1. Introduction
The assessment of daily energy expenditure is essential in clinical nutrition to elaborate diets and nutritional treatments according to the patients’ needs. Resting energy expenditure (REE) represents 60–80% of the daily energy expenditure in most patients [
1], and should be determined for an accurate dietetic prescription. In general, REE is measured by indirect calorimetry (IC), which requires sophisticated equipment and time-consuming procedures. Alternatively, REE may be predicted from anthropometric and/or body composition data using prediction equations [
2,
3]. The use of prediction equations entails associated errors due to the population-specificity of the equations and the procedures used in their development and validation [
2,
4,
5]. Some of the most used equations in the clinical setting, as the Harris and Benedict 1984 [
6] and FAO/WHO/UNU [
7], have been shown to overestimate REE in overweight and obese subjects, in contrast to the Mifflin et al. equation [
8] which is more accurate in subjects with overweight or obesity [
9,
10,
11].
Several factors may influence REE [
12], including sex [
13], race [
14], age [
15], body composition [
16], sleep duration [
14], energy balance [
16], food composition [
17], physical activity [
18], circadian rhythms [
19], and obesity-related comorbidities [
11,
20,
21,
22]. For these reasons, some equations specific to overweight and obese patients have been proposed. To avoid the potential influence of comorbidities in REE-predictive equations, Lazzer et al. [
23] developed specific equations for obese subjects after excluding the patients with overt metabolic and/or endocrine diseases (e.g., diabetes, hypothyroidism, hypertension) and those who were taking regular medications known to influence REE. Since the main determinant of REE is fat-free mass (FFM) [
16,
22,
24,
25], several equations have been proposed to account for differences in FFM [
8,
22,
23,
26,
27,
28,
29,
30,
31,
32,
33]. Nevertheless, REE equations based on body composition data do not seem to outperform those based exclusively on anthropometric variables [
23,
30].
Despite often being overlooked, environmental conditions may also influence REE [
5,
34]. For example, it has been reported that the body mass index (BMI) is more elevated in humans residing in higher environmental temperatures [
35]. Henry and Rees, using published REE data obtained in tropical populations observed that the WHO/FAO/UNU equation overestimates REE by 8–11.5% in people living in tropical regions [
5]. Nevertheless, the Henry and Rees’s equation was developed using data from different studies, obtained mostly from normal-weight people of varied ethnicities, and it is uncertain whether this equation can be applied to an overweight and moderately obese Caucasian population [
5]. Moreover, the Henry and Rees’s equation has not been validated.
Gran Canaria is located in a subtropical region with mean monthly temperatures between 18 and 24 °C in the coldest and warmest months, respectively. The prevalence of overweight (40.0%) and obesity (20.1%) in Canary Islands [
36,
37] is high compared to other European regions and countries [
38]. Although environmental conditions may be counteracted in part by behavioral factors (amount of clothing, air-conditioning, reduced physical activity, etc.), it has been suggested that increased time spent in the thermal comfort zone may reduce REE contributing to the high prevalence of obesity in subtropical regions [
34,
39]. If this was the case, overweight and obese people living in Gran Canaria should have an REE falling below that predicted by most equations. In fact, it remains unknown which is the best REE-predictive equation to use in overweight and obese adults living in a temperate weather all year round.
Therefore, the aim of this investigation was double. Firstly, to determine whether the measured REE in overweight and obese patients living in a temperate climate all year round falls below the predicted values given by most equations, particularly by equations specifically developed for overweight and obese patients. Secondly, to ascertain which is the most accurate equation in overweight and obese participants living in a temperate climate.
3. Results
The descriptive characteristics of the study population are reported in
Table 1 and
Table 2. The male and female group had similar age and BMI, while women had a greater percentage of body fat than men. Daily physical activity was similar in both sexes. Predicted REE by equations based on anthropometric and body composition variables (
Table S1) was compared with measured REE.
