
Dynamics in Anemia Development and Dysregulation of Iron Homeostasis in Hospitalized Patients with COVID-19

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patients’ Characteristics
2.2. Anemia and Iron Deficiency upon Hospital Admission
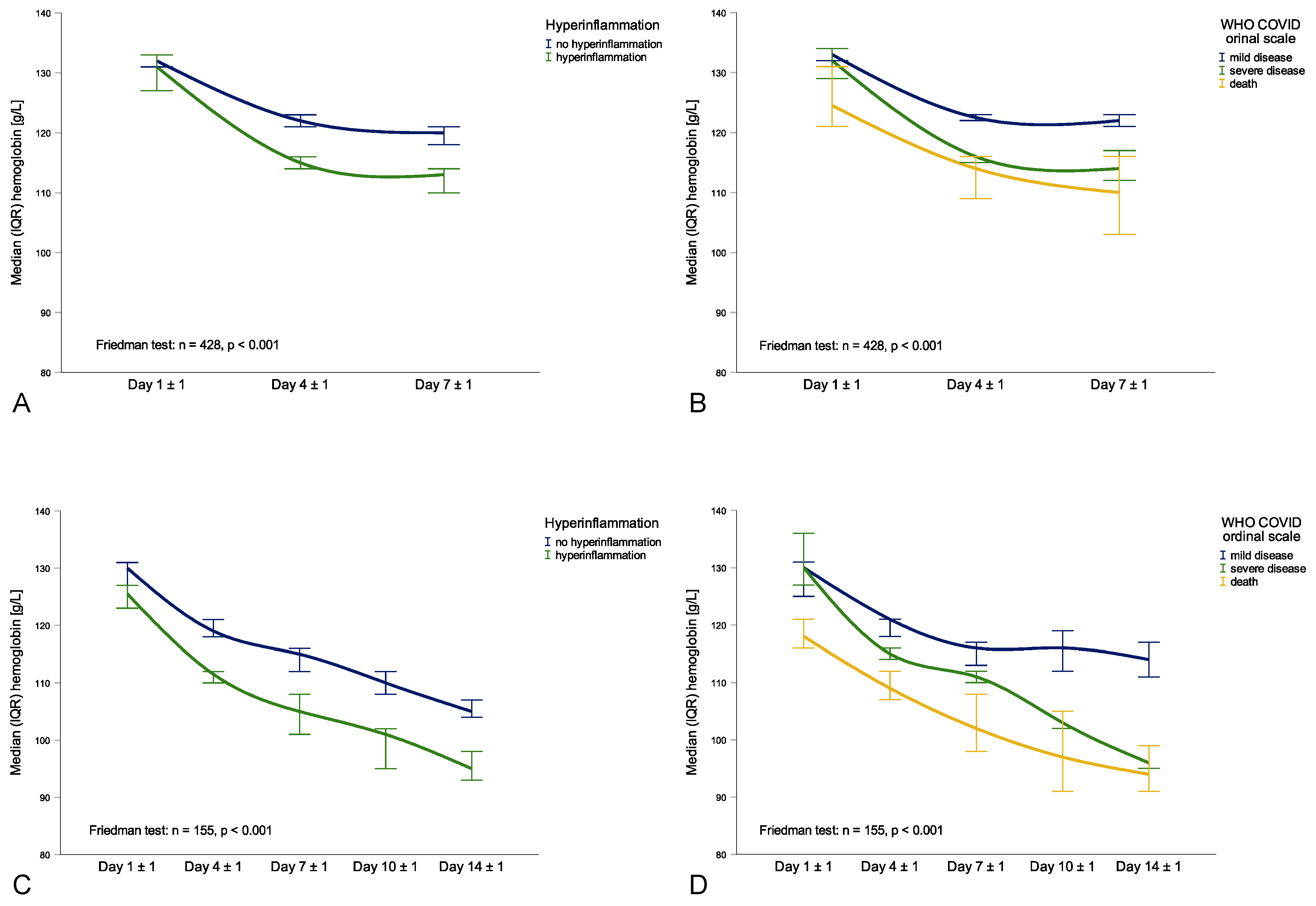
2.3. Longitudinal Association of Hemoglobin, Hyperinflammation and Disease Severity
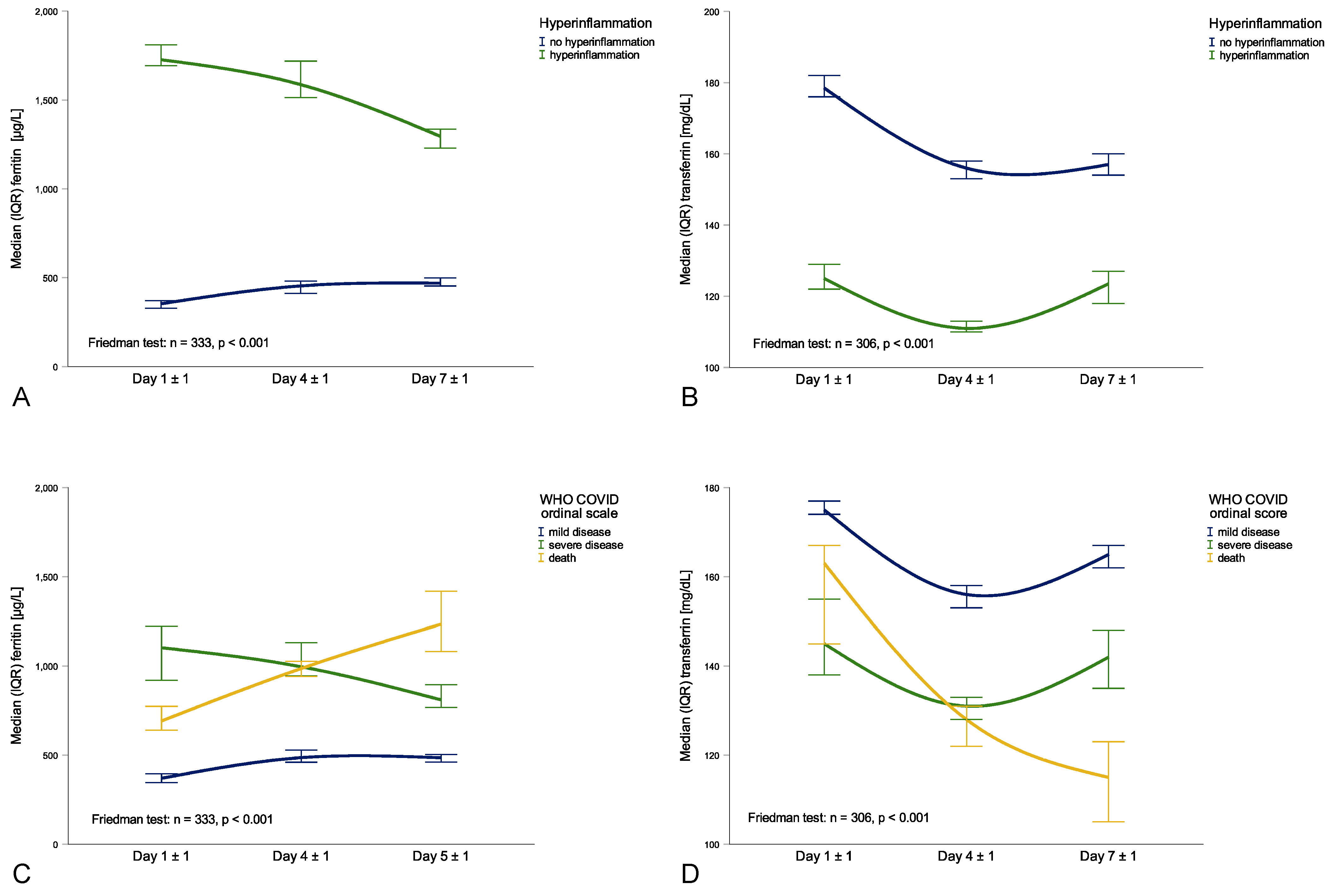
2.4. Longitudinal Association of Ferritin, Transferrin, Hyperinflammation and Disease Severity
2.5. Normalization of Hemoglobin and Iron Levels after Discharge from Hospital
3. Discussion
Limitations
4. Materials and Methods
4.1. Study Population
4.2. Labotratory Measurements
4.3. Classifications
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Thu, T.P.B.; Ngoc, P.N.H.; Hai, N.M.; Tuan, L.A. Effect of the social distancing measures on the spread of COVID-19 in 10 highly infected countries. Sci. Total Environ. 2020, 742, 140430. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, C.; Mostert, C.; Hentschker, C.; Voshaar, T.; Malzahn, J.; Schillinger, G.; Klauber, J.; Janssens, U.; Marx, G.; Weber-Carstens, S.; et al. Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: An observational study. Lancet Respir. Med. 2020, 8, 853–862. [Google Scholar] [CrossRef]
- World Health Organization. WHO R&D Blueprint: Novel Coronavirus: Outline of Trial Designs for Experimental Therapeutics, 27 January 2020, Geneva, Switzerland. Available online: https://apps.who.int/iris/handle/10665/330694 (accessed on 11 July 2021).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.G.T.; Fu, H.; et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Ellinghaus, D.; Degenhardt, F.; Bujanda, L.; Buti, M.; Albillos, A.; Invernizzi, P.; Fernández, J.; Prati, D.; Baselli, G.; Asselta, R.; et al. Genomewide Association Study of Severe Covid-19 with Respiratory Failure. N. Engl. J. Med. 2020, 383, 1522–1534. [Google Scholar] [CrossRef]
- Zhou, Y.; Yang, Q.; Chi, J.; Dong, B.; Lv, W.; Shen, L.; Wang, Y. Comorbidities and the risk of severe or fatal outcomes associated with coronavirus disease 2019: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 99, 47–56. [Google Scholar] [CrossRef]
