
Risk of Children’s Dermal Exposure to Galaxolide through Personal Care Products

Abstract
:
1. Introduction

2. Experimental Section
2.1. Questionnaire
2.2. Chemicals and Samples
2.3. Extraction and Analytical Method
2.4. Blank Issues/Quality Assurance
3. Results and Discussion
3.1. Questionnaire
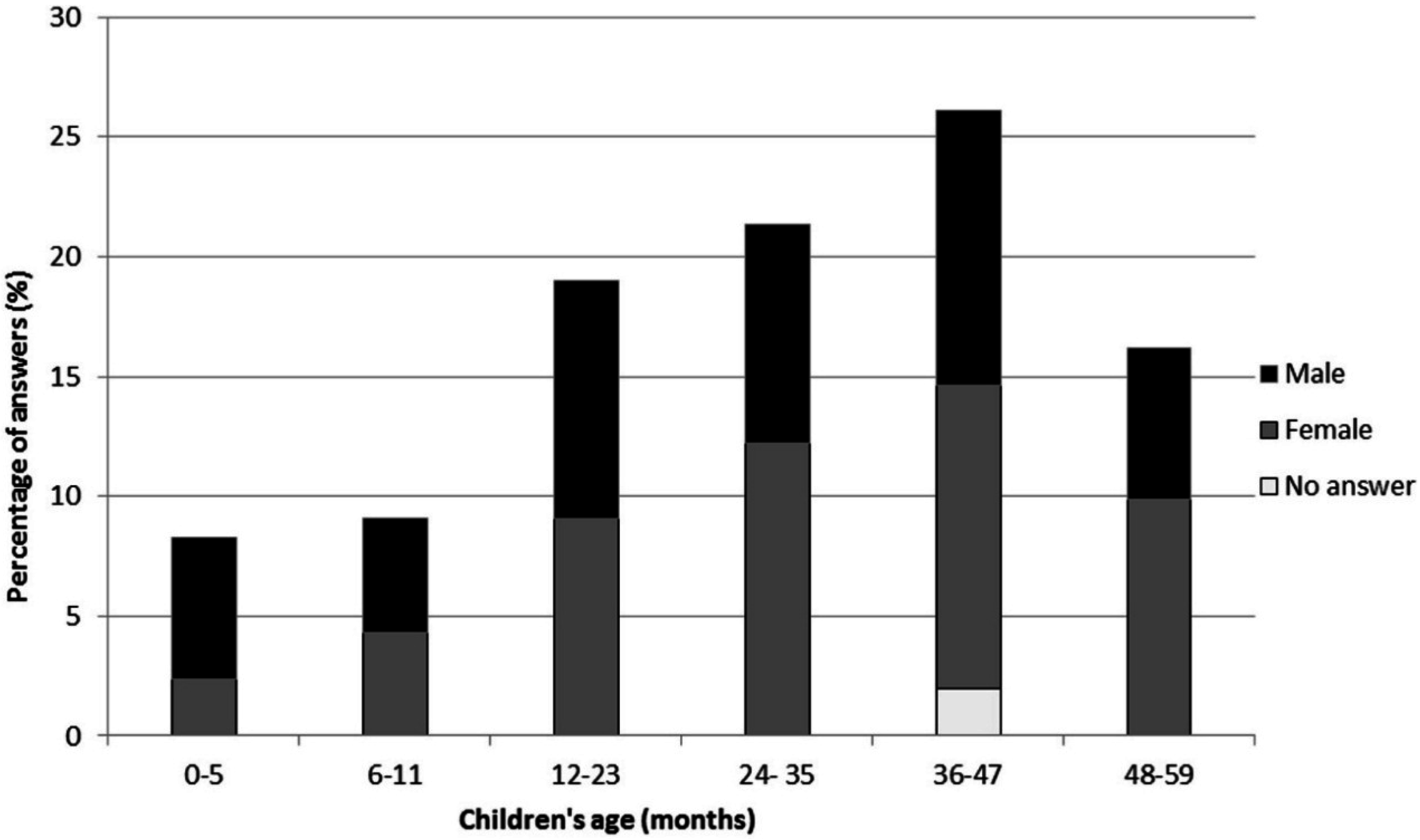
3.1.1. Social-Demographic Characterization of Children and Families
Children Characterization

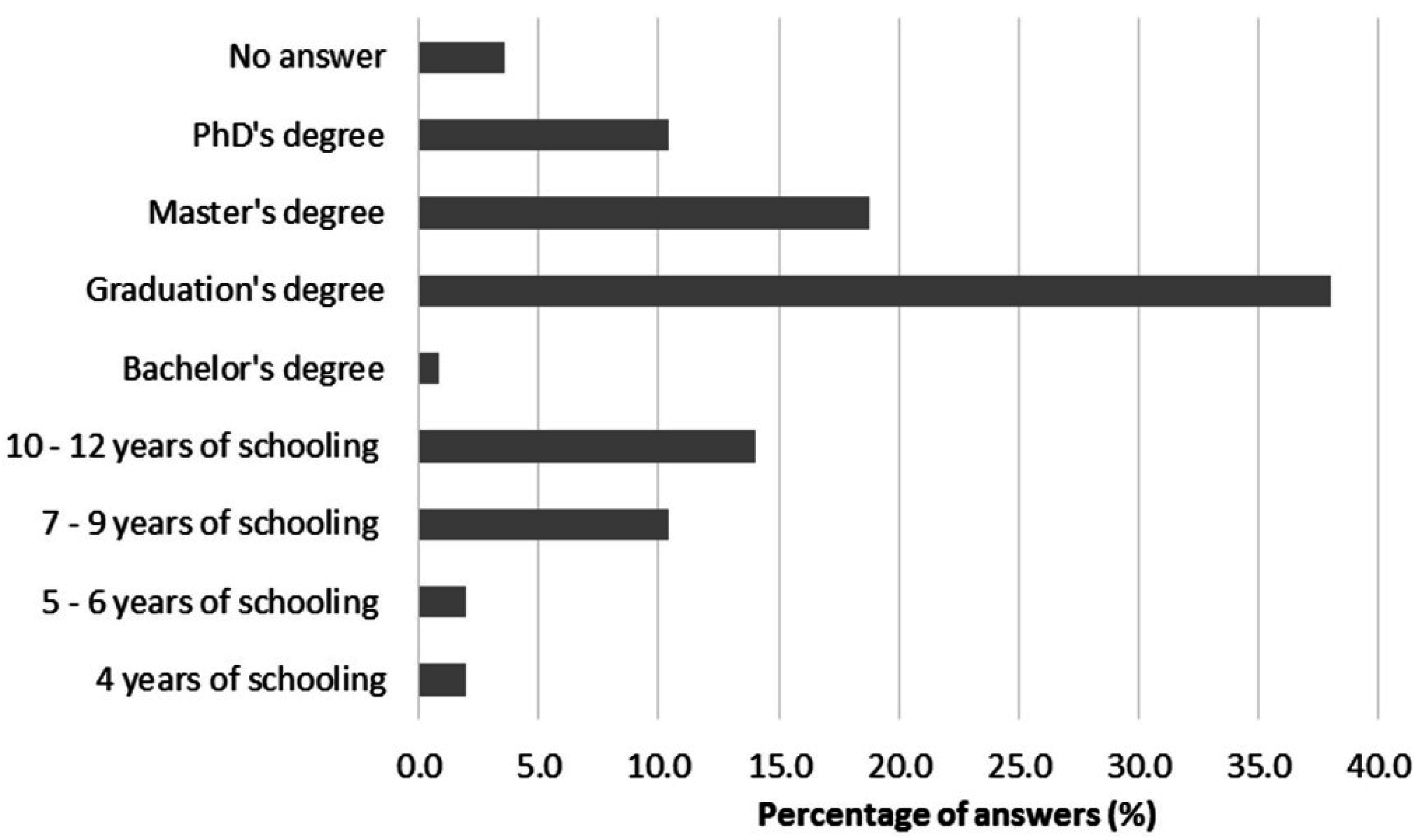
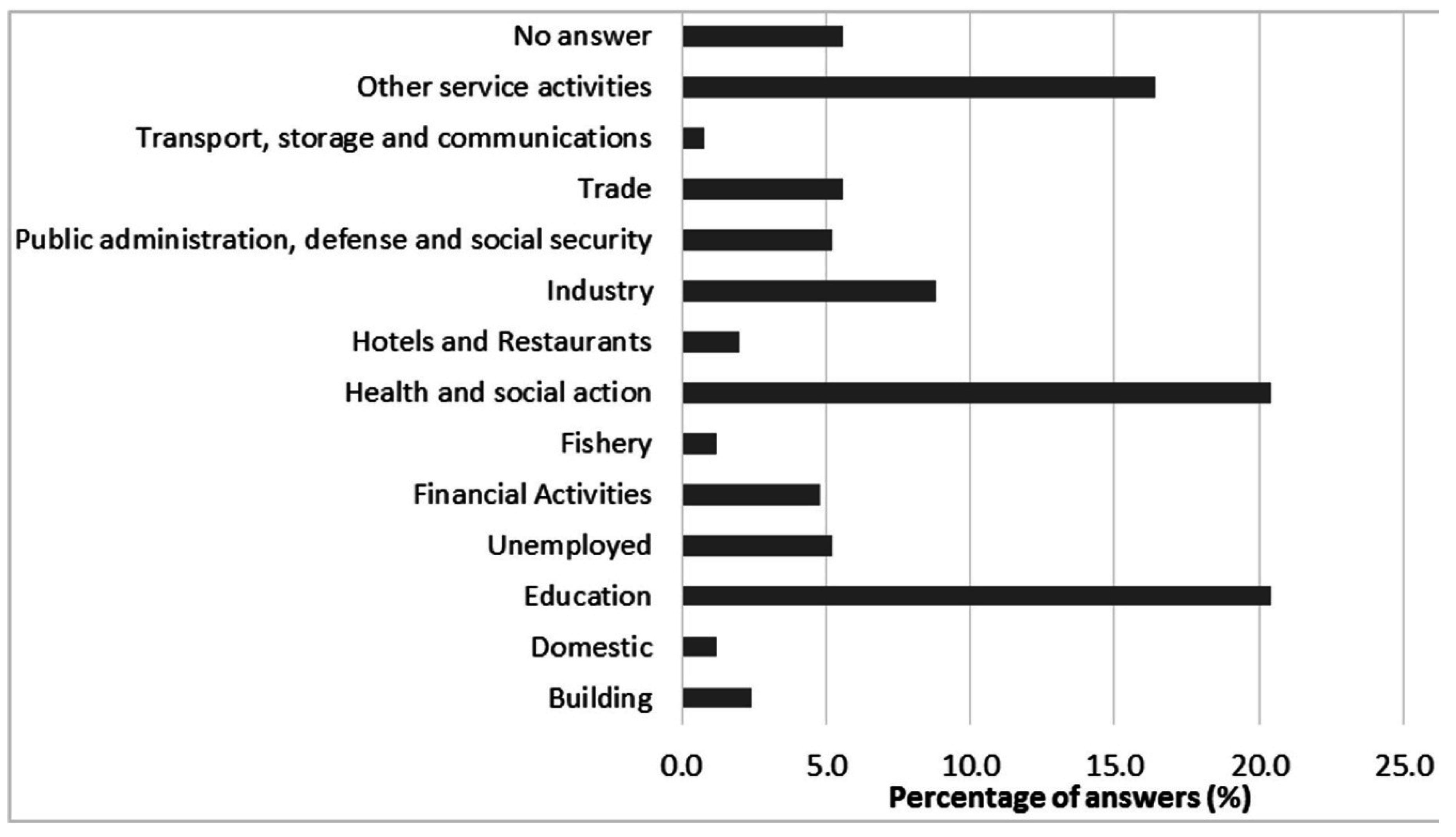
Caregivers and Families’ Characterizations


3.1.2. Consumer Habits

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Moisturizer | Toothpaste | Bath Gel/Soap | Shampoo | Hair Conditioner | Diaper Change Hygiene | Diaper Change Cream | Sunscreen |
|---|---|---|---|---|---|---|---|---|
| Frequency of utilization | Once a day (53%) | Two times a day (46%) | Once a day (68%) | Once a day (41%) | Once a day (10%) | Five times a day (mean) | Five times a day (mean) | Three times a day * (mean) |
| Applied amount | Thick layer (81%) | Nail of the little finger (60%) | A walnut of product (74%) | A walnut of product (94%) | A walnut of product (18%) | More than a wet wipe (43%) | Thick layer (39%) | Thick layer (51%) |
| Site of application | Face (93%) | Teeth and tongue (53%) | Wet skin (81%) | Wet scalp (92%) | Hair tips (22%) | Genital area (43%) | Irritated skin (40%) | All over the body (66%) |
