
Interleukin-6 Receptor Gene rs1800795 Polymorphism and Expression of Interleukin-6 in Gingival Tissue in Patients with Periodontitis
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Periodontal Examination
2.3. Genotyping
2.4. Real-Time PCR
2.5. Statistical Analysis
3. Results
3.1. IL-6 rs1800795 Polymorphism
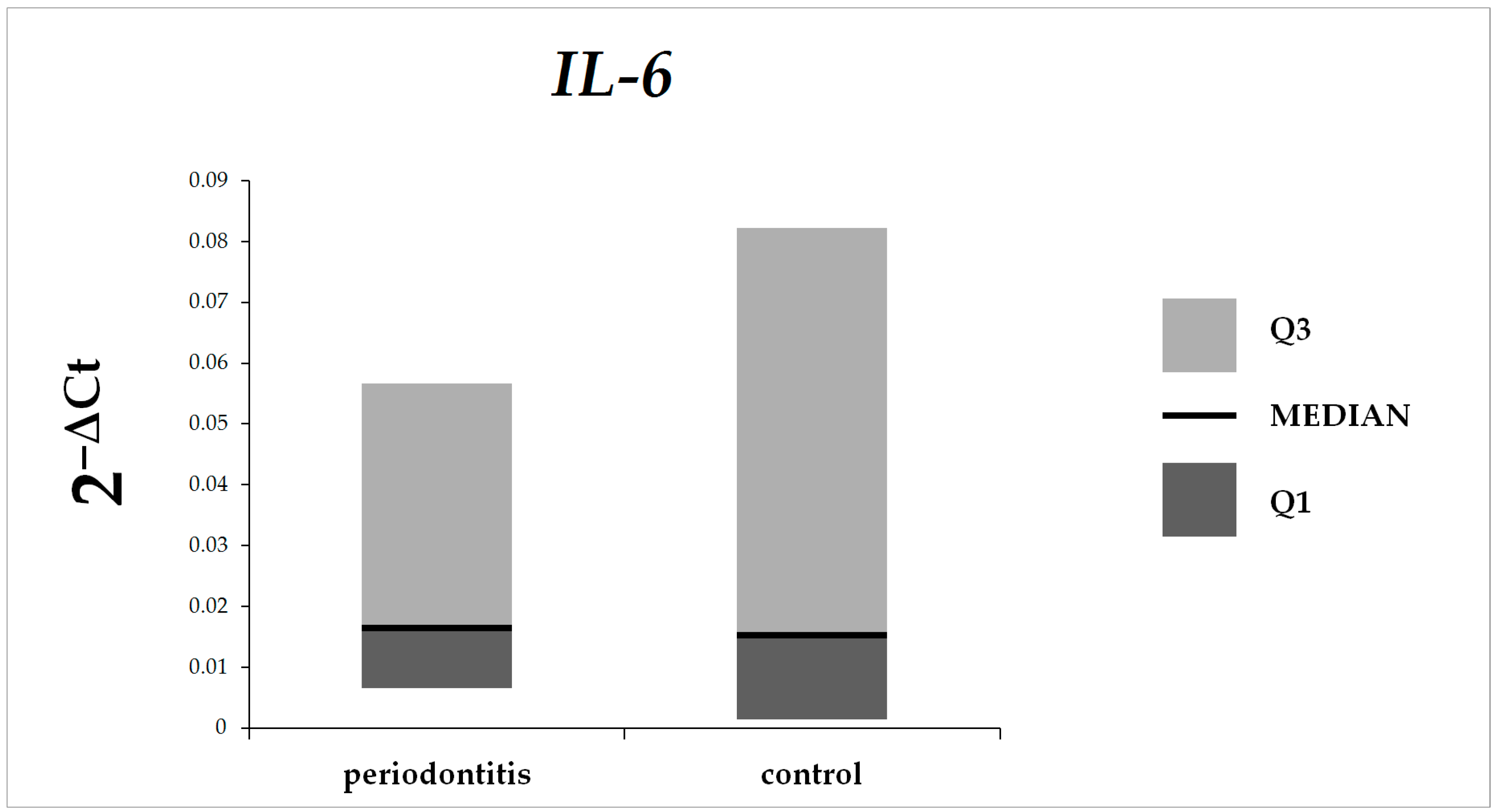
3.2. IL-6 Expression in Gingival Tissue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kwon, T.H.; Lamster, I.B.; Levin, L. Current Concepts in the Management of Periodontitis. Int. Dent. J. 2021, 71, 462–476. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.Y.; Duan, X.Q.; Hu, R.; Ouyang, X.Y. Effect of non-surgical periodontal therapy on serum levels of TNF-a, IL-6 and C-reactive protein in periodontitis subjects with stable coronary heart disease. Chin. J. Dent. Res. 2013, 16, 145–151. [Google Scholar]
- Iwashita, M. Association between Periodontal Disease and Arteriosclerosis-Related Diseases. J. Atheroscler. Thromb. 2023, 30, 1517–1524. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.; Kumar, B.K. Role of periodontal pathogens in atherosclerotic plaque development and progression: An overview. Acta Microbiol. Immunol. Hung. 2023, 70, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.; Li, Z.; Li, H.; Yan, X.; Feng, B.; Xu, L. Association of periodontitis and tooth loss with extent of coronary atherosclerosis in patients with type 2 diabetes mellitus. Front. Endocrinol. 2023, 14, 1243992. [Google Scholar] [CrossRef]
- Kajihara, R.; Sakai, H.; Han, Y.; Amari, K.; Kawamoto, M.; Hakoyama, Y.; Nagashio, S.; Yamada, S.I.; Sanjo, H.; Kurita, H. Presence of periodontitis may synergistically contribute to cancer progression via Treg and IL-6. Sci. Rep. 2022, 12, 11584. [Google Scholar] [CrossRef]
- Cardoso, E.M.; Reis, C.; Manzanares-Céspedes, M.C. Chronic periodontitis, inflammatory cytokines, and interrelationship with other chronic diseases. Postgrad. Med. 2018, 130, 98–104. [Google Scholar] [CrossRef]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Berglundh, T.; Sculean, A.; Tonetti, M.S.; EFP Workshop Participants and Methodological Consultants. Treatment of stage I–III periodontitis–The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47, 4–60. [Google Scholar] [CrossRef]
- Kang, S.; Narazaki, M.; Metwally, H.; Kishimoto, T. Historical overview of the interleukin-6 family cytokine. J. Exp. Med. 2020, 217, e20190347. [Google Scholar] [CrossRef]
- Kishimoto, T. Interleukin-6: Discovery of a pleiotropic cytokine. Arthritis Res Ther. 2006, 8, S2. [Google Scholar] [CrossRef]
