1. Introduction
The improper and unnecessary use of antibiotics and the limited availability of new antimicrobial agents have contributed to the rise in antimicrobial resistance, which represents one of the most dangerous public human health problems in the world [
1,
2,
3,
4]. Surveillance studies allow the monitoring of the emergence of antibiotic resistances, the introduction of control measures, and the guidance for antimicrobial use in patients.
Enterobacter species are Gram-negative rod-shaped opportunistic microorganisms belonging to the family
Enterobacteriaceae, and cause severe urinary tract infections (UTIs), septicemia, and pneumonia in subjects who are on mechanical ventilation in the intensive care unit (ICU), premature infants, patients with diabetes, traumatized patients, patients affected by leukemia, or those under immunosuppressive therapy [
5,
6,
7].
Enterobacter species are members of the ESKAPE group (
Enterococcus faecium,
Staphylococcus aureus,
Klebsiella pneumoniae,
Acinetobacter baumannii,
Pseudomonas aeruginosa, and
Enterobacter species), which are known to be the most significant causes of nosocomial infections. Therefore, the World Health Organization (WHO) placed
Enterobacter spp. onto the priority list of microorganisms for which it is essential to research and develop new antibiotics [
6]. Actually, out of 22 species belonging to the
Enterobacter genus, such as
E. aerogenes,
E. amnigenus,
E. arachidis,
E. asburiae,
E. carcinogenus,
E. cloacae,
E. cowanii,
E. dissolvans,
E. gergoviae,
E. helveticus,
E. hormaechei,
E. kobei,
E. ludwigii,
E. mori,
