
Tracking Listening Skill Development in Infants and Children with Hearing Loss: A Normative Dataset for the Functional Listening Index—Paediatric (FLI-P®)
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
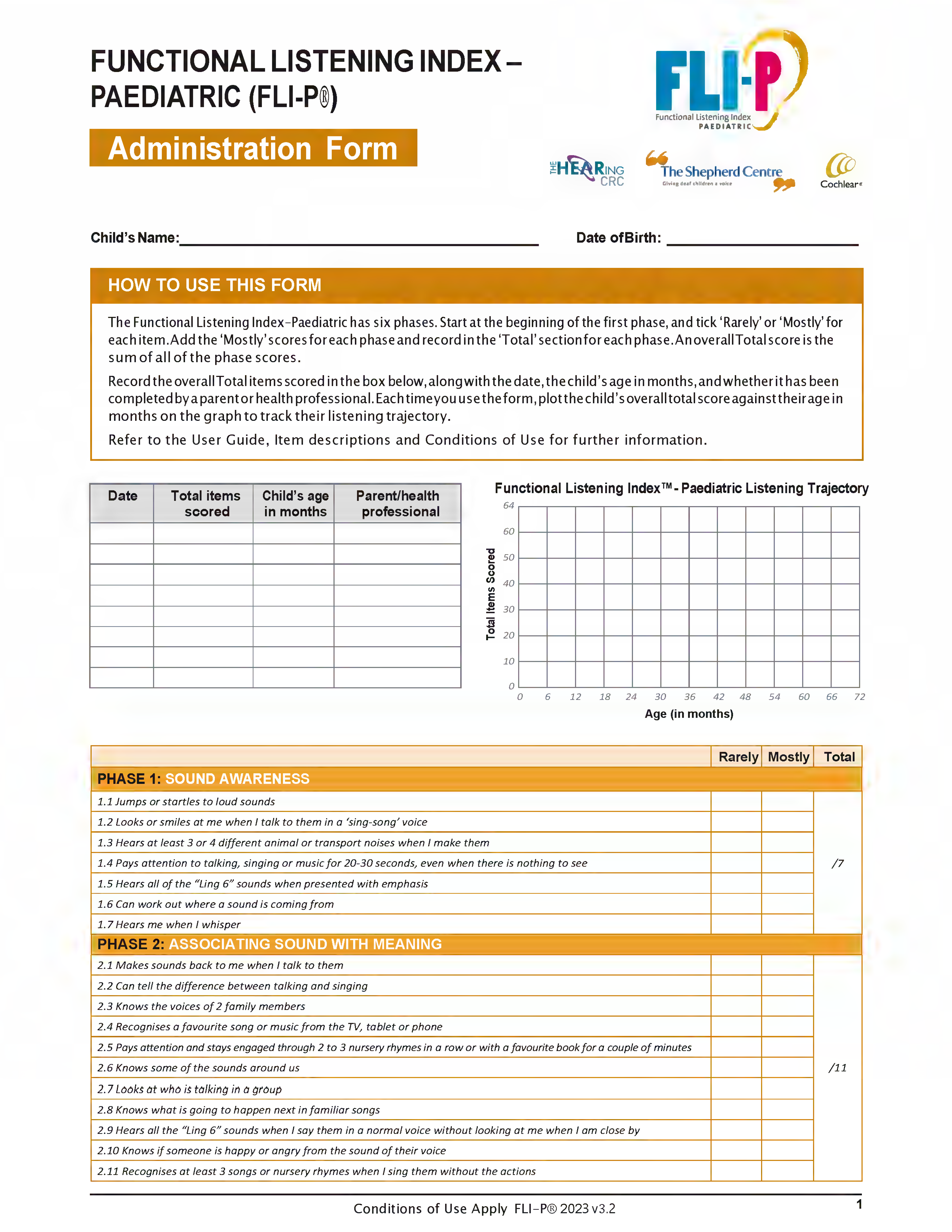
- “Mostly” means the child does it regularly, in different places, with different people;
- “Rarely” means that the child has only done it occasionally, a few times, or not at all.
- Listening, e.g., Q1: Jumps or startles to loud noises;
- Associating sound with meaning, e.g., Q8: makes sounds back to me when I talk to them;
- Comprehending simple spoken language, e.g., Q19: repeats three familiar sounds after me;
- Comprehending simple language in different listening conditions, e.g., Q31: follows short directions that are unpredictable or silly;
- Listening through discourse and narrative, e.g., Q42: recognises a familiar person on the phone;
- Advanced listening skills, e.g., Q56: can have a simple conversation with a familiar person on the phone.