- Isola, G.; Lo Giudice, A.; Polizzi, A.; Alibrandi, A.; Murabito, P.; Indelicato, F. Identification of the different salivary Interleukin-6 profiles in patients with periodontitis: A cross-sectional study. Arch. Oral Biol. 2021, 122, 104997. [Google Scholar] [CrossRef] [PubMed]
- Struppek, J.; Schnabel, R.B.; Walther, C.; Heydecke, G.; Seedorf, U.; Lamprecht, R.; Smeets, R.; Borof, K.; Zeller, T.; Beikler, T.; et al. Periodontitis, dental plaque, and atrial fibrillation in the Hamburg City Health Study. PLoS ONE 2021, 16, e0259652. [Google Scholar] [CrossRef] [PubMed]
- Apolinário Vieira, G.H.; Aparecida Rivas, A.C.; Figueiredo Costa, K.; Ferreira Oliveira, L.F.; Tanaka Suzuki, K.; Reis Messora, M.; Sprone Ricoldi, M.; Gonçalves de Almeida, A.L.; Taba, M., Jr. Specific inhibition of IL-6 receptor attenuates inflammatory bone loss in experimental periodontitis. J. Periodontol. 2021, 92, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.H.; Hardy, D.C.; Schuyler, C.A.; Slate, E.H.; Mize, T.W.; Huang, Y. Expression of periodontal interleukin-6 protein is increased across patients with neither periodontal disease nor diabetes, patients with periodontal disease alone and patients with both diseases. J. Periodontal. Res. 2010, 45, 688–694. [Google Scholar] [CrossRef]
- Thuller, K.A.B.R.; Armada, L.; Valente, M.I.; Pires, F.R.; Vilaça, C.M.M.; Gomes, C.C. Immunoexpression of Interleukin 17, 6, and 1 Beta in Primary Chronic Apical Periodontitis in Smokers and Nonsmokers. J. Endod. 2021, 47, 755–761. [Google Scholar] [CrossRef]
- Puletic, M.; Velikic, G.; Maric, D.M.; Supic, G.; Maric, D.L.; Radovic, N.; Avramov, S.; Vojvodic, D. Clinical Efficacy of Extracellular Vesicle Therapy in Periodontitis: Reduced Inflammation and Enhanced Regeneration. Int. J. Mol. Sci. 2024, 25, 5753. [Google Scholar] [CrossRef]
- Guarnieri, R.; Reda, R.; Di Nardo, D.; Miccoli, G.; Pagnoni, F.; Zanza, A.; Testarelli, L. Expression of IL-1β, IL-6, TNF-α, and a-MMP-8 in sites with healthy conditions and with periodontal and peri-implant diseases: A case-control study. J. Dent. Res. Dent. Clin. Dent. Prospect. 2024, 18, 135–142. [Google Scholar] [CrossRef]
- Yáñez, L.; Soto, C.; Tapia, H.; Pacheco, M.; Tapia, J.; Osses, G.; Salinas, D.; Rojas-Celis, V.; Hoare, A.; Quest, A.F.G.; et al. Co-Culture of P. gingivalis and F. nucleatum Synergistically Elevates IL-6 Expression via TLR4 Signaling in Oral Keratinocytes. Int. J. Mol. Sci. 2024, 250, 3611. [Google Scholar] [CrossRef]
- Kerkis, I.; da Silva, Á.P.; Araldi, R.P. The impact of interleukin-6 (IL-6) and mesenchymal stem cell-derived IL-6 on neurological conditions. Front. Immunol. 2024, 15, 1400533. [Google Scholar] [CrossRef]
