1. Introduction
Children with cancer and their families experience various psychosocial challenges during and after treatment, including physical and cognitive changes due to medical treatment, alterations in social and familial roles, and the potential threat of death [
1]. Most children and families cope and adjust well to the diagnosis and treatment of cancer [
2]. However, there is a subset of children with cancer at increased risk for anxiety and depression, as well as educational and relationship difficulties [
1,
3]. Caregivers and siblings of pediatric patients are at risk for heightened distress and post-traumatic stress [
4,
5]. Psychosocial care and interventions can play an important role in supporting the well-being of the entire family, beginning at diagnosis [
6].
The Standards of Psychosocial Care for Children with Cancer and their Families [
7] recommend that “youth with cancer and their family members should have access to psychosocial support and interventions throughout the cancer trajectory and access to psychiatry as needed” (p. S585) [
3]. Currently, there are only a few evidence-based psychotherapeutic interventions designed to decrease psychological distress and increase emotional well-being specifically for the pediatric oncology population [
8,
9]. These include the Surviving Cancer Competently Intervention Program (SCCIP) and Bright IDEAS Problem Solving Skills Training, two programs targeting distress in parents of children with cancer, demonstrating high degrees of effectiveness, and designated as evidence-based cancer control programs (EBCCP) by the National Cancer Institute (NCI). Alternatively, a range of additional interventions exist, not specifically adapted for or tested with oncology populations. These include psychoeducation, supportive individual therapy, cognitive behavioral therapy, problem-solving therapy, social support groups, social skills training, health promotion, bibliotherapy, art therapy, and mindfulness-based therapies [
10,
11]. Yet, we currently do not understand what clinical interventions are being offered by psychosocial providers or nuanced differences among provider specialties and professional stage, and it is unlikely that all pediatric cancer centers have the resources to offer clinical training and the full array of evidence-based interventions [
7]. There is some evidence that professional stage may impact care. Ramsmussen and colleagues found that older psychosocial oncologists reported significantly less burnout than their younger counterparts [
12]
.This study was designed to learn how pediatric cancer treatment programs currently address the Psychosocial Standard to provide psychotherapeutic interventions. We aimed to describe the psychotherapeutic interventions that psychosocial providers are using “in the real world” throughout the cancer trajectory (i.e., initial diagnosis, on treatment, survivorship, end of life), explore potential group differences by provider type (i.e., psychologist, social worker, child life specialist, etc.) and professional stage (i.e., early-, mid-, late-career), and to identify the education and resource needs of pediatric psychosocial providers.
4. Discussion
This paper describes the psychotherapeutic interventions provided to pediatric cancer patients and their families throughout the cancer trajectory. Most respondents were psychologists or social workers, the majority of whom were early- or mid-career providers. Findings underscore the importance of offering services to patients and caregivers and the dearth of psychosocial care being provided to siblings [
5,
15]. Lack of group differences between type of provider or professional stage and type of psychotherapeutic interventions being utilized may speak to the type and availability of training across settings and disciplines. It is important that psychosocial providers have the credentialing and training necessary to offer specialized interventions. Results are consistent with prior research demonstrating limited access to and availability of psychiatrists on psychosocial teams [
16].
We found that a broad range of psychotherapeutic interventions are being offered to children undergoing cancer therapy and their families. Psychoeducation, defined broadly as the incorporation of illness-specific information and education synergized with strategies for psychotherapeutic management [
17,
18], was a foundational intervention, and the most frequently endorsed intervention provided to children, caregivers, and siblings. As a distinct Standard of psychosocial care, experts recommend that youth with cancer and their family members receive psychoeducation and anticipatory guidance related to disease, treatment, acute and long-term effects, hospitalization, procedures, and psychosocial adaptation [
19]. Psychoeducation is most effective when content is catered specifically to the patient’s needs and provided throughout the trajectory of care. The nature of the psychoeducational information shared was not covered by the current study. However, our findings indicate it is consistently offered throughout the cancer trajectory. Not only can psychoeducation help meet unmet information needs, but it has been shown to improve disease-related knowledge and increase the health locus of control [
6,
13].
Psychosocial providers offered referrals to support groups, cognitive behavioral therapy (CBT), mindfulness, and supportive individual psychotherapy, demonstrating that “one size does not fit all”. Tailored interventions are based on many factors, requiring clinical skills to determine the appropriate interventions, which can vary by medical treatments, psychosocial factors, and availability/access to providers throughout treatment. Further, providers are utilizing multiple interventions, as they are not mutually exclusive. Aspects of mindfulness-based interventions may be offered or utilized during individual supportive psychotherapy or support groups, or individual supportive therapy may utilize mindfulness or psychoeducation in order to establish a trusting relationship between the patient and the care provider [
20].