- Bellmann-Weiler, R.; Lanser, L.; Burkert, F.; Seiwald, S.; Fritsche, G.; Wildner, S.; Schroll, A.; Koppelstätter, S.; Kurz, K.; Griesmacher, A.; et al. Neopterin predicts disease severity in hospitalized patients with COVID-19. Open Forum Infect. Dis. 2020, 8, ofaa521. [Google Scholar] [CrossRef]
- Manson, J.J.; Crooks, C.; Naja, M.; Ledlie, A.; Goulden, B.; Liddle, T.; Khan, E.; Mehta, P.; Martin-Gutierrez, L.; Waddington, K.E.; et al. COVID-19-associated hyperinflammation and escalation of patient care: A retrospective longitudinal cohort study. Lancet Rheumatol. 2020, 2, e594–e602. [Google Scholar] [CrossRef]
- Bellmann-Weiler, R.; Lanser, L.; Barket, R.; Rangger, L.; Schapfl, A.; Schaber, M.; Fritsche, G.; Wöll, E.; Weiss, G. Prevalence and Predictive Value of Anemia and Dysregulated Iron Homeostasis in Patients with COVID-19 Infection. J. Clin. Med. 2020, 9, 2429. [Google Scholar] [CrossRef]
- Lanser, L.; Burkert, F.R.; Thommes, L.; Egger, A.; Hoermann, G.; Kaser, S.; Pinggera, G.M.; Anliker, M.; Griesmacher, A.; Weiss, G.; et al. Testosterone Deficiency Is a Risk Factor for Severe COVID-19. Front. Endocrinol. (Lausanne) 2021, 12, 694083. [Google Scholar] [CrossRef]
- Zhang, X.; Tan, Y.; Ling, Y.; Lu, G.; Liu, F.; Yi, Z.; Jia, X.; Wu, M.; Shi, B.; Xu, S.; et al. Viral and host factors related to the clinical outcome of COVID-19. Nature 2020, 583, 437–440. [Google Scholar] [CrossRef]
- Weiss, G.; Ganz, T.; Goodnough, L.T. Anemia of inflammation. Blood 2019, 133, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Bergamaschi, G.; Borrelli de Andreis, F.; Aronico, N.; Lenti, M.V.; Barteselli, C.; Merli, S.; Pellegrino, I.; Coppola, L.; Cremonte, E.M.; Croce, G.; et al. Anemia in patients with Covid-19: Pathogenesis and clinical significance. Clin. Exp. Med. 2021, 21, 239–246. [Google Scholar] [CrossRef]
- Jacobs, J.; Eichbaum, Q. COVID-19 associated with severe autoimmune hemolytic anemia. Transfusion 2021, 61, 635–640. [Google Scholar] [CrossRef]
- Nairz, M.; Schroll, A.; Moschen, A.R.; Sonnweber, T.; Theurl, M.; Theurl, I.; Taub, N.; Jamnig, C.; Neurauter, D.; Huber, L.A.; et al. Erythropoietin contrastingly affects bacterial infection and experimental colitis by inhibiting nuclear factor-κB-inducible immune pathways. Immunity 2011, 34, 61–74. [Google Scholar] [CrossRef] [Green Version]
