Medication Discrepancies in Community Pharmacies in Switzerland: Identification, Classification, and Their Potential Clinical and Economic Impact


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
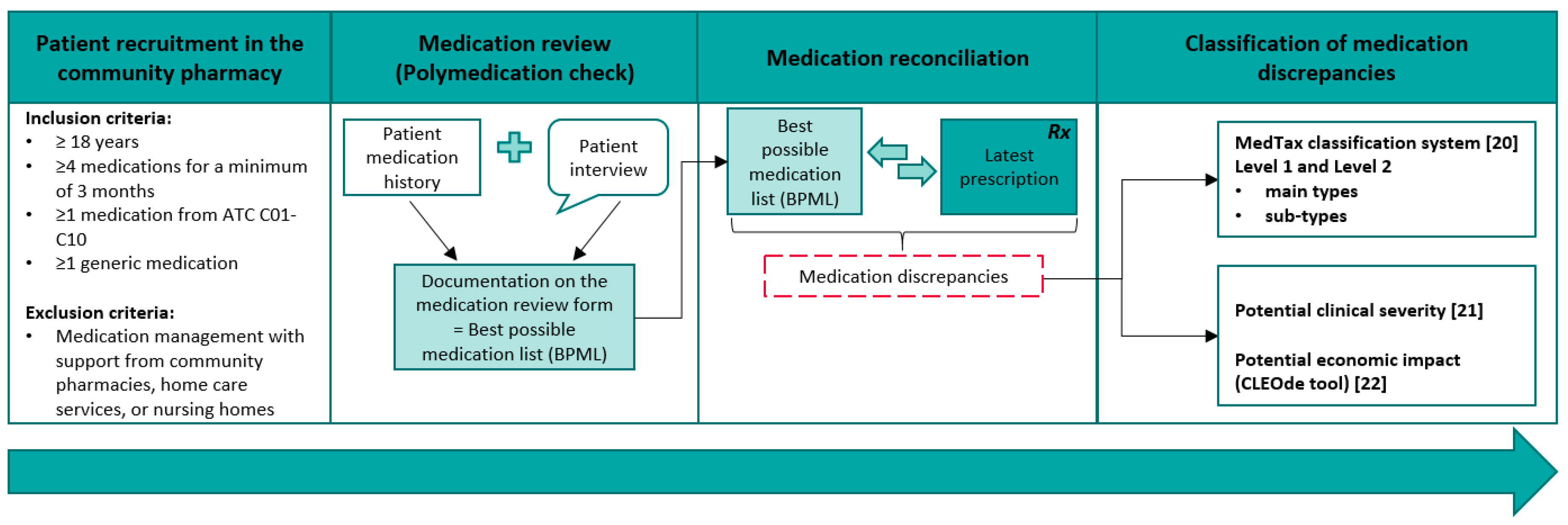
2.1. Setting and Recruitment
2.2. Medication Review
2.3. Medication Reconciliation
2.4. Data Handling
2.5. Potential Clinical Severity and Economic Impact of the Identified Medication Discrepancies
2.6. Statistical Analysis
3. Results
3.1. Medication Discrepancies—Frequency of Main Types
3.2. Medication Discrepancies—Frequency of Sub-Types
3.3. Potential Clinical Severity of the Medication Discrepancies and Economic Impact
4. Discussion
4.1. Types of Medication Discrepancies
4.2. Potential Clinical Severity and Economic Impact
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- Kreckman, J.; Wasey, W.; Wise, S.; Stevens, T.; Millburg, L.; Jaeger, C. Improving medication reconciliation at hospital admission, discharge and ambulatory care through a transition of care team. BMJ Open Qual. 2018, 7, e000281. [Google Scholar] [CrossRef] [PubMed]
- Mekonnen, A.B.; McLachlan, A.J.; Brien, J.A. Effectiveness of pharmacist-led medication reconciliation programmes on clinical outcomes at hospital transitions: A systematic review and meta-analysis. BMJ Open 2016, 6, e010003. [Google Scholar] [CrossRef] [PubMed]
- Kwan, J.L.; Lo, L.; Sampson, M.; Shojania, K.G. Medication reconciliation during transitions of care as a patient safety strategy: A systematic review. Ann. Intern. Med. 2013, 158, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Tjia, J.; Bonner, A.; Briesacher, B.A.; McGee, S.; Terrill, E.; Miller, K. Medication discrepancies upon hospital to skilled nursing facility transitions. J. Gen. Intern. Med. 2009, 24, 630–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Institute for Safe Medication Practices Canada (ISPM). Medication Reconciliation in Acute Care-Getting Started Kit: Safer Healthcare Now! Available online: https://www.ismp-canada.org/download/MedRec/Medrec_AC_English_GSK_V3.pdf (accessed on 19 September 2019).
