4. Discussion
In the current study, EUS-RV performed in accordance with our method succeeded in all patients. The first attempted methods allowed successful biliary cannulation in all except for one (6.3%) patient with failed biliary puncture, while there were no cases with failed guidewire manipulation. Adverse events occurred in 6.3% (one of 16) of the patients with pancreatitis, whereas any adverse events related to the bile leak did not occur. The hitch-and-ride method could not show a definite predominance over the other methods in the time and success rate of biliary cannulation.
Since the biliary puncture requires a short time, has a small risk of bile leak even after failure, and is the first step of the EUS-RV procedure, changing the approach route after failed biliary puncture is not so serious. Alternately, the guidewire manipulation is the most challenging and time-consuming step [
14] and has a risk of bile leak when biliary drainage fails. Then, our method was made to focus on guidewire manipulation on the basis of a previously proposed algorithm reported by Iwashita et al. [
3], in which the DEHBD/D2 route was the first-line approach, followed by both the PEHBD/D1 and LIHBD/S routes as the second-line approaches. In our method, we modified their algorithm in some ways. First, the RHIBD/D1 route was added to improve the adaptability of EUS-RV for various biliary disorders. Second, the PEHBD/D1 route was prioritized over IHBD routes because of the shorter distance between the puncture site and the ampulla and the less necessity of passing through the strictures. Third, a 22 gauge needle for an inadequately dilated bile duct in the DEHBD/D2 route was included. Fourth, insertion of a catheter was proposed in cases with poor guidewire manipulation.
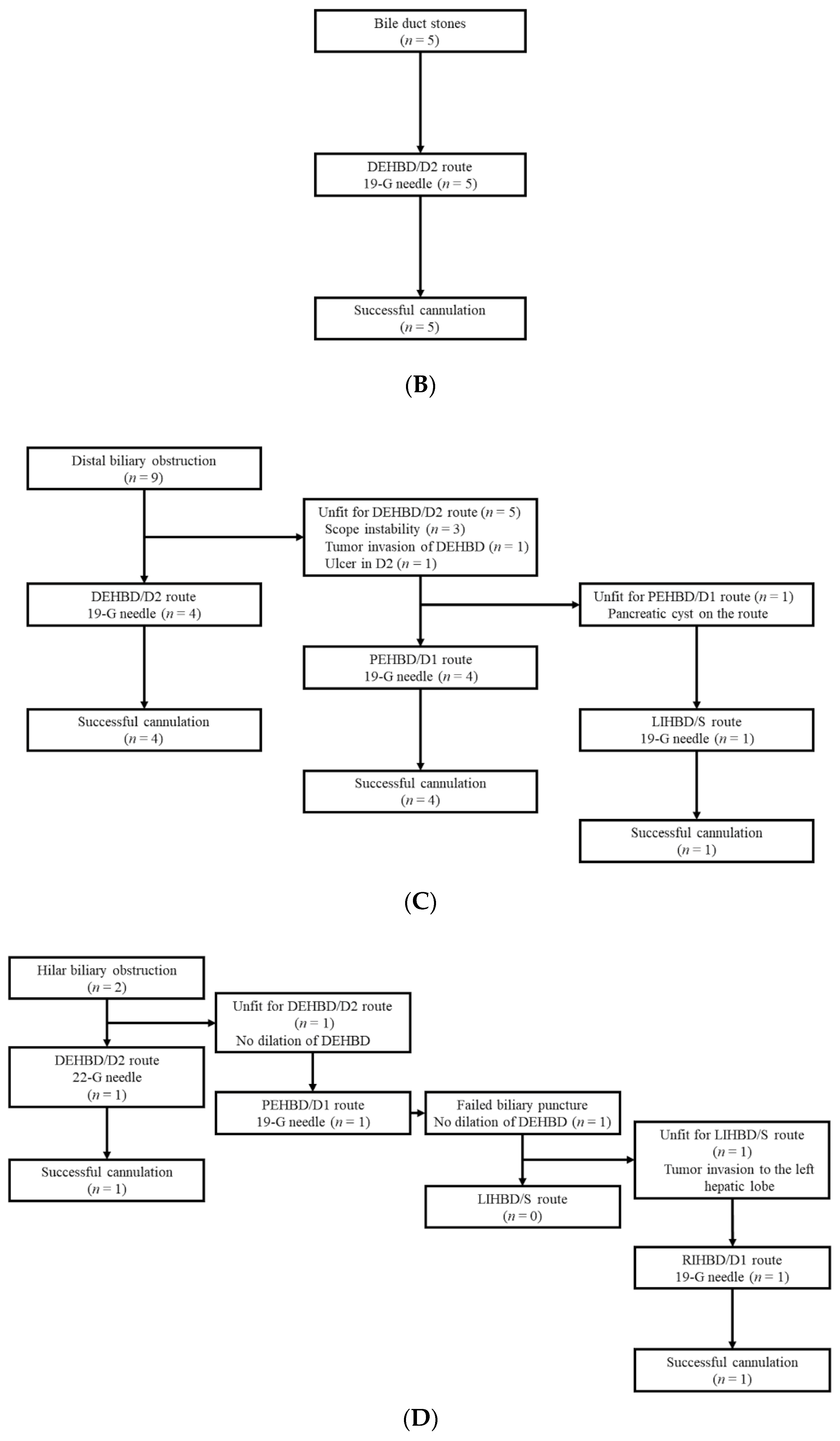
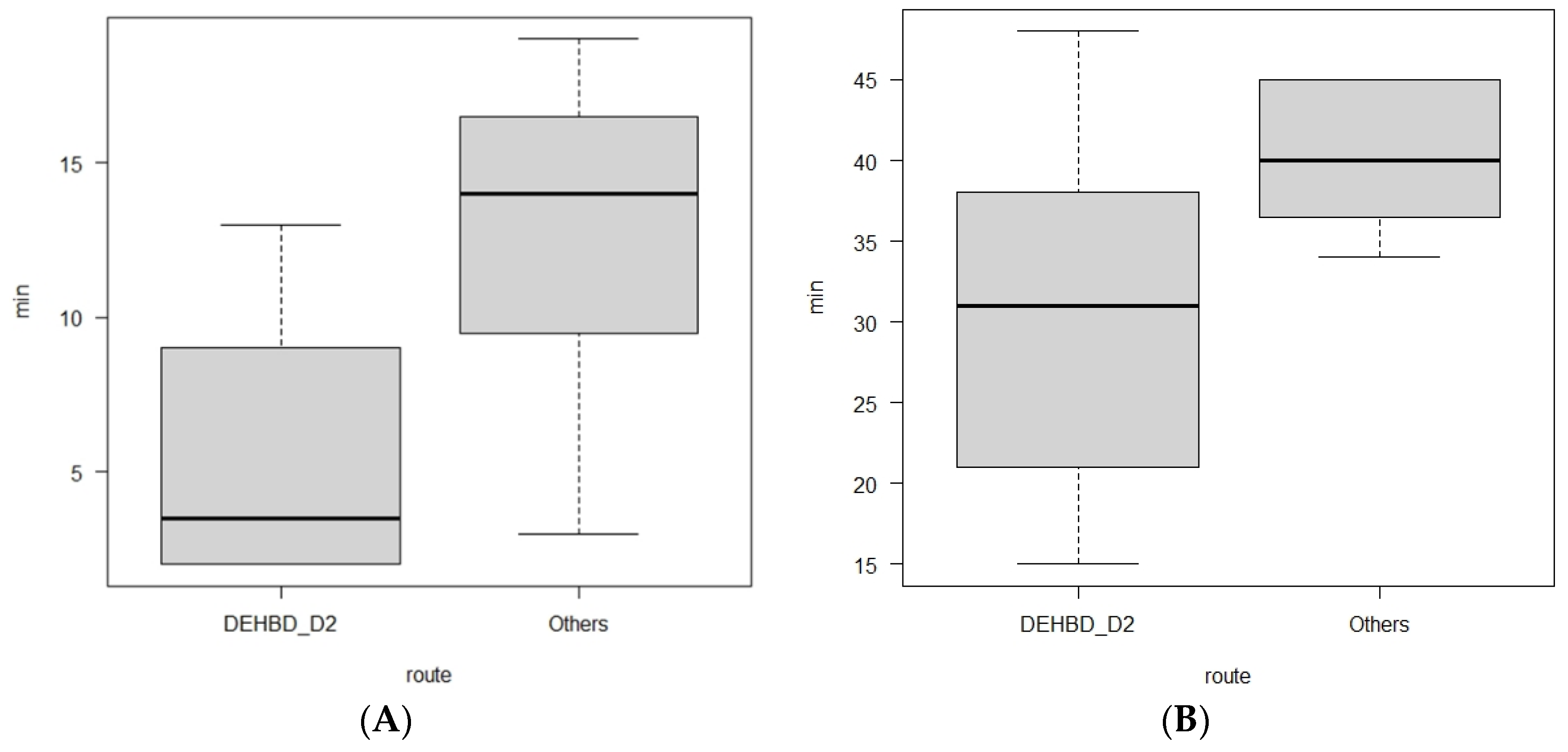
Consequently, the DEHBD/D2 route was applied to 62.5% (10/16) of the patients and allowed successful cannulation in all the patients, requiring a shorter time for guidewire manipulation than the other routes. In addition, the whole time for EUS-RV with the DEHB/D2 route was also shorter than for the other routes, although there was no significant difference, possibly due to other factors, including the cannulation time. Although multiple attempts at the biliary puncture were needed in 40% (four of 10) of patients due to a thin DEHBD, there were no