
Neurological Disorders of Patients Living with HIV Hospitalized in Infectious Departments of the Specialist Hospital in Lower Silesia in Poland


Abstract
:1. Introduction
2. Objectives
3. Materials and Methods
Statistical Analysis
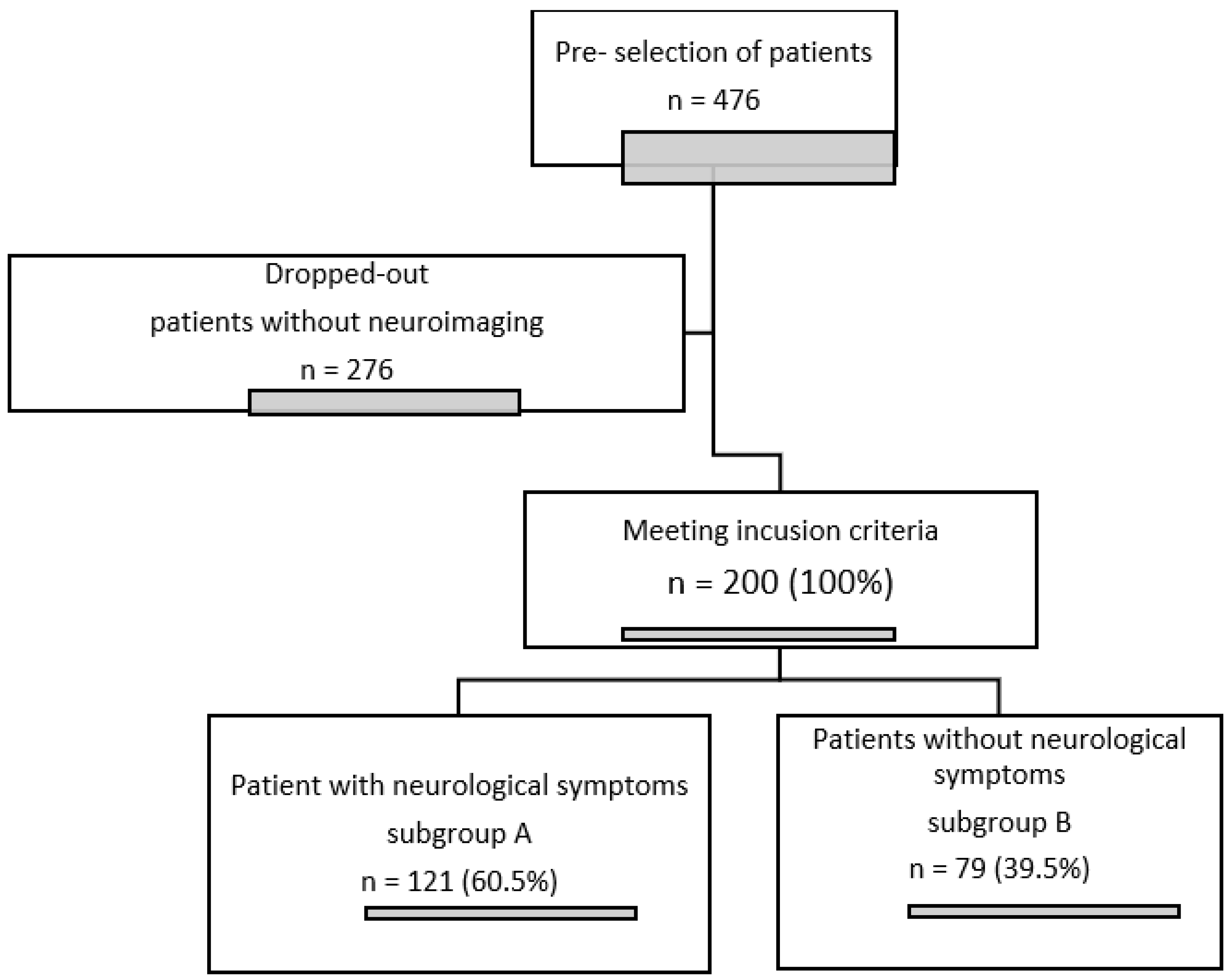
4. Results
- -
- Supplementation of the diagnosis of opportunistic diseases and patients with newly diagnosed HIV infection in the AIDS stage (34/79, 43.04%);
- -
- A follow-up after differential diagnosis in patients with symptoms other than neurological ones, e.g., patients with fever (25/79; 31.65%);
- -
- A follow-up diagnosis due to suspected neurosyphilis in patients with no symptoms due to syphilis of unknown duration or in cases of an insufficient decline in serum antibody titres after treatment (13/79; 16.45%) [9];
- -
- Head injury during hospitalisation (7/79; 8.86%).
