
Trends in Antimicrobial Resistance of Uropathogens Isolated from Urinary Tract Infections in a Tertiary Care Hospital in Dhaka, Bangladesh

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Results
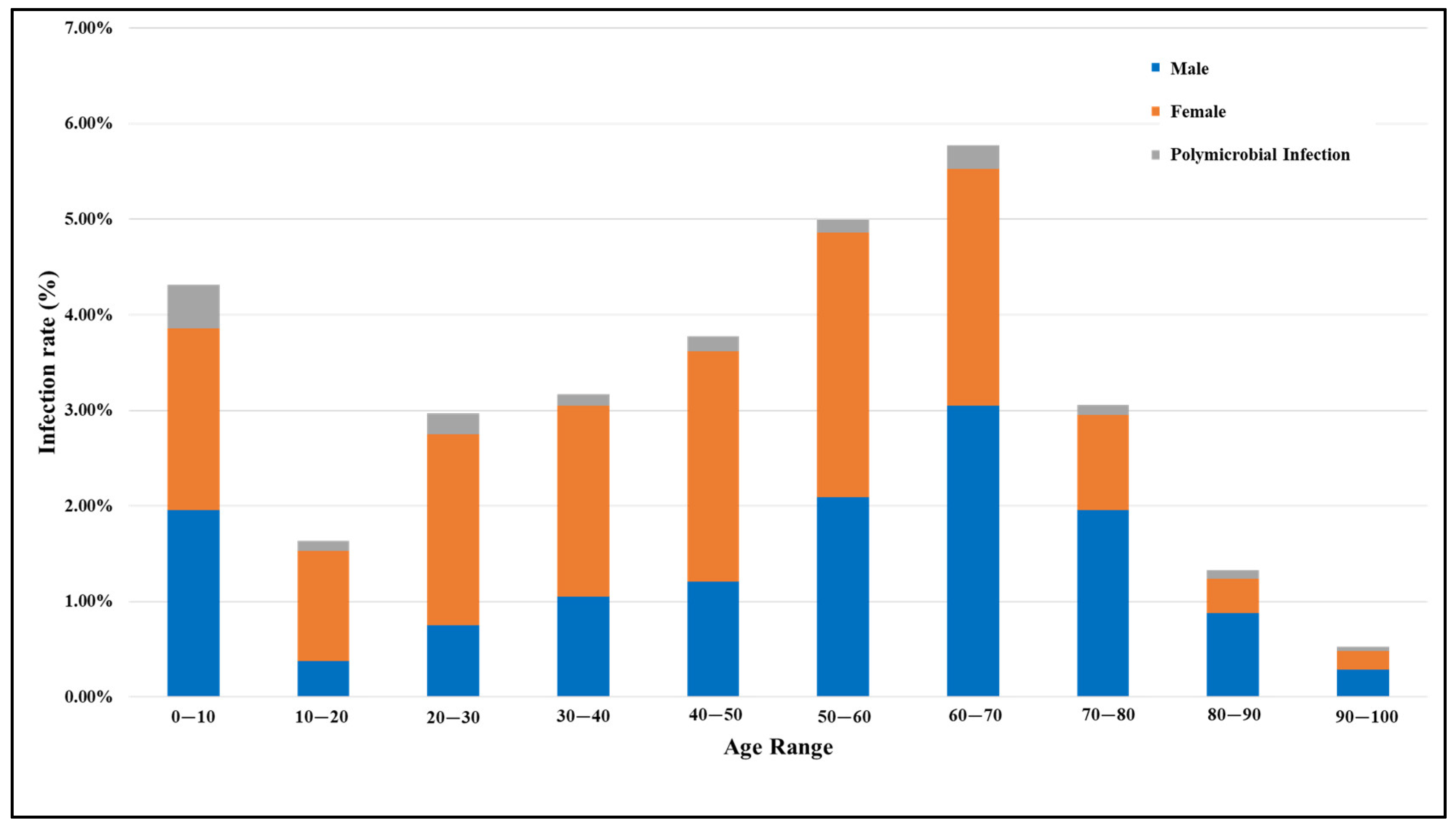
2.1. Prevalence of UTI According to Age and Gender
2.2. Microbiological Profile of Uropathogens
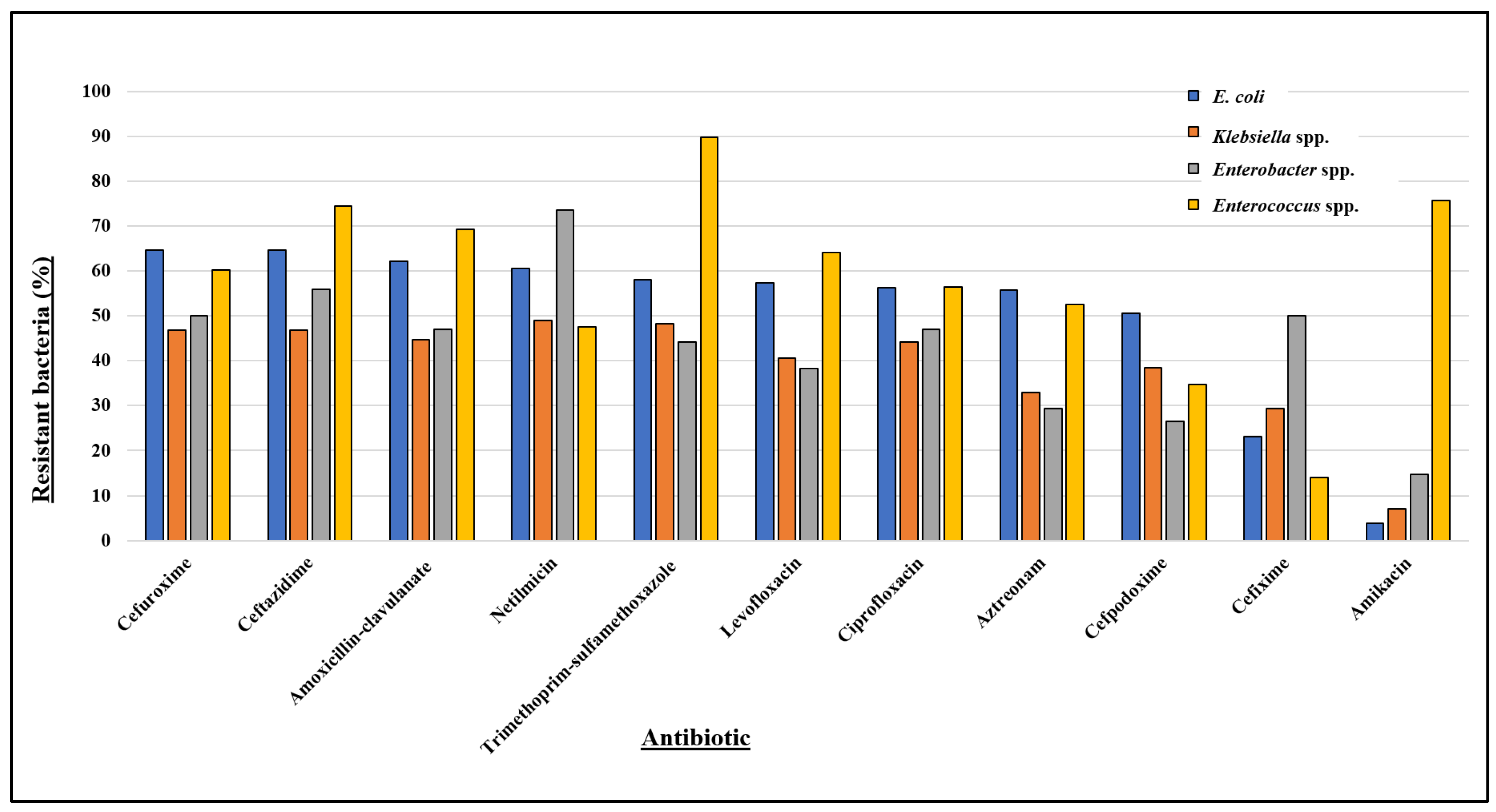
2.3. Antibiotic Resistance Patterns and Trends in Bacterial Uropathogens
2.3.1. E. coli
2.3.2. Klebsiella spp.
2.3.3. Enterobacter spp.
2.3.4. Enterococcus spp.
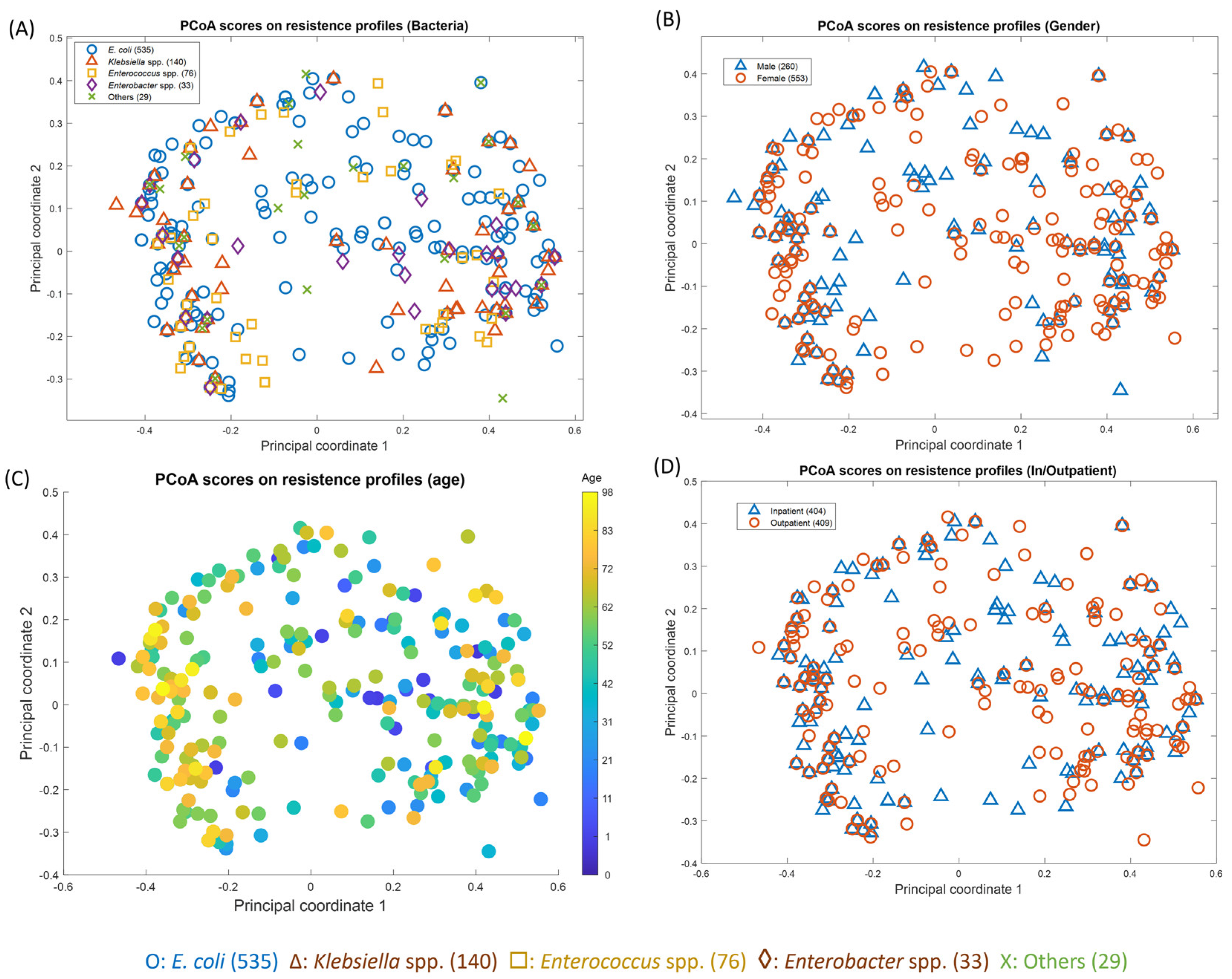
