1. Introduction
The first reports of implantology were recorded in ancient Egypt, where two teeth were connected by a gold wire passed through holes. This discovery was made by the Egyptologist Hermann Junker in 1914, and it is still the best-known proof of advanced dentistry that thrived from those times [
1]. Currently, implantology is an ever-growing branch of dentistry, and is a contemporary part of human and veterinary medicine. In order to implant a tooth prosthesis, an implant site in the bone must be prepared. This must be done using special drilling systems. The mentioned procedure destroys the surrounding tissues mechanically and by the heat generated by the rotating drill. During osteointegration, the bone temperature may not exceed the temperature of 47 °C to prevent thermal osteonecrosis [
2]. Earlier study showed that the temperature development and its influence on the bone tissue is proportional to the time of exposure to the friction during the drilling procedure [
3]. Excessive destruction of the surrounding tissues like crushed bone, necrosis, or bone architecture annihilation influences the possibility of achieving good osteointegration, which is mandatory for dental implant success [
4,
5]. This bone change can vary according to the drill’s design, parameters, and cooling system utilized. The ideal method of drilling is difficult to define due to the anisotropic structure of bone, which connects organic and inorganic components [
6]. Swine rib has a similar micro- and macrostructure to human mandible and maxilla and it can be an adequate in vitro model for biological studies [
3]. The process of bone remodeling seems to be similar in human and other animals (pigs) including trabecular and intra-cortical based remodeling as well as cortical mineralization rate [
7].
The expression of “osteointegration” describes a rigid, clinically asymptomatic connection between a bone tissue and implant, which has an integrity, allowing it to fulfil its function. The process of osseointegration is divided into primary and secondary phases. The primary phase is the connection between the implant and surrounding tissue, whilst, the second phase is based on the biologic activity of bone cells causing local inflammation, which enables healing and intensifies the contact of bone and implant [
8]. In vitro, the bone damage surrounding the implant can be estimated microscopically (size and morphology of destruction zone around drilled hole).
The aim of the study was to describe the damage zone caused by drilling using pig ribs as a model for human bones of the splanchnocranium. Accessible literature lack larger studies comparing the changes of bone tissues surrounding implantation site with regard to the drilling system used, diameter of the drill, drilling temperature, and cooling system.
Optimal elaboration method of the bone bed before implantation determines the achievement of proper implant osteointegration. A crucial element of the preparation procedure of the bed is to minimalize thermic and mechanical injuries of the bone. Increase in temperature during preparation over 47 °C (over 1 min) leads to complete denaturation of the organic component in bone cell matrix, which can negatively affect the osteointegration process [
9,
10,
11]. The main cause of this phenomenon is the disturbance of the collagen fibers’ structure and their cracking, thus implant bone connection stiffness changes and also increases vulnerability for bone tissue compression. Kim et al. and Bachus et al. proved the local thermal necrosis occurrence within the bone tissue after crossing the limit of temperature (over 50 °C) and prolonging procedure time during bone bed preparation [
12,
13].
2. Material and Methods
In this study, a total of 81 dental implant sites were made. For this purpose, nine fresh swine ribs were obtained from the Polish Large White (PLW) swine breed. The method of sample collection did not require permission from the ethical committee. The size (length, width, and thickness) of all samples were comparable, with the mean values of 146.2 mm × 24.6 mm × 21.3 mm, respectively. Implant sites were prepared using the following dental systems (
Table 1):
BEGO Semados® RS (BEGO Implant Systems GmbH & Co., Bremen, Germany)—drills: pilot, 𝜙2.5, and final, 𝜙3.0;
BIOMET 3i® T3 (Biomet 3i LLC, Palm Beach Gardens, FL, USA)—drills: pilot, 𝜙2.3, and final, 𝜙2.75); and
NEO BIOTECH® IS-III Active (Neo Biotech Co., Ltd., Seoul, Korea)—drills: pilot, 𝜙2.2, and final, 𝜙2.9.
Each of the drills was tested with different cooling methods and drill rotation speed. A cooling system was supplied with:
0.9% NaCl solution (temperature approx. 20 °C);
0.9% NaCl solution (temperature approx. 3 °C); and
without any cooling liquid supplementation.
Drilling was carried out with the following speeds (by the same person):
800 rpm;
1200 rpm; and
1500 rpm.
In order to prepare the implant sites, the NeoSurge implant micromotor was set at a contra angle with a 32:1 gear reduction. In all caused, the pilot drilling was used before the final drilling, not only because of dental systems requirements, but also to evaluate the drill diameter as an injury factor acting in bone model. Each of the drills were used only once at each drilling speed (800, 1200, and 1500 rpm) to avoid it becoming blunt. This may in turn generate additional heat during this procedure. All the implant sites were made on the anterior side of the swine ribs, reaching the depth of 10 mm. The same trained surgeon prepared each of the dental implants maintaining the optimal drilling force. Additionally, the ribs were fixed to the table mount to ensure the stability and repeatability. Drilling was done with an infrared thermographic camera ThermaCAM P640 [
14] that registered the heat produced.
The samples were fixed in a 4% formaldehyde solution of pH 7.2 for two days and were rinsed under running water. Subsequently, the ribs were cut using a low-speed, water cooled diamond saw to obtain an opened implant site with the biggest possible diameter.
The obtained material was rinsed in a shaker at 25 °C for 10 min. A 0.9% sodium chloride solution was used to extract clear bone tissue. The material was examined under a fluorescent microscope Nikon Eclipse 80i using UV-2A (EX:330-380, DM:400, BA:420) and B-2A (EX: 450-490, DM:505, BA:520) filters with a magnification of 40× and 100×. Then, the rib was observed directly under fluorescence microscope and pictures were taken. Thanks to this method, we avoided a number of potential unwanted changes in the tissue adjacent to the drill hole. Moreover, it allowed almost direct observation of the borehole after the experiment.
The morphometric analysis was carried out using NIS Elements AR software. Additionally, the performed measurements were done in a closed room under the same conditions, maintaining the temperature and humidity, without additional air flow.
All data were subjected to statistical analysis using GraphPad Prism 5.0 (GraphPad Software, La Jolla, CA, USA) software. The D’Agostino and Pearson normality test were used to determine the normality of the data. Based on the data distribution, either a one-way ANOVA with the Bonferroni post-hoc test or the Kruskal–Wallis with the post-hoc Dunns test were used to compare more than two groups of data. Correlations between the groups were determined using the Spearman correlation coefficient. p < 0.05 was considered statistically significant.