- Cornu, P.; Steurbaut, S.; Leysen, T.; De Baere, E.; Ligneel, C.; Mets, T.; Dupont, A.G. Effect of medication reconciliation at hospital admission on medication discrepancies during hospitalization and at discharge for geriatric patients. Ann. Pharm. 2012, 46, 484–494. [Google Scholar] [CrossRef] [PubMed]
- Selcuk, A.; Sancar, M.; Okuyan, B.; Demirtunc, R.; Izzettin, F.V. The potential role of clinical pharmacists in elderly patients during hospital admission. Die Pharm. Int. J. Pharm. Sci. 2015, 70, 559–562. [Google Scholar]
- Zoni, A.C.; Duran Garcia, M.E.; Jimenez Munoz, A.B.; Salomon Perez, R.; Martin, P.; Herranz Alonso, A. The impact of medication reconciliation program at admission in an internal medicine department. Eur J. Intern. Med. 2012, 23, 696–700. [Google Scholar] [CrossRef] [PubMed]
- Armor, B.L.; Wight, A.J.; Carter, S.M. Evaluation of adverse drug events and medication discrepancies in transitions of care between hospital discharge and primary care follow-up. J. Pharm. Pract. 2016, 29, 132–137. [Google Scholar] [CrossRef]
- Bishop, M.A.; Cohen, B.A.; Billings, L.K.; Thomas, E.V. Reducing errors through discharge medication reconciliation by pharmacy services. Am. J. Health Syst. Pharm. 2015, 72, 120–126. [Google Scholar] [CrossRef]
- Belda-Rustarazo, S.; Cantero-Hinojosa, J.; Salmeron-García, A.; González-García, L.; Cabeza-Barrera, J.; Galvez, J. Medication reconciliation at admission and discharge: An analysis of prevalence and associated risk factors. Int. J. Clin. Pract. 2015, 69, 1268–1274. [Google Scholar] [CrossRef]
- McNab, D.; Bowie, P.; Ross, A.; MacWalter, G.; Ryan, M.; Morrison, J. Systematic review and meta-analysis of the effectiveness of pharmacist-led medication reconciliation in the community after hospital discharge. BMJ Qual. Saf. 2017, 27, 308–320. [Google Scholar] [CrossRef] [PubMed]
- Mueller, S.K.; Sponsler, K.C.; Kripalani, S.; Schnipper, J.L. Hospital-based medication reconciliation practices: A systematic review. Arch. Intern. Med. 2012, 172, 1057–1069. [Google Scholar] [CrossRef] [PubMed]
- Andrus, M.R.; Anderson, A.D. A retrospective review of student pharmacist medication reconciliation activities in an outpatient family medicine center. Pharm. Pract. (Granada) 2015, 13, 518. [Google Scholar] [CrossRef] [PubMed]
- Rose, O.; Jaehde, U.; Köberlein-Neu, J. Discrepancies between home medication and patient documentation in primary care. Res. Soc. Adm. Pharm. 2018, 14, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Steurbaut, S.; Leemans, L.; Leysen, T.; De Baere, E.; Cornu, P.; Mets, T.; Dupont, A.G. Medication history reconciliation by clinical pharmacists in elderly inpatients admitted from home or a nursing home. Ann. Pharm. 2010, 44, 1596–1603. [Google Scholar] [CrossRef] [PubMed]
- Messerli, M.; Blozik, E.; Vriends, N.; Hersberger, K.E. Impact of a community pharmacist-led medication review on medicines use in patients on polypharmacy-a prospective randomised controlled trial. BMC Health Serv. Res. 2016, 16, 145. [Google Scholar] [CrossRef] [Green Version]
- Griese-Mammen, N.; Hersberger, K.E.; Messerli, M.; Leikola, S.; Horvat, N.; van Mil, J.F.; Kos, M. PCNE definition of medication review: Reaching agreement. Int. J. Clin Pharm. 2018, 40, 1199–1208. [Google Scholar] [CrossRef]