E. nimipressuralis,
E. oryzae,
E. pulveris,
E. pyrinus,
E. radicincitans,
E. soli,
E. taylorae, and
E. turicensis, two of them,
Enterobacter aerogenes, recently classified as
Klebsiella aerogenes after full-genome sequence analysis, and
Enterobacter cloacae, are responsible of the majority of human diseases [
6].
Enterobacter spp. present an intrinsic resistance to ampicillin and broad-spectrum cephalosporins and, through the acquisition of genetic mobile elements, have become resistant to many antibiotics, such as third-generation cephalosporins and carbapenems, thus making difficult the selection of an appropriate therapy [
5,
6,
7,
8,
9]. The increasing trends of antibiotic resistance of
Enterobacter strains are associated with higher mortality rates in infected subjects, longer hospitalizations, and higher costs of treatments [
6]. A few works on antibiotic resistances of
Enterobacter spp. have been published, particularly over a long time period [
10,
11,
12,
13]. In this study, we aimed to retrospectively investigate the susceptibility patterns of
Klebsiella aerogenes (
Enterobacter aerogenes) and
Enterobacter cloacae strains using the recorded microbiological data of the Laboratory of Italian Hospital of Desio over a 20-year period (2000–2019). The assessment of antimicrobial resistance trends might be helpful to clinicians to prescribe a more appropriate therapy and to reduce treatment failure in patients.
2. Results
We identified a total of 2277 non-duplicate
Enterobacter spp. strains from positive samples, 1037 from outpatients (45%), and 1240 from hospitalized subjects (55%). Among inpatients, most of