3. Results
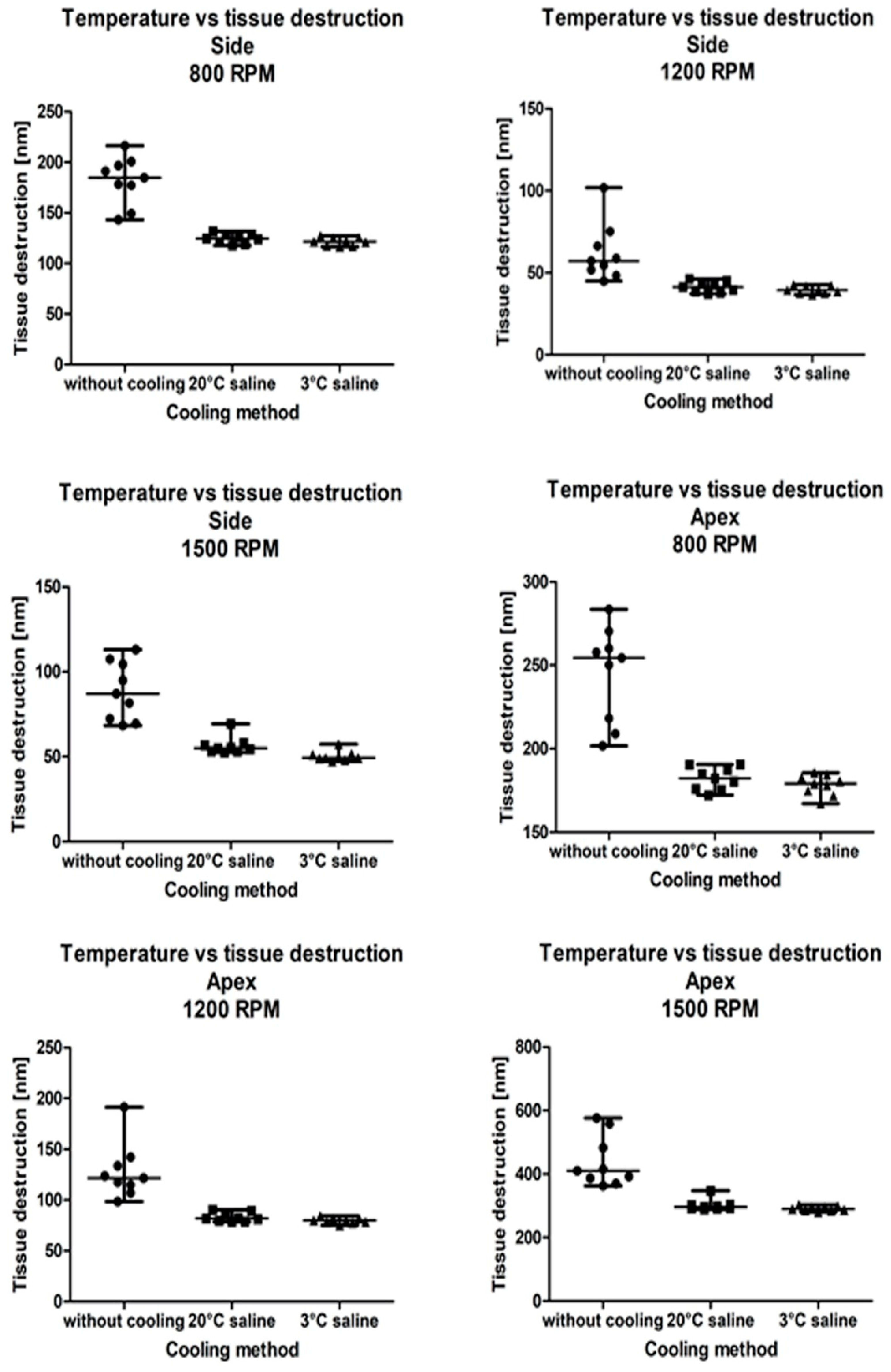
The tissue destruction zone was significantly lower when saline was used to cool down the drill in all three drill rotation speeds and both drilling sites (apex: 800 rpm:
p = 0.0001; 1200 rpm:
p < 0.0001; 1500 rpm:
p < 0.0001; side: 800 rpm:
p = 0.0001; 1200 rpm:
p = 0.0002; 1500 rpm:
p < 0.0001). A post-hoc analysis showed no differences between 20 °C and 3 °C saline, regardless of drill rotation speed and drilling site (
Figure 1). Spearman correlation coefficients between the actual temperature and tissue destruction were calculated for each drilling site, drilling speed, and cooling method (
Table 2).
