1. Introduction
Religion plays an important role in many people’s lives, and can impact both physical and mental health. A growing body of research has examined potential links between religiosity and health behaviors, particularly sexual risk behaviors, in adolescents and young adults. Risky sexual behavior is common among college students, as campus “hook-up” culture promotes casual and unplanned sexual encounters (
Burdette et al. 2009;
Grello et al. 2006). Students often perceive certain risky behaviors, such as oral and/or anal sex, to be less intimate (and therefore more allowable) than vaginal sexual intercourse (
Chambers 2007;
Kelly and Kalichman 2002;
Lyons et al. 2013). It is important to note that oral and/or anal sex are not inherently riskier than vaginal sex; they are classified in most studies as risk behaviors specifically because of the high likelihood that they will occur without protection against STIs (
American College Health Association 2015;
Boekeloo and Howard 2002;
Brückner and Bearman 2005;
Moore and Smith 2012).
Parents have consistently been identified as the most important source of religious influence, both in childhood and adolescence, and into adulthood (
Lambert and Dollahite 2010;
Smith 2003a;
Smith and Denton 2005;
Smith et al. 2003). Parental religiosity in particular has been associated with adolescents being less involved in problematic risk behaviors such as alcohol and drug use (
Foshee and Hollinger 1996;
Hayatbakhsh et al. 2014;
Pearce and Haynie 2004). In terms of sexual risk, overall family environment has been shown to play a protective role in adolescent reproductive health decisions (
Manlove et al. 2008). However, few studies have considered the specific impact of parental or family religiosity on adolescent sexual behavior, either directly or through influence on adolescents’ own religiosity. Those that do exist have used single variables, such as parents’ report of religious involvement or of specific beliefs, as a proxy for family religiosity (
Manlove et al. 2008;
Manlove et al. 2006). Further research is needed to inform a more complete understanding of the mechanisms by which multiple dimensions of family religiosity may impact adolescents’ own religiosity and their sexual health decision-making.
The current study extends the literature in order to improve our understanding of the relationships between multi-dimensional aspects of family and college students’ religiosity and sexual behavior. This study contributes to existing literature in several unique ways. First, it identifies multiple dimensions of potential religious influence, rather than the one-dimensional measure of religious attendance that is typically used. Second, it considers multiple indicators within the broader context of sexual behavior, allowing for the possibility to observe different avenues of influence by specific sexual act or practice. And third, it considers both family-level and individual-level influences on college students’ behavior, acknowledging that these different spheres may be congruent or may contradict one another.
4. Results
Demographic characteristics of the analytic sample are presented in
Table 1. Nearly 77 percent (
n = 467) of the sample identified as female, and slightly more than half (
n = 318, 52.3%) as White, with a median age of 21 years old. Religious affiliation was distributed across six separate groups, with a majority of the sample identifying as Christian (non-Catholic) (
n = 158, 26.2%), Roman Catholic (
n = 136, 22.5%), or Atheist/Agnostic (
n = 130, 21.4%). Students were most likely to describe themselves as being currently uninvolved in a sexual relationship (
n = 253, 41.6%) or involved with one serious (monogamous) sexual partner (
n = 244, 40.1%) (for reference, only 8 students reported being married).