2.2. Test Material: The Functional Listening Index—Paediatric
2.2.1. Subjects
- Children aged between birth and 6 years of age (0–72 months);
- Pass on Newborn Hearing Screen Status conducted during the New South Wales Statewide Infant Screening—Hearing (SWISH) Program;
- No current parental or professional concerns regarding hearing status.
- Pre-existing diagnosis of additional needs;
- Unrealistic expectations on the part of the subject or the subject’s parents or carers regarding the possible benefits, risks, and limitations of the study;
- Unwillingness or inability of the subject to comply with all investigational requirements.
2.2.2. Sample Size
- Proportion of parents who indicated an interest in participation;
- Proportion of children who meet eligibility criteria for investigation;
- Proportion of parents who successfully entered data into the Qualtrics website.
2.2.3. Bias Minimisation
2.2.4. Data Quality Assurance
2.3. Statistical Methods and Analyses
2.4. Ethical Approval
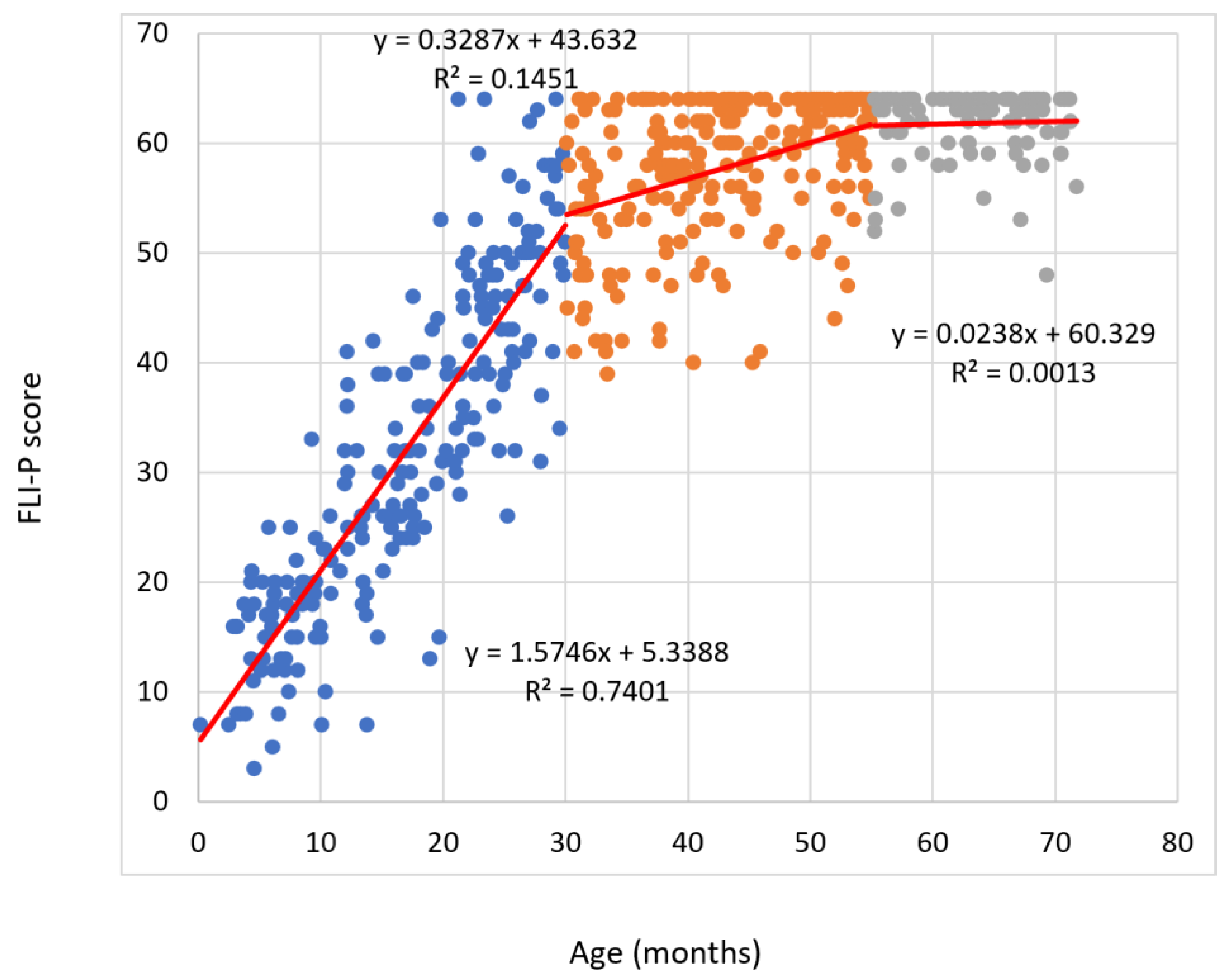
3. Results
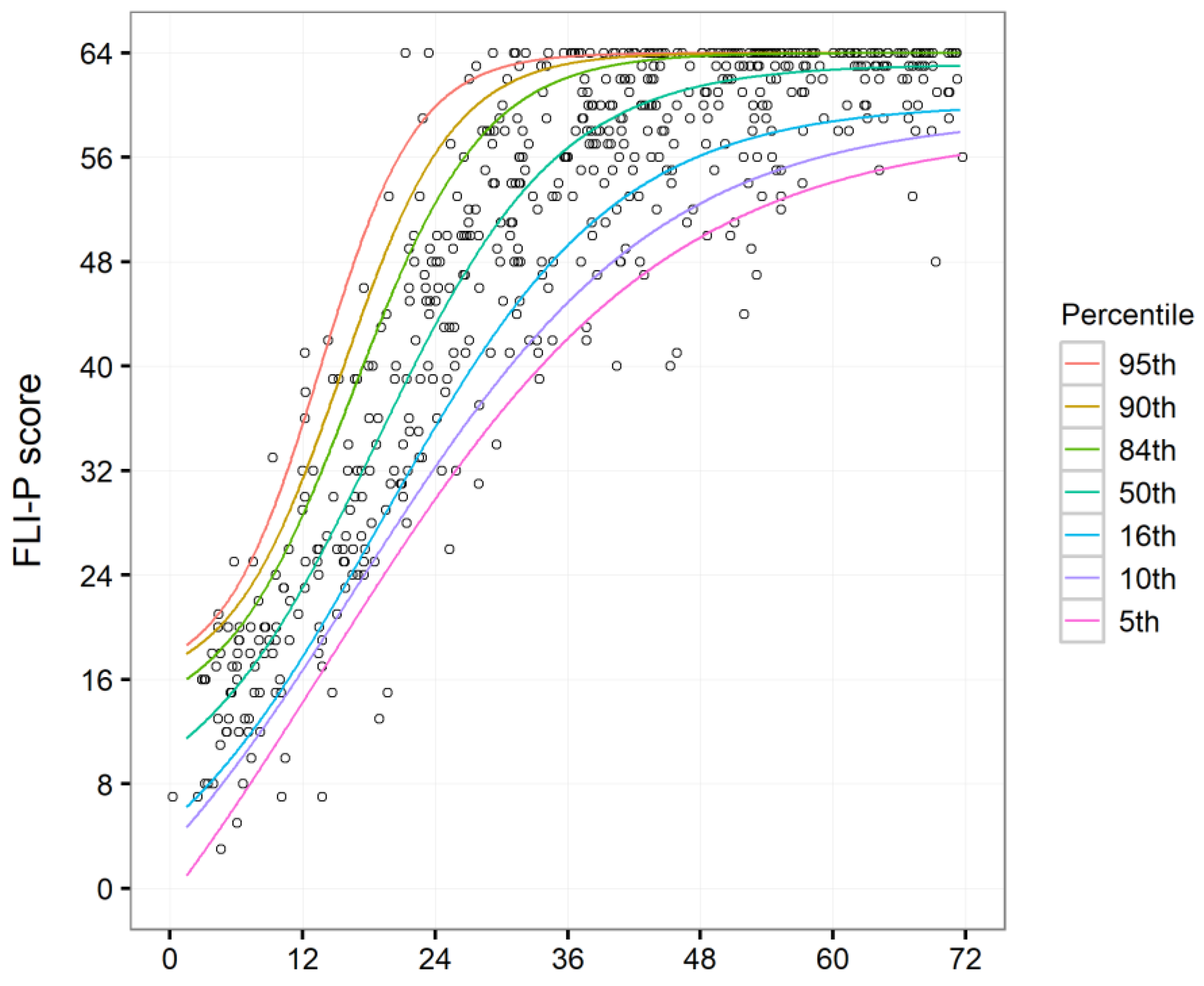
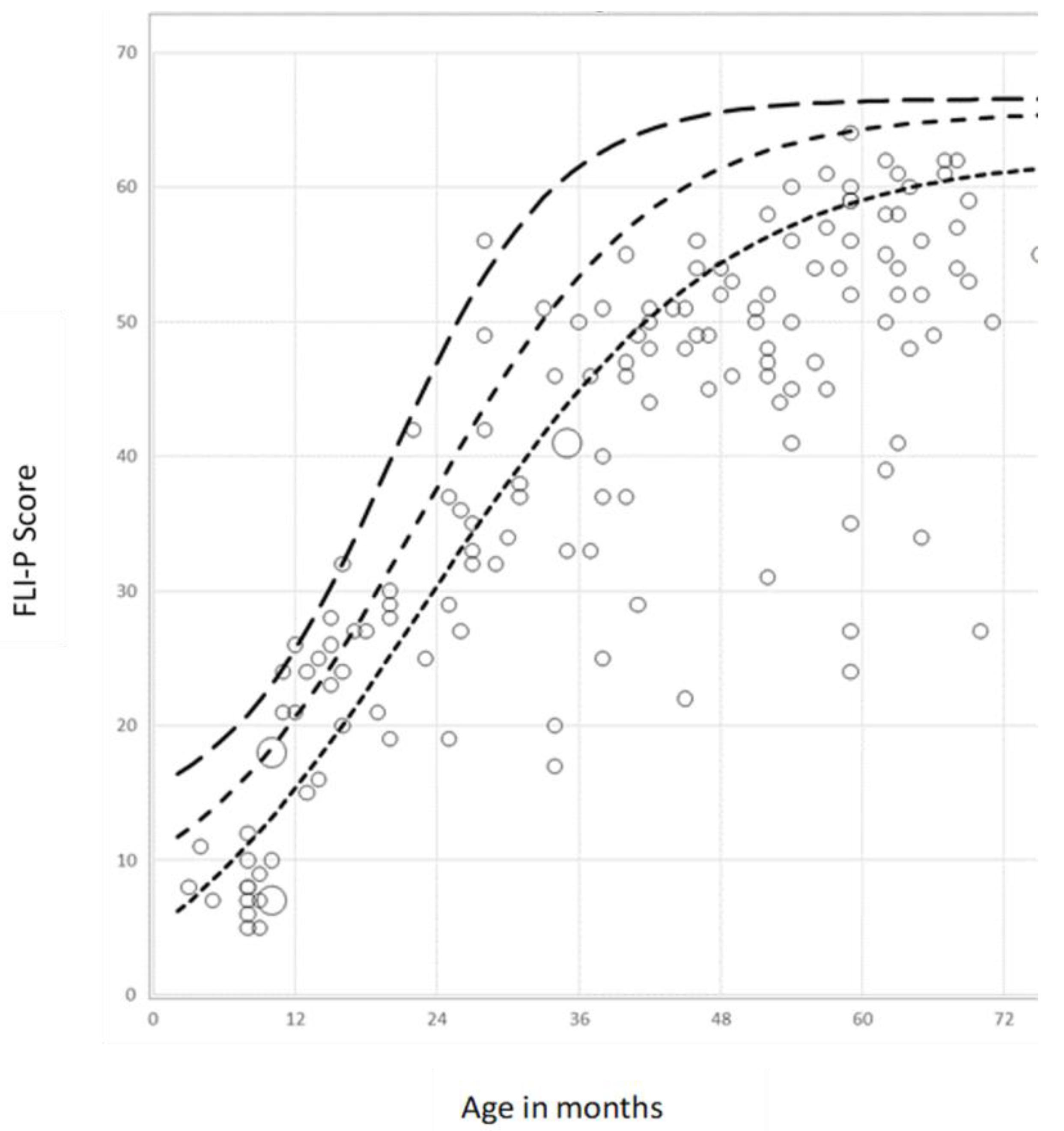
Fitted Functions and Percentile Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Kral, A.; Sharma, A. Crossmodal plasticity in hearing loss. In Trends in Neurosciences; Elsevier: Amsterdam, The Netherlands, 2023; Volume 46, pp. 377–393. [Google Scholar]
- Walker, S.P.P.; Wachs, T.D.; Grantham-McGregor, S.; Black, M.M.; Nelson, C.A.; Huffman, S.L.; Baker-Henningham, H.; Chang, S.M.; Hamadani, J.D.; Lozoff, B.; et al. Inequality in early childhood: Risk and protective factors for early child development. Lancet 2011, 378, 1325–1338. [Google Scholar] [CrossRef]
- Fulcher, A.; Purcell, A.A.; Baker, E.; Munro, N. Listen up: Children with early identified hearing loss achieve age-appropriate speech/language outcomes by 3 years-of-age. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 1785–1794. [Google Scholar] [CrossRef]
- Goldfeld, S.; Yousafzai, A. Monitoring tools for child development: An opportunity for action. Lancet Glob. Health 2018, 6, e232–e233. [Google Scholar] [CrossRef] [PubMed]
- Sheldrick, R.C.; Schlichting, L.E.; Berger, B.; Clyne, A.; Ni, P.; Perrin, E.C.; Vivier, P.M. Establishing New Norms for Developmental Milestones. Pediatrics 2019, 144, e20190374. [Google Scholar] [CrossRef]