| PCP Type | PCP Code | PCP Utilization (%) | HHCB Concentration (mg·kg−1 Sample) | PCP Presentation |
|---|---|---|---|---|
| Moisturizers (N = 70) | M1LC1 | 0.3 | 0.098 ± 0.007 | Lotion |
| M2CC1 | 0.5 | 0.022 ± 0.009 | Cream | |
| M3LC2 | 0.8 | 414.855 ± 0.016 | Lotion | |
| M4CC2 | 0.8 | 0.220 ± 0.009 | Cream | |
| M5CR1 | 1.8 | 0.024 ± 0.007 | Cream | |
| M2CC3 | 1.8 | 0.169 ± 0.010 | Cream | |
| M6CC4 | 2.1 | 0.362 ± 0.012 | Cream | |
| M2CC5 | 2.6 | 0.018 ± 0.011 | Cream | |
| M7LC3 | 3.2 | 0.032 ± 0.009 | Lotion | |
| M2CR2 | 3.9 | 0.034 ± 0.007 | Cream | |
| M7LC4 | 4.7 | 0.406 ± 0.010 | Lotion | |
| M2CC6 | 4.7 | 0.058 ± 0.007 | Cream | |
| M8CC7 | 5.0 | nd | Cream | |
| M5CC8 | 6.1 | 0.020 ± 0.011 | Cream | |
| M9CC9 | 7.4 | 0.013 ± 0.011 | Cream | |
| M4CR3 | 7.4 | 105.397 ± 0.030 | Cream | |
| M4LC5 | 11.3 | 184.174 ± 0.034 | Lotion | |
| M2LC6 | 15.0 | nd | Lotion | |
| M5LC7 | a | 0.031 ± 0.010 | Lotion | |
| M5LC8 | a | 0.023 ± 0.011 | Lotion | |
| M7LC9 | a | 0.114 ± 0.008 | Lotion | |
| Other PCPs (n = 49) | 20.5 | – | – | |
| No answer; Don’t Know/use | 1.1 | – | – | |
| Toothpastes (N = 24) | M10GD1 | 2.6 | nd | Gel |
| M10GD2 | 2.6 | 0.056 ± 0.001 | Gel | |
| M11PD1 | 9.8 | 0.009 ± 0.008 | Paste | |
| M12GD3 | 10.9 | nd | Gel | |
| M13GD4 | 18.9 | 0.006 ± 0.006 | Gel | |
| M14PD2 | 22.3 | 0.014 ± 0.010 | Paste | |
| M15GD5 | a | nd | Gel | |
| Other PCPs (n = 17) | 12.8 | – | – | |
| No answer; Don’t Know/use | 20.1 | – | – | |