Enterobacter spp. strains were isolated from surgery (
n = 207), followed by ICU (
n = 162), neurology (
n = 162), and internal medicine (
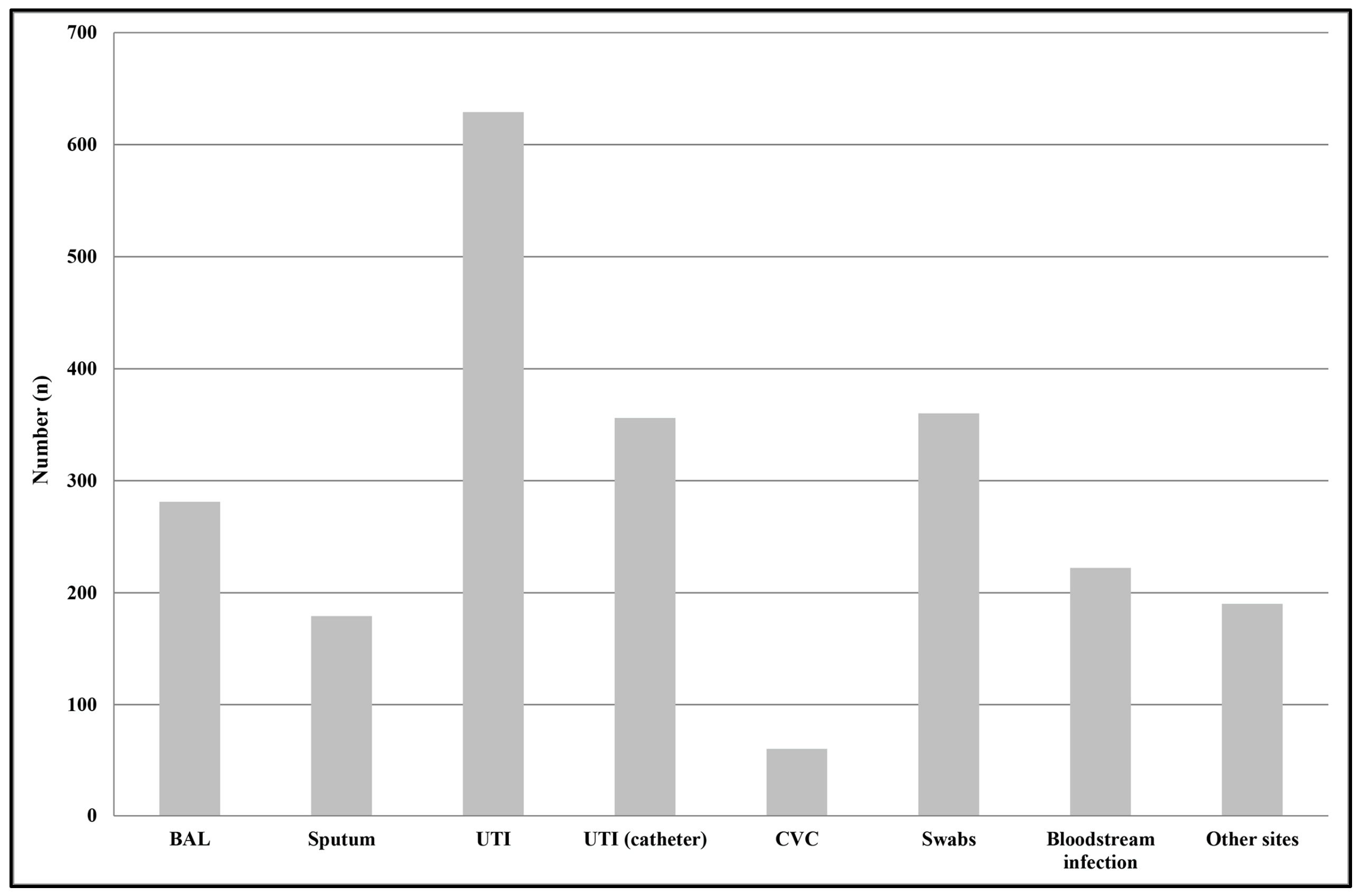
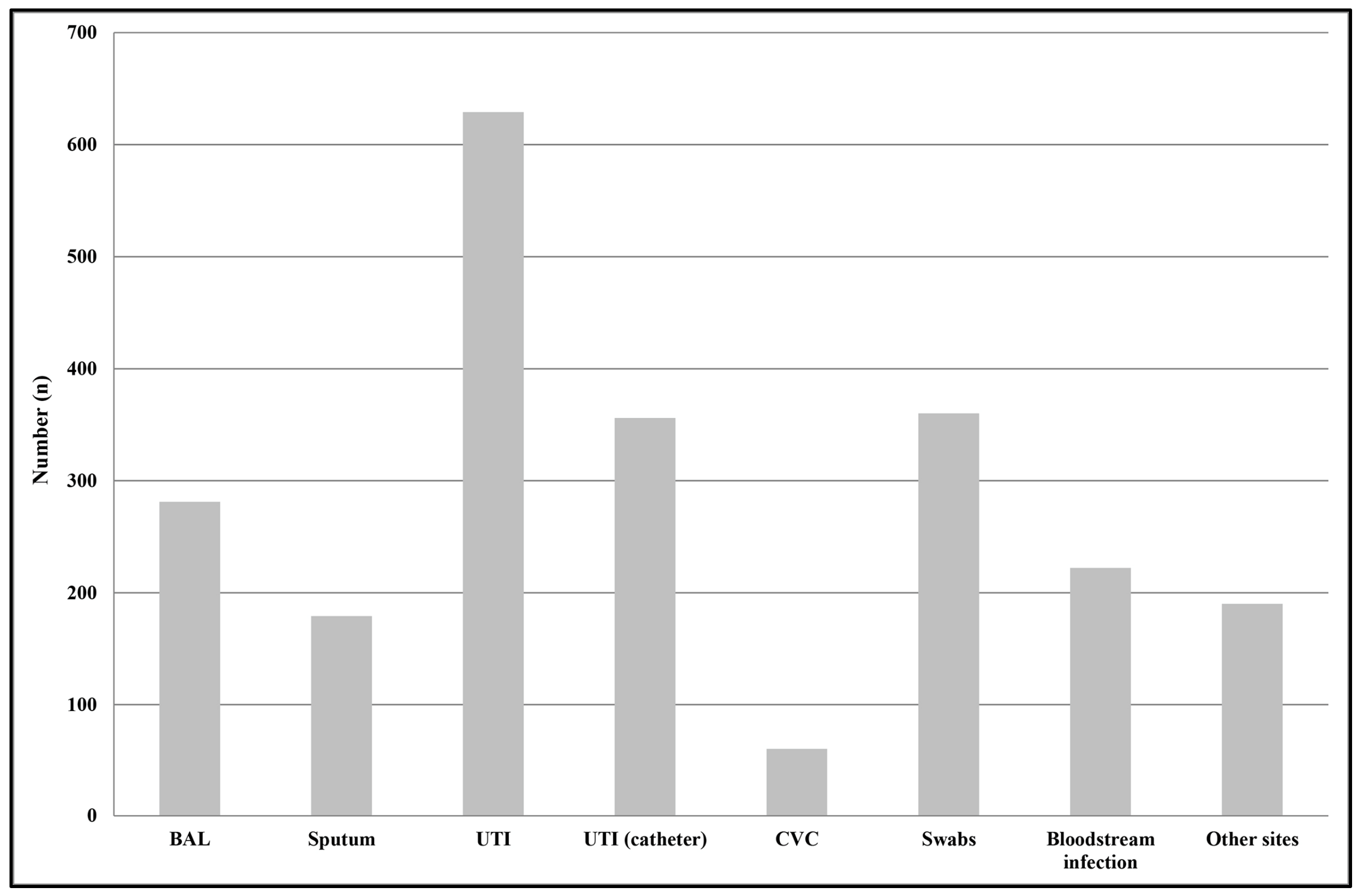
n = 156). The median age of patients was 69 years (interquartile range (IQR): 4–87 years). The majority of isolates were from females (83% compared with 17% males). The most common specimen type from which
Enterobacter spp. strains were isolated was midstream urines (28%,
n = 629), followed by swabs from different sources, particularly the skin, vagina, and urethra (16%,
n = 360); urine samples from subjects with a catheter (16%,
n = 356); bronchoalveolar lavage (BAL) (12%,
n = 281); bloodstream (10%,
n = 222); and sputum (8%,
n = 179) (
Figure 1).
Among outpatients, the most common specimen type from which
Enterobacter spp. strains were isolated was midstream urine (54%,
n = 561), while, among inpatients, the most common specimen types were urine samples from subjects with a catheter (21%,
n = 264) and BAL (20%,
n = 253) (
Figure 2). Among all of the isolates,
E. cloacae was identified in 1230 samples;
K. aerogenes (
E. aerogenes) in 907; and
E. amnigenus,
E. kobei,
E. asburiae, and
E. gergoviae in 29; while in 111 specimens, it was not possible to determine the species using either VITEK
® 1 and 2 systems or Vitek
® MALDI-TOF MS (bioMérieux, Marcy l’Étoile, France), thus they were reported as
Enterobacter spp. No significant differences were observed between inpatients and outpatients concerning the species isolated (
