
Something Happened with the Way We Work: Evaluating the Implementation of the Reducing Coercion in Norway (ReCoN) Intervention in Primary Mental Health Care

 ,
,
Abstract
:1. Introduction
1.1. The Service and Legal Context
1.2. The ReCoN Intervention and Implementation Plan
- In each site, two or three staff from the municipal mental health service were allocated the role of ‘ReCoN coordinators’. An informal working group was established in each municipality. These consisted of coordinators plus the service managers considered appropriate, so varied between sites. In one site, representatives from the user and carer organisations were included.
- A detailed implementation manual was produced by the researchers. This included the rationale and evidence for each strategy area and details of actions with specified responsibilities and suggested timelines [17]. It also contained templates for post-incident reviews and joint crisis plans, to be used or adapted for strategy area 2.
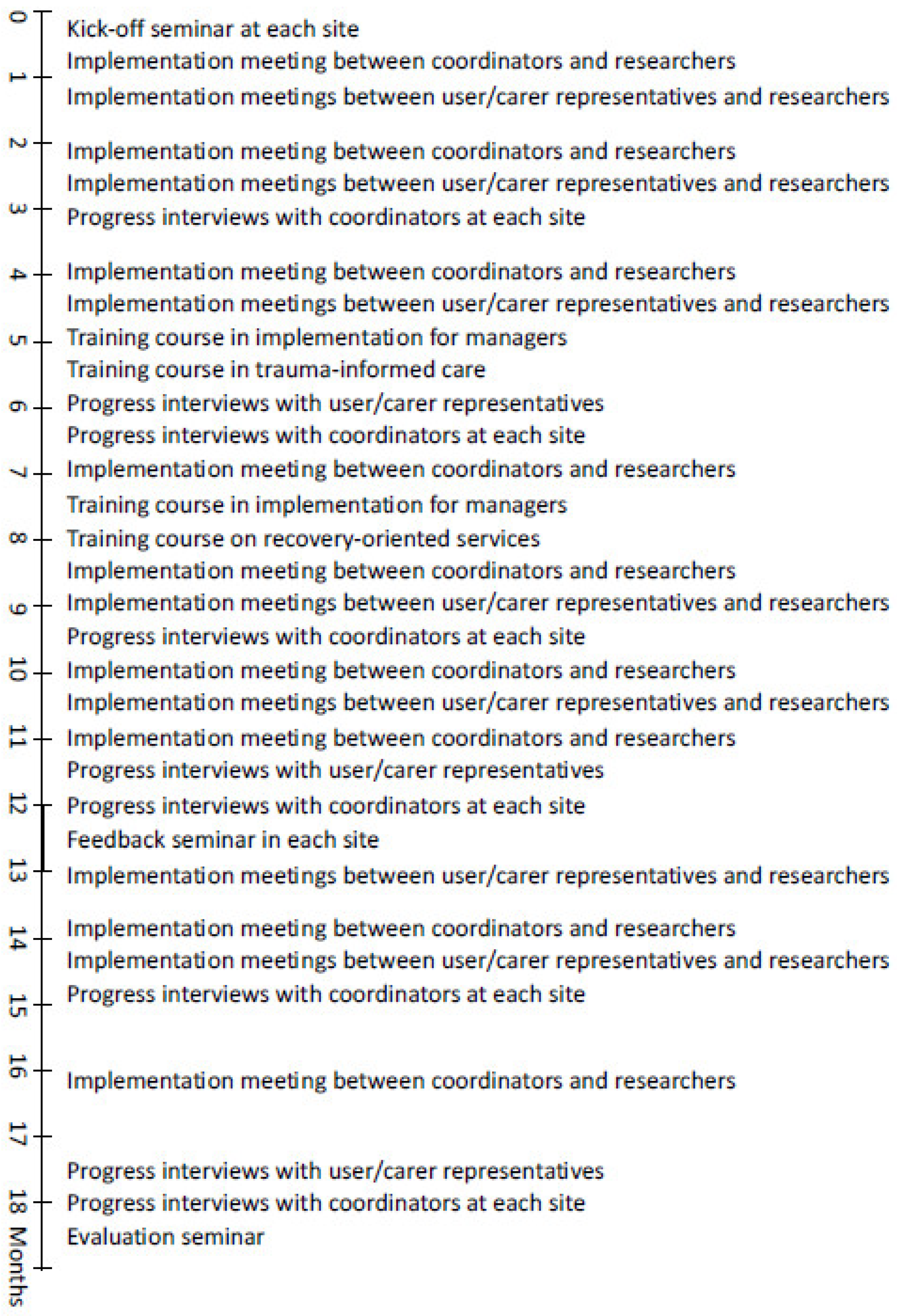
- A kick-off seminar was organized by coordinators in each municipality, to which relevant stakeholders were invited. The aim was to mark the start of the intervention period and to create enthusiasm and ownership locally.