| Body Bath Products (N = 58) | M16SB1 | 0.7 | 300.480 ± 0.017 | Soap |
| M17GB1 | 1.0 | 1.385 ± 0.033 | Gel | |
| M18SB2 | 1.0 | 0.712 ± 0.012 | Soap | |
| M7GB2 | 3.5 | 0.033 ± 0.006 | Gel | |
| M4GB3 | 4.5 | 79.718 ± 0.019 | Gel | |
| M9GB4 | 5.6 | 0.035 ± 0.007 | Gel | |
| M2SL1 | 8.0 | 0.075 ± 0.007 | Solution | |
| M4GB5 | 8.4 | 0.063 ± 0.007 | Gel | |
| M5GB6 | 9.1 | 0.025 ± 0.009 | Gel | |
| M7GB7 | 10.5 | 0.100 ± 0.009 | Gel | |
| M2GB8 | 24.0 | 0.444 ± 0.012 | Gel | |
| M1GB9 | a | 0.010 ± 0.009 | Gel | |
| M1GB10 | a | 0.068 ± 0.002 | Gel | |
| M5GB11 | a | 0.012 ± 0.010 | Gel | |
| M7GB12 | a | 0.226 ± 0.009 | Gel | |
| M3GB13 | a | 217.795 ± 0.012 | Gel | |
| Other PCPs (n = 42) | 23.3 | – | – | |
| No answer; Don’t Know/use | 0.3 | – | – | |
| Shampoos (N = 25) | M19CH1 | 1.7 | 0.038 ± 0.007 | Gel |
| M5CH2 | 10.4 | 0.193 ± 0.010 | Gel | |
| M4CH3 | 10.4 | 127.517 ± 0.030 | Gel | |
| M7CH4 | 52.2 | 0.005 ± 0.005 | Gel | |
| M1CH5 | a | 0.035 ± 0.006 | Gel | |
| M1CH6 | a | 0.796 ± 0.019 | Gel | |
| M7CH7 | a | 0.089 ± 0.008 | Gel | |
| M7CH8 | a | 0.346 ± 0.010 | Gel | |
| M7CH9 | a | 0.209 ± 0.010 | Gel | |
| Other PCPs (n = 16) | 0.9 | – | – | |
| No answer; Don’t Know/use | 24.3 | – | – | |
| Hair Conditioners (N = 8) | M20AS1 | 5.9 | 251.796 ± 0.031 | Solution |
| M7AC1 | 64.7 | 0.037 ± 0.006 | Cream | |
| M7AC2 | a | 0.017 ± 0.011 | Cream | |
| M7AS2 | a | 0.006 ± 0.006 | Solution | |
