1. Introduction
According to the World Health Organization (WHO) maternal mortality report (2000–2017) [
1], about every 2 min, a woman dies because of preventable complications due to childbirth or pregnancy. The maternal mortality ratio (MMR) in the world’s least developed countries is high, estimated at 415 maternal deaths per 100,000 live births, which is more than 40 times higher than the MMR in Europe and almost 60 times higher than in Australia and New Zealand. The target of reducing the maternal mortality ratio worldwide to less than 70 per 100,000 live births by 2030 has been set by the United Nations (sustainable development goal 3.1) [
2]. This crucially depends on ensuring that women have access to basic healthcare services before, during and after childbirth. Maternal mortality risk factors could be detected by using ultrasound imaging, but these devices are very expensive, and thus not affordable for healthcare providers in developing countries.
Furthermore, there is heightened public concern over the healthcare costs and research to miniaturize ultrasound scanners, and making them low-cost devices has been an area of active research over the years [
3,
4,
5]. The 2020 report shows that the global expenditures on healthcare in 190 countries from 2000 to 2018 continually rose and reached USD 8.3 trillion or 10% of the global GDP [
6]. Further, the National Health Service (NHS) in the UK performs over 45 million imaging procedures involving 10.5 million ultrasound scans each year [
7]. The global ultrasound equipment market is projected to grow from USD 7.80 billion in 2021 to USD 12.93 billion in 2028 at a CAGR of 7.5% in the forecast period (2021–2028) [
8]. The growth of healthcare costs worldwide, coupled with the desire for access to care in the developing world, is driving the need for low-cost, high-quality imaging services.
Conventional ultrasound devices use multi-element piezoelectric transducer arrays to produce 2D or 3D images, while only a single-element piezoelectric transducer was used in the proposed ultrasound scanner. Some of the concepts used to minimize hardware complexity in the prototype probe can be found in previous work conducted by our research team [
9]. The transducer has a diameter of 15 mm, a thickness (
) of 0.5 mm and a centre frequency (
) of approximately 4 MHz and is a type II PZT disc. Operating frequencies of 2–5 MHz are typical for ultrasound abdominal probes, as they represent the best trade-off between resolution and penetration depth. The bandwidth,
, of the transducer is 2 MHz, with a focused beam optimised for 4–15 cm penetration depth and a focal depth of 7 cm. The axial resolution is determined by the bandwidth,
, whereas the lateral and elevation beam widths are determined by the size and geometry of the transducer aperture, and the centre frequency,
. It takes 2.5 ms to obtain one scan line, which results in a frame rate of 400 frames per second (400 Hz). The sampling frequency,
, is 25 MHz, and 716 samples are obtained per scan line. This probe design greatly reduces the hardware complexity, power consumption and beamforming computational load, thus bringing the manufacturing cost down to less than USD 100. This will make the device affordable for developing countries. The cost comparison of commercially available portable ultrasound machines is as follows:
Philips Lumify—200 USD/month per probe + 75 USD/month warranty.
Sonosite IVIZ—USD 10,000.
GE VSAN Extend—starts at USD 2995.
Clarius—starts at USD 6900.
Butterfly IQ—USD 1999 + 420 USD/year for cloud user license.
There are many companies (such as GE Healthcare; Koninklijke Philips N.V.; Canon Inc.; Hitachi; Siemens Healthcare; Samsung Medison Co., Ltd.; and Esaote) that are constantly focusing on introducing new ultrasound systems with advanced technologies in the market. GE Healthcare dominated the ultrasound industry and accounted for the largest market share in 2020 [
8]. Many of the big companies are also shifting their focus towards making portable ultrasound devices that can be carried by a single person from one place to another. On 15 November 2021, TELEMED Medical Systems presented MicrUs Pro Handheld USB Ultrasound, its latest PC-based ultrasound diagnostic system, at the 2021 edition of MEDICA [
10].
The mechanical sensors traditionally used to track the ultrasound probe’s position make the device bulky and hard to operate. Therefore, those sensors were not used in this probe. Hence, the formation of a high-quality, geometrically correct ultrasound image at a reduced cost depends upon the utilization of advanced signal processing algorithms. This article provides a detailed description of the proposed image formation algorithms required to generate a geometrically correct, 2D, B-mode ultrasound image with a simple ultrasound probe. However, it does not include in-depth information on the probe’s hardware design. Please refer to [
9] for understanding some of the concepts used to minimise hardware complexity in the prototype probe. The ego-motion estimation techniques proposed in the previous work [
11], along with advanced signal processing algorithms explained in the presented work, are used to track the probe’s linear motion. The probe’s position estimates help construct a geometrically correct, 2D, B-mode ultrasound image.