- Implementation meetings between coordinators across the five municipalities and researchers took place online every two months to discuss progress. The nine meetings focused on ‘problem-solving’ particular actions that someone struggled with through discussion and exchange of experiences across sites.
- Separate implementation meetings were also held between the research team and local users and organisations, respectively. A total of 13 meetings focused on users and carers involvement in implementation, and the experiences captured were fed into subsequent implementation meetings with coordinators.
- Training courses were arranged by the research team on recovery-oriented services and trauma-informed care to support professional development as part of Strategy Area 3. The latter included a module on implementation issues aimed at managers. Training in the assessment of decision-making capacity was available online.
- A ReCoN newsletter was produced by the researchers and circulated by email every three months, featuring information about implementation progress and national research on involuntary care. A Facebook group also kept those interested updated.
- At the 12-month point, seminars aimed to take stock of progress and boost motivation for the last six months were held in each site, to which all stakeholders were invited.

2. Materials and Methods
2.1. Design and Data Collection
2.2. Analysis
2.3. Ethics
3. Results
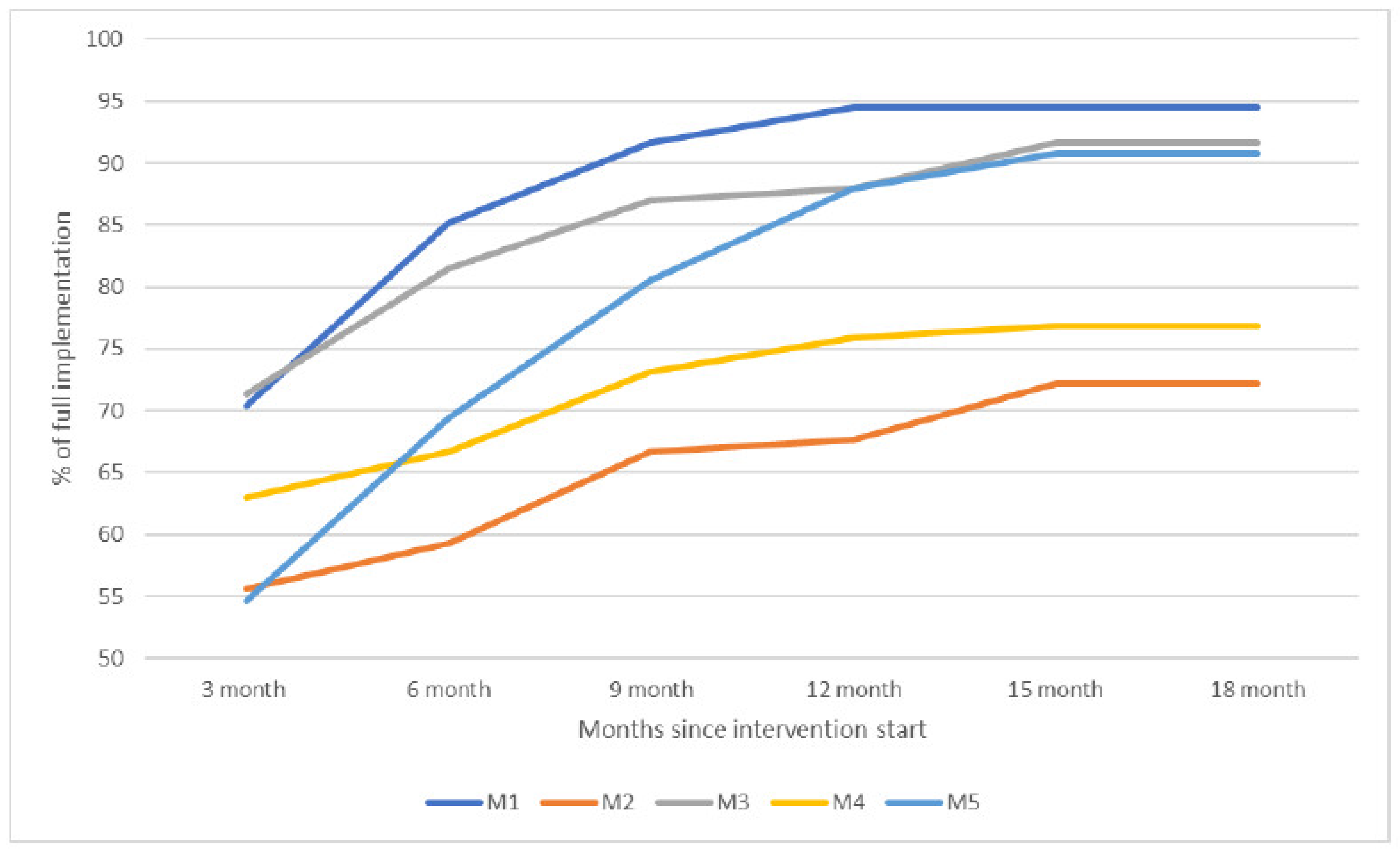
3.1. To What Extent Was the Intervention Implemented?
3.2. What Helped or Hindered Implementation?
3.2.1. Overarching Themes
“The pandemic has had a huge negative effect because we could not meet in person… Collaborating with other services has been much harder. All the work with vaccination and contact tracing has taken a lot of the time and resources of everyone working in municipal health services.”M2
“The regular and close follow-up from the research team throughout the implementation has been a success factor. It’s helped the project keep momentum.”M4
“The systematic way of working that ReCoN entails has been good, and this has spill-over effects into other parts of our work too. For example, our future plans narrow focus down to 2–3 areas that we will focus properly on”M5
“We are now cooperating more closely within the municipality and with specialist services, to stabilize the everyday lives of users when they live at home, in order to break patterns of frequent compulsory hospitalizations… This has a lot to do with attitudes to act in ways other than simply admitting.”M3
3.2.2. Strategy Area 1: Management
“We should have anchored the project differently. We anchored it at a high managerial level, but they were too far removed from service delivery, staff, and users. We did not achieve stable anchorage at lower managerial level … which has meant that it has been difficult to create enthusiasm and commitment among staff, and to prioritize systematic work with intervention across departments.”M4
“The monitoring figures and the “hands-on” from the top are crucial factors. What would have happened to some of these people if we hadn’t known about them? Now we have an overview that we didn’t have before, and we have been able to deal with more holistic follow-up, housing, and treatment for those where we identify need.”M3
“Focusing on the project’s stories of success has in itself been a success story. We share success stories [from clinical practice with the target population] as a regular part of the agenda of management meetings. It provides motivation and stimulus… it promotes learning of what different services do and… gives recognition for the work you do.”M5