2.4. Principal Coordinate Analysis (PCoA) of Antibiotic Resistance and Patient Factors
3. Discussion
3.1. Higher Prevalence of UTIs among Females
3.2. Age-Related UTI Susceptibility in Men and Women
3.3. UTI Incidence and Polymicrobial Infection in Pediatric Populations
3.4. Fungal UTIs
3.5. Gram-Positive Uropathogenic Bacteria
3.6. Gram-Negative Uropathogenic Bacteria
3.7. Prevalence of E. coli and Klebsiella spp. as Predominant Uropathogens
3.8. E. coli and Klebsiella spp.—Resistance towards Cephalosporins and Multidrug Resistance
3.9. Susceptibility of E. coli and Klebsiella spp. to Amikacin
3.10. Contributing Factors to the Soaring Antibiotic Resistance
3.11. Limitations of the Study
4. Materials and Methods
4.1. Sample Collection
4.2. Sample Processing
4.3. Antimicrobial Susceptibility Testing
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Foxman, B. Urinary tract infection syndromes: Occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect. Dis. Clin. 2014, 28, 1–13. [Google Scholar] [CrossRef]
- Sabih, A.; Leslie, S.W. Complicated Urinary Tract Infections. 2017. Available online: https://www.ncbi.nlm.nih.gov/books/NBK436013/ (accessed on 12 November 2023).