Evidence for these diverse approaches within pediatric oncology exists. Research suggests support groups are beneficial to pediatric oncology patients, caregivers, and siblings as they provide individuals with a sense of community [
20], and CBT, widely practiced in the field of pediatric oncology, has been found to be effective in lowering symptoms of depression and anxiety and improving levels of self-esteem among patients [
21]. Mindfulness, a feasible, effective intervention for adolescents with cancer that is easily adaptable to online formats, has been growing in popularity [
22,
23]. Psychosocial providers are commonly recommending apps that focus on aspects of mindfulness (e.g., breathing or relaxation techniques, meditation, and guided imagery); however, limited research has explored the effectiveness of readily available apps. This remains an important area for future investigation.
Interestingly, pediatric cancer-specific interventions such as Surviving Cancer Competently Intervention Program [
8,
24] and Bright IDEAS Problem-Solving Skills Training [
9,
25,
26] were not commonly offered by psychosocial providers, despite robust evidence supporting their efficacy. It is possible that cancer centers may not have access to the necessary resources (e.g., funding additional staff, or provider trainings) to offer these interventions or prioritize their use. Future implementation and dissemination efforts should be made to translate research to practice, increasing access to these interventions for patients and families [
27]. This may include addressing implementation barriers by advocating for increased funding for more psychosocial staff, resources, trainings, and overall prioritization of psychosocial services (e.g., messaging from medical providers/institutions, workflow consistency, care coordination among multidisciplinary teams).
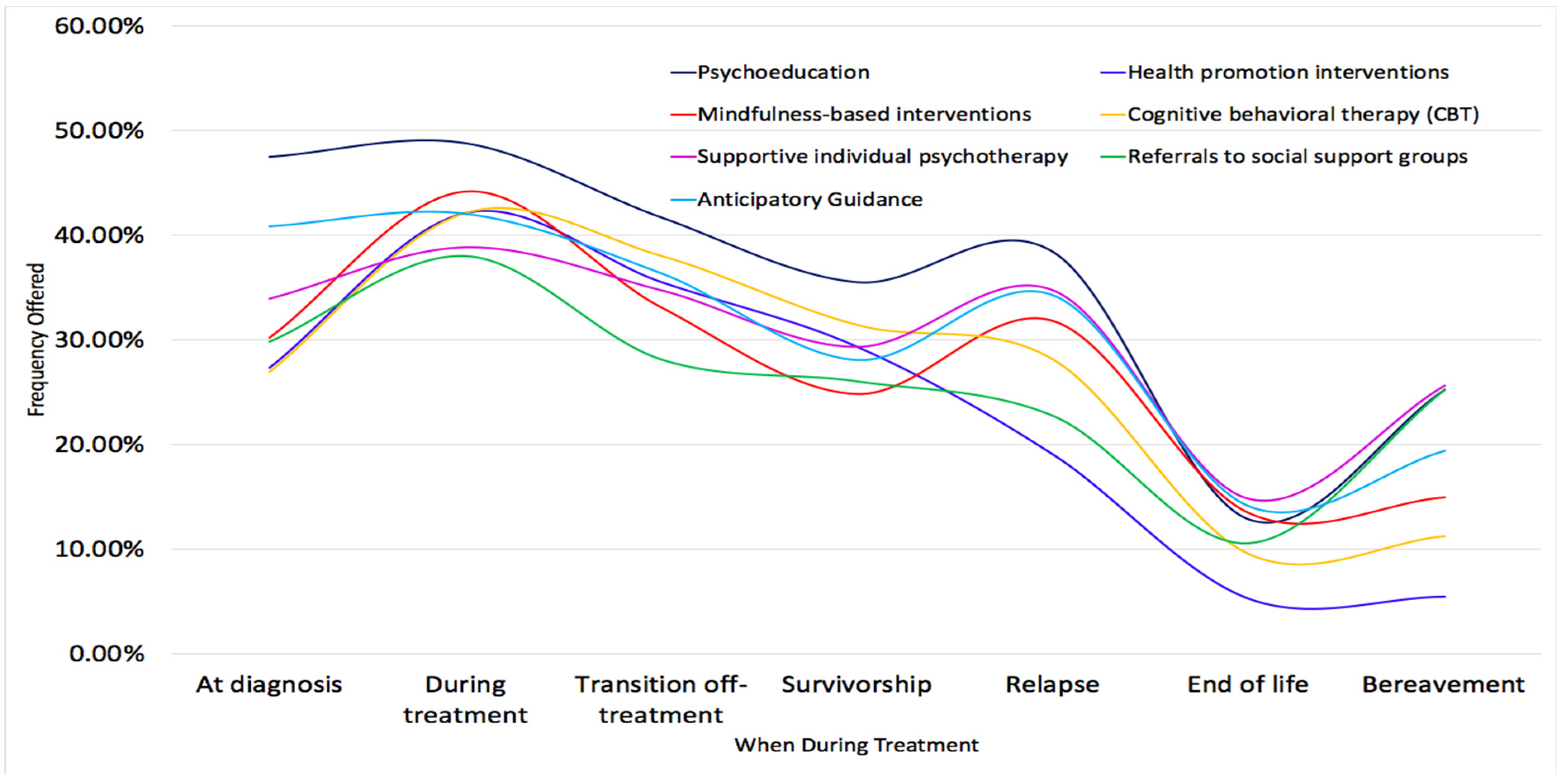
The data suggest that the most commonly offered interventions are provided while the patient is in active treatment. The Psychosocial Standards of care highlight the importance of support at diagnosis and during the early months of treatment, with less frequent delivery of services as the child progresses through treatment [
28]. However, patients and families experience increased distress at critical points such recurrence or transition off treatment and, therefore, need additional support at those times as well. It is likely that patients and families have more direct access to psychosocial providers during treatment in both outpatient and inpatient settings. Once children finish cancer treatment, their access to ongoing support from clinic or hospital staff declines as they have less scheduled contacts with providers; additionally, patients may wish to avoid or not return to the hospital whenever possible. As there are abundant data to support the need for psychotherapeutic interventions after cancer therapy ends [
29,
30], future research should explore the type and availability of interventions later in the cancer trajectory, such as the transition off-treatment and into early and long-term survivorship, and resources needed (e.g., personnel) to provide them.
Psychosocial providers reported a primary need for additional staff in order to provide quality psychosocial care. Funding for psychosocial positions and inadequate staffing are known and prominent barriers to providing adequate psychosocial care [
12,