The results obtained with equations based on anthropometric variables combined or not with age and sex are reported for the overall study population (
Table 3), as well as for men (
Table 4) and women (
Table 5) separately. The results obtained with REE equations based on body composition data are reported in
Table 6.
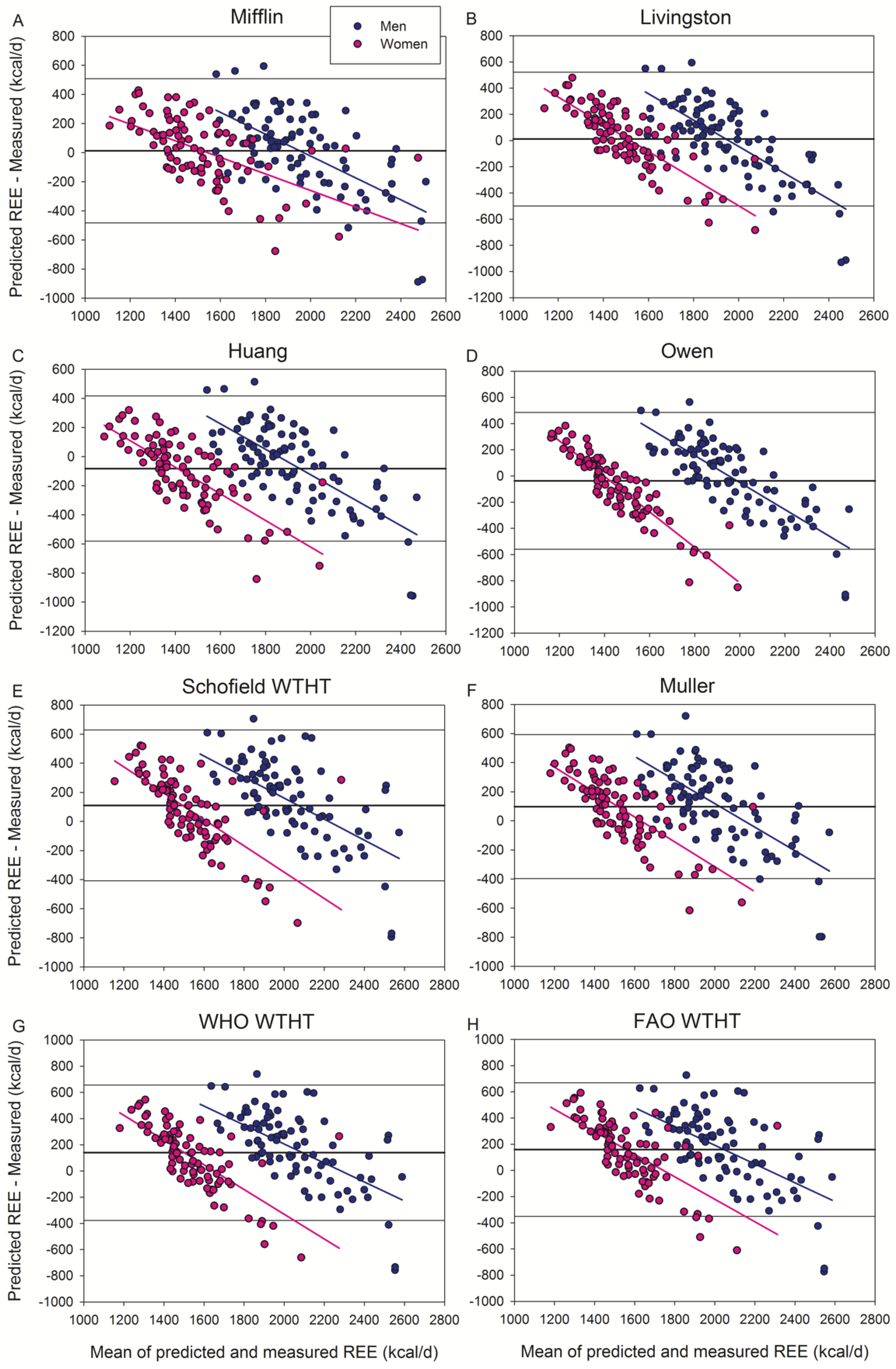