- Wilson, M.L.; Gaido, L. Laboratory Diagnosis of Urinary Tract Infections in Adult Patients. Clin. Infect. Dis. 2004, 38, 1150–1158. [Google Scholar] [CrossRef] [PubMed]
- Klumpp, D.J.; Rycyk, M.T.; Chen, M.C.; Thumbikat, P.; Sengupta, S.; Schaeffer, A.J. Uropathogenic Escherichia coli induces extrinsic and intrinsic cascades to initiate urothelial apoptosis. Infect. Immun. 2006, 74, 5106–5113. [Google Scholar] [CrossRef] [PubMed]
- Beyene, G.; Tsegaye, W. Bacterial uropathogens in urinary tract infection and antibiotic susceptibility pattern in jimma university specialized hospital, southwest ethiopia. Ethiop. J. Health Sci. 2011, 21, 141–146. [Google Scholar] [CrossRef]
- Haque, R.; Akter, M.L.; Salam, M.A. Prevalence and susceptibility of uropathogens: A recent report from a teaching hospital in Bangladesh. BMC Res. Notes 2015, 8, 416. [Google Scholar] [CrossRef]
- Zagaglia, C.; Ammendolia, M.G.; Maurizi, L.; Nicoletti, M.; Longhi, C. Urinary tract infections caused by uropathogenic Escherichia coli strains—New strategies for an old pathogen. Microorganisms 2022, 10, 1425. [Google Scholar] [CrossRef]
- Singhal, A.; Sharma, R.; Jain, M.; Vyas, L. Hospital and community isolates of uropathogens and their antibiotic sensitivity pattern from a tertiary care hospital in North West India. Ann. Med. Health Sci. Res. 2014, 4, 51–56. [Google Scholar] [CrossRef]
- Mosharraf, F.B.; Chowdhury, S.S.; Ahmed, A.; Hossain, M.M. A Comparative Study of Static Biofilm Formation and Antibiotic Resistant Pattern between Environmental and Clinical Isolate of Pseudomonas aeruginosa. Adv. Microbiol. 2020, 10, 663–672. [Google Scholar] [CrossRef]
- Pouwels, K.B.; Hopkins, S.; Llewelyn, M.J.; Walker, A.S.; McNulty, C.A.; Robotham, J.V. Duration of antibiotic treatment for common infections in English primary care: Cross sectional analysis and comparison with guidelines. BMJ 2019, 364. [Google Scholar] [CrossRef]
- Patangia, D.V.; Anthony Ryan, C.; Dempsey, E.; Paul Ross, R.; Stanton, C. Impact of antibiotics on the human microbiome and consequences for host health. Microbiologyopen 2022, 11, e1260. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.A.; Islam, M.R.; Khan, R.; Amin, M.B.; Rahman, M.; Hossain, M.I.; Ahmed, D.; Asaduzzaman, M.; Riley, L.W. Prevalence, etiology and antibiotic resistance patterns of community-acquired urinary tract infections in Dhaka, Bangladesh. PLoS ONE 2022, 17, e0274423. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Chowdhury, O.A.; Hoque, M.M.; Hoque, S.A.; Chowdhury, S.M.R.; Rahman, M.A. Antimicrobial Resistance Pattern of Uropathogenic Escherichia coli and Klebsiella species Isolated in a Tertiary Care Hospital of Sylhet. Med. Today 2018, 30, 61–66. [Google Scholar] [CrossRef]
- Alkhawaldeh, R.; Abu Farha, R.; Abu Hammour, K.; Alefishat, E. Optimizing antimicrobial therapy in urinary tract infections: A focus on urine culture and sensitivity testing. Front. Pharmacol. 2022, 13, 1058669. [Google Scholar] [CrossRef] [PubMed]
- Mihankhah, A.; Khoshbakht, R.; Raeisi, M.; Raeisi, V. Prevalence and antibiotic resistance pattern of bacteria isolated from urinary tract infections in Northern Iran. J. Res. Med. Sci. 2017, 22, 108. [Google Scholar] [CrossRef] [PubMed]