A novel ego-motion estimation algorithm that works by finding the decorrelation measurements between series of successive scan-line echo data (1D data) is proposed. This gives information about the lateral velocity of the probe in a linear scan as it is passed over the skin. These velocity estimates help map the image into a set of pixels that are geometrically correct.
The ego-motion estimation algorithm is dependent on the focal parameters of the transducer, the texture or speckle detail, and the echogenicity of the tissue. The very top layer of the human body consists of static tissues that produce a constant speckle pattern over time. The echogenicity is also similar in the top layer, which makes it the optimal region to be considered in motion calculations. However, it is far from the focal point of the transducer. The speckle detail and echogenicity of the tissue start becoming dynamic with an increase in the distance of travel of ultrasound wave in the axial direction (depth). Although these regions are near the focal point of the transducer, they consist of different types of tissues and organs, which creates a dynamic speckle pattern. This would affect the information about the probe’s motion gathered from the echo data, which can eventually impact the geometric accuracy of generated images. Therefore, choosing the optimal region depending on the layers of the human body is crucial. Therefore, the work presented using clustering techniques is needed to optimise the position estimation algorithm to be robust in more complex scenes and variable tissue properties in human scans. This will make the algorithm independent of the scanned region.
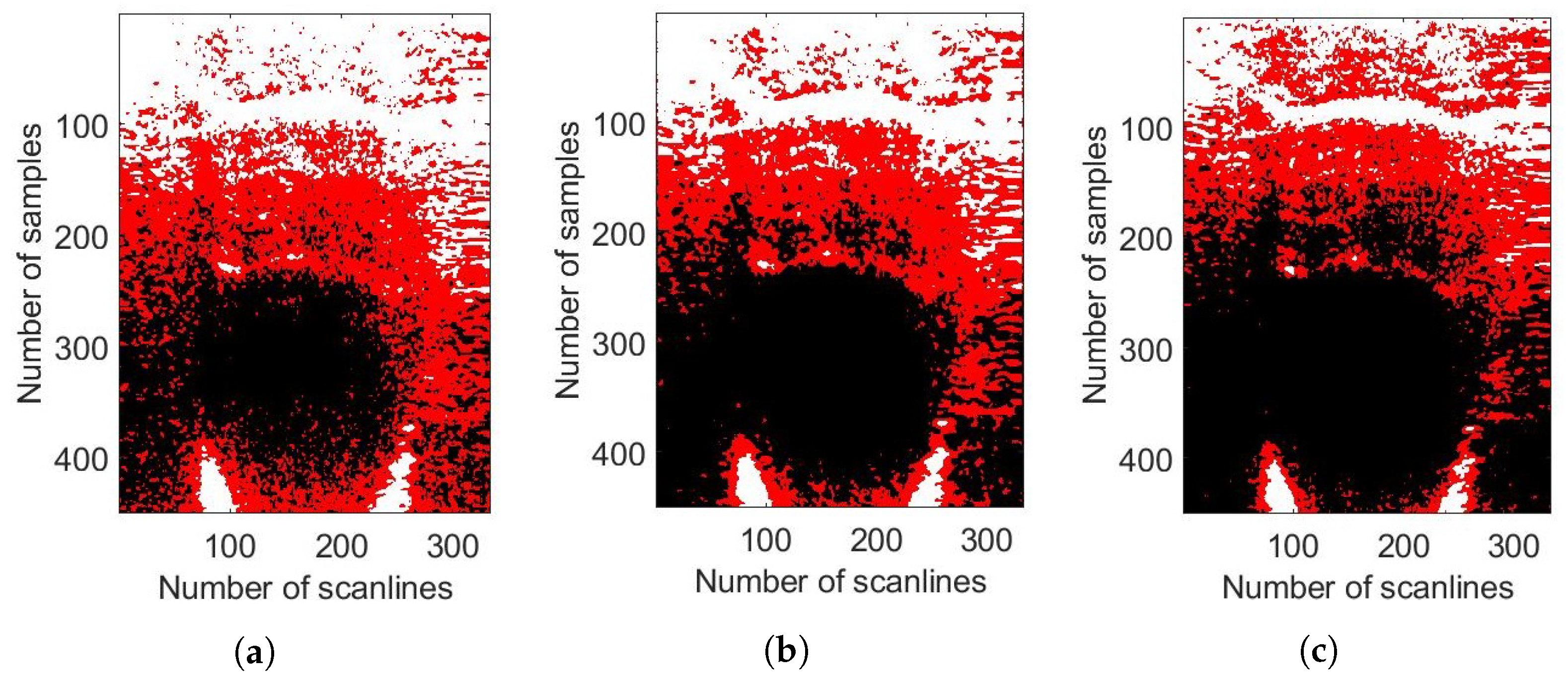
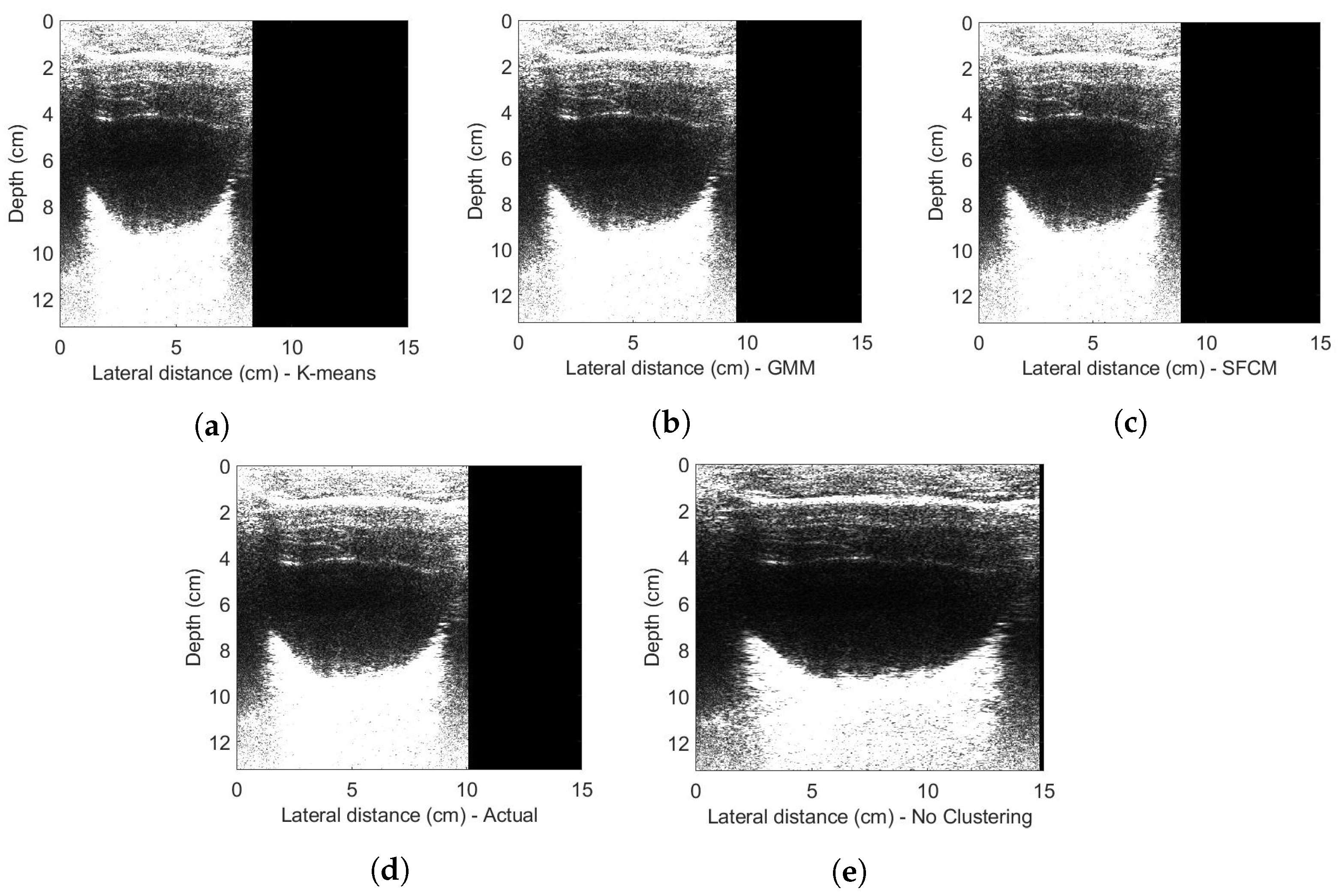
For the first time, the Gaussian mixture model (GMM), spatial fuzzy c-means (SFCM) and k-means clustering techniques have been exploited on 1D raw echo data. These techniques have been traditionally used for medical image segmentation on 2D images. But a novel approach has been presented that applies these techniques on