5. Discussion
6. Conclusions
- The most frequently presented neurological symptoms in the analysed group of HIV-positive patients were headaches, limb paresis, impaired consciousness, balance disturbances, and gait disorders.
- Cortical and subcortical atrophy, as well as vascular changes, are frequently observed pathologies among HIV-positive patients; however, their cause may be multifactorial and independent of HIV infection.
- Toxoplasmosis, progressive multifocal leukoencephalopathy, and cryptococcosis are among the most frequent CNS diseases observed in our patients with HIV/AIDS, irrespective of the presence or absence of neurological symptoms.
- The presence of CNS diseases, especially AIDS-related opportunistic diseases, is prognostically unfavourable.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hogan, C.; Wilkins, E. Neurological complications in HIV. Clin. Med. 2011, 11, 571–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyziak-Kowalska, K.; Dusza, M.; Mularska, E.; Kalinowska-Nowak, A.; Barałkiewicz, G.; Jabłonowska, E.; Bander, D.; Podlasin, R.B.; Kubicka, J. Late presenters among newly diagnosed HIV- infected in Poland in 2006–2008. HIV AIDS Rev. 2017, 16, 244–250. [Google Scholar] [CrossRef] [Green Version]
- Wójcik-Cichy, K.; Jabłonowska, O.; Piekarska, A.; Jabłonowska, E. The high incidence of late presenters for HIV/AIDS infection in the Lodz province, Poland in the years 2009-2016: We are still far from the UNAIDS 90% target. AIDS Care 2018, 30, 1538–1541. [Google Scholar] [CrossRef] [PubMed]
- Jabłonowska, E.; Szetela, B.; Bielecki, M.; Horban, A.; Bociąga-Jasik, M.; Mularska, E.; Hlebowicz, M.; Olczak, A.; Parczewski, M.; Grzeszczuk, A.; et al. Acquired immune deficiency syndrome (AIDS) and late presentation in Poland-data from Test and Keep in Care (TAK) Polska project. HIV Med. 2021, 22, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Garvey, L.; Winston, A.; Walsh, J.; Post, F.; Porter, K.; Gazzard, B.; Fisher, M.; Leen, C.; Pillay, D.; Hill, T.; et al. HIV- associated central nervous system diseases in the recent combination antiretroviral therapy era. Eur. J. Neurol. 2011, 18, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Hernandez Fustes, O.J.; Arteaga Rodriguez, C. Neurological manifestions of Acquired immunodeficiency Syndrome. Cureus 2020, 12, e10499. [Google Scholar] [CrossRef]
- Yoshino, Y.; Koga, I.; Kitazawa, T.; Oba, H.; Furui, S.; Matsuda, H.; Ota, Y. Magnetic resonance imaging changes inAsia people living with HIV. Infec. Dis. 2021, 53, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kim, S.W.; Chang, H.H.; Kwon, K.T.; Bea, S.; Hwang, S. Trends of Cause of death among Human Immunodeficiency Virus patients and the impact of low CD4 counts on diagnosis to death: A retrospective cohort study. J. Korean Med. Sci. 2020, 35, e355. [Google Scholar] [CrossRef] [PubMed]
- Wojas-Pelc, A.; Pastuszczak, M.; Serwin, A.; Rudnicka, I.; Majewski, S.; Czajkowski, R.; Flisiak, I.; Placek, W.; Maj, J.; Maleszka, R.; et al. Syphilis. Diagnostic and therapeutic recommendations of the Polish Dermatological Society. Part 2: Neurosyphilis, syphilis in pregnancy and congenital syphilis. Dermatol. Rev./Przegląd Dermatol. 2018, 105, 582–592. [Google Scholar] [CrossRef]