- Ganz, T.; Nemeth, E. Iron homeostasis in host defence and inflammation. Nat. Rev. Immunol. 2015, 15, 500–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valente de Souza, L.; Hoffmann, A.; Weiss, G. Impact of bacterial infections on erythropoiesis. Expert. Rev. Anti. Infect. Ther. 2020, 19, 619–633. [Google Scholar] [CrossRef] [PubMed]
- Drakesmith, H.; Prentice, A.M. Hepcidin and the iron-infection axis. Science 2012, 338, 768–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haschka, D.; Hoffmann, A.; Weiss, G. Iron in immune cell function and host defense. Semin. Cell Dev. Biol. 2021, 115, 27–36. [Google Scholar] [CrossRef]
- Weiss, G.; Goodnough, L.T. Anemia of Chronic Disease. N. Engl. J. Med. 2005, 352, 1011–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludwiczek, S.; Aigner, E.; Theurl, I.; Weiss, G.n. Cytokine-mediated regulation of iron transport in human monocytic cells. Blood 2003, 101, 4148–4154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arosio, P.; Carmona, F.; Gozzelino, R.; Maccarinelli, F.; Poli, M. The importance of eukaryotic ferritins in iron handling and cytoprotection. Biochem. J. 2015, 472, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torti, F.M.; Torti, S.V. Regulation of ferritin genes and protein. Blood 2002, 99, 3505–3516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegert, I.; Schödel, J.; Nairz, M.; Schatz, V.; Dettmer, K.; Dick, C.; Kalucka, J.; Franke, K.; Ehrenschwender, M.; Schley, G.; et al. Ferritin-Mediated Iron Sequestration Stabilizes Hypoxia-Inducible Factor-1α upon LPS Activation in the Presence of Ample Oxygen. Cell Rep. 2015, 13, 2048–2055. [Google Scholar] [CrossRef] [Green Version]
- Nai, A.; Lorè, N.I.; Pagani, A.; De Lorenzo, R.; Di Modica, S.; Saliu, F.; Cirillo, D.M.; Rovere-Querini, P.; Manfredi, A.A.; Silvestri, L. Hepcidin levels predict Covid-19 severity and mortality in a cohort of hospitalized Italian patients. Am. J. Hematol. 2021, 96, E32–E35. [Google Scholar] [CrossRef]
- McGonagle, D.; Sharif, K.; O’Regan, A.; Bridgewood, C. The Role of Cytokines including Interleukin-6 in COVID-19 induced Pneumonia and Macrophage Activation Syndrome-Like Disease. Autoimmun. Rev. 2020, 19, 102537. [Google Scholar] [CrossRef]