3.2.3. Strategy Area 2: Involving Persons with Lived Experience and Family Carers
“One of our successes is that we’ve achieved a unique collaboration with the user organizations at the system level. They have been very useful and contributed a lot in terms of service development…We have been fortunate in that these organizations have competent representatives willing to spend time on this… There has been mutual learning.”M5
“Information has not been a problem, but it hasn’t been that easy to get involved in the ‘bigger’ things such as the development of social activities or accommodation issues. As far as involvement in the evaluation of the intervention is concerned, we can’t say we’ve really participated in that. Involvement worked fine the first year, but nothing much has happened in the last six months.”M4
“Post-incidence reviews were one of the things that were new to us. It is now well established for those in our services who have been involuntarily admitted, but they can be challenging to achieve… Every case with a post-incidence review kind of becomes a quality improvement job regarding how those involved work and collaborate. It gives insight and promotes cooperation for all those involved.”M5
3.2.4. Strategy Area 3: Competence Development
“They learned that a person might appear angry when the user actually felt scared and unsafe. Awareness of this made them focus on making the user safe instead of being afraid of them, and this meant they got a much better relationship with her.”M4
3.2.5. Strategy Area 4: Collaboration across Primary and Specialist Care Levels
“We didn’t experience an enormous amount of enthusiasm among managers in the local specialist services when we informed them about the intervention. It was kind of “you do your work and we’ll do ours”… It’s not that easy to gain enthusiasm and commitment in specialist services to projects initiated by the municipality.”M3
“We got in place regular monthly meetings between municipal services, the FACT team, the wards, and the CMHC. Since then, it’s run smoothly. It’s been very good and has transfer-value to other parts of service delivery as well. Things get easier when we meet. I sort of notice a before-and-after effect. We’d been working for a while prior to ReCoN to get better collaboration, so when we got this joint meeting in place, it became the high point of what we’d been trying to achieve over time.”M1
“We still have people being discharged without the municipality having been notified that they were admitted. This could be because the user doesn’t want the municipality involved, or that the admission is very brief and that there is no time to contact the municipality before discharge.”M3
“Now we in municipal services also have ownership as regards involuntary care… Now we dare ask questions and make demands. Something happened with the way we work on these cases and how we cooperate on them.”M5
“Covid was a driver for establishing structured, regular collaboration with specialist services. It’s much easier to set up joint digital meetings than getting everyone to attend in person. Due to Covid, all services got online and developed a culture for online meetings.”M1
3.2.6. Strategy Area 5: Collaboration within the Primary Care Level
“Sharing experiences and success stories across services also provides knowledge about each other, and everyone becomes aware of other services.”M5
“GPs have too much—they are ‘vaccinated’ against things coming from the outside. They have an information overload aimed at them.”M2