- Stephenson, K.G.; Vargo, K.C.; Cacciato, N.M.; Albright, C.M.; Kryszak, E.M. Developmental Assessment in Children at Higher Likelihood for Developmental Delays—Comparison of Parent Report and Direct Assessment. J. Autism Dev. Disord. 2024. [Google Scholar] [CrossRef] [PubMed]
- Storkel, H.L. Using Developmental Norms for Speech Sounds as a Means of Determining Treatment Eligibility in Schools. Perspect. ASHA Spec. Interest Groups 2019, 4, 67–75. [Google Scholar] [CrossRef]
- Martins, J.H.; Alves, M.; Andrade, S.; Falé, I.; Teixeira, A. Auditory Processing Disorder Test Battery in European Portuguese—Development and Normative Data for Pediatric Population. Audiol. Res. 2021, 11, 474–490. [Google Scholar] [CrossRef]
- Yoshinaga-Itano, C.; Sedey, A.L.; Coulter, D.K.; Mehl, A.L. Language of Early- and Later-identified Children with Hearing Loss. Pediatrics 1998, 102, 1161–1171. [Google Scholar] [CrossRef]
- Ching, T.Y.C.; Crowe, K.; Martin, V.; Day, J.; Mahler, N.; Youn, S.; Street, L.; Cook, C.; Orsini, J. Language development and everyday functioning of children with hearing loss assessed at 3 years of age. Int. J. Speech Lang. Pathol. 2010, 12, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Ching, T.Y.C.; Leigh, G. Considering the impact of universal newborn hearing screening and early intervention on language outcomes for children with congenital hearing loss. Hear. Balance Commun. 2020, 18, 215–224. [Google Scholar] [CrossRef]
- Antia, S.D.; Jones, P.B.; Reed, S.; Kreimeyer, K.H. Academic Status and Progress of Deaf and Hard-of-Hearing Students in General Education Classrooms. J. Deaf. Stud. Deaf. Educ. 2009, 14, 293–311. [Google Scholar] [CrossRef] [PubMed]
- Breland, L.; Lowenstein, J.H.; Nittrouer, S. Disparate Oral and Written Language Abilities in Adolescents with Cochlear Implants: Evidence From Narrative Samples. Lang. Speech Hear. Serv. Sch. 2022, 53, 193–212. [Google Scholar] [CrossRef]
- Hogan, A.; O’Loughlin, K.; Davis, A.; Kendig, H. Hearing loss and paid employment: Australian population survey findings. Int. J. Audiol. 2009, 48, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Podury, A.; Jiam, N.T.; Kim, M.; Donnenfield, J.I.; Dhand, A. Hearing and sociality: The implications of hearing loss on social life. Front. Neurosci. 2023, 17, 1245434. [Google Scholar] [CrossRef] [PubMed]
