
A Machine Learning Multilayer Meta-Model for Prediction of Postoperative Lung Function in Lung Cancer Patients



Abstract
:1. Introduction
- Risk Stratification: The preoperative identification of patients who may be at higher risk for postoperative complications allows the medical team to implement appropriate measures to minimize complications and optimize outcomes.
- Surgical Planning: Knowing the assessment of lung function helps the surgical team plan the surgical procedure effectively.
- Informed Consent: Obtaining informed consent is crucial, as patients need to be aware of the possible postoperative challenges and complications they may face based on their individual lung function.
- Predicting Postoperative Outcomes: This information helps patients prepare for the recovery process and facilitates appropriate postoperative care planning.
- Risk-Benefit Evaluation: For some patients with compromised lung function, the risks associated with surgery may outweigh the potential benefits. Postoperative lung function assessment helps to make informed decisions regarding the appropriateness of surgery as a treatment option for individual patients.
- Postoperative Care Planning: Knowing the postoperative lung function enables healthcare providers to plan for appropriate postoperative care. It helps determine the need for intensive care, ventilatory support, or physiotherapy during the recovery period.
2. Materials and Methods
Prediction of Postoperative FEV1 by Multilayer Regression Meta-Model
- Improved Predictive Performance: Stacked regression leverages the strengths of different base regression models by blending their predictions together. As a result, it can capture complex patterns and relationships in the data that individual models might miss, yielding a performance better than any single base regression models [12].
- Reduced Overfitting: Base regression models may suffer from overfitting if they are too complex or trained on limited data. Stacking helps reduce overfitting by blending the predictions from multiple models, effectively smoothing out any model-specific noise and generalizing better to unseen data.
- Model Diversity: To benefit from stacked regression, it is important to use diverse base regression models. Diversity can be achieved by training different models with varying algorithms, hyperparameters, or feature subsets. When combined, these diverse models contribute complementary information, leading to a more robust and reliable ensemble.
- Handling Nonlinearity: Stacked regression is particularly effective at handling nonlinearity in the data. The individual base regression models might be limited in their ability to capture nonlinear relationships, but by combining them, the stacked ensemble can approximate more complex patterns.
- Adaptability: Stacked regression can be applied to a wide range of regression problems, including those with high-dimensional data, outliers, and complex interactions among features. It can be adapted to different types of regression algorithms, such as linear regression, decision trees, support vector regression, or neural networks.
- Handling Model Biases: Different base regression models may have their biases and limitations. Stacked regression can mitigate these biases by considering a variety of perspectives, leading to a more well-rounded and reliable final prediction.
- Use L-1 folds for training the base regressions and make predictions on the remaining fold (so-called out-of-fold predictions).
- Store these predictions as meta-features for fold . These are the inputs for the meta-model in this specific fold.
| Algorithm 1. Training stacked regression with hyperparameter tuning and model performance evaluation and SHAP values calculation | ||||
| Input:, T—number of base models Output: | ||||
| into equal size subsets | ||||
| 1: | for do | |||
| Training set Testing set | ||||
| 1.1: | for do | |||
| ; number of distinct hyperparameters for-th base model; denotes the number of distinct hyperparameters for meta-model | ||||
| a: | -1 times only for samples in the training set | |||
| a.1: | Training validation set -2 subsets | |||
| a.2: | Testing validation set remaining subset | |||
| a.3: | on the Training validation set using hyperparameter | |||
| a.4: | on the Testing validation set | |||
| b: | , the average performance of over K-1 Testing validation sets | |||
| end for | ||||
| 1.2: | where | |||
| 1.3: | on the Training set using hyperparameter | |||
| 1.4: | obtained in step 1.3 on the Testing set | |||
| 1.5: | Calculate SHAP values on the Testing set | |||
| end for | ||||
| 2: | over Testing sets | |||
| 3: | ) | |||
| 4: | ) | |||
| Algorithm 2. with additional L fold cross validation | ||
| Input: Training validation set; hyperparameter , see a.3 in Algorithm 1 Output: with hyperparameter , trained on training validation set | ||
| Randomly partition Training validation set into L equal size subsets V | ||
| a.3.1: | for do | |
| Training set base model Test set base model | ||
| Training first level (base) models; T is the number of base models | ||
| a.3.1.1: | ; | |
| on Training set base model | ||
| Construct a training set for second level meta-model | ||
| a.3.1.2: | on Test set base model | |
| end for | ||
| a.3.2: | Training second level meta-model | |
| on collection | ||
| a.3.3: | Re-train first level base models | |
| for do | ||
| on Training_validation set | ||
| end for | ||
| a.3.4: | ||
3. Experimental Evaluation
3.1. Collected Data and Feature Engineering
3.2. Selection of Existing Methods for Comparison
3.3. Selection of Base and Meta-Models
- Selection of base regressors dominantly employing ensemble methods
- Selection of Random Forest as the final regressor
- Nested cross-validation (see Algorithm 2), ensuring the training of stacked regressor , in an additional L-fold cross-validation. It is well known that nested cross-validation minimizes the amount of information leakage between the training and validation sets [37].