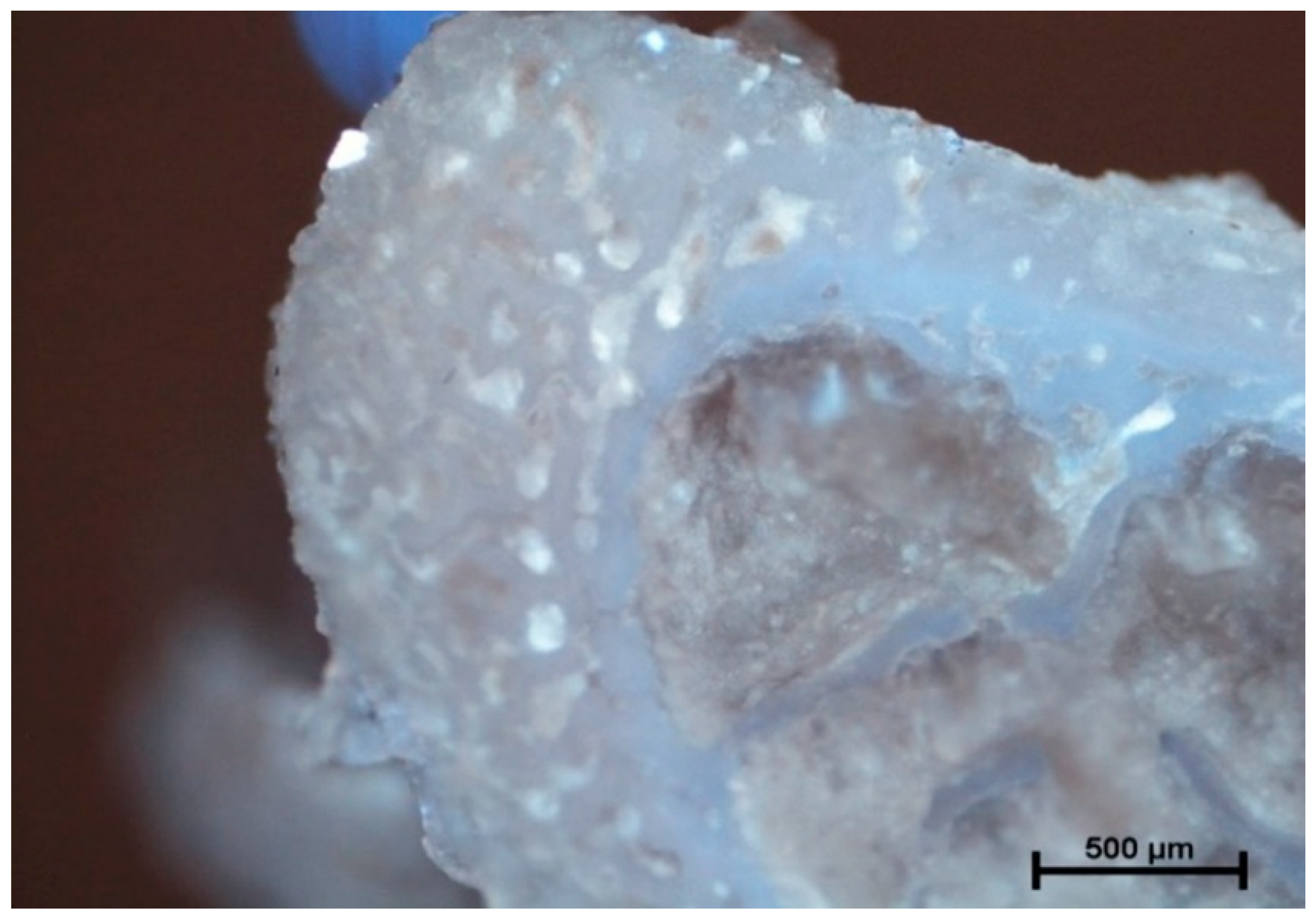
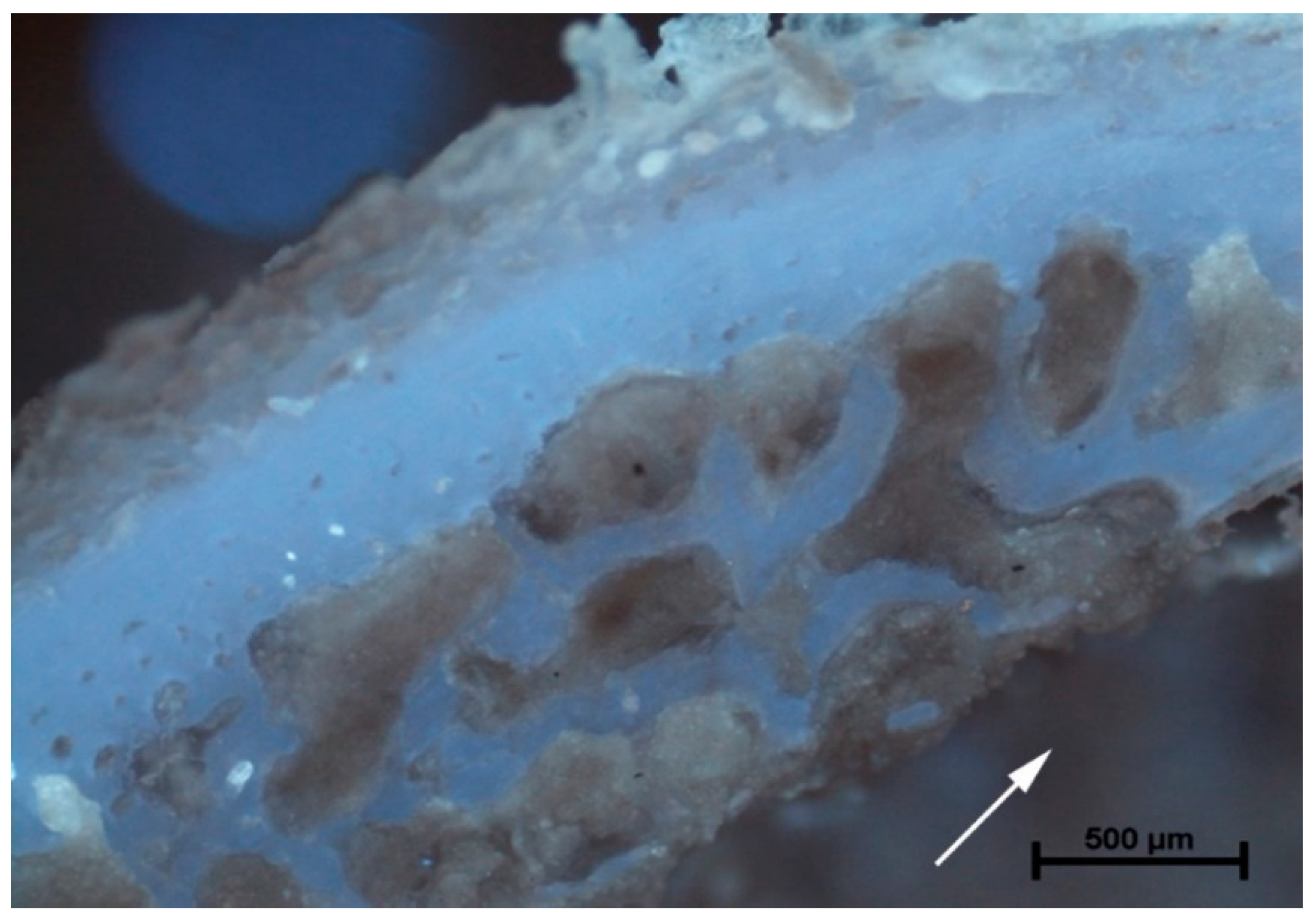
The analysis of microanatomical structure showed the different morphological changes in samples referring to the drilling speed and cooling method used. During drilling, with a speed of 800 rpm and cooling liquid at temperature 3 °C, the zone of compressed bone tissue was visible (
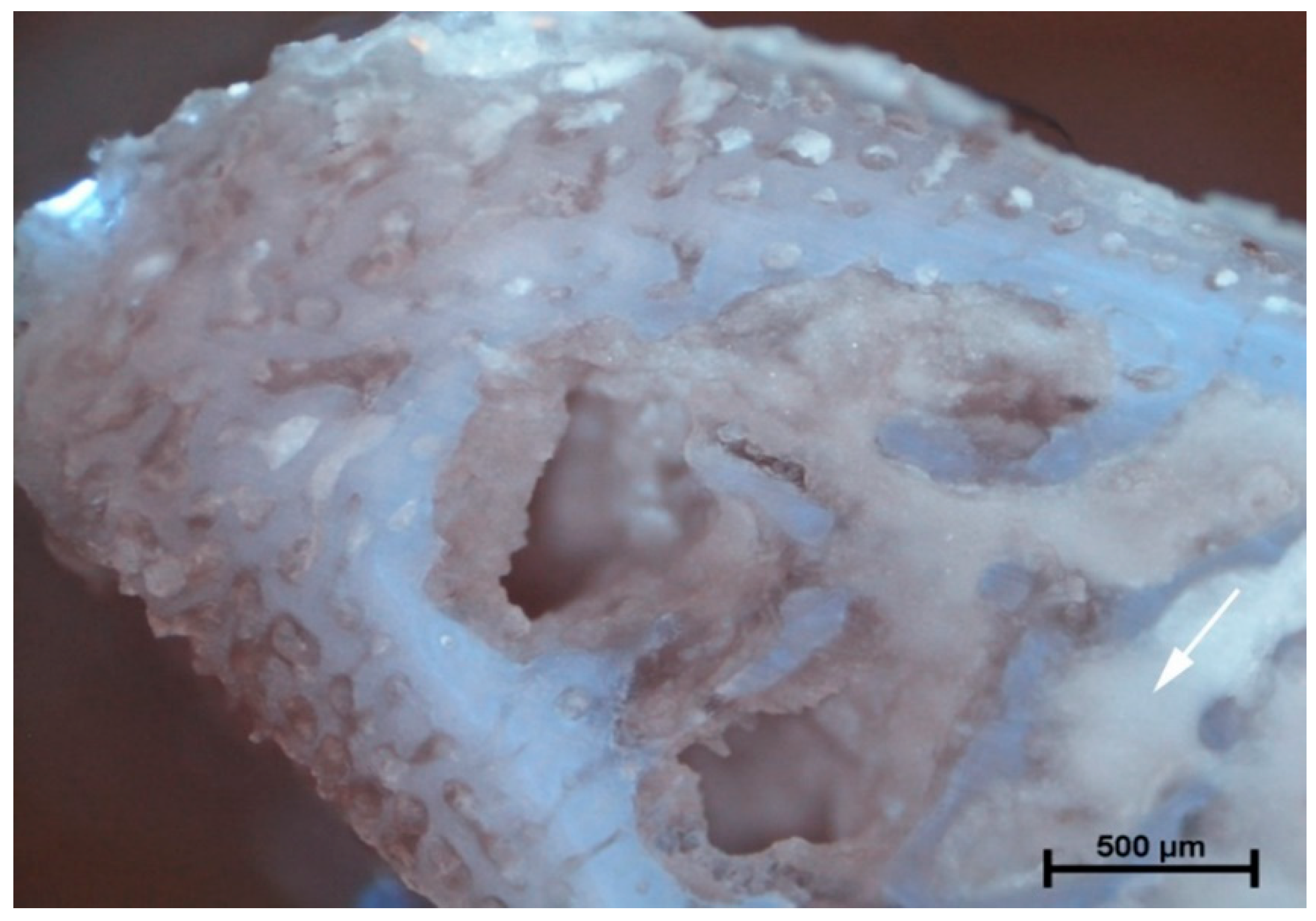
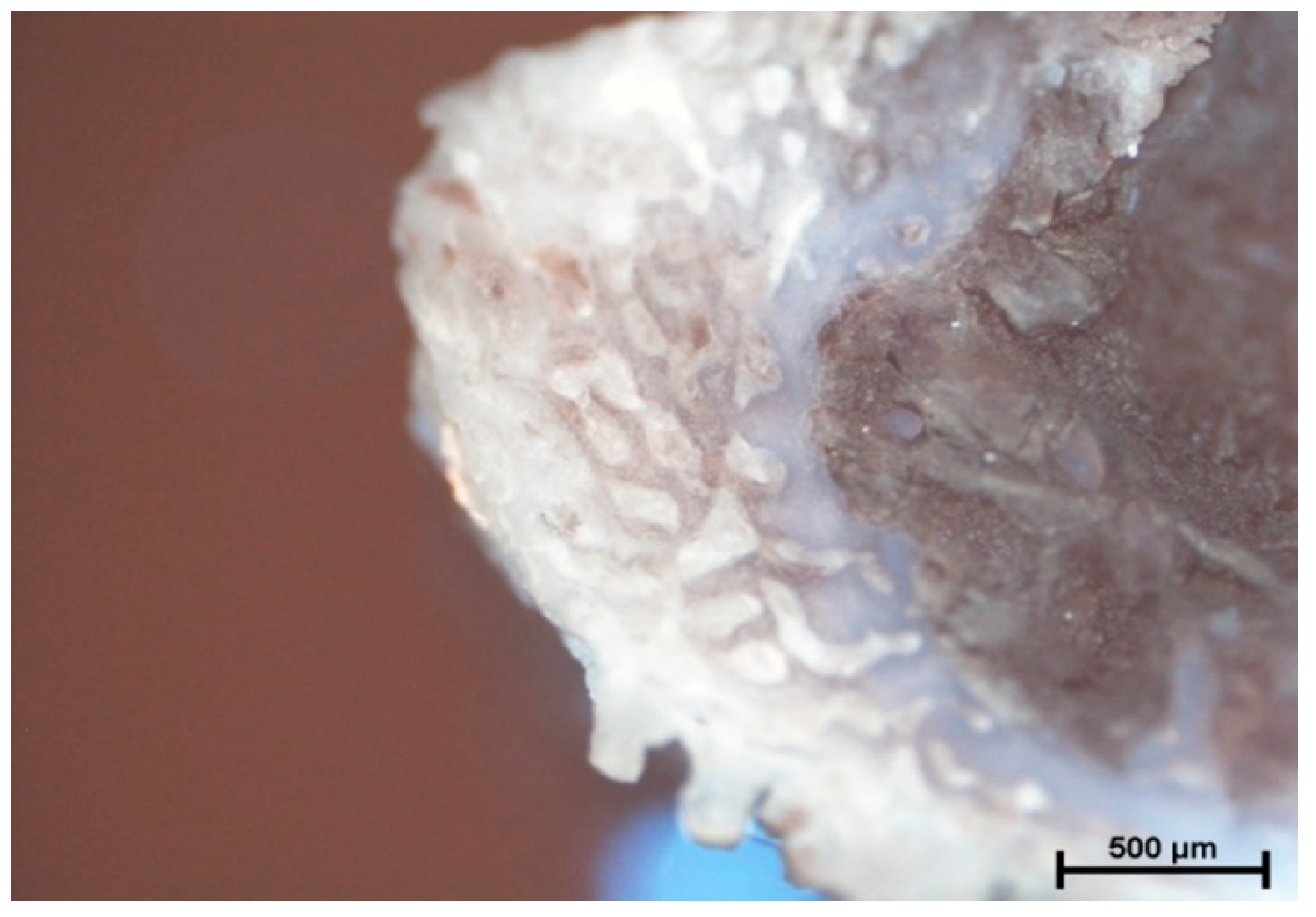
Figure 2). Simultaneously, the same speed of drilling without any cooling caused the moderate destruction of bone tissue and bone marrow (
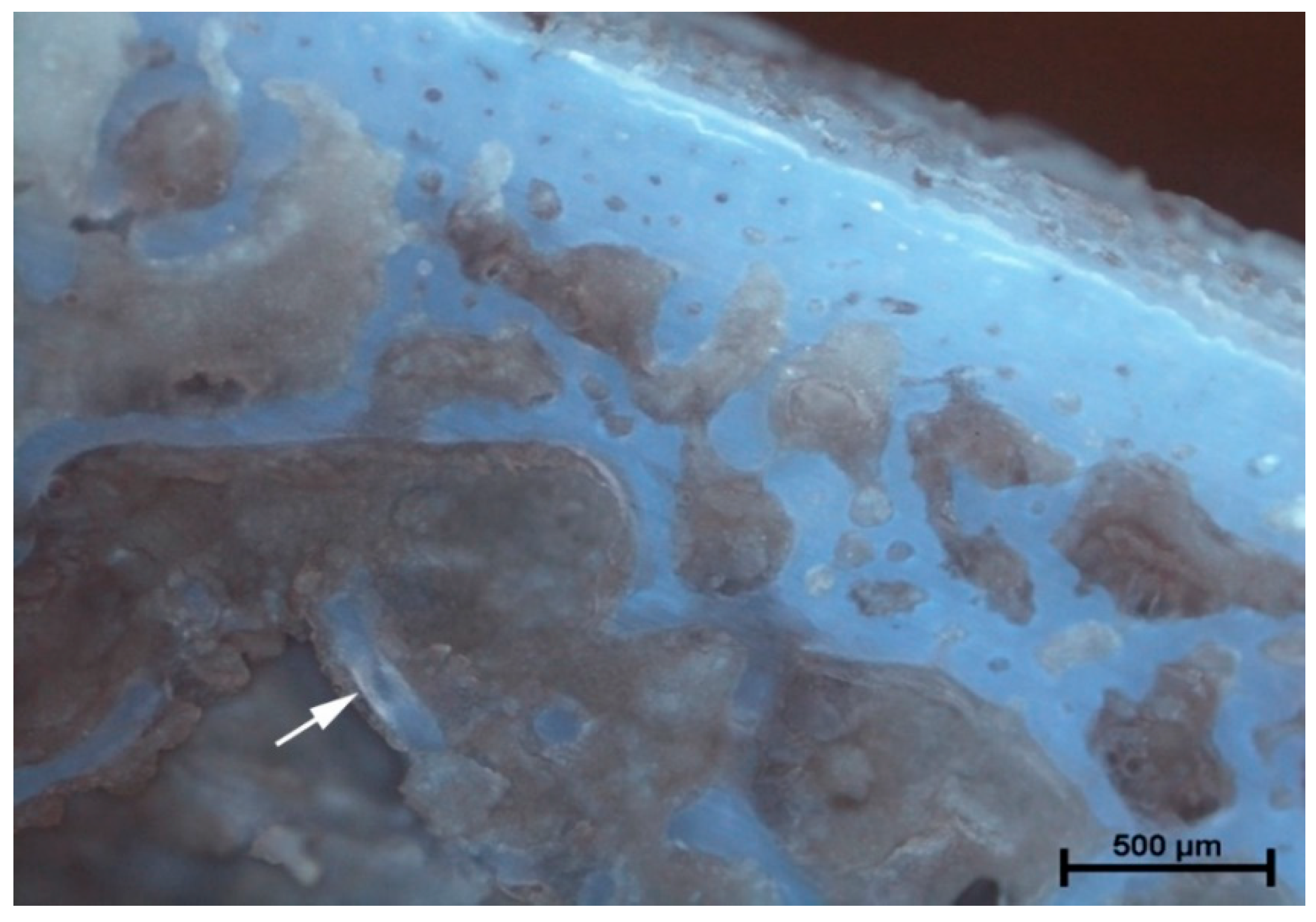
Figure 3). The microanatomical picture of changes generated by drilling with a speed of 1200 rpm (cooling liquid at 20 °C) showed the apical zone of rib with visible connective tissue without any areas of strong tissue compression (
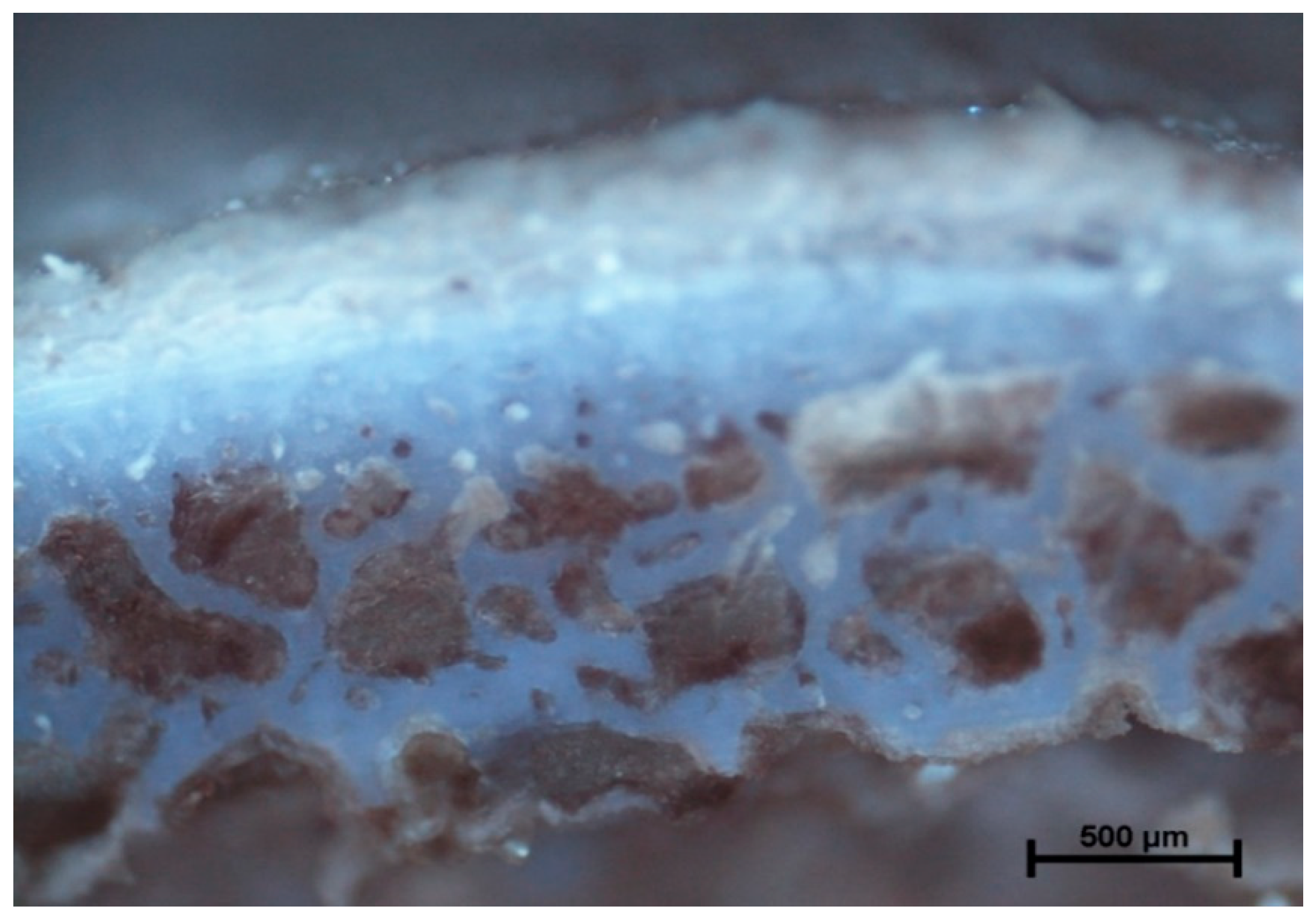
Figure 4). The same drilling speed, but with a cooling method at 3 °C, caused total destruction of the bone tissue and bone marrow. The empty bone marrow cavity was clearly distinguished from other parts of the rib’s wall (