p > 0.05). A significant decrease was observed in the isolation of
E. cloacae strains, from a mean value of 60 cases/year to 20 cases/year in the last two years (2018 and 2019) (
p < 0.01), while the number of
K. aerogenes (
E. aerogenes) isolates remained constant over the whole period (45 cases/year).
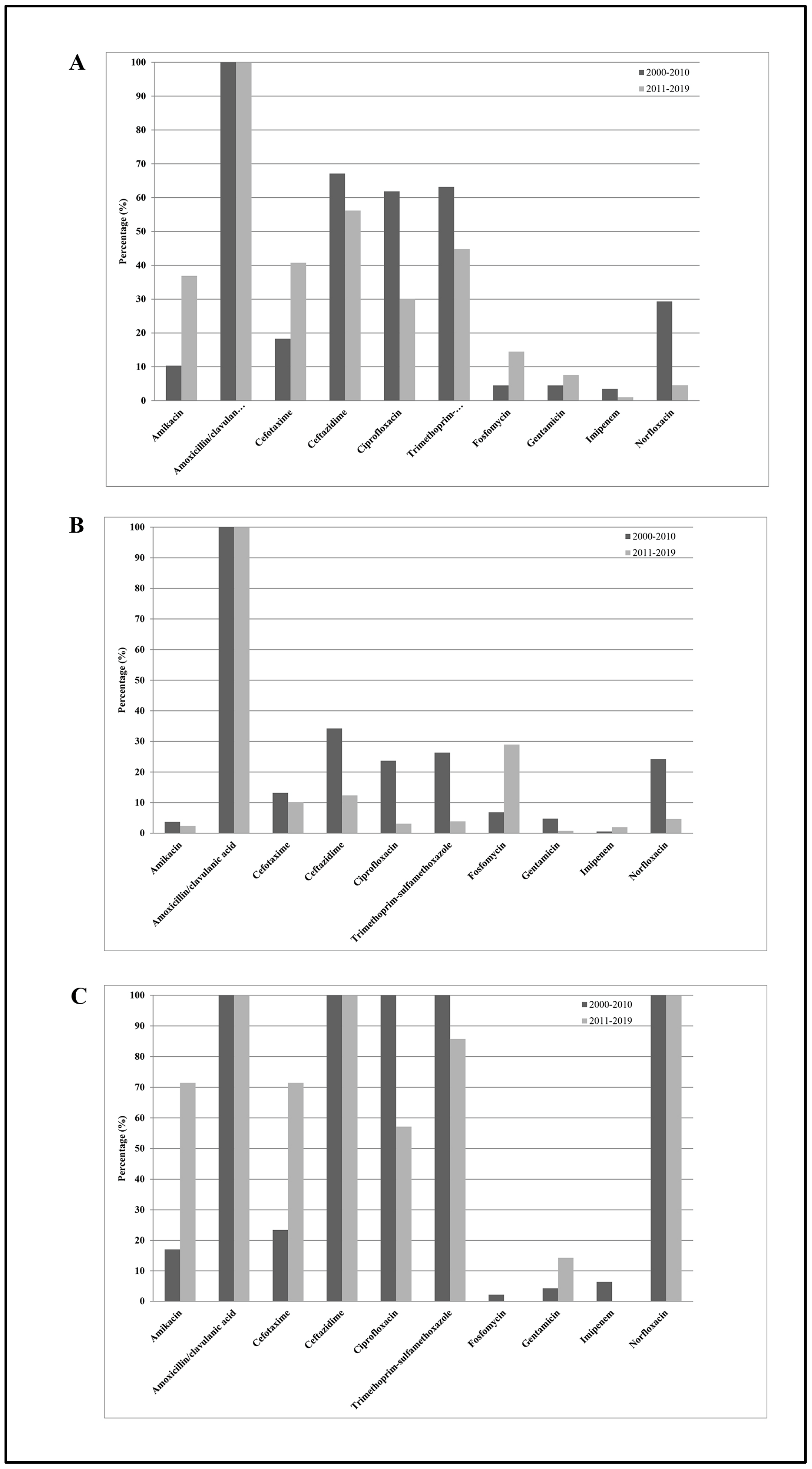
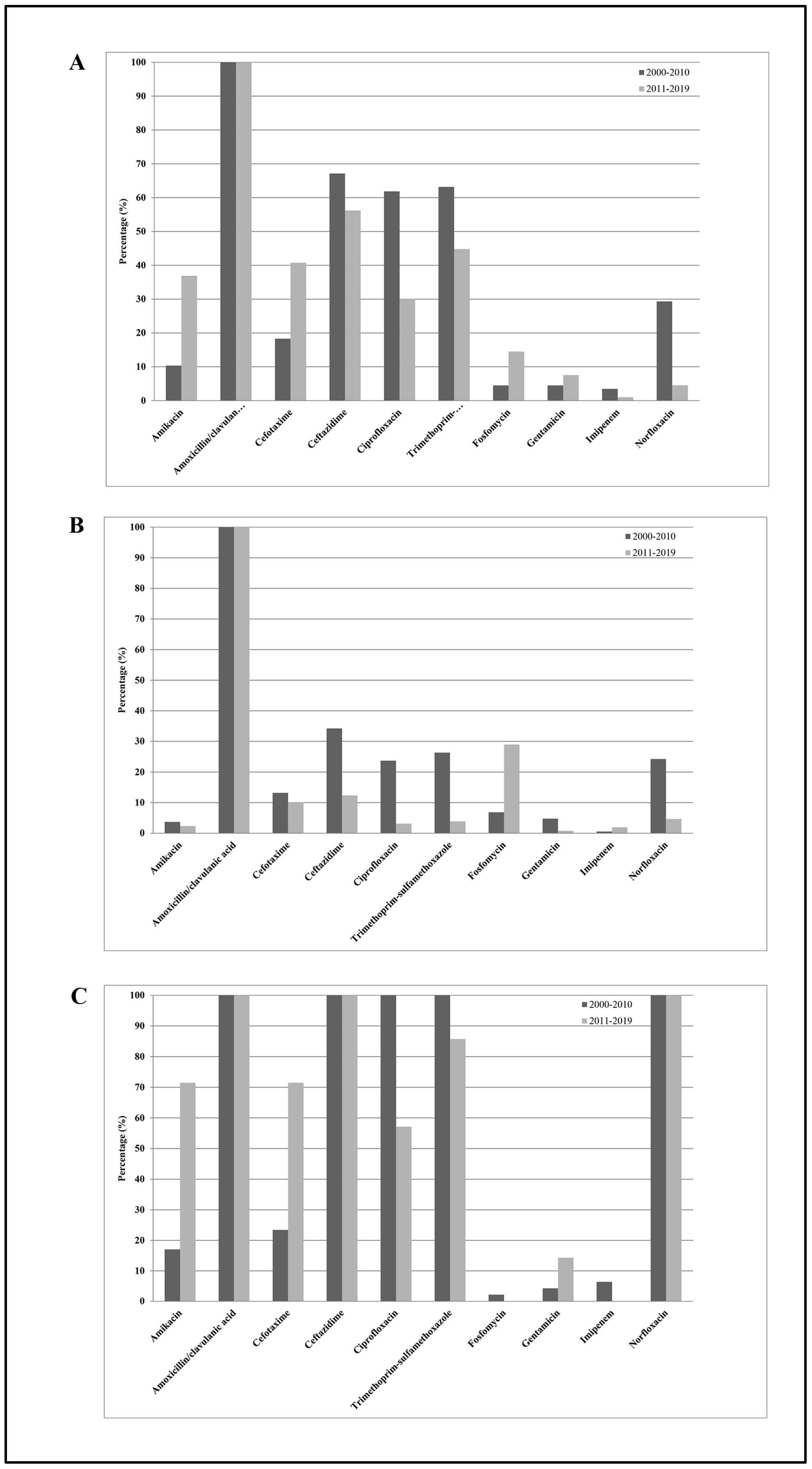
Figure 3 shows the
E. cloacae susceptibilities to the 10 antimicrobial agents tested among all subjects enrolled in the study. From 2000–2010 to 2011–2019, except for gentamicin (from 50% to 12%) and ciprofloxacin (from 55% to 18%), which showed significant decreasing resistance rates (
p trend < 0.01), and except for fosfomycin (from 9% to 37%), which showed a significant increasing resistance rate (
p trend < 0.01), none of the other antibiotics (mean values: amikacin 10%, amoxicillin/clavulanic acid 100%, cefotaxime 56%, ceftazidime 56%, imipenem 1%, and trimethoprim-sulfamethoxazole 23%) showed significant changes over time (
p trend > 0.05). Considering all antibiotics, the mean resistance rate increased from 42% in 2000–2010 to 36% in 2011–2019, representing a not statistically significant difference (
p trend > 0.05). However, separating the entire population into inpatients and outpatients, we noted the following: (1)