the 1D raw ultrasound echo data that helps towards tracking the probe’s velocity. That eventually helps in creating a geometrically correct 2D ultrasound image. These clustering techniques extract the appropriate data from the raw echo scan line data by clustering them into anechoic, hyperechoic, and hypoechoic regions. Only the clustered data in the hypoechoic region is used to estimate the probe’s position with the help of the ego-motion estimation algorithm. A specially designed mechanical rig controls the probe’s motion and measures its real-time position values. Quantitative analysis for estimating the probe’s position using different clustering techniques was carried out using phantom and in vivo experiments, which were compared with the measured probe’s position. The contributions of this article are:
Optimisation of the decorrelation-based velocity estimation technique for linear scans and application of the unscented Kalman filter (UKF) to filter out the effects of noisy velocity estimates to improve trajectory estimates.
First-time exploitation of unsupervised clustering (K-means, SFCM and GMM) on the 1D raw ultrasound imaging data.
Reconstruction of geometrically correct 2D ultrasound images of phantom and in vivo data from the single-element transducer.
The rest of this article is organized as follows. In
Section 2, the research related to these image formation algorithms and the clustering techniques is presented.
Section 3 presents the proposed ultrasound scanner design and the proposed image formation algorithms: data pre-processing techniques, ego-motion estimation algorithm and the clustering methods.
Section 4 presents the experimental setup and the results and discussions. Finally,
Section 5 concludes this article.
2. Related Research
Several design parameters need to be addressed to reduce the manufacturing cost of the ultrasound probe and to make the device portable and smaller in size. Many researchers have shown interest in developing ultrasound probes by reducing the number of piezoelectric elements in the transducer. Lokesh B and A.K Thittai presented the design of a low-cost ultrasound system by integrating only 8 or 16 active elements in the transducer [