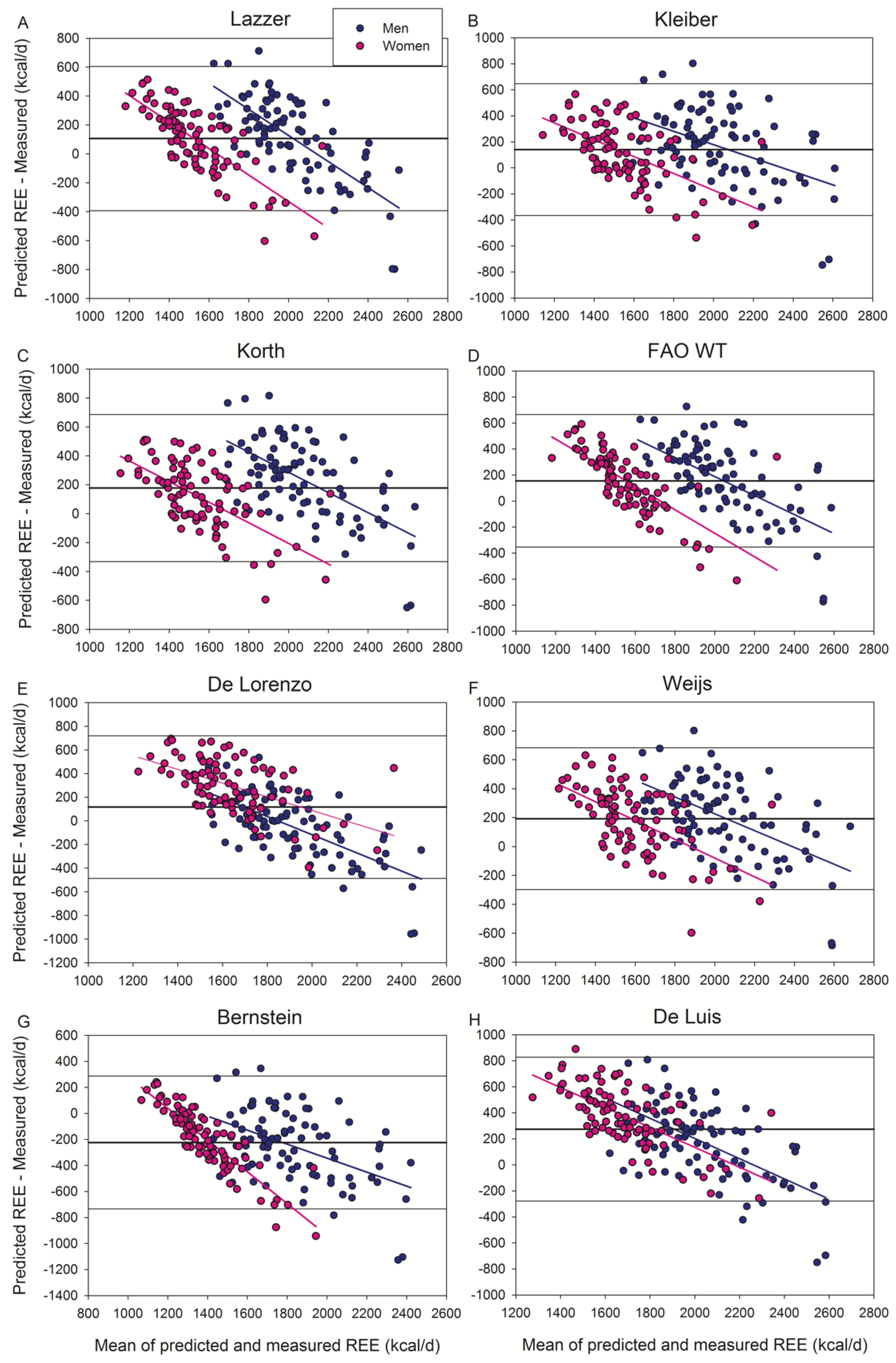
Bland and Altman’s plots are presented in
Figure 1,
Figure 2 and
Figure 3, as well as in
Figures S1–S3. When all subjects were analyzed conjointly, the equations of Mifflin et al. and Livingston et al. gave the best scores of accurate predictions (51% of patients) with a non-significant bias of 0.6–0.7% (
Figure 1A,B).