- De Bruin, A.M.; Demirel, Ö.; Hooibrink, B.; Brandts, C.H.; Nolte, M.A. Interferon-γ impairs proliferation of hematopoietic stem cells in mice. Blood 2013, 121, 3578–3585. [Google Scholar] [CrossRef] [Green Version]
- Jelkmann, W. Regulation of erythropoietin production. J. Physiol. 2011, 589, 1251–1258. [Google Scholar] [CrossRef]
- Caiado, F.; Pietras, E.M.; Manz, M.G. Inflammation as a regulator of hematopoietic stem cell function in disease, aging, and clonal selection. J. Exp. Med. 2021, 218, e20201541. [Google Scholar] [CrossRef]
- Means, R.T., Jr.; Krantz, S.B.; Luna, J.; Marsters, S.A.; Ashkenazi, A. Inhibition of murine erythroid colony formation in vitro by interferon gamma and correction by interferon receptor immunoadhesin. Blood 1994, 83, 911–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canna, S.W.; Wrobel, J.; Chu, N.; Kreiger, P.A.; Paessler, M.; Behrens, E.M. Interferon-γ mediates anemia but is dispensable for fulminant toll-like receptor 9-induced macrophage activation syndrome and hemophagocytosis in mice. Arthritis Rheum. 2013, 65, 1764–1775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beverina, I.; Borotto, E.; Novelli, C.; Radrizzani, D.; Brando, B. Iatrogenic anaemia and transfusion thresholds in ICU patients with COVID-19 disease at a tertiary care hospital. Transfus. Apher. Sci. 2021, 60, 103068. [Google Scholar] [CrossRef] [PubMed]
- Lasocki, S.; Baron, G.; Driss, F.; Westerman, M.; Puy, H.; Boutron, I.; Beaumont, C.; Montravers, P. Diagnostic accuracy of serum hepcidin for iron deficiency in critically ill patients with anemia. Intensive Care Med. 2010, 36, 1044–1048. [Google Scholar] [CrossRef] [PubMed]
- Weiss, G. Iron metabolism in the anemia of chronic disease. Biochim. Biophys. Acta 2009, 1790, 682–693. [Google Scholar] [CrossRef] [PubMed]
- Pak, M.; Lopez, M.A.; Gabayan, V.; Ganz, T.; Rivera, S. Suppression of hepcidin during anemia requires erythropoietic activity. Blood 2006, 108, 3730–3735. [Google Scholar] [CrossRef]