3.2.7. Strategy Area 6: Tailoring Individual Services
“We’ve had about 100 bed days at the Municipal Acute Unit, for 21 users. We see that a few of them are referred on, which is good. This has slowed the deterioration of symptoms. In some cases, we’ve also used Municipal Acute Units before a rehab placement to ensure that the person makes it there.”M3
“Getting figures from the hospital has helped us identify about five people with frequent involuntary admissions. We have worked extensively with these people and we have found individualised, good solutions for them so that they have managed to break the patterns of admissions. What has helped have primarily been (our) increased awareness; collaboration with the hospital; more tailored living situation, and; better cooperation with the FACT team.”M1
“This young person, with serious mental illness and also somatic disease, has shifted from regular involuntary admissions to voluntary ones. The structured work with joint crisis plans and post-incident reviews has been among the success factors here. … We have established a stable team of good professionals around this person, built relationships, and things have improved. This also applies to the collaboration with the hospital and CHMC, although this varies a bit…We are now looking at this person’s housing situation and whether it contributes to making them worse rather than promoting recovery … We need to upgrade both this person’s housing and the competence of the professionals involved.”M5
4. Discussion
4.1. Establishing and Maintaining a Shared Agenda: Leadership and Anchoring
4.2. Stimulating a Culture for Change
4.3. Clarifying the Role of User Involvement
4.4. Supporting Implementation and Intervention Sustainability
4.5. How the Intervention Should Be Modified or Adapted in Future Implementation
4.6. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Whittington, R.; Aluh, D.O.; Caldas-de-Almeida, J.-M. Zero Tolerance for Coercion? Historical, Cultural and Organisational Contexts for Effective Implementation of Coercion-Free Mental Health Services around the World. Healthcare 2023, 11, 2834. [Google Scholar] [CrossRef] [PubMed]
- Council of Europe. Good Pratices in the Council of Europe to Promote Voluntary Measures in Mental Health Services; Council of Europe: Strasbourg, France, 2021. [Google Scholar]
- The, L. Institutional and coercive mental health treatment in Europe. Lancet 2018, 391, 282. [Google Scholar] [CrossRef]
- World Health Organization. Hospital-Based Mental Health Services: Promoting Person-Centred and Rights-Based Approaches; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Good, N.; Perry, E.; Rae, S.; Rose, D. Service user perspectives on coercion and restraint in mental health. BJPsych. Int. 2017, 14, 59–61. [Google Scholar] [CrossRef]
- Sheridan Rains, L.; Zenina, T.; Dias, M.C.; Jones, R.; Jeffreys, S.; Branthonne-Foster, S.; Lloyd-Evans, B.; Johnson, S. Variations in patterns of involuntary hospitalisation and in legal frameworks: An international comparative study. Lancet Psychiatry 2019, 6, 403–417. [Google Scholar] [CrossRef] [PubMed]
- Sunkel, C.; Saxena, S. Rights-based mental health care. Lancet Psychiatry 2019, 6, 9–10. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Care. Better Quality—Increased Voluntariness. National Strategy for Increased Voluntariness in Mental Health Care 2012–2015. 2012. Available online: https://www.regjeringen.no/globalassets/upload/hod/bedrekvalitet-okt_frivillighet.pdf (accessed on 6 July 2012).