significant differences in the puncture number between approach routes. The PEHBD/D1 route was applied to 31.3% (five of 16) of the patients, and the success rate was 80% (4/5). The cause of unsuccess was failed biliary puncture due to a thin PEHBD (3 mm). The PEHBD lacked fixing by surrounding solid organs, unlike the IHBD or DEHBD, and needle handling in the long scope position was poor so that the puncture of the PEHBD might have been more difficult than that of the IHBD or DEHBD, when enough dilation of the bile duct was absent. On the contrary, the non-dilated DEHBD (2 mm) in a hilar biliary obstruction case was successfully punctured in one attempt, although a 22 gauge needle was used, possibly owing to fixing by the pancreas and favorable needle handling in the short scope position. We did not use 22 gauge needles except for in DEHBD/D2 route because the manipulation of a 0.018 inch guidewire was worse than that of a 0.025 inch guidewire. Indeed, Martínez et al. reported that the success rate of the manipulation of a 0.018 inch guidewire through a 22 gauge needle was only 80.6% (25 of 31 cases) [
19]. Some authors mentioned a method for cases with thin bile ducts in which the bile duct was punctured with a 22 gauge needle and a contrast was injected to dilate the bile duct, followed by re-puncture with a 19 gauge needle [
4,
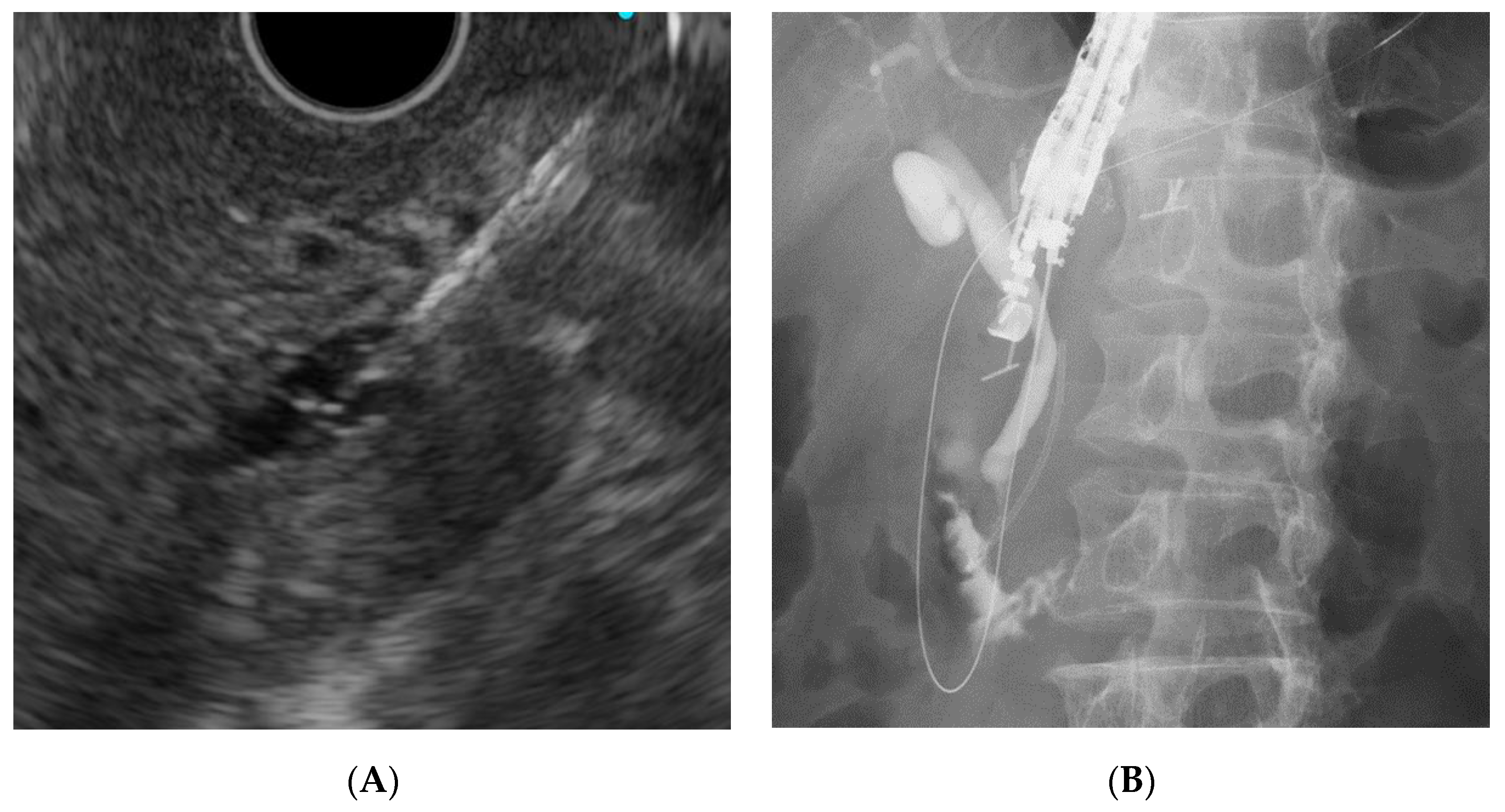
20]. However, we did not use this method because of the additional cost of the needle and the potential risk of a bile leak. Of four patients with successful punctures in the PEHBD/D1 route, the guidewire placement was successful in all patients, although a longer time was required than for the DEHBD/D2 route. Some authors mentioned that advancing the guidewire to the duodenum via the PEHBD/D1 route was troublesome and often failed owing to the needle direction toward the hepatic hilum [
3,
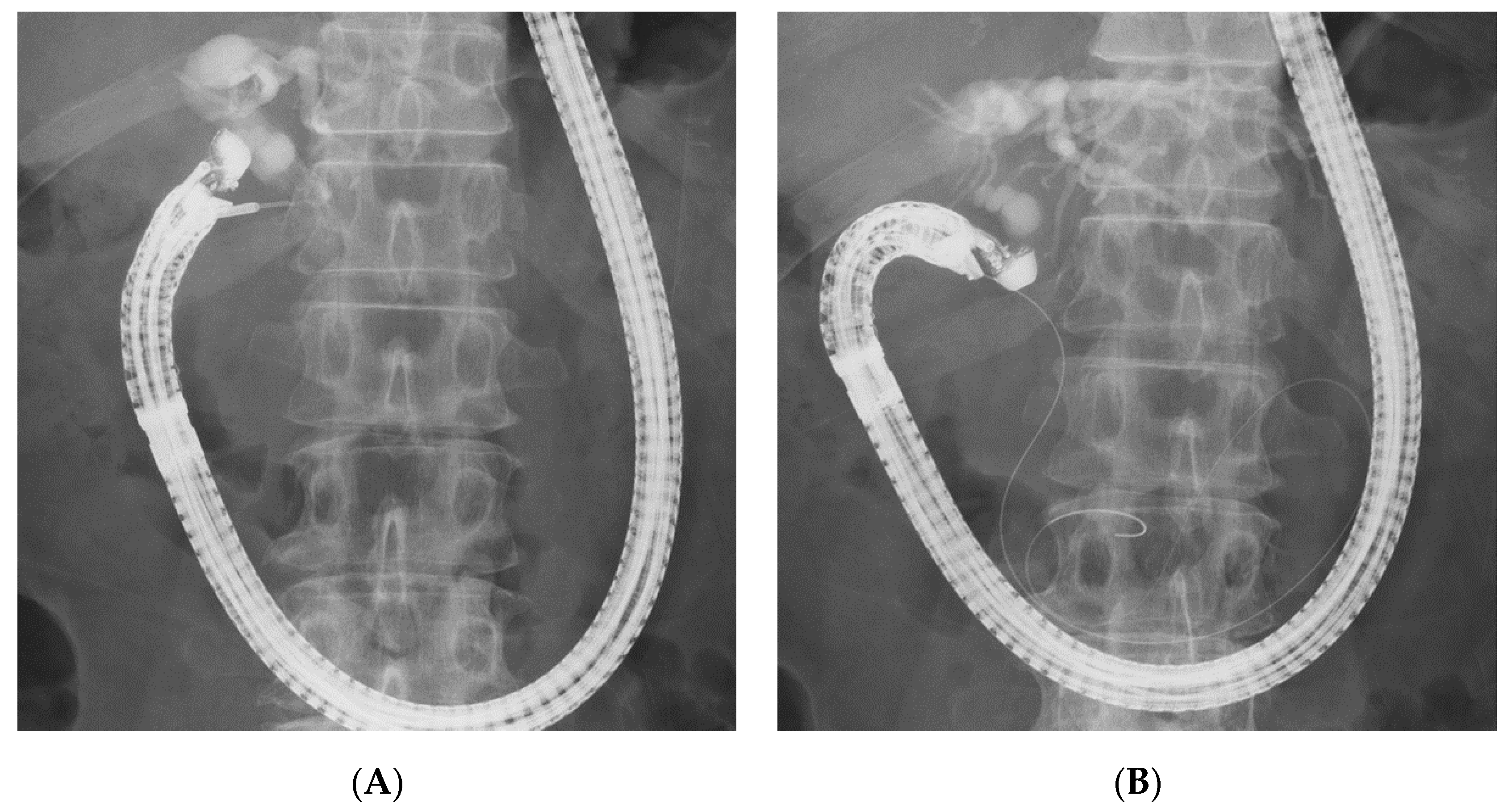
5]. To overcome this problem, we preferably used EG-580UT over GF-UCT260. The high flexibility scope shaft and the wide ranges of the angle and elevator of EG-580UT could allow the needle to advance toward the distal side of the bile duct (
Figure 2b). When the needle direction was not favorable for advancing the guidewire during the puncture, we changed the needle direction to the caudal side by pushing the scope to the cranial side and by using the up-angle of the scope (