| Other PCPs (n = 4) | 23.5 | – | – | |
| No answer; Don’t Know/use | 5.9 | – | – | |
| Baby Wipes (N = 26) | M17TL1 | 0.7 | 2.675 ± 0.009 | Wet wipe |
| M7TL2 | 3.0 | nd | Wet wipe | |
| M4TL3 | 3.3 | nd | Wet wipe | |
| M8TL4 | 4.6 | 0.001 ± 0.001 | Wet wipe | |
| M21TL5 | 6.3 | 0.022 ± 0.011 | Wet wipe | |
| M22TL6 | 43.4 | 0.154 ± 0.010 | Wet wipe | |
| Other PCPs (n = 20) | 17.4 | – | – | |
| No answer; Don’t Know/use | 21.4 | – | – | |
| Diaper Change Products (N = 28) | M2CF1 | 1.1 | nd | Cream |
| M23CF2 | 1.4 | 0.012 ± 0.011 | Cream | |
| M5CF3 | 3.2 | 0.207 ± 0.008 | Cream | |
| M24PO1 | 4.9 | 1.234 ± 0.025 | Ointment | |
| M2PA1 | 5.6 | 0.016 ± 0.011 | Paste | |
| M4CF4 | 6.0 | 71.513 ± 0.010 | Cream | |
| M6PA2 | 15.1 | 0.016 ± 0.011 | Paste | |
| M23PO2 | 21.1 | nd | Ointment | |
| Other PCPs (n = 20) | 18.3 | – | – | |
| No answer; Don’t Know/use | 23.2 | – | – | |
| Sunscreens (N = 31) | M25PL1 | 5.2 | 0.074 ± 0.006 | Lotion |
| M4CM1 | 6.6 | 1.005 ± 0.023 | Paste | |
| M26PL2 | 9.0 | 12.312 ± 0.010 | Lotion | |
| M2PL3 | 9.4 | 0.051 ± 0.007 | Lotion | |
| M2CM1 | 11.5 | 0.344 ± 0.010 | Paste | |
| M27PL4 | 12.8 | 0.229 ± 0.010 | Lotion | |
| M27CM2 | 15.3 | 0.394 ± 0.011 | Paste | |
| M1PL5 | a | 134.715 ± 0.025 | Lotion | |
| Other PCPs (n = 23) | 21.9 | – | – | |
| No answer; Don’t Know/use | 8.3 | – | – |
3.2. HHCB Concentrations