- Theurl, I.; Mattle, V.; Seifert, M.; Mariani, M.; Marth, C.; Weiss, G. Dysregulated monocyte iron homeostasis and erythropoietin formation in patients with anemia of chronic disease. Blood 2006, 107, 4142–4148. [Google Scholar] [CrossRef] [Green Version]
- Thomas, C.; Thomas, L. Anemia of chronic disease: Pathophysiology and laboratory diagnosis. Lab. Hematol. 2005, 11, 14–23. [Google Scholar] [CrossRef]
- Camaschella, C.; Girelli, D. The changing landscape of iron deficiency. Mol. Asp. Med. 2020, 75, 100861. [Google Scholar] [CrossRef]
- Tremblay, D.; Rapp, J.L.; Alpert, N.; Lieberman-Cribbin, W.; Mascarenhas, J.; Taioli, E.; Ghaffari, S. Mild anemia as a single independent predictor of mortality in patients with COVID-19. EJHaem 2021, 1–8. [Google Scholar] [CrossRef]
- Al-Jarallah, M.; Rajan, R.; Saber, A.A.; Pan, J.; Al-Sultan, A.T.; Abdelnaby, H.; Alroomi, M.; Dashti, R.; Aboelhassan, W.; Almutairi, F.; et al. In-hospital mortality in SARS-CoV-2 stratified by hemoglobin levels: A retrospective study. EJHaem 2021, 1–5. [Google Scholar] [CrossRef]
- Camaschella, C. Iron deficiency. Blood 2019, 133, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, T.; Breymann, C.; Brookes, M.J.; Lindgren, S.; Macdougall, I.C.; McMahon, L.P.; Munro, M.G.; Nemeth, E.; Rosano, G.M.C.; Schiefke, I.; et al. Questions and answers on iron deficiency treatment selection and the use of intravenous iron in routine clinical practice. Ann. Med. 2021, 53, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Sonnweber, T.; Sahanic, S.; Pizzini, A.; Luger, A.; Schwabl, C.; Sonnweber, B.; Kurz, K.; Koppelstätter, S.; Haschka, D.; Petzer, V.; et al. Cardiopulmonary recovery after COVID-19: An observational prospective multi-center trial. Eur. Respir. J. 2020, 57, 2003481. [Google Scholar] [CrossRef] [PubMed]
- Brandtner, A.; Tymoszuk, P.; Nairz, M.; Lehner, G.F.; Fritsche, G.; Vales, A.; Falkner, A.; Schennach, H.; Theurl, I.; Joannidis, M.; et al. Linkage of alterations in systemic iron homeostasis to patients’ outcome in sepsis: A prospective study. J. Intensive Care 2020, 8, 76. [Google Scholar] [CrossRef]