31]. Even in large pediatric oncology programs with greater access to psychosocial care, psychosocial teams are still often understaffed for patient volumes [
12]. A robust interprofessional team may be most effective in implementing the Standards of Care across treatment settings and the cancer trajectory [
32]. Utilizing screening tools to effectively match level of family risk to needed intervention, as demonstrated by the Pediatric Psychosocial Preventative Health Model, will allow for judicious use of psychosocial staffing resources [
33,
34].
In addition to staff, psychosocial providers indicated a desire for improved communication, opportunities to collaborate more effectively with others inside and across institutions, and a need for additional training and clinical supervision confirming previous research on the training needs of pediatric psycho-oncologists [
35]. Participating in patient care rounds/medical team meetings and documenting in the electronic health record are recommended to facilitate communication, help medical staff better understand the role of psychosocial providers and improve integration of psychosocial providers into the pediatric oncology care settings [
36].
Implications for Psychosocial Providers: This exploratory study is unique in that it explored how psychosocial providers approach treatment with children, caregivers, and siblings across the developmental and treatment trajectory. It is difficult to collect data about real-time clinical care due to nuance and complexity. This is a first step in identifying what interventions providers utilize most often. Some of the commonly reported interventions lack an evidence base for their use with the pediatric oncology population. An example of this is the often-endorsed use of apps. Conducting research on interventions that use technology (i.e., apps, telehealth, eHealth, etc.) has the potential to increase accessibility to patients and families across the treatment trajectory. Additionally, advocating for more psychosocial staff, resources, and training will allow sites to better implement and meet the Psychosocial Standards of Care. This includes making psychosocial oncology training more accessible across disciplines.
It is important to note several limitations of the current study. The study population was confined to psychosocial providers who belong to one of the accessed professional organizations. Because there was no definite sample size, response rate could not be calculated. The study design was cross-sectional, so changes in services over time were not captured. All answers were based upon self-report. It was not possible to validate the reported interventions offered, or the specific dosing, frequency, and length of sessions. Delivery of reported interventions may vary based on patient geography and logistics around a patient’s medical care rather than symptom indications (e.g., travel distance, cost of travel, or insurance barriers). The survey did include an international population but was only offered in English, thereby excluding non-English speaking psychosocial providers. Because it was administered prior to the COVID-19 global pandemic, the survey did not include telehealth/virtual interventions. Future research should focus on strategies to increase accessibility, evaluate psychosocial intervention session dosing/frequency, institutional and programmatic support for psychotherapeutic services, and training for population-specific evidenced-based interventions and for translating science to practice.


 ,
, 

{kind=link}