- Ruud, T.; Friis, S. Community-based Mental Health Services in Norway. Consort. Psychiatr. 2021, 2, 47–54. [Google Scholar] [CrossRef]
- Gooding, P.; McSherry, B.; Roper, C. Preventing and reducing ‘coercion’ in mental health services: An international scoping review of English-language studies. Acta Psychiatr. Scand. 2020, 142, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, S.; Steinert, T. Measures to Avoid Coercion in Psychiatry and Their Efficacy. Dtsch. Arztebl. Int. 2019, 116, 336–343. [Google Scholar] [CrossRef]
- Marshall, M.; Lockwood, A. Assertive community treatment for people with severe mental disorders. Cochrane Database Syst. Rev. 2000, Cd001089. [Google Scholar] [CrossRef]
- Stock, C.; Dias, S.; Dietrich, T.; Frahsa, A.; Keygnaert, I. Editorial: How can We Co-Create Solutions in Health Promotion with Users and Stakeholders? Front. Public Health 2021, 9, 773907. [Google Scholar] [CrossRef]
- Lantta, T.; Duxbury, J.; Haines-Delmont, A.; Björkdahl, A.; Husum, T.L.; Lickiewicz, J.; Douzenis, A.; Craig, E.; Goodall, K.; Bora, C.; et al. Models, frameworks and theories in the implementation of programs targeted to reduce formal coercion in mental health settings: A systematic review. Front. Psychiatry 2023, 14, 1158145. [Google Scholar] [CrossRef]
- Rugkasa, J.; Tveit, O.G.; Berteig, J.; Hussain, A.; Ruud, T. Collaborative care for mental health: A qualitative study of the experiences of patients and health professionals. BMC Health Serv. Res. 2020, 20, 844. [Google Scholar] [CrossRef]
- The Norwegian Parliament. Norwegian Mental Health Act; The Norwegian Parliament: Oslo, Norway, 1999. [Google Scholar]
- Wormdahl, I.; Hatling, T.; Husum, T.L.; Kjus, S.H.H.; Rugkasa, J.; Brodersen, D.; Christensen, S.D.; Nyborg, P.S.; Skolseng, T.B.; Odegard, E.I.; et al. The ReCoN intervention: A co-created comprehensive intervention for primary mental health care aiming to prevent involuntary admissions. BMC Health Serv. Res. 2022, 22, 931. [Google Scholar] [CrossRef] [PubMed]
- Wormdahl, I.; Husum, T.L.; Rugkåsa, J.; Rise, M.B. Professionals’ perspectives on factors within primary mental health services that can affect pathways to involuntary psychiatric admissions. Int. J. Ment. Health Syst. 2020, 14, 86. [Google Scholar] [CrossRef] [PubMed]
- Wormdahl, I.; Husum, T.L.; Kjus, S.H.H.; Rugkasa, J.; Hatling, T.; Rise, M.B. Between No Help and Coercion: Toward Referral to Involuntary Psychiatric Admission. A Qualitative Interview Study of Stakeholders’ Perspectives. Front. Psychiatry 2021, 12, 708175. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, P.; De Ruysscher, C. From monologue to dialogue in mental health care research: Reflections on a collaborative research process. Disabil. Soc. 2020, 35, 1274–1289. [Google Scholar] [CrossRef]
- Gustavsen, B. Theory and Practice: The Mediation Discourse. In Handbook of Action Research, 1st ed.; Reason, P., Bradbury, H., Eds.; SAGE: London, UK, 2001; pp. 17–26. [Google Scholar]
- Huckshorn, K.A.; CAP, I.; Director, N. Six Core Strategies for Reducing Seclusion and Restraint Use; National Association of State Mental Health Program Directors (NATC): Alexandria, Egypt, 2005. [Google Scholar]
- Riahi, S.; Dawe, I.C.; Stuckey, M.I.; Klassen, P.E. Implementation of the six core strategies for restraint minimization in a specialized mental health organization. J. Psychosoc. Nurs. Ment. Health Serv. 2016, 54, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Goulet, M.-H.; Larue, C.; Dumais, A. Evaluation of seclusion and restraint reduction programs in mental health: A systematic review. Aggress. Violent Behav. 2017, 34, 139–146. [Google Scholar] [CrossRef]
- Hatling, T.; Husum, T.L.; Kjus, S.H.H.; Wormdahl, I. ReCoN Intervensjonen. Strategier for Redusert Bruk av Tvangsinnleggelser [The ReCoN Intervention. Strategies to Reduce Involuntary Admissions]; Norwegian Resource Centre for Community Mental Health: Trondheim, Norway, 2020. [Google Scholar]
- Clarke, V.; Braun, V. Thematic analysis. J. Posit. Psychol. 2017, 12, 297–298. [Google Scholar] [CrossRef]
- Denzin, N.K.; Lincoln, Y.S. The SAGE Handbook of Qualitative Research; SAGE Publications: Thousand Oaks, CA, USA, 2011. [Google Scholar]
- Anderson, C. Presenting and evaluating qualitative research. Am. J. Pharm. Educ. 2010, 74, 141. [Google Scholar] [CrossRef]