- The proposed meta-model in the first postoperative day gave a gain of more than three times compared to any traditional method, both for MAPE and MAE criteria (average Gain_MAPE = 3.84, average Gain_MAE = 3.51). Among traditional prediction methods, Frost’s model performed best, compared to which the meta-model has Gain_MAPE = 3.43, i.e., Gain_MAE = 3.14.
- On the fourth and seventh postoperative days, the gain was over two times, more precisely an average Gain_MAPE = 2.39 for the 4th day and average Gain_MAPE = 2.21 for the 7th day, i.e., Gain_MAE = 2.18 for the 4th day and Gain_MAE = 2.10 for the 7th day. For these days, Frost’s method proved to be the best of the traditional methods, giving Gain_MAPE = 2.09 and Gain_MAPE = 1.91, for the 4th and 7th day, respectively. The corresponding values for Gain_MAE are 1.90 and 1.79, respectively.
- The superior advantage of the meta-model in the first postoperative day has the greatest clinical value since it can be used to project optimal recovery during the hospital stay, which usually ends after 7 days.
4. Model Interpretation
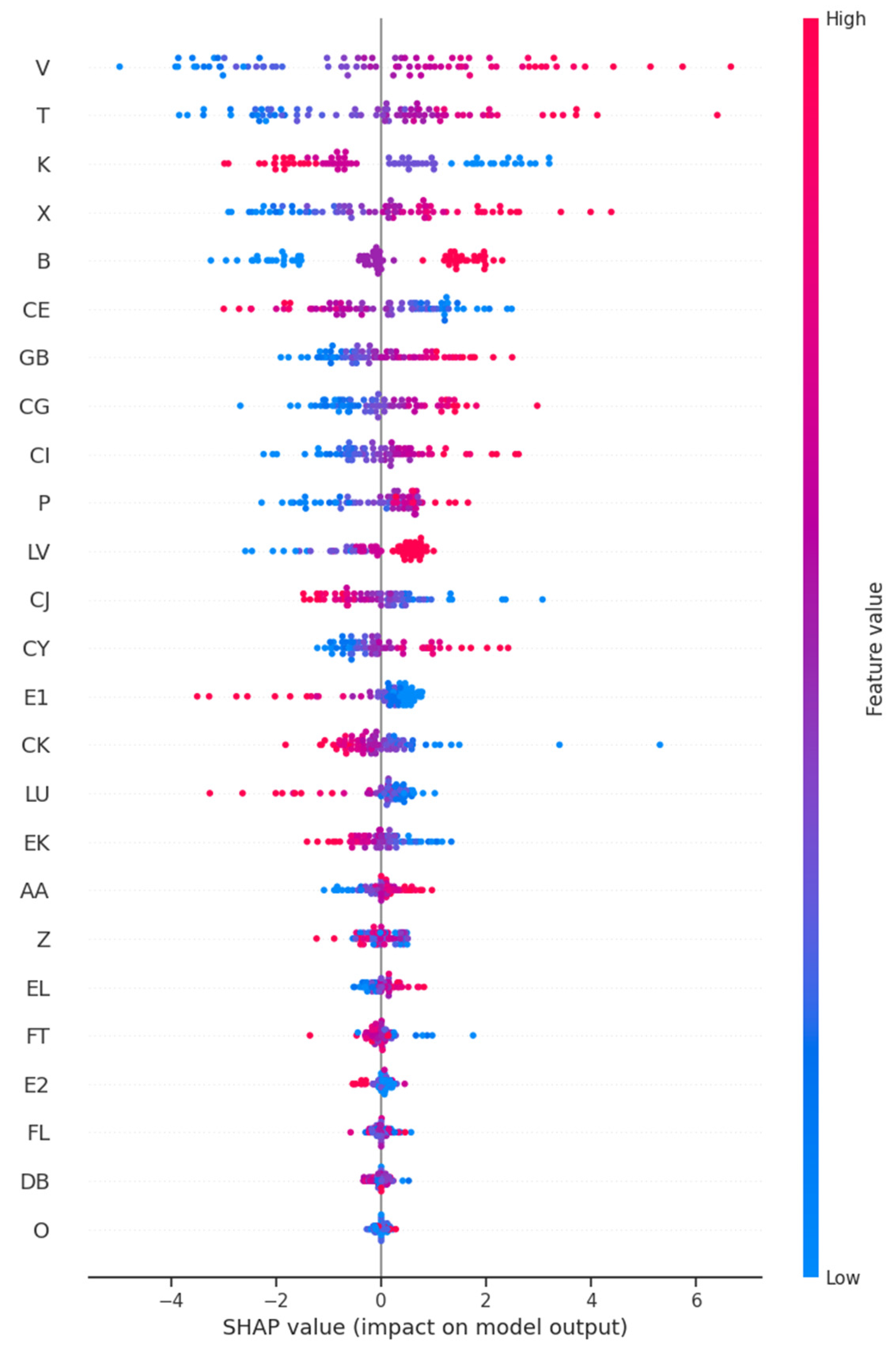
4.1. Global Model Interpretation
4.2. Local Interpretability
5. Conclusions
- It is possible for these purposes to design a multi-layer prognostic regression meta-model with sufficient accuracy even in the conditions of relatively small training sets with input features that are routinely collected in the preoperative period.
- The accuracy of the proposed model far exceeds the accuracy of traditional prognostic models.
- Global interpretation of the obtained meta-model using SHAP values showed several interesting new insights important for clinical practice, such as the role of IRM and BMI on the condition of patients on the first critical day after surgery.