12]. Whereas, M.Fuller et al. presented a system prototype of a future compact, low-cost medical ultrasound device that consists of a 32 × 32 elements, fully sampled 2D transducer array [
13,
14]. The proposed ultrasound probe consists of only a single-element transducer without the use of any position tracking sensor such as; optical sensors or electromagnetic sensors.
K. Owen et al. have first shown the use of optical sensors to track the transducer’s motion in their initial work [
15] and then in [
16] combining motion estimates from optical tracking and ultrasound decorrelation measurements, to produce an improved composite estimate of probe’s motion. Q. Cai et al. have recently demonstrated the design and prototype of an ultrasound probe’s tracking system based on a low-cost camera [
17]. These sensors make the device bulky in size and difficult to operate. Their cost also adds up to the final manufacturing cost of the low-cost ultrasound scanner. Therefore, the formation of a high-quality ultrasound image at a reduced cost depends upon the utilization of advanced signal processing algorithms with minimal use of hardware.
Several authors have shown the use of decorrelation to track transducer’s motion [
18,
19,
20,
21]. J. F. Chen et al., in [
18], have calculated decorrelation measurements from the underlying speckle pattern as the transducer moves across the elevation focus to determine the transducer’s motion in the elevation plane. A. Krupa et al. have also presented the direct use of speckle information contained in the images to track both out-of-plane and in-plane motions [
19]. A. H. Gee et al. have demonstrated the use of speckle information to acquire freehand 3D ultrasound [
20]. R. F. Cheng et al., have also proposed speckle decorrelation techniques for performing freehand 3D ultrasound imaging without the need for a position sensor to provide the location of the ultrasound probe [
21].