Figure 9). If advancing the guidewire toward the ampulla was impossible, even when using maneuvers of the scope, we inserted a catheter into the bile duct to assist the guidewire manipulation [
5,
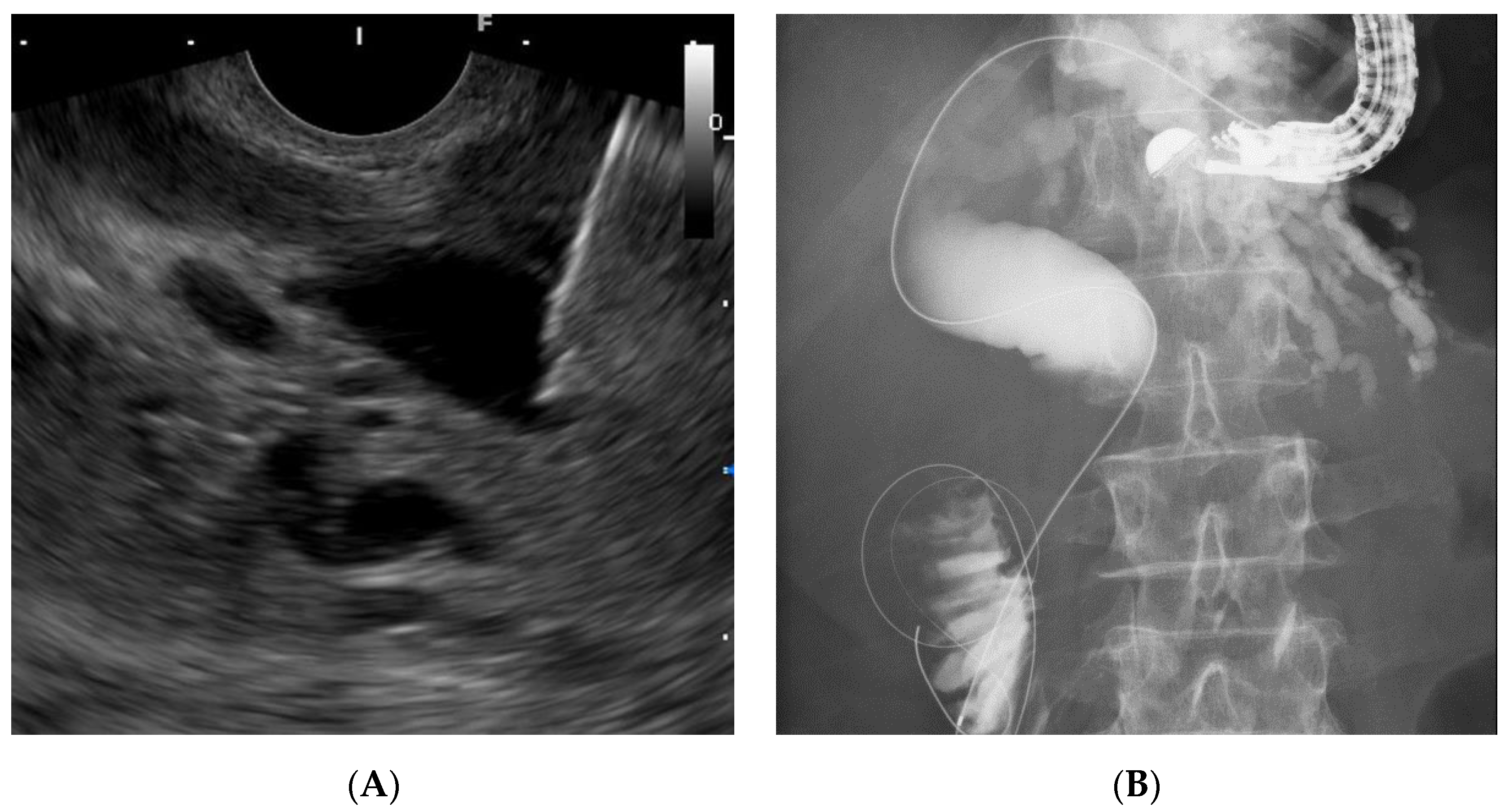
21]. IHBD approaches were needed in only two patients. The LIHBD/S route was used in the patient with a distal biliary obstruction and a pancreatic head cyst, and the guidewire passage through the stricture required a very long time (19 min), even when using the catheter support, because of the long, winding, and wide bile duct between the puncture point and the stricture (
Figure 3B). The RIHBD/D1 route was applied in one case with the difficult puncture of the EHBD or LIHBD.
Discussing according to the biliary disorders, the DEHBD/D2 route was successfully performed in 100% (five of five) of cases with bile duct stones. Generally, the puncture of the DEHBD from the D2 in cases with bile duct stones was considered to be difficult because of inadequate intraductal pressure [
3]. To prevent the collapse of the bile duct by the tip of the needle, we pushed the needle handle as quickly as possible, hitting the needle stopper with the maximum force as needed. With regard to distal biliary obstruction, the DEHBD/D2 route was used in only 44.3% (four of nine) of the patients mainly because of the unstable scope position due to the malformation of the duodenum caused by tumor infiltration or chronic pancreatitis. The PEHBD/D1 route was successfully used in all remaining patients but one for whom the LIHBD/S route was used because of an intervening pancreatic cyst. Since the guidewire passage through the distal biliary stricture in the LIHBD/S route was extremely difficult because of the long, winding, and wide bile duct in this case and in previous reports [
7,
21,
22], the PEHBD/D1 route might be better, especially in distal biliary obstruction, than IHBD approaches when the DEHBD/D2 route is impossible or failed. As for hilar biliary obstruction, the puncture of the EHBD was exceedingly challenging because of its extreme thinness due to a lack of the influx of bile juice, so the DEHBD/D2 route was successfully used in only 50% (one of two) of patients, even when using a 22 gauge needle, whereas the RIHBD/D1 route was needed in another patient. The RIHBD/D1 route was a useful option for hilar biliary obstruction when the LIHBD/S route was unavailable due to the tumor location.