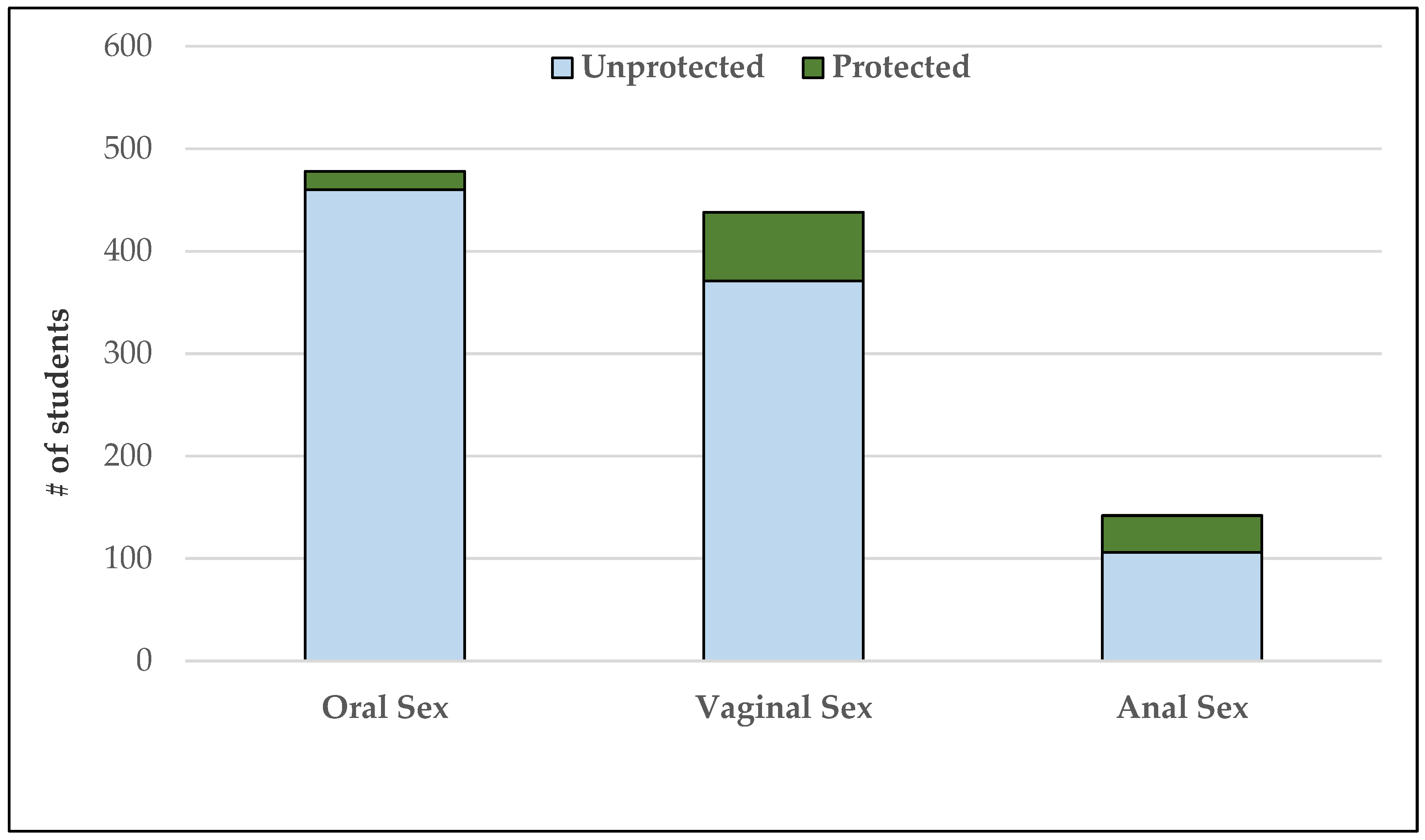
Students reported high levels of sexual activity and sexual risk behaviors; students’ participation in certain sex acts and use of pregnancy and STI prevention methods are highlighted in
Figure 1 and
Figure 2. Among students who have participated in any sexual activity (oral, vaginal, or anal), more students (
n = 282, 57%) delayed their first sexual activity until age 17 or later and slightly more than half (
n = 276, 56%) have had four or more sexual partners.
Overall, students reported low family religiosity during their childhood and adolescence (
Table 2). The mean
FAITHS frequency score was 10.56 (possible scores ranged from 0 to 54, with a higher score indicating greater frequency. Average scores in the ‘never’ or ‘yearly’ category were categorized as ‘infrequent’ (61%); average scores in the ‘monthly’ category or higher were categorized as ‘frequent’ (39%). Scores on each of the four domains of student religiosity, as well as total student religiosity scores, were low to moderate, indicating a low overall degree of current religiosity in this sample. However, students reported a moderate to high degree of parental monitoring during high school, with female students reporting significantly greater parental monitoring than male students.
Bivariate results. Unadjusted associations between family religiosity and sexual behaviors were computed first for the total sample (
Table 3) and then stratified by religious group (tables not shown). Subsequent analyses consider degree of religiosity across groups for the total sample, rather than by denomination. Students who reported frequent family religiosity were less likely ever to have had oral sex, vaginal sex, and anal sex than were those who reported infrequent family religiosity. Among students who reported ever having had vaginal sex, students who reported frequent family religiosity were less likely ever to have had it unprotected.