E. cloacae strains isolated from inpatients were resistant to two or more categories of antibiotics (
β-lactams, third-generation cephalosporins, and
fluoroquinolones) compared with those isolated from outpatients; (2) significantly decreased resistance rate values for ciprofloxacin and gentamicin from 2000–2010 to 2011–2019 in hospitalized subjects (
p trend < 0.01); (3) significantly increased levels of fosfomycin in the two groups (
p trend < 0.01); and (4) not significant changes over time for the other antibiotics tested (
p trend > 0.05).
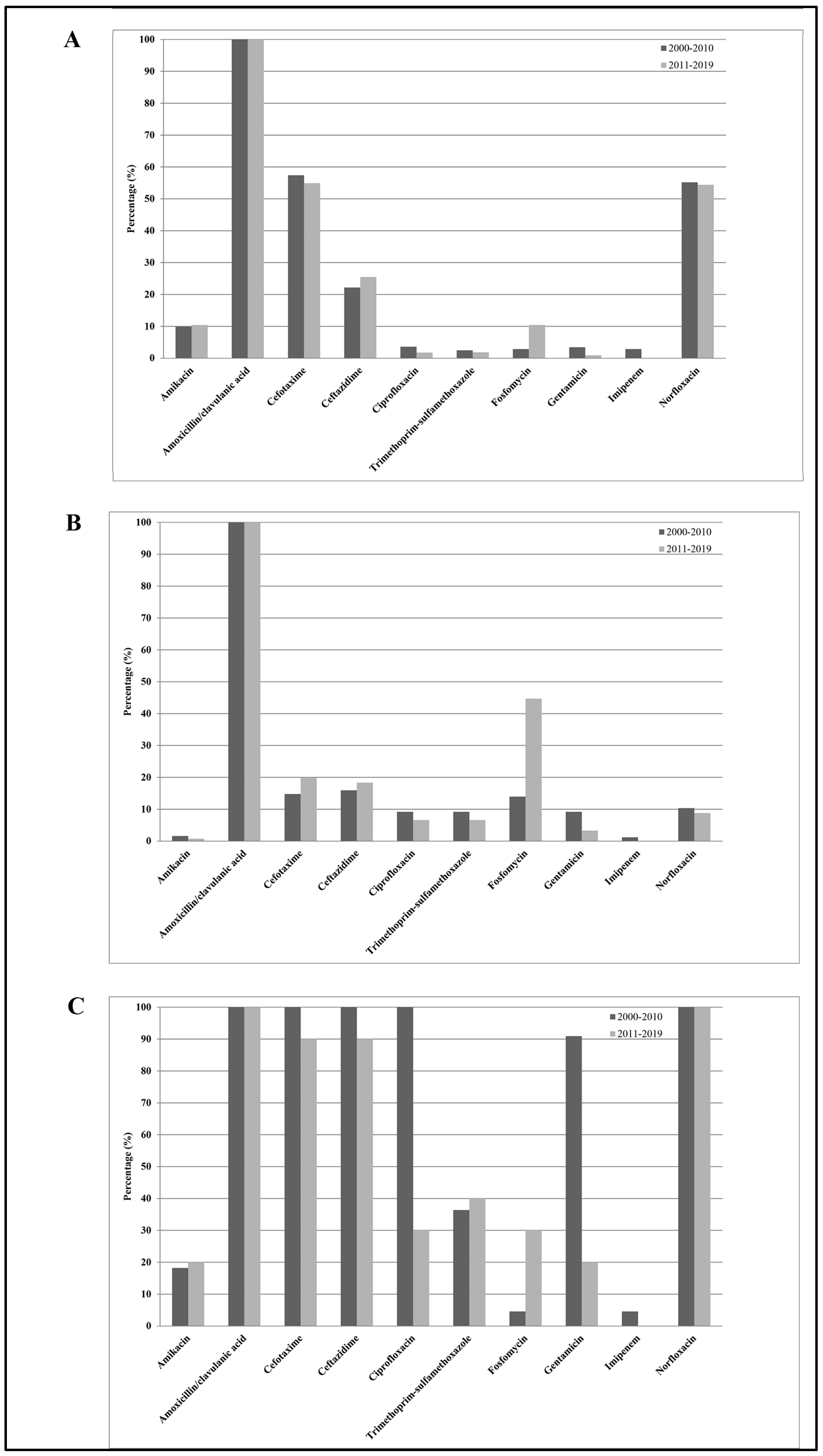
Figure 4 shows the
K. aerogenes (
E. aerogenes) susceptibilities to the 10 antimicrobial agents tested among all subjects enrolled in the study. From 2000–2010 to 2011–2019, except for amikacin (from 10% to 37%), trimethoprim-sulfamethoxazole (from 63% to 45%), ciprofloxacin (from 62% to 30%), norfloxacin (from 62% to 52%), and ceftazidime (from 67% to 56%), which showed significantly decreasing resistance rates (
p trend < 0.01), and except for cefotaxime (from 18% to 41%) and fosfomycin (from 4% to 14%), which showed a significantly increasing resistance rate (
p trend < 0.01), none of the other antibiotics (mean values: amoxicillin/clavulanic acid 100%, gentamicin 6%, and imipenem 1%) showed significant changes over time (
p trend > 0.05). Considering all antibiotics, the mean resistance rate increased from 36% in 2000–2010 to 34% in 2011–2019, representing a not statistically significant difference (
p trend > 0.05). On the other hand, among outpatients, the mean resistance rate decreased from 24% in 2000–2010 to 17% in 2011–2019, representing a statistically significant difference (
p trend < 0.01). Separating the entire population into inpatients and outpatients, we observed the following: (1)
K. aerogenes (
E. aerogenes) strains isolated from inpatients were resistant to two or more categories of antibiotics (
β-lactams, third-generation cephalosporins,
fluoroquinolones, and aminoglycosides) compared with those isolated from outpatients; (2) significantly decreased resistance rate values for ciprofloxacin in hospitalized subjects (
p trend < 0.01); (3) significantly decreased resistance rate values for
fluoroquinolones, ceftazidime, and trimethoprim-sulfamethoxazole in outpatients (
p trend < 0.01); (4) significantly increased levels of fosfomycin in outpatients (
p trend < 0.01); (5) significantly increased levels of
aminoglycosides and cefotaxime in inpatients (
p trend < 0.01); and (6) not significant changes over time for the other antibiotics tested (
p trend > 0.05).