- Powell, B.J.; Fernandez, M.E.; Williams, N.J.; Aarons, G.A.; Beidas, R.S.; Lewis, C.C.; McHugh, S.M.; Weiner, B.J. Enhancing the Impact of Implementation Strategies in Healthcare: A Research Agenda. Front. Public Health 2019, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Wood, E.; Ohlsen, S.; Ricketts, T. What are the barriers and facilitators to implementing Collaborative Care for depression? A systematic review. J. Affect. Disord. 2017, 214, 26–43. [Google Scholar] [CrossRef] [PubMed]
- McDaid, S. An equality of condition framework for user involvement in mental health policy and planning: Evidence from participatory action research. Disabil. Soc. 2009, 24, 461–474. [Google Scholar] [CrossRef]
- Sakellari, E.; Tsoukas, K.; Kolaitis, G.; Lagiou, A. The model of co-production in mental health services. Psychiatriki 2023, 34, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Jackson, C.; Shaw, S.; Janamian, T. Achieving Research Impact Through Co-creation in Community-Based Health Services: Literature Review and Case Study. Milbank Q. 2016, 94, 392–429. [Google Scholar] [CrossRef]
- Becker, T.; Puschner, B. Complex interventions in mental health services research. In Improving Mental Health Care; Wiley: Hoboken, NJ, USA, 2013; pp. 131–144. [Google Scholar] [CrossRef]
- Johnston, S.; Liddy, C.; Hogg, W.; Donskov, M.; Russell, G.; Gyorfi-Dyke, E. Barriers and facilitators to recruitment of physicians and practices for primary care health services research at one centre. BMC Med. Res. Methodol. 2010, 10, 109. [Google Scholar] [CrossRef]
- Johnston, J.L.; Bennett, D. Lost in translation? Paradigm conflict at the primary–secondary care interface. Med. Educ. 2019, 53, 56–63. [Google Scholar] [CrossRef] [PubMed]
- van Melle, A.L.; van der Ham, A.J.; Widdershoven, G.A.M.; Voskes, Y. Implementation of High and Intensive Care (HIC) in the Netherlands: A Process Evaluation. Psychiatr. Q. 2021, 92, 1327–1339. [Google Scholar] [CrossRef] [PubMed]
- Henderson, C.; Farrelly, S.; Moran, P.; Borschmann, R.; Thornicroft, G.; Birchwood, M.; Crimson, T.; Joshua. Joint crisis planning in mental health care: The challenge of implementation in randomized trials and in routine care. World Psychiatry 2015, 14, 281–283. [Google Scholar] [CrossRef]
- Allchin, B.; Goodyear, M.; O’Hanlon, B.; Weimand, B.M. Leadership perspectives on key elements influencing implementing a family-focused intervention in mental health services. J. Psychiatr. Ment. Health Nurs. 2020, 27, 616–627. [Google Scholar] [CrossRef]
- Nilsen, P.; Birken, S.A. Handbook on Implementation Science; Edward Elgar Publishing: Cheltenham, UK, 2020. [Google Scholar]
- Loorbach, D. Transition management. In New Mode of Governance for Sustainable Development; International Books: Utrecht, The Netherlands, 2007. [Google Scholar]
- Kjus, S.H.H.; Hatling, T. Brukerinvolvering i forskning (User involvement in research). Tidsskr. Nor. Psykologforening 2022, 59, 498–505. [Google Scholar]
- Bee, P.; Brooks, H.; Fraser, C.; Lovell, K. Professional perspectives on service user and carer involvement in mental health care planning: A qualitative study. Int. J. Nurs. Stud. 2015, 52, 1834–1845. [Google Scholar] [CrossRef] [PubMed]
- Mutschler, C.; Bellamy, C.; Davidson, L.; Lichtenstein, S.; Kidd, S. Implementation of peer support in mental health services: A systematic review of the literature. Psychol. Serv. 2022, 19, 360–374. [Google Scholar] [CrossRef]
- Bertram, R.M.; Blase, K.A.; Fixsen, D.L. Improving programs and outcomes: Implementation frameworks and organization change. Res. Soc. Work. Pract. 2015, 25, 477–487. [Google Scholar] [CrossRef]
- Fixsen, D.; Blase, K.; Metz, A.; Van Dyke, M. Statewide Implementation of Evidence-Based Programs. Except. Child. 2013, 79, 213–230. [Google Scholar] [CrossRef]
- Svensson, B.; Hansson, L.; Markström, U.; Lexén, A. What matters when implementing Flexible Assertive Community Treatment in a Swedish healthcare context: A two-year implementation study. Int. J. Ment. Health 2017, 46, 284–298. [Google Scholar] [CrossRef]
- Hansson, K.M.; Romøren, M.; Pedersen, R.; Weimand, B.; Hestmark, L.; Norheim, I.; Ruud, T.; Hymer, I.S.; Heiervang, K.S. Barriers and facilitators when implementing family involvement for persons with psychotic disorders in community mental health centres—A nested qualitative study. BMC Health Serv. Res. 2022, 22, 1153. [Google Scholar] [CrossRef] [PubMed]
- Hestmark, L.; Romøren, M.; Heiervang, K.S.; Hansson, K.M.; Ruud, T.; Šaltytė Benth, J.; Norheim, I.; Weimand, B.; Pedersen, R. Implementation of Guidelines on Family Involvement for Persons with Psychotic Disorders (IFIP): A Cluster Randomised Controlled Trial. Adm. Policy Ment. Health 2023, 50, 520–533. [Google Scholar] [CrossRef]