Parental monitoring differed significantly by family religiosity, with students reporting frequent family religiosity also reporting a higher degree of parental monitoring (M = 24.98, SD = 6.484) than students who reported infrequent family religiosity (M = 22.18, SD = 6.680), t(443) = −4.317, p < 0.001. Students who reported greater parental monitoring were less likely to have had four or more lifetime partners (OR = 0.959, 95% CI: 0.929, 0.989), less likely ever to have had anal sex (OR = 0.950, 95% CI: 0.920, 0.980), and less likely ever to have had unprotected vaginal sex (OR = 0.921, 95% CI: 0.874, 0.971). They were more likely to have used any effective method of pregnancy prevention at last vaginal sex (OR = 1.075, 95% CI: 1.023, 1.131), and more likely specifically to have used a condom at last vaginal sex (OR = 1.049, 95% CI: 1.014, 1.084).
Associations were also computed between the independent variable of family religiosity and the potential moderator of student religiosity (
Table 4); students who reported frequent family religiosity scored significantly higher on every domain of individual religiosity than did students who reported infrequent family religiosity.
Multivariate results.Table 5 and
Table 6 present the results of multivariate analyses. After controlling for relevant individual- and family-level covariates, we found that students who reported frequent family religiosity were significantly less likely ever to have had oral sex (aOR = 0.429, 95% CI: 0.239, 0.771) and ever to have had vaginal sex (aOR = 0.551, 95% CI: 0.323, 0.942) (
Table 4). Among students who reported having had vaginal sex, students with frequent family religiosity remained significantly less likely ever to have had unprotected vaginal sex (aOR = 0.470, 95% CI: 0.262, 0.841).
Only one outcome variable, ever having had unprotected vaginal sex, had a statistically significant relationship with both the independent variable of family religiosity (OR = 0.563, 95% CI: 0.329, 0.962) and with the potential mediator of parental monitoring (OR = 0.921, 95% CI: 0.874, 0.971); subsequent tests for mediation using hierarchical logistic regression were conducted on this outcome variable. After controlling for relevant individual-level characteristics, results suggest that, as hypothesized, there was a significant indirect effect of family religiosity on college students’ ever having had unprotected vaginal sex through parental monitoring (b = −0.261, BCa CI: −0.515, −0.085).
To test for possible moderation by student religiosity, we built separate hierarchical logistic regression models for each sexual behavior outcome and the interaction of family religiosity with each of five possible student religiosity scores (four domain scores and one total score). Results from these regressions (tables not shown) indicate that none of the five domains of student religiosity moderate the relationship between family religiosity and student sexual activity or sexual risk. Student religiosity was subsequently explored as an independent predictor of students’ sexual activity and sexual risk. After controlling for relevant individual-level and family-level characteristics, higher students’ total religiosity score was significantly associated with less likelihood of having had four or more sexual partners (aOR = 0.985, 95% CI: 0.970, 1.000), ever having had oral sex (aOR = 0.972, 95% CI: 0.952, 0.993), ever having had vaginal sex (aOR = 0.973, 95% CI: 0.953, 0.993), and ever having had anal sex (aOR = 0.979, 95% CI: 0.960, 0.998). In addition, students with a higher religiosity score were more likely to have used a condom at last vaginal sex (aOR = 1.017, 95% CI: 1.001, 1.034) (
Table 5).
5. Discussion
Findings from this study suggest that religiosity, both family and individual, may play a role in emerging adults’ sexual behavior. Greater family religiosity was associated with a decreased likelihood of students’ engaging in certain sex acts (ever having had oral or vaginal sex), but for students who did choose to engage, family religiosity was not associated with any differences in the timing of sexual onset or in the students’ number of partners. This finding confirms previous work and implies that family religiosity may influence some students’ decisions whether or not to have sex; but for students who do choose to have sex, the break from religious teachings about sex may already have occurred, so family religiosity no longer had a role to play in decisions like when to begin having sex, or whether or not to have sex with more than one partner. It is also possible that students who internalized religious messages about refraining from sexual activity might be more likely to characterize their families as being highly religious than would students for whom those religious messages were less salient.
Contrary to our expectation, higher family religiosity was associated with a decreased likelihood of risk behaviors, rather than an increased likelihood of risk. Within the context of the previous finding, it may be that students who have chosen to be sexually active, in contradiction to family religious teachings about sexual activity, would be more likely to take extra precautions so as not to be found out (through pregnancy or STIs) by their parents or other family members. Previous research on adolescents active in their church community found that participants’ parents had regularly reinforced the idea that going against biblical principles related to sexual activity would increase the likelihood of negative consequences that could derail future goals and opportunities (
Moore et al. 2014). Fear that a negative consequence like unplanned pregnancy may lead to parental disappointment or shame may drive students to protect themselves from risk by avoiding unprotected vaginal sex to maintain the secrecy of sexual activity.