Figure 5). Finally, the drilling speed of 1500 rpm resulted in the lack of strong compression of the bone tissue and the apical area of rib filled with the connective tissue (
Figure 6), when any cooling system was not used. In contrast, the use of cooling liquid at 20 °C changed the result of drilling, causing total bone tissue and bone marrow destruction and the presence of damaged trabecular architecture of bone with empty bone marrow cavity (
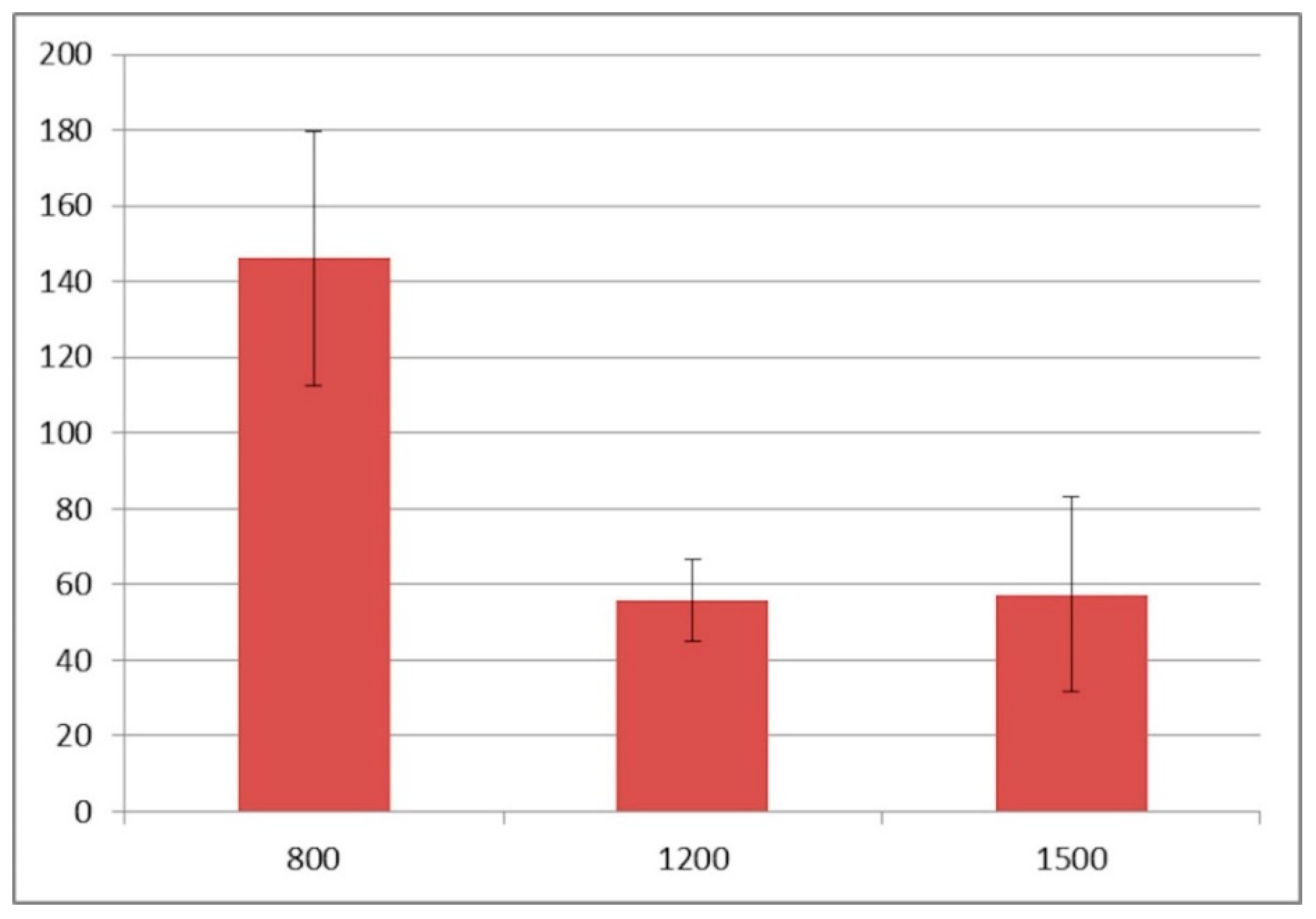
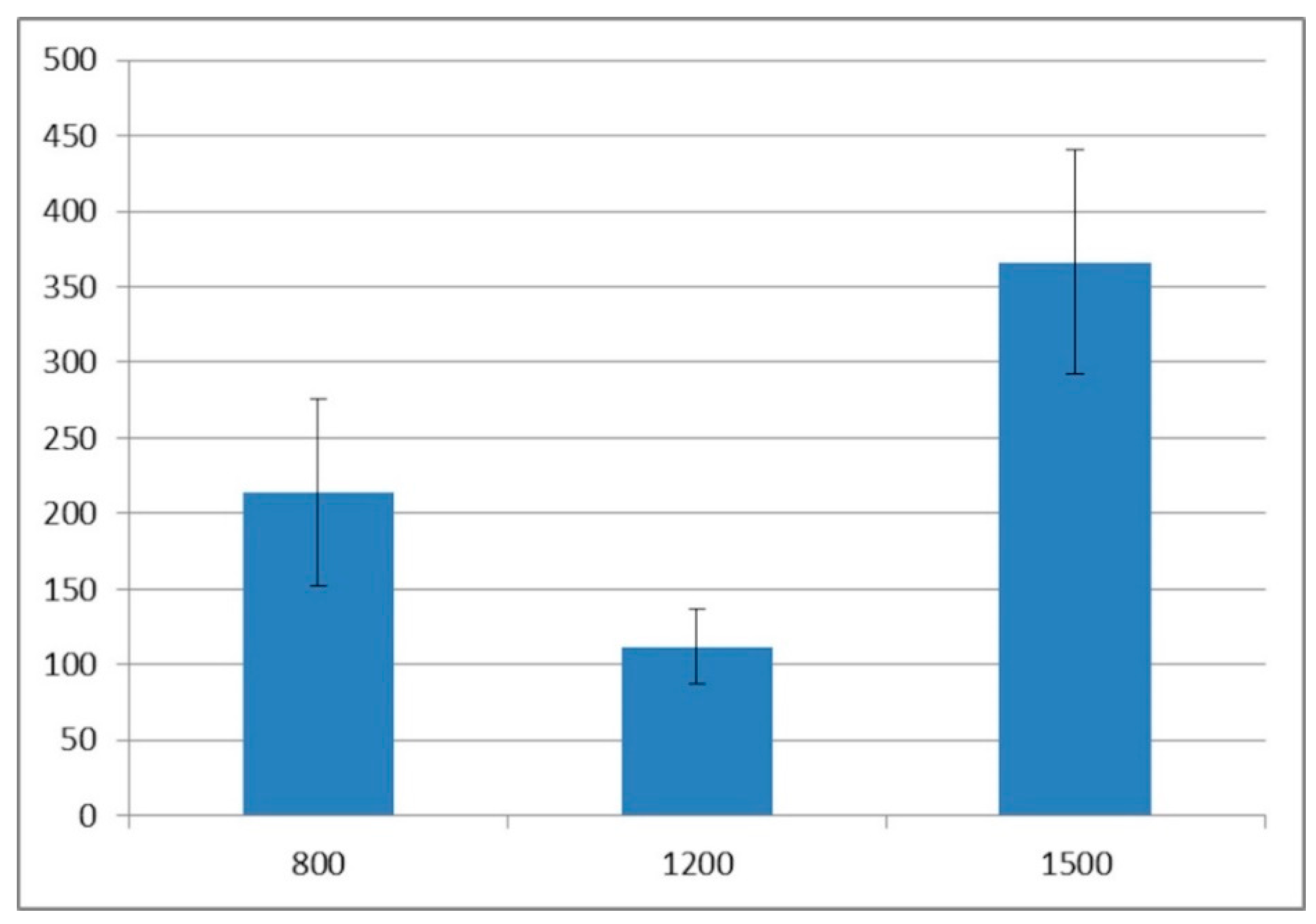
Figure 7). The histometry of the damage zone at the wall of the drilling canal (
Figure 8) and the thickness of compressed bone tissue at the top of drill (
Figure 9) proved that the use of an intermediate speed of drilling (1200 rpm) was the least traumatic for the model.
4. Discussion
Thermal osteonecrosis is a complex and multistage process, in which enzymatic and membrane proteins are destroyed, the osteoclastic and osteoblastic activity is