Among all 2277 Enterobacter spp. strains, we observed a significant increase in E. cloacae-producing ESBL isolates and a significant decrease in K. aerogenes (E. aerogenes)-producing ESBLs among both inpatients and outpatients over the study period (p trend < 0.01), as well as a constant low value of carbapenem-resistant Enterobacter spp. isolates in the period from 2000–2010 to 2011–2019 (0.5%).
3. Discussion
Enterobacter species are present in the normal flora of the human gastrointestinal tract and are also widely encountered in the environment. These bacteria are found in the soil, sewage, and water and are considered phytopathogens for several plant species. Moreover, some species are used in bioprocessing and metabolic engineering approaches. Few data are available about the pathogenicity and virulence factors of
Enterobacter spp. owing to the low number of studies. It is known that
Enterobacter spp. possess a flagellum and they have the ability to form biofilm. They produce different endotoxins, enterotoxins, alpha-hemolysins, and cytotoxins [
6]. Recently, they have emerged as important agents of respiratory tract infections, particularly in subjects on mechanical ventilation, as well as of UTI, mainly in subjects with a catheter [
6,
9]. About 5% of the bacteremia acquired in the hospital, 5% of pneumonia, 4% of UTIs, and 10% of peritonitis are caused by
Enterobacter spp. [
6]. We assessed the antimicrobial resistance trends among
Enterobacter strains from both inpatients and outpatients between 2000 and 2019. In our study,
E. cloacae and
K. aerogenes (
E. aerogenes) strains accounted for 94% of all isolates, similar to the findings reported in previous work [
6,
9]. Out of all isolates, most of them were obtained from urine samples either from midstream or catheter-associated urine specimens, as previously described [
6,
9]. The worldwide overuse, the inappropriate prescription of antibiotics, and the lack of development of new antibiotic agents by pharmaceutical companies have promoted the rapid emergence of antimicrobial resistance in bacteria, causing the death of nearly 700,000 people worldwide every year [
14]. Surveillance studies are generally seen as primary strategies in the identification of bacterial changes in antimicrobial susceptibilities, with the aim to critically review the empirical treatment protocols. The present work is one of the largest databases on susceptibility patterns of
Enterobacter clinical isolates over a long period time, thus allowing for a reliable assessment of the resistance trends. In 2010, switching from CLSI to EUCAST guidelines, most antimicrobial susceptibility percentages did not change, although an increase in fluoroquinolones’ susceptibility of
Enterobacter spp. in the application of the EUCAST criteria was reported, most probably owing to the elimination of the intermediate category [
15,
16].
Enterobacter spp. are intrinsically resistant to ampicillin, amoxicillin, first-generation cephalosporins, and cefoxitin, owing to the presence of a constitutive AmpC β-lactamase. Moreover, the adaptation to the hospital environment, the ability to acquire several genetic mobile elements, and the modulation of the expression of different proteins associated with antimicrobial resistances and virulence make their treatment difficult. In fact, carbapenemases belonging to the New Delhi metallo β-lactamase (NDM) and Verona integron-mediated metallo-β-lactamase (VIM) types have been identified in
E. cloacae and
K. aerogenes (
E. aerogenes) strains in Europe, Asia and America. Serine β-lactamases, such as KPC (
Klebsiella pneumonia carbapenemases), was also reported, and oxacillinases, such as OXA-48, seem to be the most prevalent in
Enterobacter spp. Concerning aminoglycosides’ and fluoroquinolones’ resistance, it has been demonstrated that the acquisition of the non-susceptibility phenotype is mediated by transposable elements. Porin defects and augmented levels of efflux pumps are recognized as important elements in multi-drug-resistant strains. Lipopolysaccharide (LPS) modifications are involved in polymyxin susceptibility in
Enterobacter spp., where alterations in outer membrane structure lead to a considerable decrease in antibiotic activity. In fact, owing to the previous treatments, most
Enterobacter spp. isolates become resistant to third-generation cephalosporins, penicillins, and fluoroquinolones [
6,
9].