- It was demonstrated how, based on local interpretation of SHAP values, a more accurate picture of postoperative risk factors personalized for each patient is obtained. This interpretation is performed preoperatively, which in our opinion can contribute to a significant improvement of the surgery procedure itself, as well as more successful postoperative rehabilitation of patients.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Howington, J.A.; Blum, M.G.; Chang, A.C.; Balekian, A.A.; Murthy, S.C. Treatment of stage I and II non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143, e278S–e313S. [Google Scholar] [CrossRef]
- Ettinger, S.D.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; DeCamp, M.; Dilling, T.J.; et al. Non–Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 497–530. [Google Scholar] [CrossRef]
- Steyerberg, E.W. Clinical Prediction Models; Springer: New York, NY, USA, 2009. [Google Scholar]
- Oswald, N.K.; Halle-Smith, J.; Mehdi, R.; Nightingale, P.; Naidu, B.; Turner, A.M. Predicting Postoperative Lung Function Following Lung Cancer Resection: A Systematic Review and Meta-analysis. EClinicalMedicine 2019, 15, 7–13. [Google Scholar] [CrossRef]
- Quanjer, P.H.; Tammeling, G.J.; Cotes, J.E.; Pedersen, O.F.; Peslin, R.; Yernault, J.C. Lung volumes and forced ventilatory flows. Report Working Party. Standardization of lung function tests. European Community for Steel and Coal. Official statement of the European Respiratory Society. Eur. Respir. J. Suppl. 1993, 16, 5–40. [Google Scholar] [CrossRef] [PubMed]
- Wyser, C.; Stulz, P.; Soler, M.; Tamm, M.; Muller-Brand, J.; Habicht, J.; Perruchou, A.P.; Bolliger, C.T. Prospective evaluation of an algorithm for the functional assessment of lung resection candidates. Am. J. Respir. Crit. Care Med. 1999, 159, 1450–1456. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.T.; Pan, H.B.; Chiang, A.A.; Hsu, H.K.; Chang, H.C.; Peng, N.J.; Lai, P.-H.; Liang, H.-L.; Yang, C.