Though more frequent family religiosity was associated with higher student religiosity, none of the four domains of student religiosity (overall self-ranking, private practice, forgiveness, or organizational religiosity), nor the total student religiosity score, served to moderate the relationship between family religiosity and students’ sexual behaviors. The finding that higher family religiosity is associated with higher student religiosity was expected; growing up in an environment that values religious participation and religious teachings is likely to instill an appreciation for, or sense of obligation to, those religious traditions. The lack of moderation by students’ current religiosity on the relationship between family religiosity and students’ sexual behaviors suggests that, rather than family religiosity exerting influence in the form of a parent’s voice in a student’s head or memories of a family’s religious teachings, a more thorough transmission of beliefs may occur in highly religious families, so that students now view those beliefs as their own, rather than as a holdover from parental influence in childhood. Having a high degree of personal religiosity is independently associated with certain student sexual behaviors, but that association does not change the original relationship between family religiosity and students’ behaviors; whether or not a student has internalized religious messages remains separate from the potential internalizing of other standards of behavior or sexual expectations.
Students in more religious families report a higher degree of parental monitoring, and also a significantly lower likelihood of ever having had unprotected vaginal sex (among students who have had vaginal sex). This finding seems to support earlier findings in this study and the possibility that fear of parents finding out about sexual activity may be a strong motivator for students from highly religious families to avoid sexual risk-taking. Parents in more religious families are paying more attention to students’ whereabouts and behaviors. If the family’s messaging around sex is religiously motivated and focused on abstinence or ‘saving oneself for marriage’, it is likely that students’ fear of negative consequences (like pregnancy or sexually transmitted infections) is leading them to use condoms during vaginal sex. Avoiding pregnancy or sexually transmitted infections may ensure that parents never learn about students’ sexual activity or behaviors.
It is also possible that the desire to maintain individual and family reputation within a close religious community acts as further motivation to avoid risk.
Hill et al. (
2014) suggest that an individual may be more likely to engage in a behavior like premarital sex if feelings of shame or embarrassment associated with that behavior were lower. In a highly religious family that is part of a larger religious community, stigma around premarital sex and the potential to bring community shame upon and one’s family may further motivate sexually active students to avoid unprotected vaginal sex that could result in an unintended pregnancy.
This study has certain limitations that must be considered when interpreting the results. Because participants were assessed at only one time point, causal inferences cannot be made using these cross-sectional data. In addition, because we only had access to students and not to their parents or families, family religiosity was measured by students’ retrospective report. It is possible that students’ recall of family religious activities may not be consistent with perceptions of other family members. Because religiosity (both family and individual) was low overall in this sample, it is possible that we may not be fully capturing the relationship between religiosity and emerging adults’ sexual behaviors; however, the strength and direction of certain findings related to religiosity, despite low report overall in the sample, suggest that we may be underestimating, rather than overestimating, the potential role of religiosity in emerging adults’ sexual behaviors.
A final limitation of this study relates to the fluid nature of sexual activity and sexual relationships during the developmental stages of late adolescence and emerging adulthood. An abundance of literature suggests that emerging adults develop intimate relationships and acquire new sexual experiences at a rapid pace (e.g.,
Alexander et al. 2015;
Meier and Allen 2009;
Tanner et al. 2009), often through casual hook-up encounters (
Allison and Risman 2014,
2017;
Stinson et al. 2014). Dating, love, and romantic exploration are different during emerging adulthood, with a focus on individual identity exploration as well as the potential for physical and emotional intimacy (
Arnett 2000). Given the rapid pace of change during this developmental stage, it is important to recognize that the data reported in this study only provide one snapshot of students’ sexual behaviors and do not account for the complexities inherent in emerging adult sexual encounters.
Despite these limitations, findings from this study contribute to the study of religion and family life by illuminating potential relationships between family-level influences and emerging adults’ sexual behaviors and highlighting the complex nature of religiosity and its long arm of influence. Overall, there is some evidence that both family and individual religiosity are associated with emerging adults’ sexual behavior, though the two play independent roles in the relationship, and parent religiosity seems to exert influence primarily through increased parental monitoring of adolescents.




{kind=link}
{kind=link}