- Erlich, S. Spotlight on Deaf and Hard-of-Hearing Youth in Canada and Beyond. Child Youth Serv. 2012, 33, 5–11. [Google Scholar] [CrossRef]
- Patel, S.R.; Ba, E.B.; Tey, C.S.; Govil, N.; Alfonso, K.P. Social Isolation and Loneliness in the Hearing-Impaired Pediatric Population: A Scoping Review. Laryngoscope 2021, 131, 1869–1875. [Google Scholar] [CrossRef] [PubMed]
- Cejas, I.; Barker, D.H.; Petruzzello, E.; Sarangoulis, C.M.; Quittner, A.L. Cochlear Implantation and Educational and Quality-of-Life Outcomes in Adolescence. JAMA Otolaryngol.—Head Neck Surg. 2023, 149, 708–715. [Google Scholar] [CrossRef]
- Dettman, S.J.; Charles, D.R.; Dawn, C.; Wendy, A.; Yetta, A.; Aleisha, D.; Dimity, D.; Jaime, L.; Gabriella, C.; Robert, C.; et al. Long-term Communication Outcomes for Children Receiving Cochlear Implants Younger Than 12 Months: A Multicenter Study. Otol. Neurotol. 2016, 37, e82–e95. [Google Scholar] [CrossRef]
- Cowan, R.S.C.; Edwards, B.; Ching, T.Y.C. Longitudinal outcomes of children with hearing impairment (LOCHI): 5 year data. Int. J. Audiol. 2018, 57 (Suppl. S2), S1–S2. [Google Scholar] [CrossRef] [PubMed]
- Dawson, P.W.; Nott, P.E.; Clark, G.M.; Cowan, R.S.C. A Modification of Play Audiometry to Assess Speech Discrimination Ability in Severe-Profoundly Deaf 2- to 4-Year-Old Children. Ear Hear. 1998, 19, 371–384. [Google Scholar] [CrossRef]
- Werfel, K.L.; Douglas, M. Are We Slipping Them Through the Cracks? The Insufficiency of Norm-Referenced Assessments for Identifying Language Weaknesses in Children with Hearing Loss. Perspect. ASHA Spec. Interest Groups 2017, 2, 43–53. [Google Scholar] [CrossRef]
- Mervis, C.B.; Bertrand, J. Early lexical acquisition and the vocabulary spurt: A response to Goldfield & Reznick. J. Child Lang. 1995, 22, 461–468. [Google Scholar] [PubMed]
- Yoshinaga-Itano, C. Early intervention after universal neonatal hearing screening: Impact on outcomes. Ment. Retard. Dev. Disabil. Res. Rev. 2003, 9, 252–266. [Google Scholar] [CrossRef] [PubMed]
- Moeller, M.P. Current State of Knowledge: Psychosocial Development in Children with Hearing Impairment. Ear Hear. 2007, 28, 729–739. [Google Scholar] [CrossRef]