The number of patients in the present study was so small that the validity of our method could not be confirmed. To complement the small number of patients, we performed a review of the literature that described the rates of success and adverse events for each approach route separately and had five patients or more (
Table 6). If the distinction between DEHBD/D2 and PEHBD/D1 was uncertain in cases with the EHBD approach, those cases were excluded from the review. According to this review, the DEHBD/D2 and PEHBD/D1 routes were equal in terms of the success rate (92.1% vs. 88.3%,
p = 0.477) and the adverse event rate (10.2% vs. 9.3%,
p = 1). As for the comparison of the DEPBD/D2 and PEHBD/D1 routes, Iwashita et al. directly compared them in a prospective study, and the higher cannulation success rate of the DEHBD/D2 route than that of the PEHBD/D1 route was demonstrated [
3]. In addition, the shorter guidewire manipulation time in the DEHBD/D2 route was showed in the current study. Given these facts, the DEHBD/D2 route was likely to be suitable for the first-line approach. In the review, the PEHBD/D1 route was better than the LIHBD/S route in terms of success rate (88.3% vs. 78.8%,
p = 0.059) and adverse event rate (9.3% vs. 16.9%,
p = 0.119), although there were no significant differences. Moreover, Dhir et al. reported that the time between the introduction of the echoendoscope and the introduction of the duodenoscope in the PEHBD/D1 route was significantly shorter than that in the LIHBD/S route [
22]. Consequently, our strategy in which the PEHBD/D1 route should take precedence over the LIHBD/S route was considered to be reasonable. As for the RIHBD/D1 route, we could not validate our strategy because there was only one case report including the RIHBD/D1 route [
23].
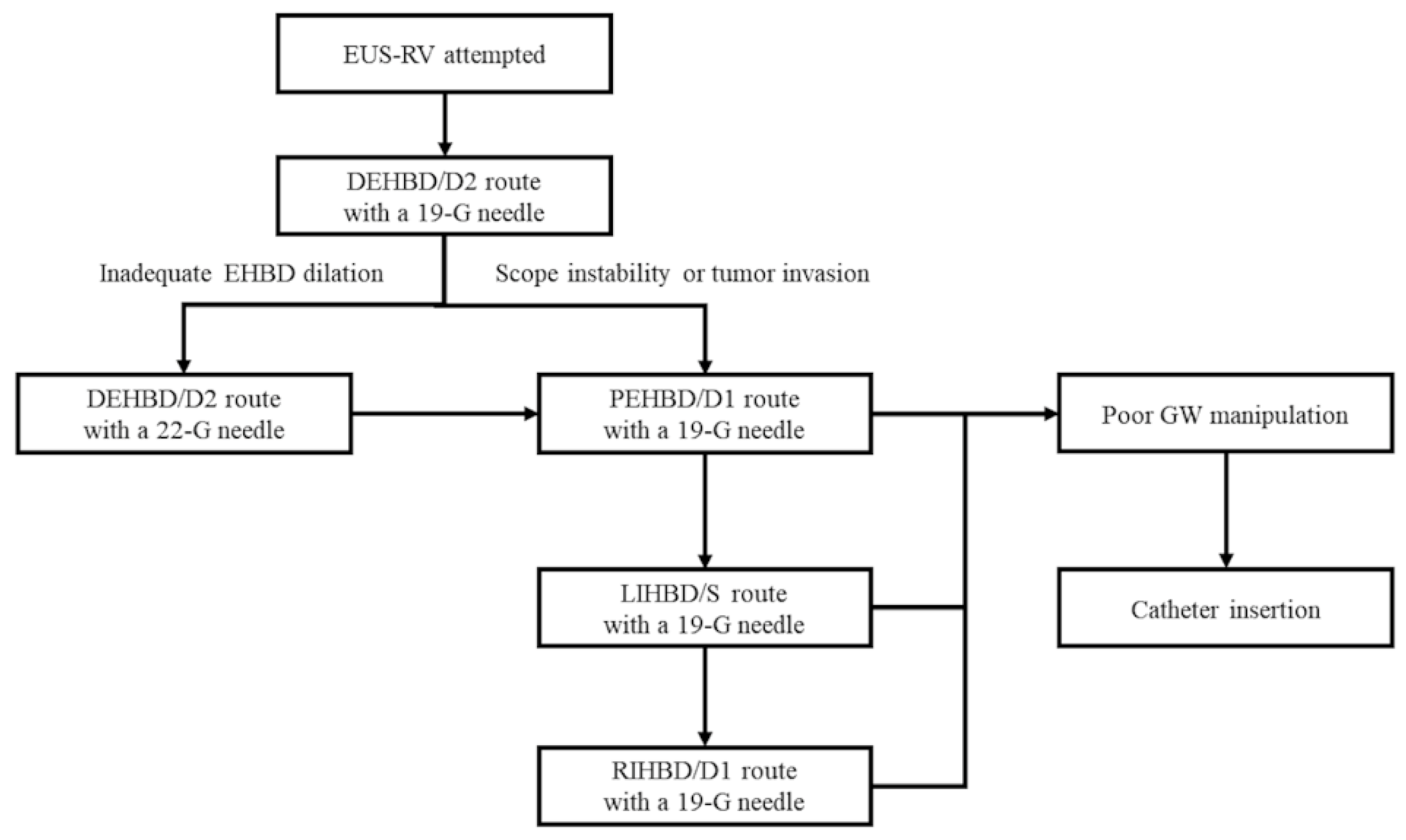
Considering both the literature review and our experiences, we proposed a new algorithm for EUS-RV based on our method (
Figure 10). The DEHBD/D2 route with a 19 gauge needle is the first-line method. If the puncture is impossible or fails due to inadequate EHBD dilation, the DEHBD/D2 route with a 22 gauge needle is recommended. If the puncture is impossible or fails even when using a 22 gauge needle or due to scope instability or tumor invasion, the PEHBD/D1 route, LIHBD/S route, and RIHBD/D1 routes are recommended in this order with a 19 gauge needle. When the guidewire is hard to advance to the duodenum, catheter insertion into the bile duct is suggested.
We previously reported that the hitch-and-ride method could shorten the cannulation time [
16]. In the present study, the hitch-and-ride method had a tendency to shorten the cannulation time compared with the other methods. However, there was no statistically significant difference. The reasons for the negative outcome in the present study were considered to be the small number of patients and the heterogeneity of the hand-made catheters. Despite the lack of decisive superiority, we recommend the hitch-and-ride method because of the possibility of reducing the cannulation time and because of its easiness.