- Imfeld-Isenegger, T.L.; Soares, I.B.; Makovec, U.N.; Horvat, N.; Kos, M.; van Mil, F.; Costa, F.A.; Hersberger, K.E. Community pharmacist-led medication review procedures across europe: Characterization, implementation and remuneration. Res. Soc. Adm. Pharm. 2019. [Google Scholar] [CrossRef]
- Almanasreh, E.; Moles, R.; Chen, T.F. The medication discrepancy taxonomy (MedTax): The development and validation of a classification system for medication discrepancies identified through medication reconciliation. Res. Social. Adm. Pharm. 2020, 16, 142–148. [Google Scholar] [CrossRef]
- Cornish, P.L.; Knowles, S.R.; Marchesano, R.; Tam, V.; Shadowitz, S.; Juurlink, D.N.; Etchells, E.E. Unintended medication discrepancies at the time of hospital admission. Arch. Intern. Med. 2005, 165, 424–429. [Google Scholar] [CrossRef]
- Stämpfli, D.; Baumgartner, P.; Boeni, F.; Bedouch, P.; Lampert, M.L.; Hersberger, K.E. Translation and validation of a tool to assess the impact of clinical pharmacists’ interventions. Int. J. Clin. Pharm. 2019, 41, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Fleiss, J.L. Measuring nominal scale agreement among many raters. Psychol Bull. 1971, 76, 378. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Becerra-Camargo, J.; Martinez-Martinez, F.; Garcia-Jimenez, E. A multicentre, double-blind, randomised, controlled, parallel-group study of the effectiveness of a pharmacist-acquired medication history in an emergency department. BMC Health Serv. Res. 2013, 13, 337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pippins, J.R.; Gandhi, T.K.; Hamann, C.; Ndumele, C.D.; Labonville, S.A.; Diedrichsen, E.K.; Carty, M.G.; Karson, A.S.; Bhan, I.; Coley, C.M. Classifying and predicting errors of inpatient medication reconciliation. J. Gen. Intern. Med. 2008, 23, 1414–1422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almanasreh, E.; Moles, R.; Chen, T.F. The medication reconciliation process and classification of discrepancies: A systematic review. Br. J. Clin. Pharmacol. 2016, 82, 645–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Håkonsen, H.; Eilertsen, M.; Borge, H.; Toverud, E.-L. Generic substitution: Additional challenge for adherence in hypertensive patients? Curr. Med. Res. Opin. 2009, 25, 2515–2521. [Google Scholar] [CrossRef]
- Kjoenniksen, I.; Lindbaek, M.; Granas, A.G. Patients’ attitudes towards and experiences of generic drug substitution in norway. Pharm. World Sci. 2006, 28, 284–289. [Google Scholar] [CrossRef]
- Himmel, W.; Simmenroth-Nayda, A.; Niebling, W.; Ledig, T.; Jansen, R.-D.; Kochen, M.; Gleiter, C.; Hummers-Pradier, E. Therapeutics. What do primary care patients think about generic drugs? Int. J. Clin. Pharmacol. Ther. 2005, 43, 16240704. [Google Scholar] [CrossRef] [Green Version]
- Decollogny, A.; Eggli, Y.; Halfon, P.; Lufkin, T.M. Determinants of generic drug substitution in switzerland. BMC Health Serv. Res. 2011, 11, 1. [Google Scholar] [CrossRef] [Green Version]