Of the seventeen additional equations tested here, the Huang et al. (
Figure 1C) and Bernstein et al. (
Figure 2G) equations underestimated (4.8% and 13.0%, respectively), while the other equations overestimated (3.4–15.9%) REE. The equations that did not include obese subjects overestimated REE (
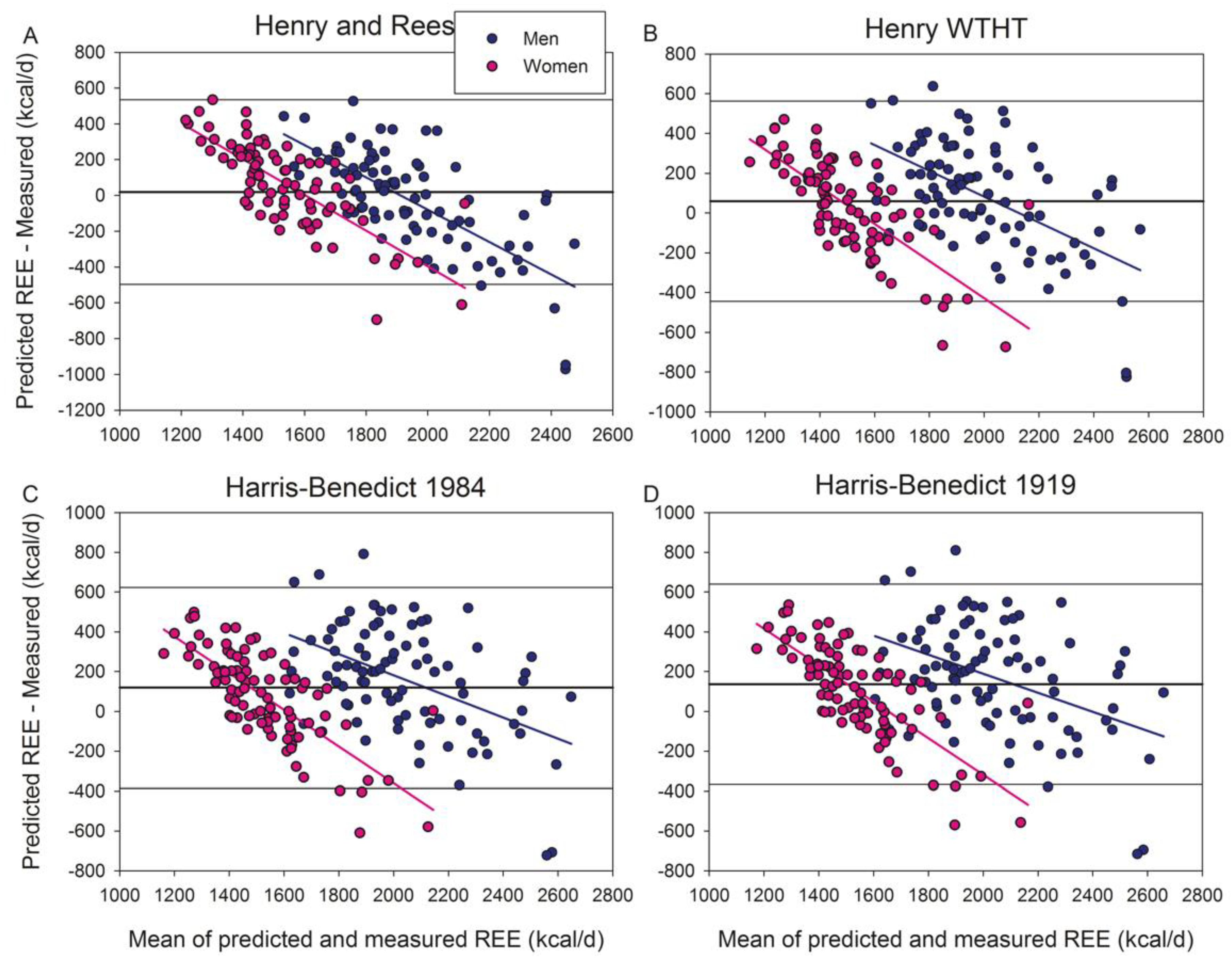
Figure 3), except the Henry and Rees equation developed for tropical inhabitants which had a non-significant bias (+1.1%) (
Figure 3A).