- Janocha-Litwin, J.; Mariańska, K.; Serafińska, S.; Simon, K. Manganese encephalopathy among efedron abusers. J. Neuroimaging 2015, 25, 832–855. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Lin, F.; Liu, S.; Da, Y.; Guo, D. Neurological manifestations, laboratory and neuroimaging features in HIV-infected patients. Neurosciences 2017, 22, 311–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, S.R.; Hussain, M.; Habung, H. Neurological manifestations of HIV-AIDS at a tertiary care institute in North Eastern India. Neurol. India 2017, 65, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Bolokadze, N.; Gabunia, P.; Ezugbaia, M.; Gatserelia, L.; Khechiashvili, G. Neurological complications in patients with HIV/AIDS. Georgian Med. News 2008, 165, 34–38. [Google Scholar]
- Berhe, T.; Melkamu, Y.; Amare, A. The pattern and predictors of mortality of HIV/AIDS patients with neurologic manifestation in Ethiopia: A retrospective study. AIDS Res. Ther. 2012, 10, 9–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Fane, M.; Sodqi, M.; Lamdini, H.; Marih, L.; Lahsen, A.O.; Chakib, A.; El Filali, K.M. Manifestations neurologiques centrales chez les patients infectés par le VIH dans le service des maladies infectieuses du CHU de Casablanca, Maroc [Central Neurological Diagnosis in Patients Infected with HIV in the Infectious Diseases Unit of University Hospital of Casablanca, Morocco]. Bull Soc. Pathol. Exot. 2018, 111, 24–30. (In French) [Google Scholar] [CrossRef] [PubMed]
- Janocha-Litwin, J.; Zińczuk, A.; Serafińska, S.; Szymanek-Pasternak, A.; Simon, K. Analysis of deaths among HIV- infected patients hospitalized in 2009–2018 in main centre of Infectious Disease in region of Lower Silesia in Poland, detailing lesions in the central nervous system. Medicina 2022, 58, 270. [Google Scholar] [CrossRef] [PubMed]
- Dai, L.; Mahajan, S.D.; Guo, C.; Zhang, T.; Wang, W.; Li, T.; Jiang, T.; Wu, H.; Li, N. Spectrum of central nervous system disorders in hospitalized HIV/AIDS patients (2009–2011) at a major HIV/AIDS referral center in Beijing, China. J. Neurol. Sci. 2014, 342, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Jung, A.C.; Paauw, D.S. Diagnosing HIV-related disease: Using the CD4 count as a guide. J. Gen. Intern. Med. 1998, 3, 131–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nir, T.M.; On behalf of the HIV Neuroimaging Consortium; Jahanshad, N.; Ching, C.R.K.; Cohen, R.A.; Harezlak, J.; Schifitto, G.; Lam, H.Y.; Hua, X.; Zhong, J.; et al. HIV Neuroimaging Consortium. Progressive brain atrophy in chronically infected and treated HIV+ individuals. J. Neurovirol. 2019, 25, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Sanford, R.; Strain, J.; Dadar, M.; Maranzano, J.; Bonnet, A.; Mayo, N.E.; Scott, S.C.; Fellows, L.K.; Ances, B.M.; Collins, D.L. HIV infection and cerebral small vessel disease are independently associated with brain atrophy and cognitive impairment. AIDS 2019, 33, 1197–1205. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Subgroup A | Number (N = 121) | % of Cases |
|---|---|---|
| Headaches | 50 | 41.3% |
| Limb paresis | 29 | 24.0% |
| Cranial nerve paresis | 5 | 4.1% |
| Impaired consciousness | 23 | 19.0% |
| Speech disorders | 5 | 4.1% |
| Gait and balance disturbance/dizziness | 24 | 19.8% |
| Vision disorders | 15 | 12.4% |
| Epileptic seizures | 14 | 11.6% |
| Behavioural disorders | 18 | 14.9% |