All these researchers have used decorrelation techniques by first dividing the image obtained with the ultrasound probe into several patches and then finding the correlation between corresponding patches of 2D, B-mode scans/images. They found an approximation of the speckle correlation function as a function of the orthogonal distance between two B-mode scans. However, this requires that the B-scans contain significant amounts of fully developed speckle. This condition is rarely satisfied in scans of real tissue, which instead exhibit fairly ubiquitous coherent scattering [
20]; whereas, in our research, a completely novel technique of using correlation-based tracking is presented, which looks directly at the grey level intensity values provided by the ultrasound imaging probe. The correlation between the decorrelation measurements (obtained between the successive scanlines at a certain depth) and the motion of the probe is presented in detail in
Section 3.
Machine learning algorithms allow systems to learn from data, identify patterns and predict outcomes without being explicitly programmed, thus having minimal human intervention. Diagnosis and detection with the help of a computer while applying machine learning algorithms can help physicians interpret medical images and reduce interpretation times [
22]. There have been various applications of machine learning in the medical field such as; mammography, colonoscopy, MR imaging and CT pulmonary angiography for the detection and diagnosis of breast cancer [
23], colon cancer [
24,
25], neurologic diseases (e.g., Alzheimer) [
26,
27,
28] and pulmonary embolism [
29,
30], respectively.
Y. Ueno et al. have compared the diagnostic efficiency of endometrial carcinoma among postmenopausal women with an endometrial width of 5 mm with irregular vaginal bleeding. The study was based on three different AI-based approaches such as logistic regression (LR), artificial neural network (ANN), and classification and regression tree (CART). The mathematical model has obtained promising preliminary results, but they must be interpreted with caution until they are validated with an independent data set [
31]. The automatic segmentation and detection of an irregular region in the cervical image to diagnose cervical cancer have been proposed by L. Sherin et al. The cervical tissue is differentiated from the normal tissue by implementing an ANN system based on a spectral database [
32]. J. Ogasawara et al. proposed a newly constructed deep neural network model (CTG-net) to detect compromised fetal status. It is a quantitative and automated diagnostic aid system that enables early intervention for putatively abnormal fetuses, resulting in a reduction in the number of cases of hypoxic injury [
33].
J. Abrantes et al. have presented a study for external validation of a deep learning model for breast density classification based on convolutional neural networks. The mammographic breast density was evaluated using an open-source density evaluation model. This model was developed using a deep convolutional neural network called ResNet-18. The results of this study suggest that while the tool demonstrates a relatively high level of accuracy compared to the original radiologist’s density assessment in distinguishing between dense and non-dense breasts, it may have limitations in accurately classifying the specific BI-RADS density categories [
34]. F. M. Calisto et al. has proposed a novel perspective to the design of adaptive communication between intelligent agents (AI) and clinicians using a human-centric AI assistant. This can reduce medical errors by helping clinicians in medical image classification and increase satisfaction by personalizing assertiveness according to the professional experience of each clinician [
35,
36]. All this has led to an increased interest in the application of machine learning in the field of medicine.
The proposed intelligent feature extraction/segmentation in this article will reduce the effects of anechoic and hyperechoic regions on the velocity estimates calculated from the position algorithm based on decorrelation. This will make the position estimation algorithm independent of the texture or speckle detail of scanned tissue and will lead to improved geometric accuracy on complex image scenes. Much work has been carried out by different researchers to facilitate medical image segmentation by using unsupervised machine learning algorithms (Kmeans, SFCM and GMM clustering or their modified/enhanced versions).
M. Ray et al. have recently (2023) proposed an uncertainty parameter weighted entropy-based fuzzy c-means clustering algorithm for noisy volumetric (3D) brain MR image segmentation. This uses complemented global and spatially constrained local membership functions. The acquired MR images produce blurry tissue boundaries due to inherent noise and intensity inhomogeneity that causes uncertainty while labelling a pixel into its proper tissue region. The proposed framework allows the algorithm to utilize the spatial intensity distribution both locally and globally within the image domain and produce more accurate cluster prototypes [
37]. R. E. Pregitha et al. have shown the fetal ultrasound image segmentation using the spatial fuzzy c-mean clustering method. The feature vectors are developed for each pixel of the fetal images used as inputs for the clustering method. The clustering methods segment the fetal image based on spatial information. Experimental results indicate that the Spatial Fuzzy C-Means clustering method can be applied with promising results [
38]. The use of kernel-based Fuzzy C-means clustering technique for early prediction of congenital abnormalities and to estimate the delivery date is shown by S. Meenakshi et al. in their work [
39]. W. A. Kissara and B. F. Hassan have applied the fuzzy c-means algorithm on the fetal anatomy parameters to determine the fetal sex. The study proved that the features extracted from the images give good results in determining the sex of the fetus [
40].