- Mayne, A.M.; Christine, Y.-I.; Allison, L.S.; Angela, C. Expressive Vocabulary Development of Infants and Toddlers Who Are Deaf or Hard of Hearing. Volta Rev. 1999, 100, 1–28. [Google Scholar]
- Nott, P.; Cowan, R.; Brown, P.M.; Wigglesworth, G. Assessment of language skills in young children with profound hearing loss under two years of age: Special Issue on Language Assessment in Deaf Children. J. Deaf. Stud. Deaf. Educ. 2003, 8, 401–421. [Google Scholar] [CrossRef] [PubMed]
- Luna-Bazaldua, D.; Pushparatnam, A.; Urzua, T.A.; Cloutier, M.-H. Getting it right by measuring it right: New global tools for measuring child development in the preschool years. Education for Global Development. Available online: https://blogs.worldbank.org/en/education/getting-it-right-measuring-it-right-new-global-tools-measuring-child-development (accessed on 25 January 2024).
- Davenport, C.; Houston, D.; Bowdrie, K.; Frush, R. Holt The Role of Early Intervention in Parental Self-Efficacy for Parents of Deaf and Hard-of-Hearing Children. J. Early Hear. Detect. Interv. 2021, 6, 38–47. [Google Scholar]
- Ravanyar, L.; Mostafavi, F.; Hashemian, S.S.; Hosseini, R.; Hazavehei, S.M.; Oryadi-Zanjani, M.M. Program to reduce empowerment barriers hindering mothers to contribute to speech skills of hearing-impaired children with cochlear implant. J. Multidiscip. Care 2022, 11, 164–171. [Google Scholar] [CrossRef]
- Shekari, E.; Nakhshab, M.; Valinejad, V.; Modarres, Z.; Hosseinpour, A. A Systematic Review of the Effectiveness of Early Intervention and the Role of Parents in Language Development of Hearing Loss Children. Iran. Rehabil. J. 2017, 15, 5–14. [Google Scholar] [CrossRef]
- Ravanyar, L.; Mostafavi, F.; Hashemian, S.S.; Oryadi-Zanjani, M.M. Effectiveness of the interventional program for empowering mothers with hearing-impaired children for the improvement of expressive language skills. Health Sci. Monit. 2023, 2, 99–109. [Google Scholar] [CrossRef]
- Oryadi-Zanjani, M.M.; Vahab, M.; Purdy, S.C. The Persian Version of the Auditory Behavior in Everyday Life Questionnaire. Int. J. Sch. Health 2018, 5, 1–5. [Google Scholar] [CrossRef]