- Hippchen, T.; Altamura, S.; Muckenthaler, M.U.; Merle, U. Hypoferremia is Associated With Increased Hospitalization and Oxygen Demand in COVID-19 Patients. Hemasphere 2020, 4, e492. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Frost, J.N.; Aaron, L.; Donovan, K.; Drakesmith, H.; McKechnie, S.R.; Stanworth, S.J.; Collaborators. Systemic hypoferremia and severity of hypoxemic respiratory failure in COVID-19. Crit. Care 2020, 24, 320. [Google Scholar] [CrossRef]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Available online: https://apps.who.int/iris/handle/10665/85839 (accessed on 11 July 2021).



{kind=link}
{kind=link}
| Characteristic | Total Cohort | Mild Disease | Severe Disease | Death | Sign. |
|---|---|---|---|---|---|
| n = 645 | n = 432 | n = 117 | n = 96 | ||
| Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | p-Value | |
| Demographic and Clinical Characteristics | |||||
| Age [years] | 69 (54–79) | 68 (53–78) | 63 (56–71) | 80 (75–88) | <0.001 |
| BMI [kg/m2] | 26.3 (23.5–29.7) | 26.0 (23.5–29.4) | 28.4 (24.4–31.4) | 24.4 (22.3–27.7) | 0.003 |
| Temperature [C] | 38.0 (37.2–38.7) | 37.8 (37.1–38.6) | 38.5 (37.5–39.1) | 38.3 (37.6–39.0) | <0.001 |
| SpO2 [%] | 90 (86–93) | 91 (88–93) | 88 (84–91) | 86 (80–91) | <0.001 |
| O2 requirement [L] | 2 (0–5) | 2 (0–4) | 6 (3–8) | 6 (2–12) | <0.001 |
| Duration symptoms start until hospitalization [days] | 6 (3–9) | 6 (3–9) | 7 (4–10) | 4 (2–8) | 0.008 |
| Duration hospitalstay [days] | 10 (7–15) | 9 (6–12) | 19 (12–33) | 10 (5–23) | <0.001 |
| Laboratory Findings | |||||
| Cholesterol [mg/dL] | 125 (102–159) | 131 (106–162) | 120 (93–151) | 116 (96–135) | 0.007 |
| LDL [mg/dL] | 73 (50–100) | 78 (53–105) | 68 (50–99) | 54 (41–76) | <0.001 |
| HDL [mg/dL] | 34 (26–44) | 35 (27–46) | 30 (22–36) | 28 (21–39) | <0.001 |
| Triglycerides [mg/dL] | 103 (81–132) | 100 (79–128) | 110 (92–138) | 113 (85–148) | 0.017 |
| HbA1c [%] | 6.1 (5.7–6.6) | 6.0 (5.7–6.5) | 6.4 (6.0–6.8) | 6.3 (5.7–6.6) | <0.001 |
| Creatinine [mg/dL] | 0.97 (0.79–1.26) | 0.94 (0.78–1.17) | 0.99 (0.81–1.21) | 1.20 (0.91–1.88) | <0.001 |
| CRP [mg/dL] | 5.06 (2.03–10.17) | 3.81 (1.42–7.51) | 10.71 (5.78–16.84) | 7.61 (3.34–11.92) | <0.001 |
| IL-6 [ng/L] | 35.8 (15.6–78.2) | 28.8 (11.9–58.7) | 50.5 (22.0–120.3) | 87.3 (28.7–186.5) | <0.001 |
| Leukocytes [G/L] | 5.9 (4.5–8.2) | 5.5 (4.3–7.0) | 7.4 (5.2–10.1) | 6.9 (5.1–11.6) | <0.001 |