- Eisman, A.B.; Quanbeck, A.; Bounthavong, M.; Panattoni, L.; Glasgow, R.E. Implementation science issues in understanding, collecting, and using cost estimates: A multi-stakeholder perspective. Implement. Sci. 2021, 16, 75. [Google Scholar] [CrossRef] [PubMed]
- Campbell, N.C.; Murray, E.; Darbyshire, J.; Emery, J.; Farmer, A.; Griffiths, F.; Guthrie, B.; Lester, H.; Wilson, P.; Kinmonth, A.L. Designing and evaluating complex interventions to improve health care. Bmj 2007, 334, 455–459. [Google Scholar] [CrossRef]
- Chien, W.-T. Strategies in Evaluation of Complex Health Care Interventions for People with Physical or Mental Health Issues; Nova Science Publishers: New York, NY, USA, 2009. [Google Scholar]


{kind=link}
{kind=link}
| Strategy Area 1: Management |
|---|
| 1.1. Management anchoring |
| Management anchoring in relevant organisations/services in the municipality |
| Appoint a minimum of two project coordinators |
| Anchoring support for the primary mental health services’ implementation of the intervention in relevant collaborating services at both primary and specialist care levels |
| Management support, facilitation, and prioritisation to enable implementation of actions |
| 1.2. Data monitoring—use of data in service development |
| Develop a plan for how to collect and use data: what, how, who should collect it, how often, and how it should be used |
| Establish routines for registering data based on the above data monitoring |
| Establish routines for utilising the data based on the data monitoring plan, e.g., every unit/service examines and evaluates the data for their unit/service in their regular staff meeting |
| Evaluating progress over time |
| 1.3. Continuous service improvement |
| Establish routines for documenting situations that led to referrals for involuntary admissions and for “success stories” where this was prevented |
| Examine and evaluate all situations that lead to referrals to involuntary admissions and “success stories” where this was prevented every third month |
| Communicate the results from such evaluative work and apply it in service improvement work |
| Strategy Area 2: Involving Persons with Lived Experience and Family Carers |
| 2.1. Involving persons with lived experience and family carers at the organisational level |
| Invite local user and carer organisations, Municipal User Boards, or other user representatives to participate in the intervention |
| User representatives participate in evaluative work |
| User representatives participate in the evaluation and reflection on referrals to involuntary admissions every third month |
| 2.2. Post-incident review |
| Establish routines for offering those referred to or discharged from an involuntary admission a post-incidence review |
| Conduct post-incident reviews after each involuntary admission |
| Conduct post-incident reviews after each referral for involuntary admission |
| Establish routines for contacting family carers of individuals who have been involuntarily admitted or referred to such admission to check if they want a post-incident review. |
| Contact and conduct a post-incident review with family carers who were not part of such reviews of those referred to or involuntarily admitted |
| 2.3. Joint crisis plan |
| Examine whether all those involuntarily admitted during the last 12 months, or who are deemed to be at risk for such admission, have a joint crisis plan, and produce a joint crisis plan for those who do not have one |
| Establish routines to secure that up-to-date joint crisis plans are anchored in and available to involved services (consent needed) |
| Prepare a joint crisis plan for all those discharged from an involuntary admission. |
| Update the joint crisis plan, together with the individual, at least every sixth month, and always after a crisis or an involuntary admission |
| 2.4. Peer worker |
| The municipal mental health services have peer worker(s) with relevant lived experience who work closely with individuals at risk of involuntary admission. |
| Strategy Area 3: Competence Development |
| 3.1. Recovery-oriented framework |
| Have an explicit principle of a recovery-oriented foundation for service provision |
| 3.2. Competence-building measures |
| All relevant services/staff participate in a three-hour digital course in assessing decision-making capacity |
| People with a mental illness and their family carers and network could be encouraged to undertake the digital course in assessing decision-making capacity |
| A one-day training course on recovery-orientated services |
| Training course in trauma-informed care |