- Clark, M.D.; Greene-Woods, A.; Alofi, A.; Sides, M.; Buchanan, B.; Hauschildt, S.; Alford, A.; Courson, F.; Venable, T. The Spoken Language Checklist: A User-Friendly Normed Language Acquisition Checklist. J. Deaf. Stud. Deaf. Educ. 2021, 26, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Cuda, D.; Guerzoni, L.; Mariani, V.; Murri, A.; Biasucci, G.; Fabrizi, E. Production of Infant Scale Evaluation (PRISE) in Italian normal hearing children: A validation study. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 1969–1974. [Google Scholar] [CrossRef]
- Oryadi-Zanjani, M.M. Production of Infant Scale Evaluation (PRISE) in Persian normal hearing children: A validation study. Int. J. Pediatr. Otorhinolaryngol. 2018, 113, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.-q.; Chen, X.-Q.; Wang, H. A normative study of auditory development in Mandarin-speaking infants. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi Chin. J. Otorhinolaryngol. Head Neck Surg. 2013, 48, 908–912. [Google Scholar]
- O’Connor, P.J. Normative data: Their definition, interpretation, and importance for primary care physicians. Fam. Med. 1990, 22, 307–311. [Google Scholar]
- Raudeberg, R.; Iverson, G.L.; Hammar, Å. The importance of clinical normative data for conceptualizing neuropsychological deficits in people with schizophrenia spectrum disorders. Appl. Neuropsychol. Adult 2021, 28, 752–760. [Google Scholar] [CrossRef]
- Cantle Moore, R.; Colyvas, K. The Infant Monitor of vocal Production (IMP) normative study: Important foundations. Deaf. Educ. Int. 2018, 20, 228–244. [Google Scholar] [CrossRef]
- Ching, T.Y.C.; Hill, M. The Parents’ Evaluation of Aural/Oral Performance of Children (PEACH) Scale: Normative Data. J. Am. Acad. Audiol. 2007, 18, 220–235. [Google Scholar] [CrossRef]
- Zhong, Y.; Xu, T.; Dong, R.; Lyu, J.; Liu, B.; Chen, X. The analysis of reliability and validity of the IT-MAIS, MAIS and MUSS. Int. J. Pediatr. Otorhinolaryngol. 2017, 96, 106–110. [Google Scholar] [CrossRef]
- Ching, T.Y.; Harvey, D.; Vivienne, M.; Sanna, H.; Julia, D.; Mark, S.; Mark, S.; Laura, S.; Jessica, T.; Patricia, V.B.; et al. Outcomes of early- and late-identified children at 3 years of age: Findings from a prospective population-based study. Ear Hear. 2013, 34, 535–552. [Google Scholar] [CrossRef] [PubMed]
- McCreery, R.W.; Walker, E.A.; Spratford, M.; Bentler, R.; Holte, L.; Roush, P.; Oleson, J.; Van Buren, J.; Moeller, M.P. Longitudinal Predictors of Aided Speech Audibility in Infants and Children. Ear Hear. 2015, 36 (Suppl. S1), 24S–37S. [Google Scholar] [CrossRef]