-F. Prediction of postoperative lung function in patients with lung cancer: Comparison of quantitative CT with perfusion scintigraphy. Am. J. Roentgenol. 2002, 178, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Cukic, V. Preoperative prediction of lung function in pneumonectomy by spirometry and lung perfusion scintigraphy. Acta Inf. Med. 2012, 20, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Varela, G.; Brunelli, A.; Rocco, G.; Marasco, R.; Jimenez, M.F.; Sciarra, V.; Aranda, J.L.; Gatani, T. Predicted versus observed FEV1 in the immediate postoperative period after pulmonary lobectomy. Eur. J. Cardiothorac. Surg. 2006, 30, 644–648. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, S.M.; Lee, S.I. A unified approach to interpreting model predictions. In Proceedings of the Advances in Neural Information Processing Systems, Long Beach, CA, USA, 4–9 December 2017; p. 30. [Google Scholar]
- Shapley, L.S. A Value for n-Person Games. In Contributions to the Theory of Games (AM-28); Kuhn, H.W., Tucker, A.W., Eds.; Princeton University Press: Princeton, NJ, USA, 2016; Volume 2, pp. 307–318. [Google Scholar]
- Vesovic, R.; Milosavljevic, M.; Punt, M.; Radomirovic, J.; Bascarevic, S.; Savic, M.; Milenkovic, V.; Popovic, M. The Role of the Diaphragm in Prediction of Respiratory Function in the Immediate Postoperative Period in Lung Cancer Patients Using a Machine Learning Model. World J. Surg. Oncol. 2023, 21, 393. [Google Scholar] [CrossRef]
- Wolpert, D.H. Stacked Generalization. Neural Netw. 1992, 5, 241–259. [Google Scholar] [CrossRef]
- Breiman, L. Stacked regressions. Mach. Learn. 1996, 24, 49–64. [Google Scholar] [CrossRef]
- Aggarwal, C.C. Data Classification Algorithms and Applications, 1st ed.; CRC Press: Boca, Raton, FL, USA, 2015. [Google Scholar]
- Stacking. StackingCVRegressor-mlxtend. Available online: https://rasbt.github.io/mlxtend/user_guide/regressor/StackingCVRegressor/ (accessed on 4 July 2023).