Bing et al. [
41] proposed the enhanced FCM algorithm with spatial information (SFCM) to approximate the boundaries of interest. A multi-scale fuzzy c-means method integrated with particle swarm optimization (MsFCM-PSO) has been used for ultrasound image segmentation by Zhang et al. [
42]. Yan [
43] also proposed the use of fuzzy c-means (FCM) clustering while incorporating spatial information based on image decomposition. All these methods were validated on both simulated and clinical ultrasound images. Sombutkaew et al. [
44] have proposed the use of fuzzy c-mean clustering to achieve higher encoding efficiency for medical image data.
The k-means grouping algorithm was initially proposed by MacQueen in 1967 and later enhanced by Hartigan and Wong. Ciklacandir et al. [
45] studied the application of the k-means clustering technique for early diagnosis of breast cancer. K-means clustering has been applied for renal calculi detection and on three-dimensional synthetic ultrasound breast images by Upadhyay et al. [
46] and Yang et al. [
47], respectively. EM-MPM performs significantly better, especially in the cases of high density, which means EM-MPM could greatly help with the dense proportion—cancer risk. Meanwhile, Mandwe and Anjum [
48] have proposed a computer-aided system for brain MR image segmentation for the detection of tumour location using an advanced k-means clustering algorithm and fuzzy c-means algorithm. A design approach for performance analysis of infant’s abnormality has been proposed by R. Agrawal et al., using k-means clustering. The parameters like head diameter and abdomen circumference are used to incorporate feature extraction and following that the k-means clustering algorithm is used to classify abnormalities in infants. The proposed system gives promising results for detecting the abnormalities of fetuses and the accuracy is coming out to be 83.76% by using the k-means clustering algorithm [
49]. A. A. Hussain et al. have shown the use of k-means clustering or hybrid clustering that combines k-means clustering with a feed-forward neural network (FFNN) to accurately determine the fetal biometry [
50].
The expectation maximization (EM) algorithm was introduced by Dempster (1977) for maximization likelihood functions with missing data. Khanna et al. [
51] studied the segmentation of ultrasound images based on the conventional expectation maximization (EM) algorithm applied to texture features extracted by a bank of Gabor filters. The segmentation results were compared with the work accomplished using K-means clustering. It was concluded that K-means being a basic technique, results in over-segmentation and converges in local minima. Huang et al. [
52] have shown the use of an improved expectation maximization (EM) algorithm to incorporate neutrosophic logic to diagnose breast cancer. S.Belciug et al. proposed a medical decision-making framework designed as a merger between deep learning algorithms and Gaussian Mixture Modelling clustering (GMM) to prevent pregnancy complications and maternal deaths [
53]. Ravindraiah and Tejaswini [
54] studied the comparison of three segmentation algorithms, K-means clustering, fuzzy c-means (FCM) clustering, and expectation maximization (EM) on intravascular ultrasound images. Experiment results show that the new algorithm (GMM-EM) yields better segmentation results. Furthermore, E. Nsugbe et al. have presented the investigation of combining datasets, using physiological signals such as uterine contractions and foetal and maternal heart rate signals, with various forms of prediction machines. This study is based on predicting premature births in Hispanic labour patients. The results have shown the use of two effective unsupervised learning methods, that is, GMM and K-means, towards the self-sorting of data samples based on the acquired physiological signals [
55].
All the papers describe the use of clustering techniques in the field of medical imaging for image segmentation. A novel approach has been presented that applies these techniques on the 1D raw echo data, collected from a simple probe to create a geometrically correct 2D ultrasound image.
5. Conclusions and Future Work
The production cost of the very low-cost medical ultrasound imaging system was reduced to approximately USD 100 by replacing a multi-element piezoelectric transducer array with a single piezoelectric element. This probe design greatly reduces the hardware complexity, power consumption and beamforming computational load. Raw echo data were gathered by scanning the transducer over the phantom or the skin in a freehand linear/polar motion or with the help of a specially designed mechanical rig. These data were transmitted to the computer via Wi-Fi for further processing.