- Setu, S.K.; Sattar, A.N.I.; Saleh, A.A.; Roy, C.K.; Ahmed, M.; Muhammadullah, S.; Kabir, M.H. Study of Bacterial pathogens in Urinary Tract Infection and their antibiotic resistance profile in a tertiary care hospital of Bangladesh. Bangladesh J. Med. Microbiol. 2016, 10, 22–26. [Google Scholar] [CrossRef]
- Al-Badr, A.; Al-Shaikh, G. Recurrent urinary tract infections management in women: A review. Sultan Qaboos Univ. Med. J. 2013, 13, 359. [Google Scholar] [CrossRef]
- Dougherty, J.M.; Leslie, S.W.; Aeddula, N.R. Male Urinary Retention: Acute and Chronic. 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK538499/ (accessed on 20 April 2024).
- Oli, A.N.; Akabueze, V.B.; Ezeudu, C.E.; Eleje, G.U.; Ejiofor, O.S.; Ezebialu, I.U.; Oguejiofor, C.B.; Ekejindu, I.M.; Emechebe, G.O.; Okeke, K.N. Bacteriology and antibiogram of urinary tract infection among female patients in a tertiary health facility in south eastern Nigeria. Open Microbiol. J. 2017, 11, 292. [Google Scholar] [CrossRef]
- Veeraraghavan, B.; Jesudason, M.R.; Prakasah, J.A.J.; Anandan, S.; Sahni, R.D.; Pragasam, A.K.; Bakthavatchalam, Y.D.; Selvakumar, R.J.; Dhole, T.; Rodrigues, C. Antimicrobial susceptibility profiles of gram-negative bacteria causing infections collected across India during 2014–2016: Study for monitoring antimicrobial resistance trend report. Indian J. Med. Microbiol. 2018, 36, 32–36. [Google Scholar] [CrossRef]
- Musa-Aisien, A.; Ibadin, O.; Ukoh, G.; Akpede, G. Prevalence and antimicrobial sensitivity pattern in urinary tract infection in febrile under-5s at a children’s emergency unit in Nigeria. Ann. Trop. Paediatr. 2003, 23, 39–45. [Google Scholar] [CrossRef]
- Nuutinen, M.; Uhari, M. Recurrence and follow-up after urinary tract infection under the age of 1 year. Pediatr. Nephrol. 2001, 16, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Mishra, M.P.; Sarangi, R.; Padhy, R.N. Prevalence of multidrug resistant uropathogenic bacteria in pediatric patients of a tertiary care hospital in eastern India. J. Infect. Public Health 2016, 9, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.L.; Finlay, J.C.; Lang, M.E.; Bortolussi, R.; Society, C.P.; Committee, C.P.; Diseases, I.; Committee, I. Urinary tract infection in infants and children: Diagnosis and management. Paediatr. Child Health 2014, 19, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Behzadi, P.; Behzadi, E. The microbial agents of urinary tract infections at central laboratory of Dr. Shariati Hospital, Tehran, Iran. Turk Klin Tip Bilim 2008, 28, 445. [Google Scholar]
- Behzadi, P.; Behzadi, E.; Yazdanbod, H.; Aghapour, R.; Cheshmeh, M.A.; Omran, D.S. Urinary tract infections associated with Candida albicans. Maedica 2010, 5, 277. [Google Scholar]
- Helbig, S.; Achkar, J.; Jain, N.; Wang, X.; Gialanella, P.; Levi, M.; Fries, B. Diagnosis and inflammatory response of patients with candiduria. Mycoses 2013, 56, 61–69. [Google Scholar] [CrossRef]
- Behzadi, P.; Behzadi, E.; Ranjbar, R. Urinary tract infections and Candida albicans. Cent. Eur. J. Urol. 2015, 68, 96. [Google Scholar] [CrossRef]