significantly lowered, and dehydration as well as desiccation of the cell occurs. All these processes may lead to cell death, impaired healing, prolonged remodeling, and early implant failure. The first symptom of osteonecrosis is usually blood flow reduction, followed by osteoclastic resorption, which can no longer play their role in keeping a healthy structure cortical and spongy bone. Accurate temperature, which causes thermal damage, remains unclear [
6,
15].
The aim of the study was to measure the damage done during drilling to the tissues surrounding the implantation site in comparison to the drilling system, its diameter, drilling temperature, and cooling methods. The material was examined under a fluorescent microscope in order to receive the results, which accurately illustrated the thermal damage of the bone. Many factors have been described as the reasons for temperature rise during the dental implant site preparation including bone quality and its cortical thickness, drill type (material, design, diameter and wearing), drilling speed, feed rate and depth, pressure put while drilling, cooling approach and pre-drilling [
6]. Previous studies showed that when the temperature during dental implant site preparation rises to 47 °C and remains so for 1 min, the bone is resorbed and replaced with fat tissue. We may therefore hypothesize, that a temperature under 47 °C combined with drilling time not exceeding 1 min is safe and protects against osteonecrosis. On the other hand, they revealed that heating the bone during the implant site preparation to the temperature of 50 °C caused resorption of the bone in the amount of 30% [
16]. Many studies have been conducted in order to determine which cooling system and cooling conditions are the most efficient to avoid thermal necrosis. In general, cooling systems are divided into internal and external coolant approaches. Internal cooling systems deliver coolant (fluid or air) through the channel in the drill, whereas an external cooling system delivers it on the outer side of the drill or directly to the drilling point using fully automatic systems or a simple manual syringe [
17]. As the depths are unknown for their infiltration sites, which are done by the external cooling systems, there is a limited possibility of cooling in the area where the drill has contact with the bone. In 1975, Kirschner and Mayer introduced the first internally cooled drills, so the coolant could also achieve the top of the rotating drill [
18]. What is interesting to note is that another study performed many years after introducing the invention above-mentioned showed that more heat was generated in the superficial part of the bone than at the bottom of the drilling cavity. This means that the external delivery of the coolant should remain a sufficient method of lowering the temperature while drilling [
19]. Therefore in our study, an external cooling system was used and evaluated. It was clearly visible that the lack of any coolant significantly increased the bone tissue destruction significantly in all three drill rotation speeds and both drilling sites (
Figure 1 and
Table 2).