- Brunelli, A.; Charloux, A.; Bolliger, C.; Rocco, G.; Sculier, J.-P.; Varela, G.; Licker, M.; Ferguson, M.K.; Faivre-Finn, C.; Huber, R.M.; et al. ERS-ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur. Respir. J. 2009, 34, 17–41. [Google Scholar] [CrossRef]
- Juhl, B.; Frost, N. A comparison between measured and calculated changes in the lung function after operation for pulmonary cancer. Acta Anaesthesiol. Scand. Suppl. 1975, 57, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Nakahara, K.; Monden, Y.; Ohno, K.; Miyoshi, S.; Maeda, H.; Kawashima, Y. A method for predicting postoperative lung function and its relation to postoperative complications in patients with lung cancer. Ann. Thorac Surg. 1985, 39, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.-H. Ensemble Learning. In Encyclopedia of Biometrics; Li, S.Z., Jain, A.K., Eds.; Springer: Boston, MA, USA, 2015; pp. 411–416. [Google Scholar]
- Tibshirani, R. Regression Shrinkage and Selection via the lasso. J. R. Stat. Society. Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Geurts, P.; Ernst, D.; Wehenkel, L. Extremely randomized trees. Mach. Learn. 2006, 63, 3–42. [Google Scholar] [CrossRef]
- Braiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Guolin, K.; Qi, M.; Thomas, F.; Taifeng, W.; Wei, C.; Weidong, M.; Qiwei, Y.; Tie-Yan, L. LightGBM: A Highly Efficient Gradient Boosting Decision Tree. In Proceedings of the 31st International Conference on Neural Information Processing Systems, Long Beach, CA, USA, 4–9 December 2017; Curran Associates Inc.: New York, NY, USA, 2017; Volume 30, pp. 3149–3157. [Google Scholar]
- Drucker, B.; Kaufman, L.; Smola, J.; Vapnik, V. Support Vector Regression Machines. Adv. Neural Inf. Process. Syst. 1997, 28, 779–784. [Google Scholar]
- Solomatine, D.; Shrestha, D. AdaBoost.RT: A boosting algorithm for regression problems. IEEE Int. Conf. Neural Netw. Conf. Proc. 2004, 2, 1163–1168. [Google Scholar]
- Pedregosa, F.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; Vanderplas, J.; Passos, A.; Cournapeau, D. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Schmidhuber, J. Annotated History of Modern AI and Deep Learning. arXiv 2022, arXiv:2212.11279. [Google Scholar]
- Hoerl, E.; Kennard, W. Ridge Regression: Biased Estimation for Nonorthogonal Problems. Technometrics 1970, 12, 55–67. [Google Scholar] [CrossRef]
- Tianqi, C.; Carlos, G. XGBoost: A Scalable Tree Boosting System. arXiv 2016, arXiv:1603.02754. [Google Scholar]
- Tolles, J.; Meurer, J. Logistic Regression Relating Patient Characteristics to Outcomes. JAMA 2016, 316, 533–534. [Google Scholar] [CrossRef]
- Scikit-learn. Available online: https://scikit-learn.org/stable/ (accessed on 7 August 2023).
- LightGBM. Available online: https://lightgbm.readthedocs.io/en/stable/ (accessed on 5 February 2024).
- XGBoost. Available online: https://xgboost.readthedocs.io/en/stable/ (accessed on 5 February 2024).
- Grinsztajn, L.; Oyallon, E.; Varoquaux, G. Why do tree-based models still outperform deep learning on typical tabular data? arXiv 2022, arXiv:2207.08815. [Google Scholar]
- Shwartz-Ziv, R.; Armon, A. Tabular data: Deep learning is not all you need. Inf. Fusion 2022, 81, 84–90. [Google Scholar] [CrossRef]
- Scheffer, T. Error Estimation and Model Selection. Ph.D. Thesis, Technischen University at Berlin, School of Computer Science, Berlin, Germany, 1999. [Google Scholar]
- Nardini, C. Machine learning in oncology: A review. Ecancermedicalscience 2020, 14, 1065. [Google Scholar] [CrossRef]
- Lu, S.C.; Swisher, C.L.; Chung, C.; Jaffray, D.; Sidey-Gibbons, C. On the importance of interpretable machine learning predictions to inform clinical decision making in oncology. Front. Oncol. 2023, 13, 1129380. [Google Scholar] [CrossRef]
- Linardatos, P.; Papastefanopoulos, V.; Kotsiantis, S. Explainable AI: A review of machine learning interpretability methods. Entropy 2020, 23, 18. [Google Scholar] [CrossRef]
- Shap. Available online: https://shap.readthedocs.io/en/latest/ (accessed on 20 August 2023).