- Urban, R.; Paloumpi, E.; Rana, N.; Morgan, J. Communicating medication changes to community pharmacy post-discharge: The good, the bad, and the improvements. Int. J. Clin. Pharm. 2013, 35, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Bruhwiler, L.D.; Hersberger, K.E.; Lutters, M. Hospital discharge: What are the problems, information needs and objectives of community pharmacists? A mixed method approach. Pharm. Pract. (Granada) 2017, 15, 1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eggink, R.N.; Lenderink, A.W.; Widdershoven, J.W.; van den Bemt, P.M. The effect of a clinical pharmacist discharge service on medication discrepancies in patients with heart failure. Pharm. World Sci. 2010, 32, 759–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munday, A.; Kelly, B.; Forrester, J.; Timoney, A.; McGovern, E.J.B.J.G.P. Do general practitioners and community pharmacists want information on the reasons for drug therapy changes implemented by secondary care? Br. J. Gen. Pract. 1997, 47, 563–566. [Google Scholar] [PubMed]
- Ensing, H.T.; Koster, E.S.; van Berkel, P.I.; van Dooren, A.A.; Bouvy, M.L. Problems with continuity of care identified by community pharmacists post-discharge. J. Clin. Pharm. Ther. 2017, 42, 170–177. [Google Scholar] [CrossRef] [Green Version]
- Brühwiler, L.D.; Beeler, P.E.; Böni, F.; Giger, R.; Wiedemeier, P.G.; Hersberger, K.E.; Lutters, M. A RCT evaluating a pragmatic in-hospital service to increase the quality of discharge prescriptions. Int. J. Qual. Health Care 2019. [Google Scholar] [CrossRef]
- Karapinar-Carkit, F.; van Breukelen, B.R.; Borgsteede, S.D.; Janssen, M.J.; Egberts, A.C.; van den Bemt, P.M. Completeness of patient records in community pharmacies post-discharge after in-patient medication reconciliation: A before-after study. Int. J. Clin. Pharm. 2014, 36, 807–814. [Google Scholar] [CrossRef]
- Kennelty, K.A.; Chewning, B.; Wise, M.; Kind, A.; Roberts, T.; Kreling, D. Barriers and facilitators of medication reconciliation processes for recently discharged patients from community pharmacists’ perspectives. Res. Social Adm. Pharm. 2015, 11, 517–530. [Google Scholar] [CrossRef] [Green Version]
- Leguelinel-Blache, G.; Arnaud, F.; Bouvet, S.; Dubois, F.; Castelli, C.; Roux-Marson, C.; Ray, V.; Sotto, A.; Kinowski, J.-M. Impact of admission medication reconciliation performed by clinical pharmacists on medication safety. Eur. J. Intern. Med. 2014, 25, 808–814. [Google Scholar] [CrossRef]
- Whalley, A.S.; Salvo, M.C.; Levine, S.F.; Chamberlin, K.W.; Beaudoin, D. Evaluation of pharmacist involvement in outpatient transitions of care. J. Gen. Intern. Med. 2018, 33, 1227–1228. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| ATC Group | Contents | Number (%) |
|---|---|---|
| A | Alimentary Tract and Metabolism | 80 (25.2) |
| B | Blood and Blood Forming Organs | 25 (7.9) |
| C | Cardiovascular System | 108 (34.1) |
| D | Dermatologicals | 6 (1.9) |
| G | Genito Urinary System and Sex Hormones | 3 (0.9) |
| H | Systemic Hormonal Preparations, Excl. Sex Hormones and Insulines | 7 (2.2) |
| J | Antiinfectives for Systemic Use | 1 (0.3) |
| L | Antineoplastic and Immunomodulating Agents | 3 (0.9) |
| M | Musculo-Skeletal System | 24 (7.6) |
| N | Nervous System | 44 (13.9) |