| Strategy Area 4: Collaboration across Primary and Specialist Care Levels |
| 4.1. Collaboration when assessing someone for involuntary admission |
| Getting support from the specialist mental health service provided when assessing individuals’ capacity to consent to treatment, especially when there is uncertainty |
| Collaborating with specialist services on finding alternatives to involuntary admissions |
| Establish routines for primary mental health services to be notified when an individual is referred to involuntary admission, but such an admission is not established |
| 4.2. Collaboration during and following involuntary admission |
| Collaborate with specialist mental health care on conducting post-incident reviews after each involuntary admission |
| Collaborate on preparing joint crisis plans during admissions (Can form part of the “discharge meeting” below) |
| The relevant primary care services participate in discharge meetings from involuntary admissions |
| 4.3. Joint meeting points |
| Joint evaluation meetings at the management level. Can take place on existing meeting areas at the managerial level |
| Primary and specialist services participate in ‘case collaboration meetings’ for individuals at risk of involuntary admissions |
| Strategy Area 5: Collaboration within the Primary Care Level |
| 5.1. Collaboration between GPs/A&E services and the primary mental health services |
| Familiarise local GPs with the intervention in collaboration with the chief municipal medical officer |
| Provide an overview of available primary care level services that might provide alternatives to involuntary admission |
| Communicate/disseminate this overview to all collaborating GPs and emergency medical services |
| 5.2. Joint meeting points |
| Establish ‘case management meetings’ for all individuals at risk of involuntary admissions if these are not already in place |
| Have reduction of involuntary admissions on the agenda of meetings at the managerial level |
| Arrange a kick-off seminar of the intervention period with relevant services from primary services and other stakeholders such as user and carer organisations and specialist services. |
| Arrange a day for joint professional development on recovery-orientation |
| Strategy Area 6: Tailoring Individual Services |
| 6.1. Individually tailored accommodation |
| Assess, during discharge meetings/post-incidence reviews, whether someone’s current accommodation is appropriate and stable |
| 6.2. Primary level crisis or short-term placement |
| Establish primary crisis retreats or short-term institutional places, or, if already present, evaluate how such beds are utilised |
| Use such services for those in the target group when the individual and services assess it to be appropriate |
| 6.3. Support for meaningful everyday lives |
| Establish collaboration with the Labour and Welfare Organisation for those in the target group who are eligible for and wish to receive these services |
| Assess the need for support, offered by the municipality, to engage in social interaction and leisure activities |
| Assist individuals in the target group to seek economic support from the municipality to participate in activities they want and need |
| Assist individuals in the target group with transport to and from activities if they need and wish it |
| Assess needs and consider appropriate actions to help individuals manage their sleep, diet, exercise, and money |
| The case manager is involved in an individual’s interaction with his/her GP follow-up regarding medication |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Husum, T.L.; Wormdahl, I.; Kjus, S.H.H.; Hatling, T.; Rugkåsa, J. Something Happened with the Way We Work: Evaluating the Implementation of the Reducing Coercion in Norway (ReCoN) Intervention in Primary Mental Health Care. Healthcare 2024, 12, 786. https://doi.org/10.3390/healthcare12070786
Husum TL, Wormdahl I, Kjus SHH, Hatling T, Rugkåsa J. Something Happened with the Way We Work: Evaluating the Implementation of the Reducing Coercion in Norway (ReCoN) Intervention in Primary Mental Health Care. Healthcare. 2024; 12(7):786. https://doi.org/10.3390/healthcare12070786
Chicago/Turabian StyleHusum, Tonje Lossius, Irene Wormdahl, Solveig H. H. Kjus, Trond Hatling, and Jorun Rugkåsa. 2024. "Something Happened with the Way We Work: Evaluating the Implementation of the Reducing Coercion in Norway (ReCoN) Intervention in Primary Mental Health Care" Healthcare 12, no. 7: 786. https://doi.org/10.3390/healthcare12070786