| PCP Category | PCP Presentation | PCP Code | HHCB Concentration (mg·kg−1 Sample) | HHCB Concentration Spike (mg·kg−1 Sample) | HHCB Recovery (%) |
|---|---|---|---|---|---|
| Moisturizers | Lotion | M7LC3 | 0.032 ± 0.009 | 320.0 | 65 |
| Cream | M4CR3 | 105.397 ± 0.030 | 300.0 | 98 | |
| Toothpastes | Paste | M14PD2 | 0.014 ± 0.010 | 300.0 | 80 |
| Gel | M15GD5 | nd | 227.5 | 80 | |
| Body Bath Products | Soap | M16SB1 | 300.480 ± 0.017 | 227.5 | 98 |
| Solution | M2SL1 | 0.075 ± 0.007 | 230.0 | 85 | |
| Gel | M1GB9 | 0.010 ± 0.009 | 230.0 | 84 | |
| Shampoos | Gel | M4CH3 | 127.517 ± 0.030 | 300.0 | 81 |
| Hair Conditioners | Cream | M7AC2 | 0.017 ± 0.011 | 227.5 | 75 |
| Baby Wipes | Wet wipe | M17TL1 | 2.675 ± 0.009 | 227.5 | 68 |
| Diaper Change Products | Paste | M27CM2 | 0.394 ± 0.011 | 230.0 | 79 |
| Ointment | M24PO1 | 1.234 ± 0.025 | 320.0 | 70 | |
| Sunscreens | Lotion | M7LC3 | 0.032 ± 0.009 | 320.0 | 65 |
| Paste | M27CM2 | 0.394 ± 0.011 | 230.0 | 79 |
3.3. HHCB Risk of Dermal Exposure
| Personal Care Products (PCPs) | Application Site | Exposure Route | Number of Analyzed PCPs | Mean HHCB Concentration c (mg·kg−1 Sample) | Mean daily Application Amount (g·Sample·day−1) | Retention Factor (%) [21] | Mean Daily HHCB Retention (µg·day−1) |
|---|---|---|---|---|---|---|---|
| Body lotions/creams | Whole body | Dermal | 18 | 37.539 | 1.4 | 100.0% | 52.5541 |
| Facial creams | Face | Dermal | 3 | 35.152 | 0.5 | 100.0% | 17.5759 |