- Maillet, F.; Passeron, A.; Podglajen, I.; Ranque, B.; Pouchot, J. Lactobacillus delbrueckii urinary tract infection in a male patient. Médecine Et Mal. Infect. 2019, 49, 226–228. [Google Scholar] [CrossRef]
- Darbro, B.W.; Petroelje, B.K.; Doern, G.V. Lactobacillus delbrueckii as the cause of urinary tract infection. J. Clin. Microbiol. 2009, 47, 275–277. [Google Scholar] [CrossRef]
- Malmartel, A.; Ghasarossian, C. Epidemiology of urinary tract infections, bacterial species and resistances in primary care in France. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 447–451. [Google Scholar] [CrossRef]
- Codelia-Anjum, A.; Lerner, L.B.; Elterman, D.; Zorn, K.C.; Bhojani, N.; Chughtai, B. Enterococcal urinary tract infections: A review of the pathogenicity, epidemiology, and treatment. Antibiotics 2023, 12, 778. [Google Scholar] [CrossRef] [PubMed]
- Das, R.; Chandrashekhar, T.; Joshi, H.; Gurung, M.; Shrestha, N.; Shivananda, P. Frequency and susceptibility profile of pathogens causing urinary tract infections at a tertiary care hospital in western Nepal. Singap. Med. J. 2006, 47, 281. [Google Scholar]
- Shakya, S.; Edwards, J.; Gupte, H.; Shrestha, S.; Shakya, B.; Parajuli, K.; Kattel, H.; Shrestha, P.; Ghimire, R.; Thekkur, P. High multidrug resistance in urinary tract infections in a tertiary hospital, Kathmandu, Nepal. Public Health Action 2021, 11, 24–31. [Google Scholar] [CrossRef]
- Dasgupta, C.; Rafi, M.A.; Salam, M.A. High prevalence of multidrug resistant uropathogens: A recent audit of antimicrobial susceptibility testing from a tertiary care hospital in Bangladesh. Pak. J. Med. Sci. 2020, 36, 1297. [Google Scholar] [CrossRef]
- Mohapatra, S.; Panigrahy, R.; Tak, V.; JV, S.; KC, S.; Chaudhuri, S.; Pundir, S.; Kocher, D.; Gautam, H.; Sood, S. Prevalence and resistance pattern of uropathogens from community settings of different regions: An experience from India. Access Microbiol. 2022, 4, 000321. [Google Scholar] [CrossRef]
- Sugianli, A.K.; Ginting, F.; Parwati, I.; de Jong, M.D.; van Leth, F.; Schultsz, C. Antimicrobial resistance among uropathogens in the Asia-Pacific region: A systematic review. JAC-Antimicrob. Resist. 2021, 3, dlab003. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, S.; Saud, B.; Paudel, G.; Bajracharya, D. Emergence of antimicrobial drug resistant bacteria in Nepal: A current scenario. PBCR 2019, 1, 31–33. [Google Scholar]
- Shakya, P.; Shrestha, D.; Maharjan, E.; Sharma, V.K.; Paudyal, R. ESBL production among E. coli and Klebsiella spp. causing urinary tract infection: A hospital based study. Open Microbiol. J. 2017, 11, 23. [Google Scholar] [CrossRef]
- Baral, P.; Neupane, S.; Marasini, B.P.; Ghimire, K.R.; Lekhak, B.; Shrestha, B. High prevalence of multidrug resistance in bacterial uropathogens from Kathmandu, Nepal. BMC Res. Notes 2012, 5, 38. [Google Scholar] [CrossRef]
- Iqbal, Z.; Mumtaz, M.Z.; Malik, A. Extensive drug-resistance in strains of Escherichia coli and Klebsiella pneumoniae isolated from paediatric urinary tract infections. J. Taibah Univ. Med. Sci. 2021, 16, 565–574. [Google Scholar] [CrossRef]