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Feature Label | Description | Type (Value Range) | Mean ± std |
|---|---|---|---|---|
| 1 | B | age | Integer [40, 78] | 60.24 ± 7.31 |
| 2 | E1 | Type of the operation on the right lung | Categorical | |
| 3 | E2 | Type of the operation on the left lung | Categorical | |
| 4 | K | BMI () | Float [17.06, 35.25] | 26.07 ± 1.84 |
| 5 | O | Type of respiratory function | Categorical | |
| 6 | P | COPD (Chronic Obstructive Pulmonary Disease) index | Float [0.9210, 2.2166] | 1.66 ± 0.22 |
| 7 | S | Preoperative FEV1—Preoperative forced expiratory volume in the first second (L) | Integer [1570, 4350] | 2656.96 ± 510.98 |
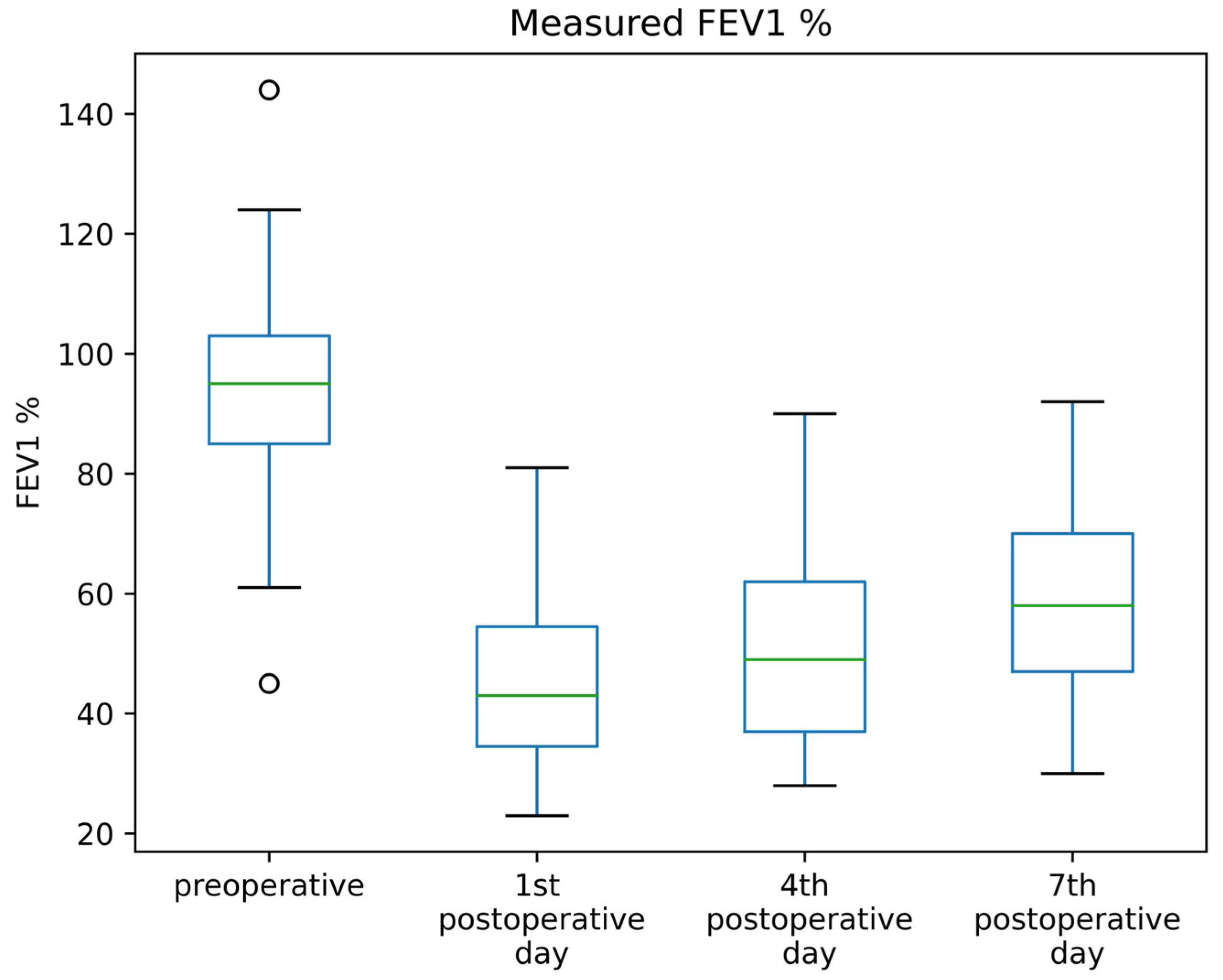
| 8 | T | Preoperative FEV1 %—Preoperative forced expiratory volume in the first second in [%] | Integer [45, 144] | 94.53 ± 15.63 |
| 9 | U | Preoperative VC—Preoperative vital capacity (L) | Integer [2040, 6780] | 3968.99 ± 872.34 |
| 10 | V | Preoperative VC %—Preoperative vital capacity in [%] | Integer [76, 148] | 109.23 ± 15.87 |
| 11 | W | Preoperative FVC—Preoperative forced vital capacity (L) | Integer [2010, 5960] | 3754.05 ± 755.19 |
| 12 | X | Preoperative FVC %—Preoperative forced vital capacity in [%] | Integer [73, 143] | 107.86 ± 15.04 |
| 13 | Y | Preoperative VCin—Preoperative vital capacity in inspiration (L) | Integer [2070, 6020] | 3822.78 ± 794.46 |
| 14 | Z | Preoperative VCin %—Preoperative vital capacity in inspiration in [%] | Integer [76, 143] | 105.51 ± 14.20 |
| 15 | AA | Preoperative FEV1 %/FVC | Float [47.10, 97.36] | 71.32 ± 9.41 |
| 16 | CD | TLC—Total lung capacity (L) | Integer [4100, 9650] | 6953.16 ± 1220.52 |
| 17 | CE | TLC %—Total lung capacity in [%] | Integer [90, 160] | 116.27 ± 14.41 |
| 18 | CF | RV—Residual volume (L) | Integer [770, 5670] | 2988.10 ± 805.40 |
| 19 | CG | RV %—Residual volume in [%] | Integer [45, 292] | 137.13 ± 34.03 |
| 20 | CH | FRC (ITGV)—Functional residual capacity (L) | Integer [2090, 6200] | 4227.72 ± 922.76 |