| P | Antiparasitic Products, Insecticides, and Repellents | 2 (0.6) |
| R | Respiratory System | 11 (3.5) |
| S | Sensory Organs | 3 (0.9) |
| V | Various | 0 (0.0) |
| Levels and Main Types | Number (%) |
|---|---|
| 1. Medication mismatched | 18 (5.7) |
| 1.1 Medication omission | 0 (0.0) |
| 1.2 Medication commission (or addition) | 2 (0.6) |
| 1.3 Medication duplication | 1 (0.3) |
| 1.4 Therapeutic class substitution (medication change within a medication class) | 12 (3.8) |
| 1.5 Allergy or intolerance* | 0 (0.0) |
| 1.6 Other | 3 (0.9) |
| 2. Medication partially matched | 299 (94.3) |
| 2.1 Discrepancy in the name of medication | 43 (13.6) |
| 2.2 Discrepancy in the strength and/or frequency and/or number of units of dosage form and/or total daily dose | 134 (42.3) |
| 2.3 Discrepancy in the dosage form/route of administration | 0 (0.0) |
| 2.4 Discrepancy in the time of medication administration | 35 (11.0) |
| 2.5 Discrepancy in the duration or length of the therapy | 0 (0.0) |
| 2.6 Other | 87 (27.4) |
| Main Types and Sub-Types | Number (%) |
|---|---|
| 2.1. Discrepancy in the name of medication | 43 (13.6) |
| 2.1.1. Unclear or wrong name (brand name or generic name) | - |
| 2.1.2. Omission of brand name | - |
| 2.1.3. Omission of generic name | - |
| 2.1.4 Different brand name but same generic name | 43 (13.6) |
| 2.2. Discrepancy in the strength and/or frequency and/or number of units of dosage form and/or total daily dose | 134 (42.3) |
| 2.2.1. Unclear or wrong strength | - |
| 2.2.2. Omission of strength | - |
| 2.2.3. Different strength and different total daily dose | 8 (2.5) |
| 2.2.4. Different strength but same total daily dose | 4 (1.3) |
| 2.2.5. Omission of unit of strength | - |
| 2.2.6. Different or wrong unit of strength | - |
| 2.2.7. Same strength but unclear or wrong frequency | 40 (12.6) |
| 2.2.8. Same strength but omission of frequency | 29 (9.1) |
| 2.2.9. Same strength but different frequency and omission of the number of units | - |
| 2.2.10. Same strength and same frequency but omission of the number of units | - |
| 2.2.11. Same strength and same number of units but different frequency and different total daily dose | 21 (6.6) |
| 2.2.12. Same strength but different frequency and different number of units and different total daily dose | 9 (2.8) |
| 2.2.13. Same strength but different frequency and different number of units but same total daily dose | 4 (1.3) |
| 2.2.14. Same strength and same frequency but different number of units and different total daily dose | 19 (6.0) |
| 2.3 Discrepancy in the dosage form / route of administration | 0 (0.0) |
| 2.3.1. Unclear or wrong dosage form | - |
| 2.3.2. Unclear or wrong route of administration | - |
| 2.3.3. Omission of dosage form | - |
| 2.3.4. Omission of route of administration | - |
| 2.3.5. Different dosage form but same route of administration | - |
| 2.3.6. Different dosage form and different route of administration | - |
| 2.3.7. Same dosage form but different route of administration | - |
| 2.4. Discrepancy in the time of medication administration | 35 (11.0) |
| 2.4.1. Omission of the time of administration | 3 (0.9) |