| Toothpastes | Perioral region and mouth mucous membranes | Dermal and oral | 7 | 0.021 | 0.2 | 10.0% | 0.0004 |
| Bath gels | Whole body | Dermal | 14 | 21.428 | 2.1 | 10.0% | 4.4998 |
| Soap bars | Hands | Dermal | 2 | 150.431 | 1.1 | 10.0% | 16.5474 |
| Shampoos | Scalp, neck and hands | Dermal | 9 | 14.359 | 0.9 | 10.0% | 1.2923 |
| Hair conditioners | Hair tips and hands | Dermal | 4 | 62.964 | 0.6 | 10.0% | 3.7779 |
| Baby wipes a | Genital area | Dermal | 6 | 0.713 | 21.7 | 100.0% | 9.9853 |
| Diaper change creams | Genital area | Dermal | 8 | 12.167 | 0.7 | 100.0% | 8.5166 |
| Sunscreens b | Whole body | Dermal | 8 | 18.672 | 8.4 | 100.0% | 156.8443 |
| Total daily dermal exposure to HHCB (µg·day−1) | 277.10 ± 0.02 | ||||||
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Arbulu, M.; Sampedro, M.C.; Unceta, N.; Gómez-Caballero, A.; Goicolea, M.A.; Barrio, R.J. A retention time locked gas chromatography–mass spectrometry method based on stir-bar sorptive extraction and thermal desorption for automated determination of synthetic musk fragrances in natural and wastewaters. J. Chromatogr. A 2011, 1218, 3048–3055. [Google Scholar] [CrossRef] [PubMed]
- HERA (Human and Environmental Risk Assessment on Ingredients of Household Cleaning Products). Environmental Risk Assessment Polycyclic Musks AHTN (CAS 1506-02-1) and HHCB (CAS 122-05-05). 2004. Available online: http://www.heraproject.com/RiskAssessment.cfm?subID=29 (accessed on 2 September 2011).