- Sininger, Y.S.; Grimes, A.; Christensen, E. Auditory Development in Early Amplified Children: Factors Influencing Auditory-Based Communication Outcomes in Children with Hearing Loss. Ear Hear. 2010, 31, 166–185. [Google Scholar] [CrossRef] [PubMed]
- Wake, M.; Gerner, B.; Gallagher, S. Does Parents’ Evaluation of Developmental Status at School Entry Predict Language, Achievement, and Quality of Life 2 Years Later? Ambul. Pediatr. 2005, 5, 143–149. [Google Scholar] [CrossRef]
- Davis, A.; Harrison, E.; Cowan, R. The Feasibility of the Functional Listening Index—Paediatric (FLI-P®) for Young Children with Hearing Loss. J. Clin. Med. 2022, 11, 2764. [Google Scholar] [CrossRef] [PubMed]
- Culbertson, S.R.; Dillon, M.T.; Richter, M.E.; Brown, K.D.; Anderson, M.R.; Hancock, S.L.; Park, L.R. Younger Age at Cochlear Implant Activation Results in Improved Auditory Skill Development for Children with Congenital Deafness. J. Speech Lang. Hear. Res. 2022, 65, 3539–3547. [Google Scholar] [CrossRef] [PubMed]
- Ling, D. Speech and the hearing-impaired child: Theory and practice. In Speech and the Hearing-Impaired Child, 2nd ed.; Alexander Graham Bell Association for the Deaf and Hard of Hearing: Washington, DC, USA, 2002. [Google Scholar]
- Pollack, D. Educational Audiology for the Limited Hearing Infant; Charles C Thomas Pub Ltd.: Springfield, IL, USA, 1970. [Google Scholar]
- Estabrooks, W. Auditory-Verbal Therapy and Practice; Alexander Graham Bell Association for the Deaf and Hard of Hearing: Washington, DC, USA, 2006. [Google Scholar]
- Couchenour, D.; Chrisman, J.K. The SAGE Encyclopedia of Contemporary Early Childhood Education, 1st ed.; SAGE Publications Inc.: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Brown, C.S. Language and Literacy Development in the Early Years: Foundational Skills that Support Emergent Readers. Lang. Lit. Spectr. 2014, 24, 35–49. [Google Scholar]
- North, B. The development of a common framework scale of descriptors of language proficiency based on a theory of measurement. System 1995, 23, 445–465. [Google Scholar] [CrossRef]
- Morin, A. Developmental Milestons from Birth to age 1. 2022. Available online: https://www.understood.org/en/articles/developmental-milestones-from-birth-to-age-1 (accessed on 5 May 2024).