Another extremely significant cooling practice, done while drilling, is irrigation and the amount of coolant. Several studies have compared the efficiency of lowering the temperature depending on the presence of coolant and its amount. Kalidindi compared the drilling with and without coolant, which showed a significant increase in temperature in cases without [
20]. Sindel et al. compared irrigation volumes of 12 mL/min and 30 mL/min and revealed no significant difference between them [
21]. In contrast, Mercan et al., who compared 32 mL/min, 44 mL/min, 56 mL/min, and 68 mL/min amounts of coolant, showed a visible reduction in thermal damages with volumes higher than 32 mL/min. They suggested that the most effective volume, which should be used to provide continuous cooling and limited thermal damage, is 56 mL/min [
22]. Additionally, the temperature of the coolant may significantly impact the thermal necrosis and reduce its risk. Sener et al. showed that a lower temperature of the coolant (10 °C compared to 25 °C) may sufficiently decrease the final temperature and lower the risk of thermal damage [
19]. In our study, we compared thermal damage in three conditions: without cooling and with cooling by 3 °C, and 20 °C of the 0.9% NaCl, which revealed a notable higher thermal damage in cases without coolant compared to cases with coolant, but the differences in damage zone between cases with 3 °C and 20 °C coolant temperatures were irrelevant.
According to many different results published, the optimal speed for bone drilling remains unidentified. There is no compromise regarding the relationship between the drilling speed and temperature. The first research carried out in 1958 in order to examine the correlation between drilling rate and temperature revealed that the increase in drilling speed increased the temperature while drilling [
23]. Many years later, these results were confirmed by Augustin et al., who evaluated five drill speeds between 188 and 1820 rpm, Nam et al., who used 600 and 1200 rpm drilling speeds, and Kalidindi, who investigated 1200, 1800, and 2200 rpm drilling rates. They all received the same result—the higher the speed, the higher the temperature [
20,
24,
25]. As opposed to previously mentioned investigations, Sharawy et al. showed that the higher the speed, the lower the temperature. He obtained these research results using three different speeds: 1225, 1667, and 2500 rpm [
26]. The latest results of the research carried out by Kim et al. showed that the optimal rate that stimulates osteointegration and minimalizes thermal damage ranged from 1000 rpm to 1500 rpm [
12]. In our study, we used three rotation speeds: suboptimal (800 rpm), optimal (1200 rpm), and maximal (1500 rpm). The force applied during the creation of the implant site remains one of the factors that may influence the temperature while drilling. The average force put on the implant site during its preparation is 1.2 kg [
27]. Brisman et al. compared drilling at 1200 and 2400 rpm under loads of 1.2 and 2.4 kg. It turned out that drilling at the speed of 1800 rpm at the load of 1.2 kg generated an identical amount of heat as that of the 2400 rpm speed at the load of 2.4 kg. To obtain the same conditions while making all the implant sites, all of them were made by the same researcher with a synonymous force. Furthermore, an increase of one of the parameters (speed or load) caused an increased heat generation. On the other hand, increasing both parameters (speed and load) caused an unnoticeable rise in temperature and allowed for more effective implant site preparation [
28]. In our study, we also used pre-drilling as the method that allows for broadening of the drilling site and causing heat dissipation. During implant site preparation, the drill diameter was increased gradually from the smallest to the largest diameter. The method of pre-drilling was introduced in 1983 by Branemark and later confirmed by many researchers, but remains a rarely used procedure [
20,
29]. Our study showed that both speed and coolant used during drilling with constant force provoked significantly different changes in bone tissue. The bone tissue compression was visible after low speed (800 rpm), cooled drilling (
Figure 2), and the lack of coolant caused only moderate destruction of bone tissue and bone marrow (
Figure 3). Moderate speed drilling (1200 rpm) with coolant at room temperature microscopically showed no bone tissue compression (
Figure 4), but if the temperature of coolant was lower (3 °C), the same drilling method caused total destruction of the bone tissue and bone marrow (
Figure 5). Subsequently, high speed drilling (1500 rpm) did not give any intense compression of the bone tissue without coolant (
Figure 6). The use of coolant increased the destructive activity of the drill (total bone tissue and bone marrow destruction together with the presence of damaged trabecular architecture of bone), being the most traumatic (
Figure 7). These results proved that an increase in drilling speed and the level of bone tissue injury relation was interfered more by coolant existence than its temperature. Low speed drilling is the most predisposed to bone tissue compression and high speed drilling to bone tissue destruction. The microanatomical analysis of investigated material proved that the lowest bone tissue destruction zone was observed in moderate and high speed drilling (
Figure 8), but simultaneously, the lowest bone tissue compression caused moderate speed drilling (
Figure 9). Therefore we can conclude that the use of intermediate speed of drilling (1200 rpm) is the least traumatic, not only for the model, but also for further studies in vivo.
As well known, the existence of bone tissue within the drilling canal can be a facilitator in osteogenesis and consequently in implant integration with acceptor tissue. On the other hand, the same can increase removal of the cell debris process and decrease or prevent the healing process. In our model, both mentioned assumptions are impossible to verify per se. Further in vivo studies should be carried out to solve the hypothesis.
Moreover, we have to add that studies on the most important factors of successful implantation are not only narrowed to drilling and cooling methods. Modal analysis of implant stability brought new assumptions and point of view on osteointegration of various-shaped implants and thread pinches [
6]. Similarly, the biomechanics of implant integrated with the bone tissue in vivo can be a sufficient evaluation method for experimental implantology [
7].


 ,
, 











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}