| Lymphocytes [G/L] | 0.89 (0.63–1.35) | 1.02 (0.69–1.46) | 0.74 (0.55–1.02) | 0.72 (0.41–1.00) | <0.001 |
| Hemoglobin [g/L] | 133 (119–144) | 134 (122–145) | 133 (119–144) | 123 (105–144) | 0.004 |
| Hematocrit [L/L] | 0.384 (0.347–0.417) | 0.387 (0.353–0.417) | 0.377 (0.345–0.419) | 0.362 (0.315–0.411) | 0.013 |
| Thrombocytes [g/L] | 181 (147–242) | 180 (146–238) | 196 (155–278) | 167 (134–237) | 0.015 |
| MCH [pg] | 30.2 (28.9–31.3) | 30.2 (28.8–31.2) | 30.3 (29.2–31.1) | 30.1 (29.1–32.0) | 0.582 |
| MCV [fL] | 87.0 (83.8–90.4) | 86.8 (83.7–89.8) | 86.9 (84.3–89.8) | 88.9 (84.5–92.5) | 0.010 |
| MCHC [g/L] | 345 (336–353) | 345 (338–352) | 347 (339–355) | 338 (327–350) | <0.001 |
| Iron [µmol/L] | 4.8 (3.5–6.9) | 5.0 (3.6–7.1) | 4.3 (3.1–6.2) | 4.1 (3.2–6.2) | <0.001 |
| Ferritin [µg/L] | 458 (245–1.096) | 363 (217–757) | 1.103 (436–1.937) | 661 (346–1.353) | <0.001 |
| Transferrin [mg/dL] | 172 (139–204) | 182 (155–214) | 144 (121–182) | 142 (114–170) | <0.001 |
| TSAT [mg/dL] | 11 (8–17) | 11 (8–16) | 12 (8–19) | 12 (8–22) | 0.820 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lanser, L.; Burkert, F.R.; Bellmann-Weiler, R.; Schroll, A.; Wildner, S.; Fritsche, G.; Weiss, G. Dynamics in Anemia Development and Dysregulation of Iron Homeostasis in Hospitalized Patients with COVID-19. Metabolites 2021, 11, 653. https://doi.org/10.3390/metabo11100653
Lanser L, Burkert FR, Bellmann-Weiler R, Schroll A, Wildner S, Fritsche G, Weiss G. Dynamics in Anemia Development and Dysregulation of Iron Homeostasis in Hospitalized Patients with COVID-19. Metabolites. 2021; 11(10):653. https://doi.org/10.3390/metabo11100653
Chicago/Turabian StyleLanser, Lukas, Francesco Robert Burkert, Rosa Bellmann-Weiler, Andrea Schroll, Sophie Wildner, Gernot Fritsche, and Günter Weiss. 2021. "Dynamics in Anemia Development and Dysregulation of Iron Homeostasis in Hospitalized Patients with COVID-19" Metabolites 11, no. 10: 653. https://doi.org/10.3390/metabo11100653
APA StyleLanser, L., Burkert, F. R., Bellmann-Weiler, R., Schroll, A., Wildner, S., Fritsche, G., & Weiss, G. (2021). Dynamics in Anemia Development and Dysregulation of Iron Homeostasis in Hospitalized Patients with COVID-19. Metabolites, 11(10), 653. https://doi.org/10.3390/metabo11100653