| 21 | CI | FRC (ITGV) %—Functional residual capacity in [%] | Integer [78, 223] | 133.67 ± 27.32 |
| 22 | CJ | RV/TLC (% predicted) | Integer [48, 178] | 109.49 ± 20.25 |
| 23 | CK | FRC (ITGV) % (% predicted) | Integer [39, 151] | 107.51 ± 18.53 |
| 24 | CY | Mobility of the right hemidiaphragm measured radiographically (cm) | Float [0.9, 4.3] | 4.16 ± 1.41 |
| 25 | DB | Mobility of the left hemidiaphragm measured radiographically (cm) | Float [0.4, 4.70] | 4.08 ± 1.39 |
| 26 | EK | Mobility of the right hemidiaphragm measured by ultrasound (mm) | Float [47.9, 94.2] | 68.25 ± 10.28 |
| 27 | EL | Mobility of the left hemidiaphragm measured by ultrasound (mm) | Float [36.5, 95.0] | 62.58 ± 11.10 |
| 28 | FK | Preoperative PImax (cmH20)—Preoperative maximum inspiratory pressure (cmH2O) | Integer [26, 154] | 83.38 ± 28.08 |
| 29 | FL | Preoperative PImax %—Preoperative maximum inspiratory pressure in [%] | Float [35.75, 201.60] | 109.63 ± 35.76 |
| 30 | FS | Preoperative PEmax (cmH20)—Preoperative maximal expiratory pressure | Integer [43, 155] | 102.22 ± 25.16 |
| 31 | FT | Preoperative PEmax %—Preoperative maximal expiratory pressure in [%] | Float [46.16, 129.84] | 92.19 ± 18.04 |
| 32 | GA | Preoperative Snip (cmH20)—Preoperative „sniff” inspiratory pressure (cmH20) | Integer [20, 139] | 86.53 ± 25.09 |
| 33 | GB | Preoperative Snip %—Preoperative „sniff” inspiratory pressure in [%] | Float [24.61, 143.90] | 91.83 ± 23.26 |
| 34 | LU | The number of functional segments removed by the operation | Integer [1, 9] | 3.41 ± 2.02 |
| 35 | LV | The number of total functional segments in the lungs | Integer [14, 18] | 17.23 ± 1.07 |
| 1st Postoperative Day | 4th Postoperative Day | 7th Postoperative Day | |
|---|---|---|---|
| mean | 44.68 | 50.95 | 58.01 |
| std | 14.07 | 15.80 | 14.78 |
| No. | Model | MAPE | MAE |
|---|---|---|---|
| 1 | Lasso | 19.57 | 9.05 |
| 2 | Extra Tree | 20.27 | 9.55 |
| 3 | Random Forest | 20.44 | 9.66 |
| 4 | LightGBM | 20.96 | 9.80 |
| 5 | SVM Linear | 21.11 | 9.83 |
| 6 | AdaBoost | 20.90 | 9.93 |
| 7 | KNN | 22.46 | 10.23 |