- Jalil, M.B.; Al Atbee, M.Y.N. The prevalence of multiple drug resistance Escherichia coli and Klebsiella pneumoniae isolated from patients with urinary tract infections. J. Clin. Lab. Anal. 2022, 36, e24619. [Google Scholar] [CrossRef] [PubMed]
- Shams, F.; Hasani, A.; Pormohammad, A.; Rezaee, M.A.; Reza, M.; Nahaie, A.H.; Haghi, M.H.S.B.; Gholizade, P.; Arbatan, A.E. qnrA implicated quinolone resistance in Escherichia coli and Klebsiella pneumoniae clinical isolates from a University Teaching Hospital. Life Sci. J. 2014, 11, 1032–1035. [Google Scholar]
- Kang, K.T.; Ng, K.; Kendrick, J.; Tilley, P.; Ting, J.; Rassekh, S.; Murthy, S.; Roberts, A. Third-generation cephalosporin-resistant urinary tract infections in children presenting to the paediatric emergency department. Paediatr. Child Health 2020, 25, 166–172. [Google Scholar] [CrossRef]
- Kothari, A.; Sagar, V. Antibiotic resistance in pathogens causing community-acquired urinary tract infections in India: A multicenter study. J. Infect. Dev. Ctries. 2008, 2, 354–358. [Google Scholar] [CrossRef]
- Fasugba, O.; Mitchell, B.G.; Mnatzaganian, G.; Das, A.; Collignon, P.; Gardner, A. Five-year antimicrobial resistance patterns of urinary Escherichia coli at an Australian tertiary hospital: Time series analyses of prevalence data. PLoS ONE 2016, 11, e0164306. [Google Scholar] [CrossRef]
- Hossain, M.D.; Ahsan, S.; Kabir, M.S. Antibiotic resistance patterns of uropathogens isolated from catheterized and noncatheterized patients in Dhaka, Bangladesh. Tzu Chi Med. J. 2014, 26, 127–131. [Google Scholar] [CrossRef]
- Lee, H.; Yoon, E.-J.; Kim, D.; Jeong, S.H.; Won, E.J.; Shin, J.H.; Kim, S.H.; Shin, J.H.; Shin, K.S.; Kim, Y.A. Antimicrobial resistance of major clinical pathogens in South Korea, May 2016 to April 2017: First one-year report from Kor-GLASS. Eurosurveillance 2018, 23, 1800047. [Google Scholar] [CrossRef]
- Turnidge, J.D.; Gottlieb, T.; Mitchell, D.H.; Coombs, G.W.; Daly, D.A.; Bell, J.M.; Australian Group on Antimicrobial Resistance. Community-onset Gram-negative Surveillance Program annual report, 2012. Commun. Dis. Intell. Q. Rep. 2014, 38, E54–E58. [Google Scholar]
- Jancel, T.; Dudas, V. Management of uncomplicated urinary tract infections. West. J. Med. 2002, 176, 51. [Google Scholar] [CrossRef]
- Devi, A.; Rajkumar, J. A study on antibiotic susceptibility and resistance profiles of bacterial strains isolated from patients with urinary tract infection (UTI) at Kanchipuram District, Tamilnadu, India. Int. J. Pharm. Pharm. Sci. 2013, 5, 817–820. [Google Scholar] [CrossRef]
- Cho, S.-Y.; Choi, S.-M.; Park, S.H.; Lee, D.-G.; Choi, J.-H.; Yoo, J.-H. Amikacin therapy for urinary tract infections caused by extended-spectrum β-lactamase-producing Escherichia coli. Korean J. Intern. Med. 2016, 31, 156. [Google Scholar] [CrossRef] [PubMed]
- Do, N.T.; Vu, H.T.; Nguyen, C.T.; Punpuing, S.; Khan, W.A.; Gyapong, M.; Asante, K.P.; Munguambe, K.; Gómez-Olivé, F.X.; John-Langba, J. Community-based antibiotic access and use in six low-income and middle-income countries: A mixed-method approach. Lancet Glob. Health 2021, 9, e610–e619. [Google Scholar] [CrossRef] [PubMed]