Adverse events included only one instance of pancreatitis (6.3%) in the present study. Although some authors explained that EHBD approaches have a larger risk of bile leak than IHBD approaches due to a lack of the tamponade effect in the surrounding liver parenchyma [
2,
7,
11,
12], we did not encounter any adverse events related bile leak, notwithstanding the use of EHBD routes in 87.5% (14 of 16) of patients. Dhir et al. reported that a higher incidence of adverse events was seen with the LIHBD/S route than with the PEHBD/D1 route and suggested that the reason might be the dynamic movement of the left lobe of the liver with respiration [
22]. Actually, the adverse event rate was higher in the LIHBD/S route than in EHBD approaches in our literature review. We believe that a major cause of bile leak is failed cannulation after successful biliary puncture, as well as a long procedure time between the puncture and the biliary drainage. Thus, our strategy, which highlights the guidewire manipulation over the biliary puncture, could prevent bile leak. Moreover, we deployed biliary stents or naso-biliary tubes across the puncture site where possible to prevent bile leak, particularly when a catheter was inserted via the puncture point.
There are some limitations in the present study. First, the retrospective design including a small number of patients was the major limitation of this study. Second, all procedures were performed at a single center and by a single endoscopist. Third, the timing of the EUS-RV was not definite, which was likely to affect the rates of successful cannulation and adverse events.
In conclusion, the new proposed algorithm, which highlights guidewire manipulation, might facilitate EUS-RV for failed biliary cannulation. The DEHBD/D2 route was the first-line approach but was sometimes unavailable, especially in cases of distal and hilar biliary obstruction, because of scope instability and the thin bile duct, respectively. The PEHBD/D1 route was the second-line approach. Particularly in cases of distal biliary obstruction, the PEHBD/D1 route might be more suitable than the IHBD approach because guidewire manipulation in the IHBD approach was extremely difficult. In cases of hilar biliary obstruction, the biliary puncture in the PEHBD/D1 route might be difficult, and the puncture of the dilated IHBD was useful. If the LIHBD/S route was unavailable due to the tumor location, the RIHBD/D1 route was recommended. Further investigation in a prospective study with a large cohort is warranted.

 ,
, 












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