| 8 | MLP2 | 22.95 | 10.66 |
| 9 | Ridge Regression | 23.73 | 10.78 |
| 10 | XGBoost | 22.72 | 11.10 |
| 11 | SVM.RBF | 23.82 | 11.39 |
| 12 | LogisticReg | 23.89 | 11.73 |
| 13 | MLP1 | 25.33 | 11.84 |
| 14 | Meta-model | 18.64 | 8.93 |
| 1st Day after Surgery | 4th Day after Surgery | 7th Day after Surgery | ||||
|---|---|---|---|---|---|---|
| MAPE | Gain_MAPE | MAPE | Gain_MAPE | MAPE | Gain_MAPE | |
| Our meta-model | 19.36 ± 1.11 | 22.16 ± 2.79 | 14.40 ± 1.96 | |||
| Functional segments | 80.32 ± 6.00 | 4.15 | 58.14 ± 6.20 | 2.62 | 35.64 ± 2.81 | 2.47 |
| Juhl-Frost | 66.43 ± 4.20 | 3.43 | 46.42 ± 4.72 | 2.09 | 27.47 ± 3.60 | 1.91 |
| Nakahara | 76.28 ± 5.46 | 3.94 | 54.59 ± 5.33 | 2.46 | 32.58 ± 3.06 | 2.62 |
| Average gain | 3.84 | 2.39 | 2.21 | |||
| 1st Day after Surgery | 4th Day after Surgery | 7th Day after Surgery | ||||
| MAE | Gain_MAE | MAE | Gain_MAE | MAE | Gain_MAE | |
| Our meta-model | 8.24 ± 0.93 | 10.56 ± 0.87 | 7.98 ± 1.51 | |||
| Functional segments | 31.30 ± 2.44 | 3.80 | 25.40 ± 2.51 | 2.41 | 18.86 ± 1.01 | 2.36 |
| Juhl-Frost | 25.87 ± 1.79 | 3.14 | 20.03 ± 2.32 | 1.90 | 14.32 ± 1.64 | 1.79 |
| Nakahara | 29.57 ± 2.06 | 3.59 | 23.65 ± 2.40 | 2.34 | 17.11 ± 1.25 | 2.14 |
| Average gain | 3.51 | 2.18 | 2.10 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vešović, R.; Milosavljević, M.; Punt, M.; Radomirović, J. A Machine Learning Multilayer Meta-Model for Prediction of Postoperative Lung Function in Lung Cancer Patients. Appl. Sci. 2024, 14, 1566. https://doi.org/10.3390/app14041566
Vešović R, Milosavljević M, Punt M, Radomirović J. A Machine Learning Multilayer Meta-Model for Prediction of Postoperative Lung Function in Lung Cancer Patients. Applied Sciences. 2024; 14(4):1566. https://doi.org/10.3390/app14041566
Chicago/Turabian StyleVešović, Radomir, Milan Milosavljević, Marija Punt, and Jelica Radomirović. 2024. "A Machine Learning Multilayer Meta-Model for Prediction of Postoperative Lung Function in Lung Cancer Patients" Applied Sciences 14, no. 4: 1566. https://doi.org/10.3390/app14041566