirect effect: 0.65, SE = 0.24, 95% CI [0.20–1.13]), meaning that psychopathologies fully mediate the relationship between PTE and PTSD since the direct effect is no longer significant (direct effect: 0.47, SE = 0.24, 95% CI
Figure 2 shows the coefficient results in the mediation model.
4. Discussion
It is not surprising that the consequences of traumatic stress continue to be the focus of several studies in the medical, psychological and social sciences, since society is continually affected by traumatic events. Wars, accidents, pandemics and natural disasters immobilize communities, countries and continents that seek explanations, means of intervention, minimizing damages and preventing recurrences. Disasters are constituted of multiple stress-inducing factors (e.g., fear, pain, losses and physical sequelae) and arouse the interest of professionals and researchers dedicated to the study of traumatic stress, as well as of the factors that influence the development of psychopathologies following exposure to PTE.
Exposure to traumatic events is associated with the development of both psychopathologies addressed in this study, PTSD and SSD [
4,
6,
23], which is why firefighters are seen as a high-risk group for the development of these conditions. Firefighting is a stressful occupation that exposes individuals to occupational stressors, poor sleep, and extreme and tragic events. They face situations that require quick reactions and precise communication, in addition to performing strenuous physical tasks (e.g., running, carrying heavy loads and dragging victims to safety) in challenging and unpredictable conditions [
10,
23,
24,
25,
26,
27].
In Portugal, forest fires are a major government concern due to environmental issues and the impact on the health of the affected population. However, “as in many other potentially traumatic events, the attention of media, government, and health professionals is often to primary victims” [
27] (p. 1). The so-called secondary victim is one who witnesses or becomes aware of a traumatic event experienced by another person, either attempting to help others, or even listening to reports of suffering [
12,
27]. As previously highlighted, the concept of secondary PTSD is based on the concept of secondary stress, the stress resulting from the indirect experience of traumatic situations, as is the case of professionals who work in crises and catastrophe scenarios [
2]. “It is evident that firefighters are used to dealing with physical discomfort, unpredictability, the pressure and expectation of society and their departments, the fear of the victims and their own fears. However, being prepared to face extreme situations is not synonymous with being immune to traumatic stress” [
1] (p. 80).
Studies have found different prevalence rates of PTSD among firefighters, although most of them have indicated that firefighters have higher rates compared to the general population [
9,
10,
11,
23,
26]. A previous study conducted in Portugal [
28] found that firefighters are exposed to an average of 25.5 PTE throughout their career. The sample of this study consisted mostly of men (77.8%), with a mean age of 31.85 years old, and 10.5 years of schooling, showing similarity with the sample of the present study. Furthermore, symptoms of psychopathologies were significantly correlated with PTSD symptoms.
Professionals who work in crisis situations may experience a set of stress reactions such as fatigue, depression, anxiety, alcohol abuse, as well as PTSD and SSD [
3]. In addition to the lack of recognition of their suffering, the stigma related to mental illness is prevalent in Fire Departments and influences the way firefighters deal with their stress reactions and, subsequently, the development of psychopathologies [
1,
3].
Previous studies [
3,
9,
23] have indicated that the development of stress-related psychopathologies is influenced by a set of factors such as personality traits, working conditions, social support, and mental and physical health problems. All these factors interfere in the perception of stress, thereby affecting the choice of coping strategies, which can lead to either psychopathologies or normal stress reactions and a recovery process [
1]. PTSD and SSD are associated with denial and avoidance behaviors, seen as common coping strategies applied by the fear of stigma and the will to meet social and organizational expectations [
3,
4]. Stigma related to mental disorders seems to be the main reason for the low rates of PTSD among firefighters, as well as for the low adherence of these professionals to mental health treatments [
27].
Considering the professional factors indicated in a relational model for stress in firefighters [
1], identified in a systematic review on the risk and protective factors for the development of stress-related diseases in these professionals, we have tested whether the years of service as a firefighter and the firefighter status (volunteer or professional) have influenced the development of psychopathologies in our sample, and these factors were not significant. Experience and training are often mentioned as influencing the development of PTSD in firefighters [
1], and not exactly the fact of being a professional firefighter or a volunteer firefighter. According to studies on the differences between professional and volunteer firefighters [
24,
25], the lack of appropriate training and uncertainties regarding the tasks and the situations that firefighters face, combined with the lack of social and organizational support, lead to stress reactions. Therefore, we can assume that firefighter status was not a relevant factor since Portuguese volunteer firefighters are used to facing violent forest fires, and many of them maintain a strong connection with their Fire Departments, taking work shifts and participating in training throughout the year.