In men (
Table 3), the equation of Henry and Rees (developed for tropical populations) was accurate (non-significant bias of −1.1%) and was the equation having the highest proportion of accurate predictions (53.5%). The equations of Livingston, Owen and Mifflin were also accurate (with non-statistically significant biases) and able to accurately predict REE in at least 50% of subjects. Non-significant differences were observed in mean absolute percentage errors between the equations of Henry and Rees, Livingston, Owen, and Mifflin in men. However, the CCC was slightly worse for the Henry and Rees equation than for the Mifflin et al. equation. The Mifflin et al. equation had a non-significant 0.5% bias, being accurate in 50% of men. The rest of the equations were less accurate with a predominance of equations overestimating the measured REE (14/2, equations over/underestimating).
The equations of Henry and Rees, De Lorenzo, De Luis and Lazzer (body composition) 2010 were more accurate in men than women, while the rest of the equations were similarly accurate in both sexes (
Table 4 and
Table 5). The Mifflin equation gave the most accurate REE predictions in women, with a non-significant 1.1% bias and more than 52% accurate predictions. The Mifflin equation was followed by Livingston and Henry WTHT equation, which also had a small (1.3–2.2%) non-significant bias and scored 48.8% accurate predictions. The Henry and Rees equation for tropical populations overestimated REE in women by 4.7%. The other