- Kumar, S. Evidence-Based Update on Diagnosis and Management of Gingivitis and Periodontitis. Dent. Clin. N. Am. 2019, 63, 69–81. [Google Scholar] [CrossRef]
- Ptasiewicz, M.; Bębnowska, D.; Małkowska, P.; Sierawska, O.; Poniewierska-Baran, A.; Hrynkiewicz, R.; Niedźwiedzka-Rystwej, P.; Grywalska, E.; Chałas, R. Immunoglobulin Disorders and the Oral Cavity: A Narrative Review. J. Clin. Med. 2022, 11, 4873. [Google Scholar] [CrossRef] [PubMed]
- Ptasiewicz, M.; Grywalska, E.; Mertowska, P.; Korona-Głowniak, I.; Poniewierska-Baran, A.; Niedźwiedzka-Rystwej, P.; Chałas, R. Armed to the Teeth-The Oral Mucosa Immunity System and Microbiota. Int. J. Mol. Sci. 2022, 23, 882. [Google Scholar] [CrossRef] [PubMed]
- Soysal, F.; Unsal, B.; Isler, S.C.; Akca, G.; Bakirarar, B.; Ozcan, M. Evaluation of salivary stress markers and inflammatory cytokine levels in peri-implantitis patients. Clin. Oral Investig. 2024, 28, 290. [Google Scholar] [CrossRef]
- Syrjäläinen, S.; Männistö, S.; Könönen, E.; Pussinen, P.; Gürsoy, M.; Suominen, A.L.; Jousilahti, P.; Gürsoy, U.K. Dietary inflammatory index in relation to salivary cytokine concentrations and periodontitis: A cross-sectional analysis. J. Clin. Periodontol. 2024, 51, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Arunachalam, L.T.; Suresh, S.; Lavu, V.; Vedamanickam, S.; Viswanathan, S.; Thirumalai Nathan, R.D. Association of salivary levels of DNA sensing inflammasomes AIM2, IFI16, and cytokine IL18 with periodontitis and diabetes. J. Periodontol. 2024, 95, 114–124. [Google Scholar] [CrossRef]
- Weber, J.; Scholz, K.J.; Schenke, I.M.; Pfab, F.; Cieplik, F.; Hiller, K.A.; Buchalla, W.; Sahm, C.; Kirschneck, C.; Paddenberg-Schubert, E. Randomized controlled clinical trial on the efficacy of a novel antimicrobial chewing gum in reducing plaque and gingivitis in adolescent orthodontic patients. Clin. Oral Investig. 2024, 28, 272. [Google Scholar] [CrossRef]
- Jaafar, A.; Dhar, V.; Hsu, K.L.; Tinanoff, N.J. Associations between risk factors, including approximal contact types and dental caries in children from low-income families. Pilot study. Clin. Pediatr. Dent. 2024, 48, 60–68. [Google Scholar] [CrossRef]
- Santos, R.T.N.D.; Lima, L.P.O.; Muniz, M.T.C.; Álvares, P.R.; Silveira, M.M.F.D.; Sobral, A.P.V. Genetic polymorphism of interleukins 6 and 17 correlated with apical periodontitis: A Cross-sectional study. Braz. Dent. J. 2023, 34, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Sitompul, S.I.; Pikir, B.S.; Aryati; Kencono Wungu, C.D.; Supandi, S.K.; Sinta, M.E. Analysis of the Effects of IL-6-572 C/G, CRP-757 A/G, and CRP-717 T/C Gene Polymorphisms; IL-6 Levels; and CRP Levels on Chronic Periodontitis in Coronary Artery Disease in Indonesia. Genes 2023, 14, 1073. [Google Scholar] [CrossRef]