If, on the one hand, the hypothesis about the influence of the experience and the firefighter status on PTSD severity was not proven by the current study, then on the other hand, our findings corroborate that the female gender is associated with a higher prevalence of somatic symptoms. “According to the literature, women generally report more bodily distress and more frequent somatic symptoms than men” [
5] (p. 5).
In addition to the social and occupational impairments to patients’ lives, SSD represents higher costs for health services and contributes to long waitlists [
5,
6]. When referring to somatic patients, Cooper et al. [
6] highlighted that “if the psychological and emotional factors underlying these conditions are not addressed, multiple and unnecessary biological investigations, drug tests, and specialist referrals may be initiated in an attempt to find an organic cause” (p. 2).
In this study, we have found that psychopathologies mediate the relationship between PTE and PTSD. PTSD patients are known to have comorbidities, justifying the greater association between PTSD and other psychopathological symptoms. “It is possible that depressive disorders as well as anxiety symptoms can be a consequence of PTSD as well as an independent risk factor for PTSD following trauma exposure” [
29] (p. 325). Regarding the mediation role of SSD, our findings corroborate that somatic symptoms may be considered a central characteristic of PTSD [
30]. As beforementioned, studies [
3,
4,
27] have shown that PTSD is associated with an increase in the somatic symptom burden, and that “firefighters with PTSD are affected by substantially more physical health symptoms than those without PTSD” [
4] (p. 4).
Portuguese firefighters face extreme events such as violent forest fires, in addition to work in medical emergencies and various types of rescue (e.g., car accidents, flooding and water rescue), having to deal with direct victims, as well as with people who have lost property and loved ones [
1,
27]. Since their work is physically demanding and includes repeated exposure to PTE, firefighters tend to be affected by physical and mental health problems. Likewise, other emergency services professionals are constantly exposed to PTE, seeking strategies to mitigate their impact in order to ensure that they can continue to play a vital role in protecting society [
4].
This study presents some limitations. First, the greater representation of men in the sample can be considered a bias. However, gender was not a significant variable, with the exception of influencing the severity of somatic symptoms. The significance of the gender is in line with other studies in this field, which had found that women reported higher levels of somatic symptoms than men [
31,
32]. Second, the cross-sectional nature of this study prevented us from inferring causality. Third, the use of self-report instruments to infer the presence of PTSD and SSD symptoms. “However, although PHQ-15 does not explicitly ask for functional somatic symptoms, it is highly associated with clinician-rated somatic disorder symptom counts” [
5] (p. 6), as well as PCL-5 is used to screen individuals for PTSD and make a provisional diagnosis [
13]. Despite these limitations, this study has important clinical implications for the treatment of professionals who work in crisis and catastrophe scenarios. Identifying factors that may aggravate psychiatric disorders is critical to improving psychological interventions, which must be tailored to the needs of different individuals and populations. In addition, this study may favor the development of prevention strategies that can be extended to other emergency service professionals.
5. Conclusions
Firefighting is a mentally and physically stressful profession, making firefighters an interest group for research on stress-related psychopathologies. However, most of studies focus on psychopathologies, such as depression and PTSD, when analyzing the consequences of the exposure to extreme events. Although SSD has been associated with PTSD and trauma exposure, there is a paucity of studies investigating the prevalence of somatic symptoms among firefighters. The relevance of this study is due not only to the scarcity of studies on this topic, but also to the impact that forest fires have in Portugal, as well as in other countries around the world (e.g., Greece, USA and Australia).
Our findings have indicated that the firefighter status (being a volunteer firefighter or a professional firefighter) has no influence on the development or the severity of PTSD symptoms, diverging from most of the literature in this field. As abovementioned, characteristics of Portuguese volunteer firefighters can justify such results. The exposure to traumatic events is one of the main factors for the development of stress-related psychopathologies such as PTSD and SSD. According to our analysis, SSD fully mediated the relationship between PTE and PTSD, suggesting that these conditions influence each other.
Further studies may focus on the causal relationship between different stress-related psychopathologies, considering sociodemographic characteristics, in order to determine the risk factors and/or the associated comorbidities. In addition, a longitudinal study could assess the relationship between the exposure to PTE on the severity of PTSD and SSD by considering the influence of a set of risk and protective factors for the development of these conditions in firefighters.








{kind=link}
{kind=link}