| Entire Group N = 200 | Subgroup with Neurological Symptoms (A) N = 121 | Group with No Neurological Symptoms (B) N = 79 | ||||||
|---|---|---|---|---|---|---|---|---|
| N | Average | Median Value | Average | Median Value | Average | Median Value | ||
| Age | 200 | 41.66 | 41 | 41.28 | 41 | 42.23 | 40 | t = 0.673 p = 0.50 |
| Current CD4 T-lymphocyte count | 195 | 170 | 79 | 174.5 | 80 | 164.41 | 73 | Z = 0.019 p = 0.984 |
| Number of years since diagnosed HIV infection | 200 | 3.7 | 0.5 | 3.72 | 0.5 | 3.68 | 1 | Z = −0.292 p = 0.769 |
| Assessed Variable | Entire Group N = 200 | Subgroup A N = 121 | Subgroup B | N = 79 | Chi2 p | |||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Gender | Female | 37 | 18.5% | 28 | 23.1% | 9 | 11.4% | Chi2 = 4.375 p < 0.05 |
| Male | 163 | 81.5% | 93 | 76.9% | 70 | 88.6% | ||
| HIV transmission routes | Intravenous drug users (IVDU) | 94 | 47.0% | 63 | 52.1% | 31 | 39.2% | Chi2 = 3.16 p = 0.08 |
| Men having sex with men (MSM) | 49 | 24.5% | 21 | 17.4% | 28 | 35.4% | Chi2 = 8.45 p < 0.01 | |
| Heterosexual contacts (HTX) | 46 | 23.0% | 29 | 24.0% | 17 | 21.5% | Chi2 = 0.16 p = 0.69 | |
| Bisexual contacts | 3 | 1.5% | 2 | 1.7% | 1 | 1.3% | Chi2 = 0.14 p = 0.71 | |
| Unknown | 6 | 3.0% | 4 | 3.3% | 2 | 2.5% | Chi2 = 0.01 p = 0.91 | |
| Congenital infection | 3 | 1.5% | 3 | 2.5% | 0 | 0.0% | Chi2 = 0.66 p = 0.42 | |
| Assessed Variable | Entire Group N = 200 | Subgroup A N = 121 | Subgroup B N = 79 | Chi2 p | ||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Death | 31 | 15.5% | 22 | 18.2% | 9 | 11.4% | Chi2 = 1.68 p = 0.19 | |
| Late presenters | 104 | 52% | 65 | 52.7% | 39 | 49.4% | Chi2 = 0.36 p = 0.55 | |
| ARV treatment | de novo | 77 | 38.5% | 47 | 38.8% | 30 | 38.0% | Chi2 = 0.05 p = 0.98 |
| YES | 74 | 37% | 45 | 37.2% | 29 | 36.7% | ||
| NO | 49 | 24.5% | 29 | 24.0% | 20 | 25.3% | ||
| Entire group N = 1P96 | Subgroup A N = 117 | Subgroup B N = 79 | Entire group N = 156 | Subgroup A N = 103 | Subgroup B N = 53 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anti-HCV reactive | T. gondii IgG positive | |||||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | |
| YES | 76 | 38.8% | 46 | 39.3% | 30 | 38.0% | 79 | 57 | 55.3% | 22 | 41.5% | |
| NO | 120 | 61.2% | 71 | 60.7% | 49 | 62.0% | 77 | 46 | 44.7% | 31 | 58.5% | |
| Chi2 p | Chi2 = 0.36 p = 0.85 | Chi2 = 2.68 p = 0.10 | ||||||||||
| Entire group N = 195 | Subgroup A N = 79 | Subgroup B N = 116 | Entire group N = 195 | Subgroup A N = 116 | Subgroup B N = 79 | |||||||
| HBsAg positive | Latent HBV infection (HBsAg negative, anti HBc total positive) | |||||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | |
| YES | 15 | 7.7% | 11 | 9.5% | 4 | 5.1% | 58 | 29.7% | 34 | 29.3% | 24 | 30.4% |
| NO | 180 | 92.3% | 105 | 90.5% | 75 | 94.9% | 137 | 70.3% | 82 | 70.7% | 55 | 69.6% |
| Chi2 p | Chi2 = 0.75 p = 0.39 | Chi2 = 0.26 p = 0.87 | ||||||||||
| Entire group N = 183 | Subgroup A N = 110 | Subgroup B N = 73 | Entire group N = 52 | Subgroup A N = 23 | Subgroup B N = 29 | |||||||
| VDRL positive | Positive syphilis test | |||||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | |
| YES | 57 | 31.2% | 25 | 22.7% | 32 | 43.8% | 42 | 80.8 % | 15 | 65.2% | 27 | 93.1% |
| NO | 126 | 68.8% | 85 | 77.3% | 41 | 56.2% | 10 | 19.2% | 8 | 34.8% | 2 | 6.9% |
| Chi2 p | Chi2 = 9.12 p < 0.01 | Chi2 = 4.75 p < 0.05 | ||||||||||