- Mehar, R.; Swarnakar, S.; Lakkakula, S.; Verma, H.K.; Bhaskar, L.V.K.S. Interleukin-6 gene -174G>C promoter polymorphism reduces the risk of periodontitis in Brazilian populations: A meta-analysis. J. Oral Biosci. 2021, 63, 388–393. [Google Scholar] [CrossRef]
- Cirelli, T.; Nepomuceno, R.; Rios, A.C.S.; Orrico, S.R.P.; Cirelli, J.A.; Theodoro, L.H.; Barros, S.P.; Scarel-Caminaga, R.M.J. Genetic polymorphisms in the Interleukins IL1B, IL4, and IL6 are associated with concomitant periodontitis and type 2 diabetes mellitus in Brazilian patients. Periodontal. Res. 2020, 55, 918–930. [Google Scholar] [CrossRef] [PubMed]
- Mazurek-Mochol, M.; Bonsmann, T.; Mochol, M.; Poniewierska-Baran, A.; Pawlik, A. The Role of Interleukin 6 in Periodontitis and Its Complications. Int. J. Mol. Sci. 2024, 25, 2146. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Zhang, C.; Mi, Y. IL-6 gene rs1800795 polymorphism and diabetes mellitus: A comprehensive analysis involving 42,150 participants from a meta-analysis. Diabetol. Metab. Syndr. 2022, 14, 95. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| PD Patients (n = 200) | Control Group (n = 158) | p a | p b | OR (95% CI) | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | |||||
| IL-6 rs1800795 | ||||||||
| genotype | ||||||||
| GG | 48 | 24.00% | 46 | 29.12% | 0.35 | CC + GC vs. GG | 0.28 | 1.30 (0.81–2.09) |
| GC | 100 | 50.00% | 80 | 50.63% | CC vs. GC + GG | 0.21 | 1.38 (0.84–2.28) | |
| CC | 52 | 26.00% | 32 | 20.25% | CC vs. GG | 0.17 | 1.56 (0.86–2.83) | |
| GC vs. GG | 0.52 | 1.20 (0.73–1.98) | ||||||
| CC vs. GC | 0.35 | 1.30 (0.77–2.21) | ||||||
| IL-6 rs1800795 | ||||||||
| allele | ||||||||
| G | 196 | 49.00% | 172 | 54.43% | ||||
| C | 204 | 51.00% | 144 | 45.57% | C vs. G | 0.15 | 1.24 (0.93–1.67) | |
| PD Patients (n = 130) | Control Group (n = 124) | p a | p b | OR (95% CI) | ||||
|---|---|---|---|---|---|---|---|---|
| (Nonsmokers) | (Nonsmokers) | |||||||
| n | % | n | % | |||||
| IL-6 rs1800795 | ||||||||
| genotype | ||||||||
| GG | 34 | 26.15% | 37 | 29.84% | 0.50 | CC + GC vs. GG | 0.58 | 1.20 (0.69–2.08) |
| GC | 63 | 48.46% | 63 | 50.81% | CC vs. GC + GG | 0.29 | 1.42 (0.78–2.57) | |
| CC | 33 | 25.39% | 24 | 19.35% | CC vs. GG | 0.29 | 1.50 (0.74–3.02) | |
| GC vs. GG | 0.88 | 1.09 (0.61–1.95) | ||||||
| CC vs. GC | 0.34 | 1.38 (0.73–2.59) | ||||||
| IL-6 rs1800795 | ||||||||
| allele | ||||||||
| G | 131 | 50.38% | 137 | 55.24% | ||||
| C | 129 | 49.62% | 111 | 44.76% | C vs. G | 0.29 | 1.22 (0.86–1.72) | |