equations had a bias above 5%, with a predominance of equations overestimating the measured REE (14/3, equations over/underestimating). The FAO WT, Weijs, De Lorenzo, and De Luis equations overestimated REE in women by more than 10%.
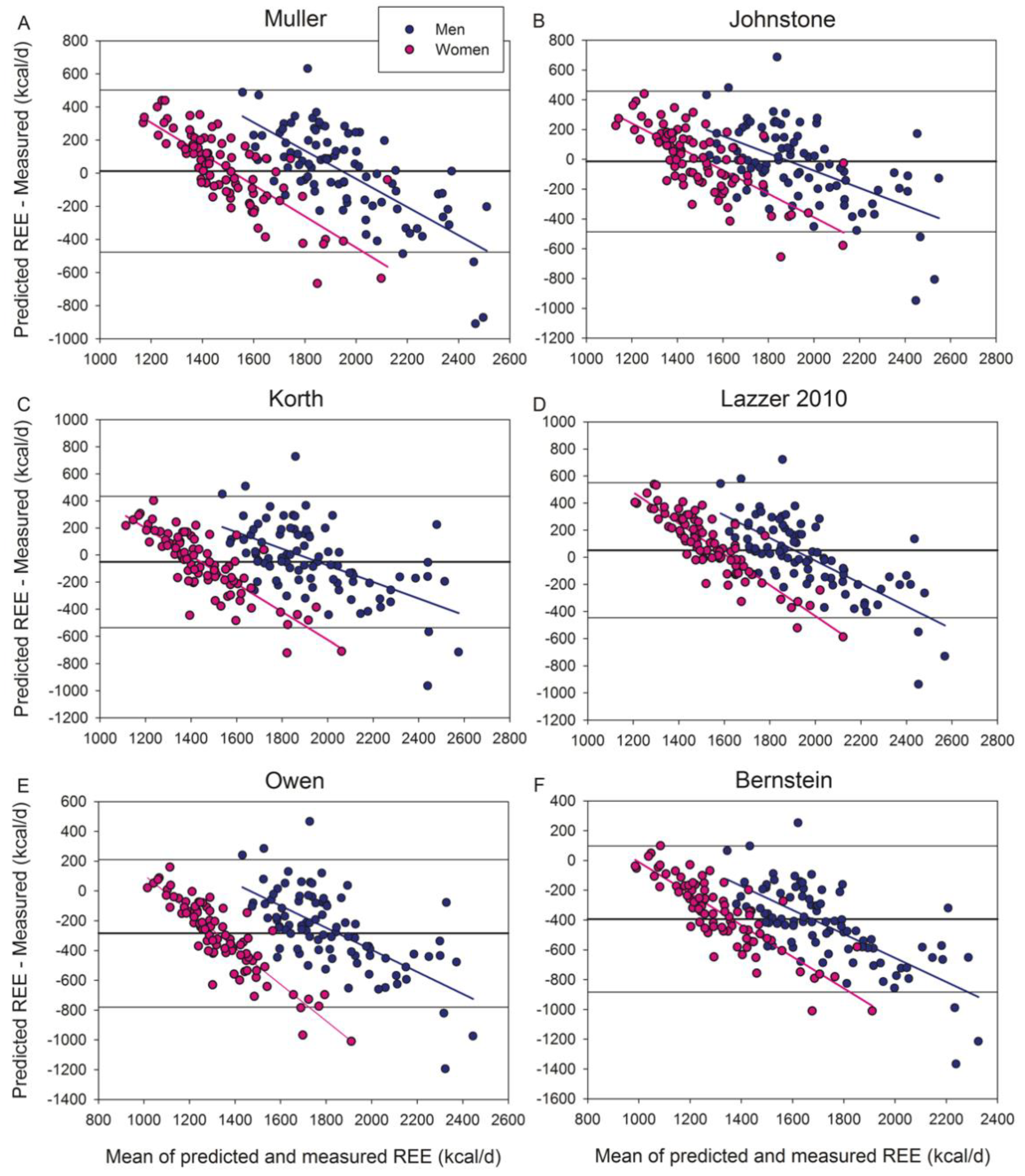
Of the equations based on body composition variables (
Table 6) (
Figure 4 and
Figure 4S), Muller, Lazzer 2010, Johnstone, and Korth equations scored accurate predictions in at least 55% of men, while only Muller’s reached 50% accurate predictions in women. The body composition-based equations of Muller, Korth, Owen, and Bernstein had a lower MAPE than their respective anthropometry-based equations, both in men and women. In men, Lazzer 2010 body composition equation had a lower MAPE than its anthropometry-based equation (
Table 6) and was as accurate as the Mifflin equation in our male population. Of the body composition-based equations, Johnstone’s had a significantly lower MAPE compared with Livingston, Owen, and Mifflin, in men. The MAPEs of Johnstone and Henry and Rees equations were similar. None of the body composition-based equations outperformed the Mifflin equation in women.
Multiple regression analysis showed that REE can be predicted in our population with equation 1 or 2, as follows
(R = 0.76, R
2 = 0.58, SEE = 252.7,
p < 0.001); age, BMI and height were excluded from the model (sex: 0 = women; 1 = men).
(R = 0.79, R2 = 0.62, SEE = 241.4, p < 0.001); age and sex excluded from the model (sex: 0 = women; 1 = men).