- Reiner, J.L.; Kannan, K. A survey of polycyclic musks in selected household commodities from the United States. Chemosphere 2006, 62, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Bagasra, O.; Golkar, Z.; Garcia, M.; Rice, L.N.; Pace, D.G. Role of perfumes in pathogenesis of autism. Med. Hypoth. 2013, 80, 795–803. [Google Scholar] [CrossRef]
- Regulation of the European Parliament and of the Council on Cosmetic Products (recast). PE-CONS 3623/09. 2009. Available online: http://register.consilium.europa.eu/doc/srv?l=EN&f=ST%203623%202009%20INIT (accessed on 25 August 2011).
- Bridges, B. Fragrance: Emerging health and environmental concerns. Flavour Fragr. J. 2002, 17, 361–371. [Google Scholar] [CrossRef]
- Fluhr, J.; Darlenski, R.; Taieb, A.; Hachem, J.-P.; Baudouin, C.; Msika, P.; de Belilovsky, C.; Berardesca, E. Functional skin adaptation in infancy—Almost complete but not fully competent. Exp. Dermatol. 2010, 19, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Blume-Peytavi, U.; Hauser, M.; Stamatas, G.N.; Pathirana, D.; Bartels, N.G. Skin care practices for newborns and infants: Review of the clinical evidence for best practices. Pediatr. Dermatol. 2012, 29, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Lavender, T.; Bedwell, C.; O’Brien, E.; Cork, M.J.; Turner, M.; Hart, A. Infant skin-cleansing product versus water: A pilot randomized, assessor-blinded controlled trial. BMC Pediatr. 2011, 11. [Google Scholar] [CrossRef] [Green Version]
- Stamatas, G.N.; Nikolovski, J.; Mack, M.C.; Kollias, N. Infant skin physiology and development during the first years of life: A review of recent findings based on in vivo studies. Int. J. Cosmet. Sci. 2011, 33, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Imai, S.; Kuwabara, C. Infant skin and its care. Cosmet. Toilet. 1992, 107, 85–90. [Google Scholar]
- Hutter, H.P.; Wallner, P.; Hartl, W.; Uhl, M.; Lorbeer, G.; Gminski, R.; Mersh-Sundermann, V.; Kundi, M. Higher blood concentrations of synthetic musks in women above fifty years than in younger women. Int. J. Hyg. Environ. Health 2010, 213, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Roosens, L.; Covaci, A.; Neels, H. Concentrations of synthetic musk compounds in personal care and sanitation products and human exposure profiles through dermal application. Chemosphere 2007, 69, 1540–1547. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Yuan, T.; Wang, W.; Kannan, K. Concentrations and assessment of exposure to siloxanes and synthetic musks in personal care products from China. Environ. Pollut. 2011, 159, 3522–3528. [Google Scholar] [CrossRef] [PubMed]
- Correia, P.; Cruz, A.; Santos, L.; Alves, A. Human dermal exposure to galaxolide from personal care products. Int. J. Cosmet. Sci. 2013, 35, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Yao, Y.; Zeng, X.; Qian, G.; Guo, Y.; Wu, M.; Sheng, G.; Fu, J. Synthetic musks in the aquatic environment and personal care products in Shanghai, China. Chemosphere 2008, 72, 1553–1558. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Girón, A.B.; Crego, A.L.; González, M.J.; Marina, M.L. Enantiomeric separation of chiral polycyclic musks by capillary electrophoresis: Application to the analysis of cosmetic samples. J. Chromatogr. A 2010, 1217, 1157–1165. [Google Scholar] [CrossRef] [PubMed]