| PD Patients (n = 70) | Control Group (n = 34) | p a | p b | OR (95% CI) | ||||
|---|---|---|---|---|---|---|---|---|
| (Smokers) | (Smokers) | |||||||
| n | % | n | % | |||||
| IL-6 rs1800795 | ||||||||
| genotype | ||||||||
| GG | 14 | 20.00% | 9 | 26.47% | 0.75 | CC + GC vs. GG | 0.46 | 1.44 (0.55–3.77) |
| GC | 37 | 52.86% | 17 | 50.00% | CC vs. GC + GG | 0.81 | 1.21 (0.47–3.14) | |
| CC | 19 | 27.14% | 8 | 23.53% | CC vs. GG | 0.56 | 1.53 (0.47–4.95) | |
| GC vs. GG | 0.60 | 1.40 (0.51–3.86) | ||||||
| CC vs. GC | 1.00 | 1.09 (0.40–2.98) | ||||||
| IL-6 rs1800795 | ||||||||
| allele | ||||||||
| G | 65 | 46.43% | 35 | 51.47% | ||||
| C | 75 | 53.57% | 33 | 48.53% | C vs. G | 0.56 | 1.22 (0.69–2.19) | |
| GG | GC | CC | GG vs. GC * p-Value | GG vs. CC * p-Value | CC vs. GC * p-Value | GG vs. GC + CC * p-Value | CC vs. GC + GG * p-Value | |
|---|---|---|---|---|---|---|---|---|
| API (%) | 72.19 ± 18.99 | 74.63 ± 20.97 | 72.67 ± 19.33 | 0.385 | 0.860 | 0.465 | 0.496 | 0.652 |
| BoP (%) | 61.35 ± 24.59 | 57.10 ± 23.82 | 56.50 ± 27.98 | 0.313 | 0.396 | 0.724 | 0.290 | 0.550 |
| PPD | 4.67 ± 1.09 | 4.60 ± 1.29 | 4.42 ± 1.09 | 0.576 | 0.341 | 0.581 | 0.431 | 0.435 |
| CAL | 5.22 ± 1.60 | 5.06 ± 1.58 | 4.92 ± 1.43 | 0.677 | 0.309 | 0.523 | 0.475 | 0.384 |
| Parameter | R | p |
|---|---|---|
| API | 0.17822 | 0.542 |
| BoP | −0.44884 | 0.107 |
| PPD | −0.17802 | 0.542 |
| CAL | 0.17822 | 0.542 |
| Parameter | R | p |
|---|---|---|
| API | −0.72294 | 0.042 |
| BoP | −0.63434 | 0.091 |
| PPD | −0.64286 | 0.085 |
| CAL | −0.17964 | 0.670 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazurek-Mochol, M.; Bonsmann, T.; Malinowski, D.; Serwin, K.; Czerewaty, M.; Safranow, K.; Pawlik, A. Interleukin-6 Receptor Gene rs1800795 Polymorphism and Expression of Interleukin-6 in Gingival Tissue in Patients with Periodontitis. Microorganisms 2024, 12, 1954. https://doi.org/10.3390/microorganisms12101954
Mazurek-Mochol M, Bonsmann T, Malinowski D, Serwin K, Czerewaty M, Safranow K, Pawlik A. Interleukin-6 Receptor Gene rs1800795 Polymorphism and Expression of Interleukin-6 in Gingival Tissue in Patients with Periodontitis. Microorganisms. 2024; 12(10):1954. https://doi.org/10.3390/microorganisms12101954
Chicago/Turabian StyleMazurek-Mochol, Małgorzata, Tobias Bonsmann, Damian Malinowski, Karol Serwin, Michał Czerewaty, Krzysztof Safranow, and Andrzej Pawlik. 2024. "Interleukin-6 Receptor Gene rs1800795 Polymorphism and Expression of Interleukin-6 in Gingival Tissue in Patients with Periodontitis" Microorganisms 12, no. 10: 1954. https://doi.org/10.3390/microorganisms12101954