4. Discussion
In agreement with our hypothesis, most equations overpredicted REE in overweight and obese humans living in a temperate climate all year round, including the equations specifically developed for overweight and obese patients. This study also shows that the most accurate equations to predict REE in overweight and obese Caucasian patients living in an all-year-round temperate climate are the Henry and Rees, Johnstone, Mifflin, Owen and Livingston equations in men, and the Mifflin equation in women. Our study also indicates that the Johnstone equation outperforms the rest of the equations based on body composition variables in men. Interestingly, none of the body composition-based equations outperformed the Mifflin equation in women. Out of the most used equations in the clinical setting, i.e., the Harris and Benedict [
46], the Owen et al. [
31,
47], the WHO/FAO/UNU [
48], and the Mifflin et al. [
2,
8], in women, only the Mifflin, and in men, the Henry and Rees, Owen, and the Livingston equations had no significant bias and scored accurate predictions in approximately 50% of subjects in our population. This close-to-50% accuracy is what can be expected from the best predictive equations in overweight and obese patients [
30]. Given the extended use of Mifflin’s equation and the fact that none of the anthropometry-based equations were more accurate than the Mifflin equation in men nor women in overweight and moderately obese patients living in a temperate climate, the Mifflin equation emerges as the equation of choice for similar populations. Nevertheless, given the large inter-individual variability in REE, whenever possible, REE must be measured rather than estimated from predictive equations.
Reduced thermogenesis in overweight and obese humans living in a temperate climate may contribute to obesity [
49,
50]. Cold exposure increases REE in humans by diverse mechanisms, including activation of brown adipose tissue [
51], increased muscle thermogenesis [
52], and fat cell thermogenesis [
53]. Chronic activation of these thermogenic processes by daily cold exposure during several days is required to induce a sustained increase in REE in humans and cold acclimatization [
54]. Since in the Canary Islands cold days are exceptional and rarely last for more than two weeks, the predominantly temperate and warm weather may result in a sustained attenuation of REE, being this the most plausible reason why the majority of REE predictive equations overestimate the measured REE in our overweight and obese population. Nevertheless, it should also be taken into account that, in men, several equations, not specifically developed for patients living in tropical regions, were predicting REE with similar or slightly better accuracy than the equations developed including tropical or subtropical populations. The latter would suggest that part of the smaller REE observed in our population may just reflect differences in body composition.
The Livingston et al. [
55] equation performed well in our male and female population, although the CCC was slightly below that of the Mifflin et al. equation [
8]. The excellent performance of the Livingston and Mifflin equations may be in part due to the use of metabolic carts from SensorMedics in these two studies, as in the present investigation. Moreover, in the case of the Livingston equation, almost half of the subjects used in developing their predictive equation were residing in Dallas area, also a region with temperate/warm weather most of the year. Despite the inherent variability that may affect the equation proposed by Henry and Rees for tropical populations, due to the use of data obtained in different populations, with different habits (diet, physical activity, sleep patterns, etc.) and body composition, this equation achieved a good agreement with our measured REE, particularly in men.
Lazzer et al. developed equations specific for severely obese patients, after excluding the patients with comorbidities that could influence REE [
23]. Lazzer 2010 equations were obtained using the same type of metabolic cart (Vmax N29, SensorMedics) as in the present study. Moreover, Canary Island ancestry is somewhat similar to that of the North of Italy, making this equation and population ideal for comparison with our population living in a temperate climate. Nevertheless, Lazzer 2010 anthropometry-based equations overestimated REE in men (+6.0%) and women (+6.3%) when applied to our population. Although some comorbidities and drugs have been associated with increased REE in obese patients [
11], our main results were not altered when the subjects on medical treatment were excluded from the analysis. This was somehow expected since both diabetes [
22], and hypertension [
20,
21] have been associated with increased REE and could not explain the decreased REE of our population. Moreover, none of our diabetic patients were on insulin therapy.