The research presented in this article describes the design and implementation of image formation techniques for a linear scan. In the free-hand linear scan, the probe is manually scanned over the desired region of interest (ROI), by translating it from one direction to the other while keeping the orientation near constant. A novel position estimation algorithm is proposed, which measures the decorrelation between successive scanlines to estimate the probe’s velocity. With the aid of an unscented Kalman filter (UKF), this is used to estimate the probe’s position. Clustering is used to make the position estimation algorithm be robust in more complex scenes and variable tissue properties in human scans. For the first time, the Gaussian mixture model (GMM), spatial fuzzy c-means (SFCM) and k-means clustering techniques have been exploited on a 1D raw echo data.
Quantitative analysis for estimating probe’s position was carried out, and it is observed that the Gaussian mixture model (GMM) works the best in classifying the desired data points in the correct cluster and reduces the mean percentage error, for estimating a probe’s position, from 28.7% to 4.2% and mean square error from 37 × 10 to 2.1 × 10 cm2. Although, this method is computationally expensive as compared to other presented techniques: SFCM and K-means. The reason that the other two clustering methods do not give the best result is because k-means uses a standard Euclidean distance metric to create clusters which is usually insufficient for image clustering. Also, SFCM clustering is truly concentrated on updating new centroids and then the membership function. Whereas, GMM includes the necessary information on the mean and variance of the individual regions to obtain optimum results. It could be concluded that the clustering algorithms have substantially improved the quality of egomotion estimation and hence the geometric accuracy of the images produced by the freehand scanner. These clustering methods have reduced its sensitivity to non-ideal operator behaviour and variation in tissue types. Initial in vivo experiments have shown promising results for clinical diagnosis, and with further work this technique has the potential to deliver a very low-cost ultrasound probe design for use in the developing world.
Future Work
The feasibility of a freehand scanner based on ego-motion estimation has been demonstrated, making use of unsupervised learning techniques to improve geometric accuracy. The implementation of these algorithms was based on the condition that the ultrasound probe would have moved in a linear manner (having only translation and almost no rotation in any of the axes). The ultimate goal of this project is to design the image formation algorithms for a single-element, free-hand ultrasound scanner. And indeed, the free-hand motion includes multiple and time-variant rotations on different axes. Therefore, future work is required to enable the algorithms to work in the case of combined motions (translation and rotation) by using the clustering techniques and ego-motion algorithm together with the motion sensor data.
The current ultrasonic parameters (frequency band, beam shape) are the best estimate of what is suited to abdominal imaging. However, there are numerous directions for future investigation to enhance the imaging performance of such a scanner, optimise for different imaging applications and assess the clinical potential of such a device:
Physical beam shape—in a fixed focus ultrasonic design, it is clear that the beam width and depth of focus have a strong influence on the backscattered signals and hence both the image resolution and the performance of correlation-based ego-motion estimation. More investigation is required to understand this relationship and to determine the optimum parameters for different applications.
Synthetic focusing—a fixed focus design places constraints on lateral resolution vs. depth. It is interesting to consider whether monostatic synthetic aperture concepts as in [
9] could be applied to the freehand scanner. This is very challenging, however, due to the requirement for precise tracking/control of the transducer trajectory and orientation.
Frequency band—the frequency band considered in this paper (fc = 4.2 MHz, B = 2 MHz) was chosen for abdominal imaging with penetration up to 15 cm. Other possible applications aimed at imaging more superficial structures (e.g., muscles, vascular, breast) would favour a higher frequency design and the scalability of the proposed scanner design and the algorithms needs to be investigated.
Front end—the ultrasound front end design in these experiments is sub-optimal in terms of noise performance and this limits both the image SNR and the depth range, which can be effectively utilised for correlation. A review of the front-end amplifier and impedance matching arrangements has significant potential to improve on this.
Clinical applications— Once the design has been optimised, close collaboration with clinicians is needed in the future to assess the diagnostic potential of such a device in low-resource settings. The authors limited research on this suggests that the most promising applications are in basic obstetric monitoring in developing nations, bladder imaging for self-management of urological conditions and early detection of aortic aneurysms. Larger scale studies are required to compare images with “ground truth” obtained from high-end ultrasound scanners over a wide range of patients.






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}