| CNS CHANGES | Entire Group N = 200 | Subgroup A N = 121 | Subgroup B N = 79 | Chi2 p | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| CNS toxoplasmosis | 27 | 13.5% | 25 | 20.7% | 2 | 2.5% | Chi2 = 13.45 p < 0.001 |
| CNS cryptococcosis | 14 | 7% | 14 | 11.6% | 0 | 0% | Chi2 = 8.13 p < 0.01 |
| PML | 19 | 9.5% | 16 | 13.2% | 3 | 3.8% | Chi2 = 3.9 p < 0.05 |
| CNS tuberculosis | 3 | 1.5% | 3 | 2.5% | 0 | 0% | Chi2 = 0.66 p = 0.41 |
| Neuroinfection | 6 | 3.0% | 6 | 5.0% | 0 | 0% | Chi2 = 2.51 p = 0.11 |
| Stroke | 2 | 1.0% | 2 | 1.7% | 0 | 0% | Chi2 = 0.17 p = 0.67 |
| Neurosyphilis | 16 | 8.0% | 8 | 6.6% | 8 | 10.1% | Chi2 = 0.4 p = 0.53 |
| Other | 10 | 5.0% | 6 | 5.0% | 4 | 5.1% | Chi2 = 0.09 p = 0.77 |
| Entire Group N = 200 | Subgroup A N = 121 | Subgroup B N = 79 | Chi2 p | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Vascular changes | 35 | 17.5% | 25 | 20.6% | 10 | 12.7% | Chi2 = 2.12 p = 0.14 |
| Cortical and subcortical atrophy | 22 | 11.0% | 14 | 11.6% | 8 | 10.1% | Chi2 = 0.08 p = 0.09 |
| CNS Cryptococcosis N = 14 | Toxoplasmosis CNS N = 25 | PML N = 17 | H p | ||||
|---|---|---|---|---|---|---|---|
| Average | Median Value | Average | Median Value | Average | Median Value | ||
| Age (number of years) | 40.35 | 41 | 38.32 | 38 | 43.82 | 45 | H = 5.19 p = 0.07 |
| CD 4 T-lymphocyte count | 30.64 | 22 | 84.9 | 47 | 100.53 | 27 | H = 5.66 p = 0.70 |
| How many years since the infection | 3.28 | 0 | 2.1 | 0 | 2.9 | 0 | H = 0.7 p = 0.70 |
| CNS Cryptococcosis N = 14 | Toxoplasmosis CNS N = 25 | PML N = 17 | Chi2 p | |||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Gender | Female | 1 | 7.1 | 10 | 40% | 3 | 17.7% | Chi2 = 5.87 p = 0.05 |
| Male | 13 | 92.9% | 15 | 60% | 14 | 82.4% | ||
| Late presenters | 11 | 78.6% | 21 | 84% | 12 | 70.6% | Chi2 = 1.08 p = 0.58 | |
| Transmission routes | IVDU | 8 | 57.1% | 4 | 16% | 8 | 47.1% | Chi2 = 7.98 p < 0.05 |
| MSM | 2 | 14.3% | 8 | 32% | 2 | 11.8% | Chi2 = 3.03 p = 0.22 | |
| HTX | 4 | 28.6% | 11 | 44% | 4 | 23.5% | Chi2 = 2.13 p = 0.34 | |
| BI | 0 | 0% | 0 | 0% | 1 | 5.9% | Chi2 = 2.34 p = 0.31 | |
| Congenital | 1 | 7.1% | 1 | 4% | 1 | 5.9% | Chi2 = 0.19 p = 0.91 | |
| Unknown | 0 | 0% | 1 | 4% | 1 | 5.9% | Chi2 = 0.8 p = 0.67 | |
| ARV treatment | de novo | 6 | 42.9% | 17 | 68% | 9 | 52.9% | Chi2 = 5.09 p = 0.28 |
| YES | 2 | 14.3% | 5 | 20% | 4 | 23.5% | ||
| NO | 6 | 42.9% | 3 | 12% | 4 | 23.5% | ||
| Death | 2 | 14.3% | 5 | 20% | 10 | 58.8% | Chi2 = 9.49 p < 0.01 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janocha-Litwin, J.; Simon, K. Neurological Disorders of Patients Living with HIV Hospitalized in Infectious Departments of the Specialist Hospital in Lower Silesia in Poland. Healthcare 2022, 10, 1481. https://doi.org/10.3390/healthcare10081481
Janocha-Litwin J, Simon K. Neurological Disorders of Patients Living with HIV Hospitalized in Infectious Departments of the Specialist Hospital in Lower Silesia in Poland. Healthcare. 2022; 10(8):1481. https://doi.org/10.3390/healthcare10081481
Chicago/Turabian StyleJanocha-Litwin, Justyna, and Krzysztof Simon. 2022. "Neurological Disorders of Patients Living with HIV Hospitalized in Infectious Departments of the Specialist Hospital in Lower Silesia in Poland" Healthcare 10, no. 8: 1481. https://doi.org/10.3390/healthcare10081481