Previous studies have reported lower accuracy [
8,
22,
26,
27,
28], or no clear advantage of REE equations derived using body composition data [
23,
29,
30,
31,
32,
33] when compared with equations solely based on anthropometric measurements. This has been attributed to the variability and diversity of procedures applied to measure FFM and FM (bioelectrical impedance, anthropometry, hydrodensitometry, air-displacement plethysmography, whole-body water assessment with deuterium, total-body potassium, and dual-energy x-ray absorptiometry). Here, DXA was used to determine FFM and FM; a procedure also applied by Johnstone et al. [
56] and Korth et al. [
57]. This may be one of the reasons why Johnstone’s and Korth’s equations predicted the REE of our men with acceptable accuracy. However, our results also indicate that the equations developed using bioelectrical impedance [
23,
29] are as accurate as Johnstone’s in our population. In contrast, the body composition-based equations of Owen and Bernstein, both based on hydrodensitometry [
31,
33,
47], underestimated the measured REE markedly. In agreement with Marra et al. [
30], our findings indicate that obese-specific equations do not necessarily predict the REE of an obese population more accurately than those obtained from normal-weight subjects.
The fact that our population may have slightly lower REE than others may explain why three of the four equations developed for non-obese subjects were also accurate in our subjects. The reason why the Henry and Rees equation performed worse in our female population might originate from the small number of women used to develop the equation (98 women for the 30–60 age range) and the fact that we studied women with overweight and obesity.
The Harris-Benedict equation, being the oldest in use, has been subjected to more validation studies than any other equation [
9]. In general, these validation studies have shown a 5–10% overestimation of REE [
8,
29,
31,
47,
58,
59,
60,
61,
62]. In agreement, we have also observed that the Harris and Benedict equations (1919 and the 1984 modifications) overestimated REE by 5–9% in our overweight/obese population. This overestimation could be even greater in severely obese patients [
2].
Our results aligned well with the systematic review by Frankenfield et al. [
2] and the recent study by Cancello et al. [
11], the latter including 4247 morbidly obese patients. Both studies [
2,
11] concluded that the best equation to estimate the REE of obese patients is the Mifflin equation, even when comorbidities are present, although Mifflin’s equation may lose accuracy in patients with hypertension [
11]. In our population, 44 patients were hypertense, but they were on treatment, which may have counteracted some of the hypertension-related mechanisms increasing REE, for example, increased sympathetic activity [
20,
21]. In any case, the accuracy of the Mifflin equation was similar in our overweight/obese subjects to that reported for other populations with no or several comorbidities [
11].
Even though the Mifflin et al. equation was slightly less accurate in our male population, when using the concordance correlation coefficient as a criterion, the Mifflin et al. equation achieved rather good scores both in men and women, compared to the rest of the equations tested here and had no bias. Moreover, the Mifflin equation had the lowest MAPE in men, and one of the smallest in women. The latter combined with the extended use of the Mifflin et al. equation are strong arguments for defending its use in our population, as well as in similar patients with overweight or moderate obesity (up to BMI close to 40 kg m
−2) [
30,
63,
64,
65], and especially in patients from regions with a temperate climate. Besides, recent reports have shown that the Mifflin equation is robust and may even improve its accuracy in severely obese patients with comorbidities [
11].
This study has several limitations. We enrolled a heterogeneous group of overweight and obese patients without excluding subjects due to comorbidities, which in one side may improve the transferability to the general obese population but on the other may have resulted in greater variability and imprecision [
11]. This was necessary due to the numerous measurements performed which included assessment of body composition by DXA, aerobic fitness (exercise test), oral glucose tolerance tests, and assessment of daily physical activity. The final sample was similar in size to that of Johnstone et al. [
32] who also determined body composition by DXA, and developed an equation that performed very well in our male population. We used two different metabolic carts during the study, but both were verified with a butane combustion test and cross-calibrated, as previously reported [
43,
66]. The observations made in this investigation are specific to our Caucasian populations and cannot be generalized to other ethnic groups. Despite these limitations, the standard error of the estimate of equation 1 and 2 was similar to that reported for the equations developed for overweight and obese populations [
23,
26,
65].

 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}