- Schüssler, W.; Nitschke, L. Determination of trace amounts of Galaxolide® (HHCB) by HPLC. Fresenius J. Anal. Chem. 1998, 361, 220–221. [Google Scholar] [CrossRef]
- Instituto Nacional de Estatística (Statistics Portugal), INE, IP, Censos 2011—XV Recenseamento geral da população, V Recenseamento geral da habitação—Resultados provisórios, Lisboa, Portugal, 2011. Available online: http://www.google.pt/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0CB8QFjAA&url=http%3A%2F%2Fcensos.ine.pt%2Fngt_server%2Fattachfileu.jsp%3Flook_parentBoui%3D131010986%26att_display%3Dn%26att_download%3Dy&ei=Q1QwVeyvMKiR7Aat7oDgDg&usg=AFQjCNEdobEaXIfk1EIB_1v7sI117bsbrA (accessed on 20 November 2014). (In Portuguese)
- Bonamonte, D.; Filoni, A.; Vestita, M.; Angelini, G.; Foti, C. Market trends in baby skin care products and implications for clinical practice. Pediatr. Dermatol. 2014, 31, 734–738. [Google Scholar] [CrossRef] [PubMed]
- Cadby, P.A.; Troy, W.R.; Vey, M.G.H. Consumer exposure to fragrance ingredients: Providing estimates for safety evaluation. Regul. Toxicol. Pharmacol. 2002, 36, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Wester, R.C.; Maibach, H.I. Interrelationships in the dose-response of percutaneous absorption. In Topical Absorption of Dermatological Products; Bronaugh, R.L., Maibach, H.I., Eds.; Marcel Dekker, Inc.: New York, NY, USA, 2002; pp. 169–184. [Google Scholar]
- Wester, R.C.; Maibach, H.I. Regional variation in percutaneous absortion. In Topical Absorption of Dermatological Products; Bronaugh, R.L., Maibach, H.I., Eds.; Marcel Dekker, Inc.: New York, NY, USA, 2002; pp. 33–39. [Google Scholar]
- Ford, R.A.; Hawkins, D.R.; Schwarzenbach, R.; Api, A.M. The systemic exposure to the polycyclic musks, AHTN and HHCB, under conditions of use as fragrance ingredients: Evidence of lack of complete absorption from a skin reservoir. Toxicol. Lett. 1999, 111, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Masuck, I.; Hutzler, C.; Luch, A. Estimation of dermal and oral exposure of children to scented toys: Analysis of the migration of fragrance allergens by dynamic headspace GC-MS. J. Sep. Sci. 2011, 34, 2686–2696. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Correia, P.; Cruz, A.; Santos, L.; Alves, A. Risk of Children’s Dermal Exposure to Galaxolide through Personal Care Products. Cosmetics 2015, 2, 93-109. https://doi.org/10.3390/cosmetics2020093
Correia P, Cruz A, Santos L, Alves A. Risk of Children’s Dermal Exposure to Galaxolide through Personal Care Products. Cosmetics. 2015; 2(2):93-109. https://doi.org/10.3390/cosmetics2020093
Chicago/Turabian StyleCorreia, Patrícia, Agostinho Cruz, Lúcia Santos, and Arminda Alves. 2015. "Risk of Children’s Dermal Exposure to Galaxolide through Personal Care Products" Cosmetics 2, no. 2: 93-109. https://doi.org/10.3390/cosmetics2020093