| 2.4.2. Different time of administration through the day | 25 (7.9) |
| 2.4.3. Discrepancy in the medication administration with respect to food/meal | 7 (2.2) |
| 2.5. Discrepancy in the duration or length of therapy | 0 (0.0) |
| 2.6. Other | 87 (27.4) |
| Medication Discrepancy | Potential Clinical Severity a | Potential Economic Impact b | |||||
|---|---|---|---|---|---|---|---|
| Type | No. (%) | Class 1* | Class 2* | Class 3* | Increase in Cost | Null | Decrease in Cost |
| 1.1 Medication omission | - | - | - | - | - | - | - |
| 1.2 Medication commission | 2 (0.6) | - | 2 (0.6) | - | 2 (0.6) | - | - |
| 1.3 Medication duplication | 1 (0.3) | - | 1 (0.3) | - | 1 (0.3) | - | - |
| 1.4 Therapeutic class substitution | 12 (3.8) | 2 (0.6) | 10 (3.2) | - | 3 (0.9) | 1 (0.3) | 8 (2.5) |
| 1.5 Allergy or intolerance* | - | - | - | - | - | - | - |
| 1.6 Other (mismatched) | 3 (0.9) | 1 (0.3) | 2 (0.6) | - | 3 (0.9) | - | - |
| 2.1 Discrepancy in the name of the medication | 43 (13.6) | 42 (13.2) | 1 (0.3) | - | 3 (0.9) | 23 (7.3) | 17 (5.4) |
| 2.2 Discrepancy in the strength and/or frequency and/or number of units of dosage form and/or total daily dose | 134 (42.3) | 60 (18.9) | 71 (22.4) | 3 (0.9) | 29 (9.1) | 43 (13.6) | 62 (19.6) |
| 2.3 Discrepancy in the dosage form/route of administration | - | - | - | - | - | - | - |
| 2.4 Discrepancy in the time of medication administration | 35 (11.0) | 31 (9.8) | 4 (1.3) | - | - | 35 (11.0) | - |
| 2.5 Discrepancy in the duration or length of therapy | - | - | - | - | - | - | - |
| 2.6 Other (partially matched) | 87 (27.4) | 39 (12.3) | 46 (14.5) | 2 (0.6) | 8 (2.5) | 9 (2.8) | 70 (22.1) |
| Total | 317 (100.0) | 175 (55.2) | 137 (43.2) | 5 (1.6) | 49 (15.5) | 111 (35.0) | 157 (49.5) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imfeld-Isenegger, T.L.; Pham, M.B.T.; Stämpfli, D.; Albert, V.; Almanasreh, E.; Moles, R.; Chen, T.F.; Hersberger, K.E. Medication Discrepancies in Community Pharmacies in Switzerland: Identification, Classification, and Their Potential Clinical and Economic Impact. Pharmacy 2020, 8, 36. https://doi.org/10.3390/pharmacy8010036
Imfeld-Isenegger TL, Pham MBT, Stämpfli D, Albert V, Almanasreh E, Moles R, Chen TF, Hersberger KE. Medication Discrepancies in Community Pharmacies in Switzerland: Identification, Classification, and Their Potential Clinical and Economic Impact. Pharmacy. 2020; 8(1):36. https://doi.org/10.3390/pharmacy8010036
Chicago/Turabian StyleImfeld-Isenegger, Tamara L, Melanie Bich Tram Pham, Dominik Stämpfli, Valerie Albert, Enas Almanasreh, Rebekah Moles, Timothy F Chen, and Kurt E Hersberger. 2020. "Medication Discrepancies in Community Pharmacies in Switzerland: Identification, Classification, and Their Potential Clinical and Economic Impact" Pharmacy 8, no. 1: 36. https://doi.org/10.3390/pharmacy8010036
APA StyleImfeld-Isenegger, T. L., Pham, M. B. T., Stämpfli, D., Albert, V., Almanasreh, E., Moles, R., Chen, T. F., & Hersberger, K. E. (2020). Medication Discrepancies in Community Pharmacies in Switzerland: Identification, Classification, and Their Potential Clinical and Economic Impact. Pharmacy, 8(1), 36. https://doi.org/10.3390/pharmacy8010036