Over the whole study period, we observed significant increasing and decreasing trends in antibiotic resistance rates of
E. cloacae and
K. aerogenes (
E. aerogenes) clinical isolates among both inpatients and outpatients. Considering the comparison between the periods of 2000–2009 and 2011–2020, the overall resistance rates of
E. cloacae strains increased for fosfomycin, in both community and hospital-related infections, whereas they decreased for fluoroquinolones and aminoglycosides, principally in the hospitalized population. On the other hand, the overall resistance rates of
K. aerogenes (
E. aerogenes) strains increased for Fosfomycin in both groups, increased for aminoglycosides and third-generation cephalosporins in the hospitalized population, and decreased for fluoroquinolones in both outpatients and inpatients. Our data agree with the Italian surveillance report 2015–2021, which described that, among Enterobacterales, particularly
Escherichia coli, antimicrobial resistance trends decreased for fluoroquinolones and aminoglycosides [
17]. Moreover, the European surveillance report of antimicrobial resistance in the same period described that the highest EU/EEA resistance percentages in
Escherichia coli were observed for aminopenicillins, followed by fluoroquinolones, cephalosporins, and aminoglycosides, although their trends significantly decreased [
18]. The differences observed between the hospitalized population and outpatients were most probably due to the different antimicrobial treatments used in hospital compared with those administered in community, as most of the
E. cloacae and
K. aerogenes (
E. aerogenes) strains isolated in the hospital were resistant to more than one class of antibiotic. The antimicrobials most commonly administered in
Enterobacter infections include fourth-generation cephalosporins, such as cefepime and cefpirome; carbapenems, which seem more effective, even if the use of carbapenems should be rigorously restricted; the piperacillin–tazobactam combination, which presents good treatment results; and aminoglycosides, particularly amikacin, which remain active against more than 95% of
Enterobacter strains, according to the Infectious Diseases Society of America (IDSA) guidelines [
6,
9,
19,
20].
In Italy, fluoroquinolones were the most common antibiotic prescribed in 2019, particularly in the treatment of UTI, preceded only by β-lactams and macrolides [
21]. In 2018, the European Medicines Agency (EMA) restricted the usage of fluoroquinolone-containing antibiotics, such as ciprofloxacin, owing to severe, disabling, and potentially permanent side effects, in accordance to following the Pharmacovigilance Risk Assessment Committee (PRAC) recommendations [
22]. In 2019, Italy followed these recommendations and our data confirmed the decreasing resistance trends for fluoroquinolones due to a probable diminished clinical usage. As a consequence, the greater administration of aminoglycosides, cephalosporins, and particularly fosfomycin increased the resistance rates to these drugs in
Enterobacter infections. Fosfomycin, also known as Monuril
® or Monurol
®, is an antibiotic used to treat complicated and uncomplicated UTI and, because most of our samples are infections of the urinary tract, the increasing trend observed was most likely due to an uncontrolled and inappropriate usage. Therefore, our data highlight the importance to follow national and international guidelines in the prudent use of antimicrobials in human health [
23]. Moreover, a strong modulation and adequate antimicrobial therapy based on patient’s clinical situation, as well as more attention to the different routes of transmission, which include (I) from environment to patient, (II) from colonized patients to the environment, and (III) between patients, are needed.
Reviewing the literature, our data agreed with the results obtained in other studies, including the increased fosfomycin resistance, as detected in
E cloacae strains by Jimenez-Guerra and coauthors [
12]; the low carbapenem resistance, particularly imipenem, as also described by Jimenez-Guerra and coauthors and Al-Tawfiq and coauthors in
Enterobacter spp. [
10,
12]; and high resistance rates to cephalosporins, both third- and four generations, as reported by Quraishi and coauthors [
9]. However, Quraishi and coauthors found a percentage of resistance of
Enterobacter to meropenem of 22%, which disagreed with our results concerning carbapenem non-susceptibility [
9]. Carbapenems are the antibiotics used as the first line against strains that produce AmpC beta lactamases, and a high percentage of resistance could be due to possible excessive use in treatments, as previously described [
9,
10,
12]. Moreover, Al-Tawfiq and coauthors observed that nosocomial
E. cloacae and
E. aerogenes isolates were statistically more resistant compared with those identified in outpatients, a result similar to our data [
10]. As we reported an increased trend of fosfomycin resistance due to inappropriate use in urinary infection, Adhikari and coauthors also described that, in Iran, most urinary
Enterobacter isolates were resistant to nitrofurantoin, which was incorrectly used to treat these types of infections without an analysis of susceptibility patterns [
9].
In this study, 111 bacterial strains were identified as
Enterobacter spp. using commercialized systems, such as Vitek 1 and 2, based on biochemical tests, and Vitek MALDI-TOF MS, based on mass spectrometry. These techniques present limitations in species’ identification, particularly within the
E. cloacae complex and between
E. hormaechei,
E. cloacae,
E. asburiae,
E. kobei, and
E. ludwigii, owing to the high similarity between them [
6]. A precise identification of the species is important for correct antibiotic therapy and misidentifications could have a negative impact on patient outcomes. Molecular biology methods, such as sequencing of 16S rRNA, real-time PCR, and microarray comparative genomic hybridization, are able to identify the species exactly, but these are time-consuming, expensive, and difficult to perform routinely in the laboratory [
6].
Our study presents a few limitations that should be considered: (A) the work is retrospective and was performed in a single centre; (B) the lack of clinical data cannot provide a more comprehensive representation of resistance trends; and (C) the unavailability of the previous antimicrobial therapies.


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}