- Biswas, M.; Roy, D.N.; Tajmim, A.; Rajib, S.S.; Hossain, M.; Farzana, F.; Yasmen, N. Prescription antibiotics for outpatients in Bangladesh: A cross-sectional health survey conducted in three cities. Ann. Clin. Microbiol. Antimicrob. 2014, 13, 15. [Google Scholar] [CrossRef] [PubMed]
- MacFaddin, J.F. Biochemical Tests for Identification of Medical Bacteria; Lippinccot, Williams & Williams: Baltimore, MD, USA, 2000. [Google Scholar]
- Forbes, B.A.; Sahm, D.F.; Weissfeld, A.S. Diagnostic Microbiology; Mosby: St Louis, MO, USA, 2007. [Google Scholar]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, 27th ed.; CLSI Document M100; CLSI: Wayne, PA, USA, 2017. [Google Scholar]
- Borg, I.; Groenen, P.J. Modern Multidimensional Scaling: Theory and Applications; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2005. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total UTI Suspected Cases (n = 6549) | Infection Rate 1 (%) | |||
|---|---|---|---|---|
| Male | Female | |||
| 2392 | 4257 | |||
| Total UTI Cases (n = 1001) | ||||
| Age Range | Male | Female | Male | Female |
| 0–10 | 47 | 79 | 1.96% | 1.90% |
| 10–20 | 9 | 48 | 0.38% | 1.15% |
| 20–30 | 18 | 83 | 0.75% | 2.00% |
| 30–40 | 25 | 83 | 1.05% | 2.00% |
| 40–50 | 29 | 100 | 1.21% | 2.41% |
| 50–60 | 50 | 115 | 2.09% | 2.77% |
| 60–70 | 73 | 103 | 3.05% | 2.48% |
| 70–80 | 47 | 41 | 1.96% | 0.99% |
| 80–90 | 21 | 15 | 0.88% | 0.36% |
| 90–100 | 7 | 8 | 0.29% | 0.19% |
| Total | 326 | 675 | 13.62% | 16.25% |
| Uropathogens | Frequency of Culture-Positive Isolates | Frequency of 1 MDR Isolates | 1 MDR Prevalence (%) of the Isolates |
|---|---|---|---|
| E. coli | 544 | 402 | 73.90 |
| Klebsiella spp. | 143 | 70 | 48.95 |
| Enterobacter spp. | 34 | 24 | 70.59 |
| Pseudomonas spp. | 9 | 9 | 100.00 |
| Proteus spp. | 8 | 5 | 62.50 |
| Acinetobacter spp. | 5 | 3 | 60.00 |
| Acetobacter spp. | 2 | 1 | 50.00 |
| Citrobacter spp. | 1 | 1 | 100.00 |
| Morganella morganii | 1 | 1 | 100.00 |
| Enterococcus spp. | 78 | 74 | 94.87 |
| Staphylococcus aureus | 7 | 2 | 28.57 |
| Lactobacillus spp. | 1 | 1 | 100.00 |
| Total | 833 | 593 | 71.19 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chowdhury, S.S.; Tahsin, P.; Xu, Y.; Mosaddek, A.S.M.; Muhamadali, H.; Goodacre, R. Trends in Antimicrobial Resistance of Uropathogens Isolated from Urinary Tract Infections in a Tertiary Care Hospital in Dhaka, Bangladesh. Antibiotics 2024, 13, 925. https://doi.org/10.3390/antibiotics13100925
Chowdhury SS, Tahsin P, Xu Y, Mosaddek ASM, Muhamadali H, Goodacre R. Trends in Antimicrobial Resistance of Uropathogens Isolated from Urinary Tract Infections in a Tertiary Care Hospital in Dhaka, Bangladesh. Antibiotics. 2024; 13(10):925. https://doi.org/10.3390/antibiotics13100925
Chicago/Turabian StyleChowdhury, Sara Sadia, Promi Tahsin, Yun Xu, Abu Syed Md. Mosaddek, Howbeer Muhamadali, and Royston Goodacre. 2024. "Trends in Antimicrobial Resistance of Uropathogens Isolated from Urinary Tract Infections in a Tertiary Care Hospital in Dhaka, Bangladesh" Antibiotics 13, no. 10: 925. https://doi.org/10.3390/antibiotics13100925