- Neilson, R. Sutherland Phonological Awareness Test, Revised (SPAT-R). 2003. Available online: https://www.roslynneilson.com.au/ (accessed on 5 May 2024).
- Barbaro, J.; Dissanayake, C. Early markers of autism spectrum disorders in infants and toddlers prospectively identified in the Social Attention and Communication Study. Autism Int. J. Res. Pract. 2013, 17, 64–86. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing (Version 3.5.2), 2018. Available online: https://www.r-project.org (accessed on 5 May 2024).
- Koenker, R. Quantreg: Quantile Regression (Version 5.38), 2018. Available online: https://cran.r-project.org/package=quantreg (accessed on 5 May 2024).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis (Version 3.1.0), 2018. Available online: https://cran.r-project.org/package=ggplot2 (accessed on 5 May 2024).
- Zimmerman-Phillips, S.; Osberger, M.; Robbins, A. Infant-Toddler: Meaningful Auditory Integration Scale (It-Mais); Advanced Bionics Corporation: Kansas City, MO, USA, 1997. [Google Scholar]
- Coninx, F.; Weichbold, V.; Tsiakpini, L.; Autrique, E.; Bescond, G.; Tamas, L.; Compernol, A.; Georgescu, M.; Koroleva, I.; Le Maner-Idrissi, G.; et al. Validation of the LittlEARS® Auditory Questionnaire in children with normal hearing. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 1761–1768. [Google Scholar] [CrossRef]
- Rawes, C.; Ngaage, L.M.; Mackenzie, R.; Martin, J.; Cordingley, A.; Raine, C. A review of the outcomes of children with designated additional needs receiving cochlear implantation for severe to profound hearing loss. Cochlear Implant. Int. 2021, 22, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.M.; Borders, C.M.; Ely, M.S. Prevalence of Educationally Significant Disabilities Among Deaf and Hard of Hearing Students. Am. Ann. Deaf 2023, 167, 583–596. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 0–6 | 7–12 | 13–18 | 19–24 | 25–30 | 31–36 | 37–42 | 43–48 | 49–54 | 55–60 | 61–66 | 67–72 | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Target | 36 | 36 | 36 | 36 | 36 | 36 | 36 | 36 | 36 | 36 | 36 | 36 | 432 |
| Actural | 36 | 40 | 42 | 49 | 42 | 47 | 63 | 46 | 53 | 36 | 36 | 36 | 536 |
| Percentile | a1 | a2 | a3 | a4 |
|---|---|---|---|---|
| 5th | −25.3196 | 58.1656 | 0.0641 | 13.6060 |
| 10th | −13.2335 | 59.2565 | 0.0728 | 16.8049 |
| 16th | −4.2314 | 60.1019 | 0.0938 | 18.9745 |
| 50th | 4.9005 | 63.1047 | 0.1204 | 18.5796 |
| 84th | 12.2876 | 64.0000 | 0.1691 | 16.5906 |
| 90th | 15.1011 | 64.0000 | 0.1978 | 15.5172 |
| 95th | 15.7385 | 64.0000 | 0.2277 | 13.5759 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cowan, R.S.C.; Davis, A.; Watkins, P.; Neal, K.; Brookman, R.; Seeto, M.; Oliver, J. Tracking Listening Skill Development in Infants and Children with Hearing Loss: A Normative Dataset for the Functional Listening Index—Paediatric (FLI-P®). Children 2024, 11, 1052. https://doi.org/10.3390/children11091052
Cowan RSC, Davis A, Watkins P, Neal K, Brookman R, Seeto M, Oliver J. Tracking Listening Skill Development in Infants and Children with Hearing Loss: A Normative Dataset for the Functional Listening Index—Paediatric (FLI-P®). Children. 2024; 11(9):1052. https://doi.org/10.3390/children11091052
Chicago/Turabian StyleCowan, Robert S. C., Aleisha Davis, Pia Watkins, Katie Neal, Ruth Brookman, Mark Seeto, and Janette Oliver. 2024. "Tracking Listening Skill Development in Infants and Children with Hearing Loss: A Normative Dataset for the Functional Listening Index—Paediatric (FLI-P®)" Children 11, no. 9: 1052. https://doi.org/10.3390/children11091052