
Cutaneous Syncytial Myoepithelioma with Positive CD34 Immunohistochemical Staining: An Unusual Tumor and a Challenging Diagnosis

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
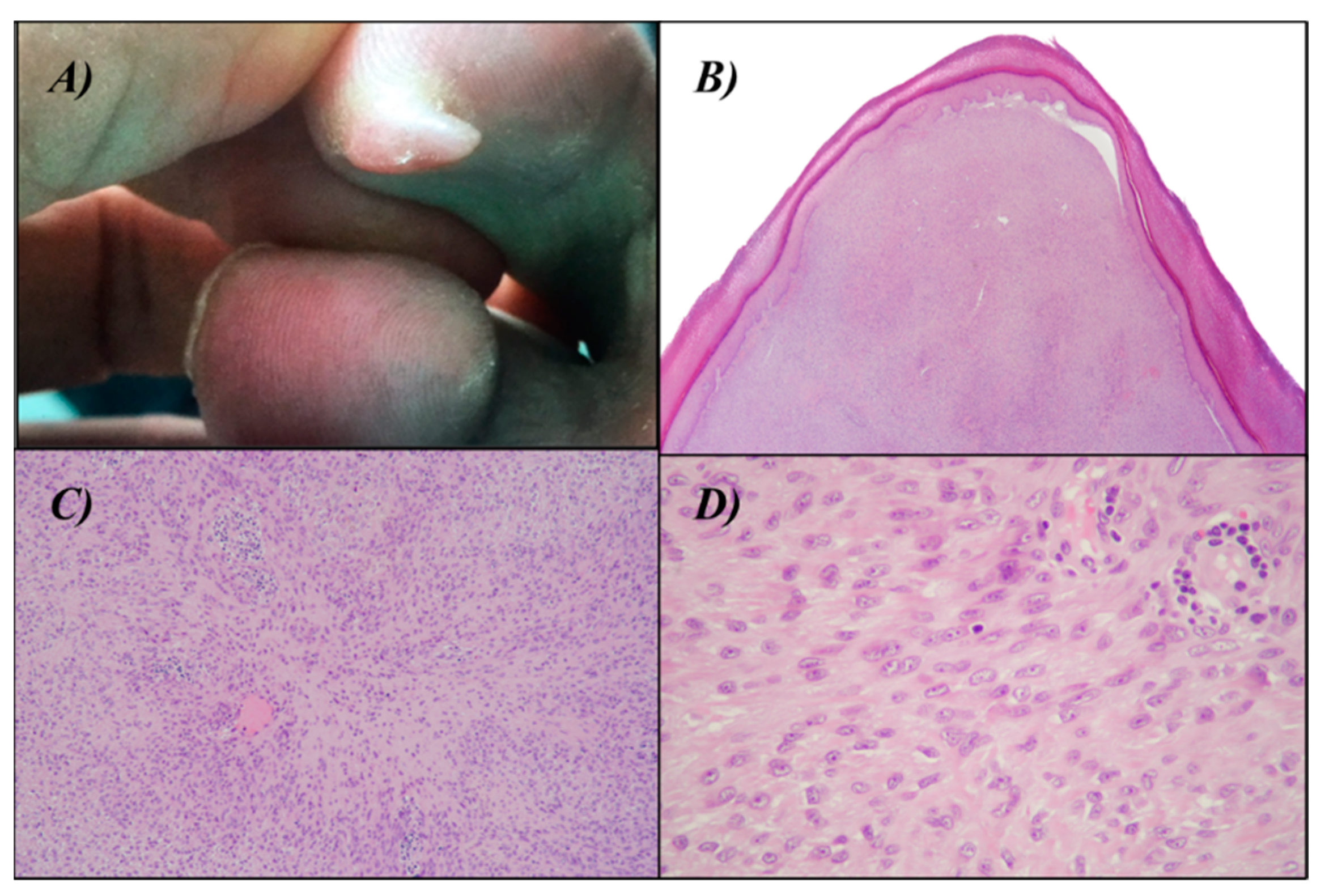
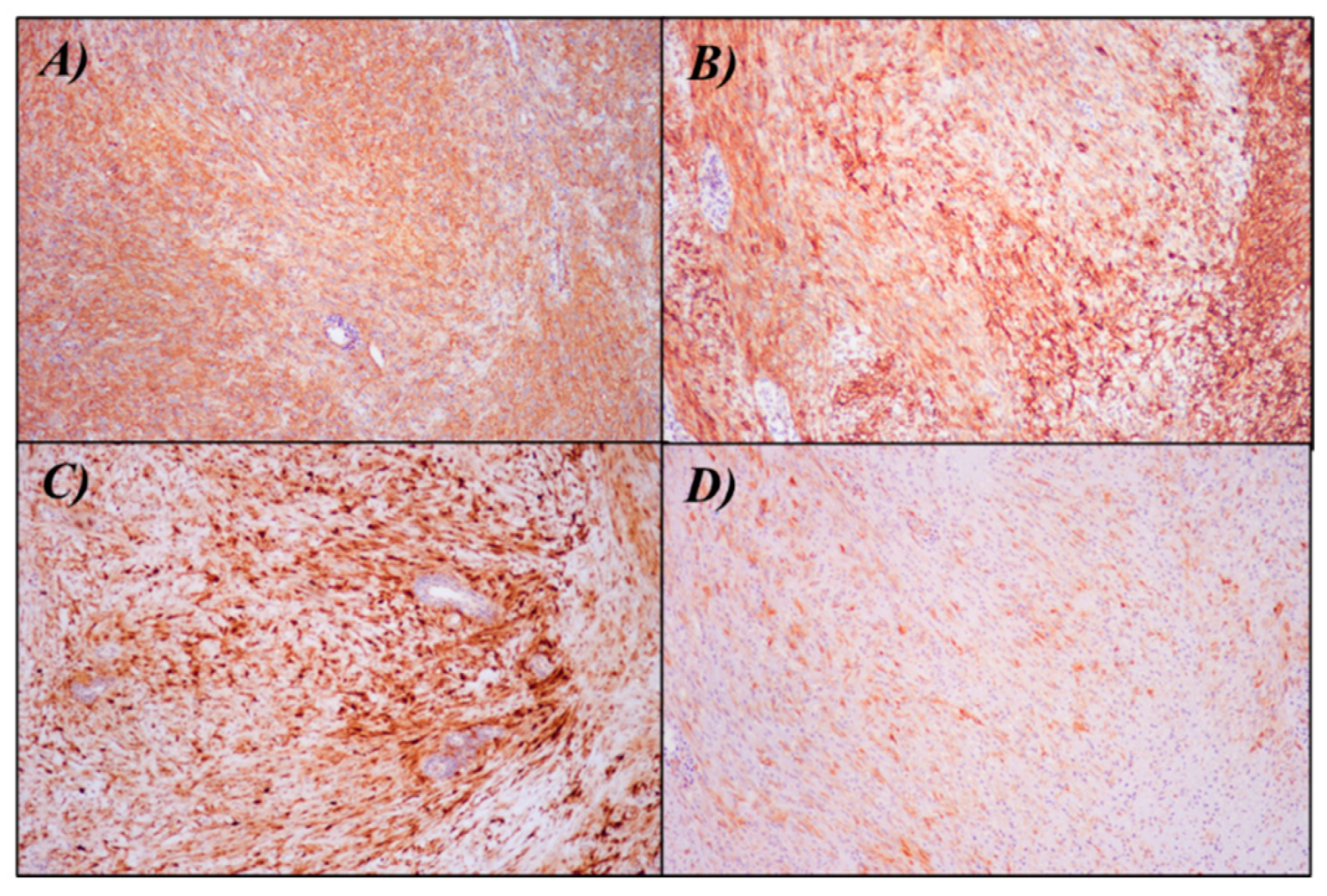
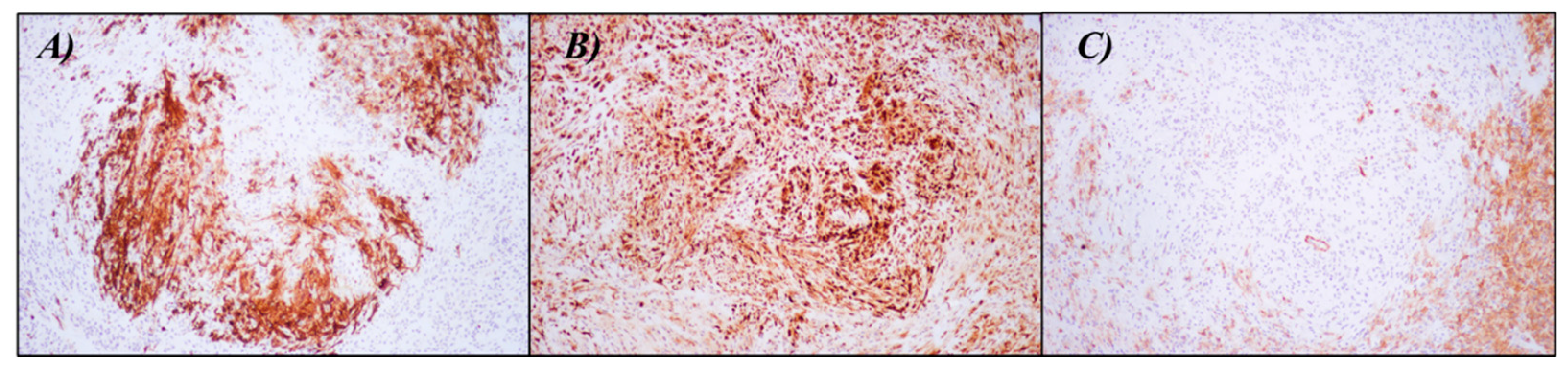
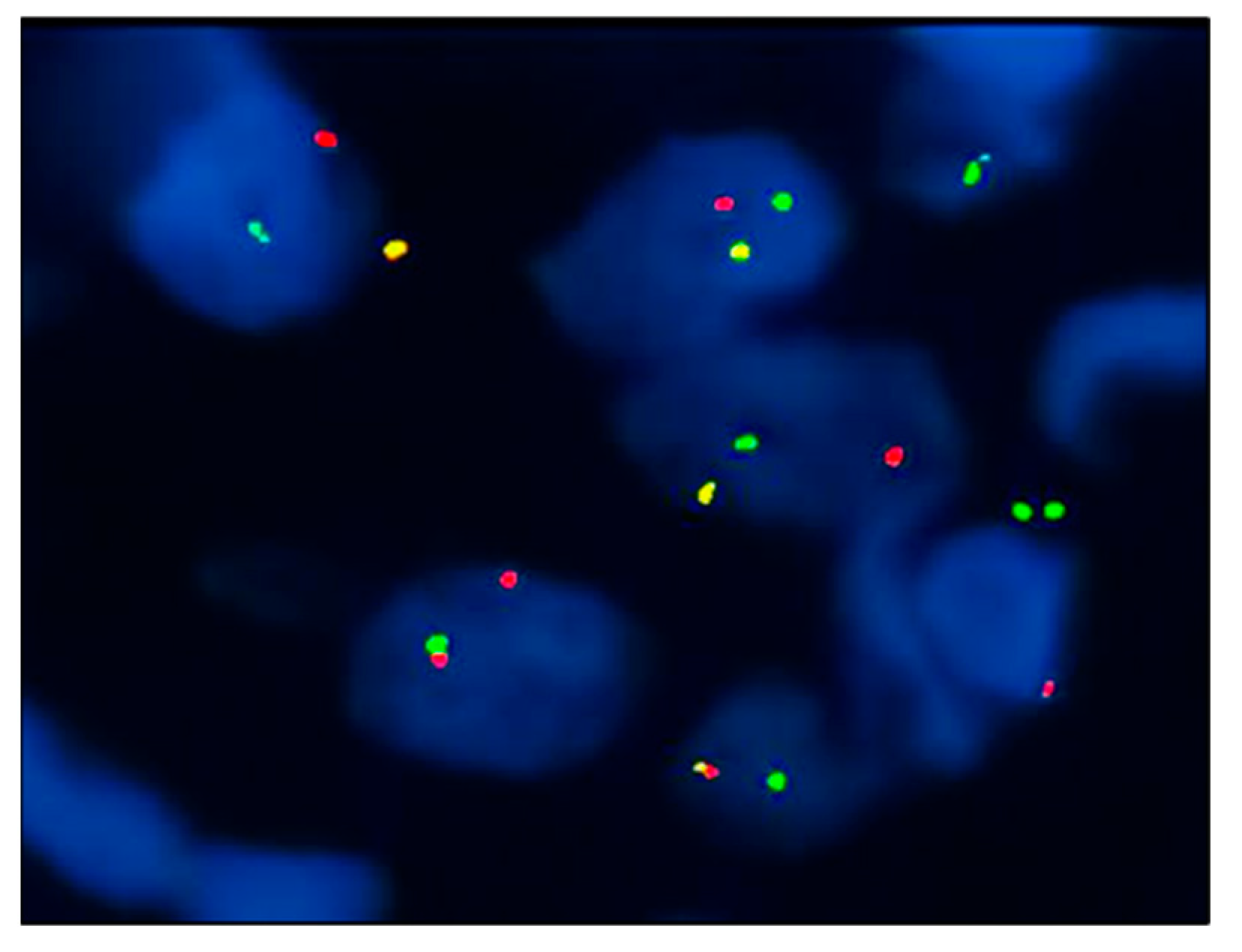
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gleason, B.C.; Hornick, J.L. Myoepithelial tumours of skin and soft tissue: An update. Diagn. Histopathol. 2008, 14, 552–562. [Google Scholar]
- Hornick, J.L.; Fletcher, C.D.M. Cutaneous myoepithelioma: A clinicopathologic and immunohistochemical study of 14 cases. Hum. Pathol. 2004, 35, 14–24. [Google Scholar] [PubMed]
- Jo, V.Y.; Antonescu, C.R.; Zhang, L.; Dal Cin, P.; Hornick, J.L.; Fletcher, C.D.M. Cutaneous syncytial myoepithelioma: Clinicopathologic characterization in a series of 38 cases. Am. J. Surg. Pathol. 2013, 37, 710–718. [Google Scholar] [PubMed]
- Jo, V.Y.; Antonescu, C.R.; Dickson, B.C.; Swanson, D.; Zhang, L.; Fletcher, C.D.M.; Demicco, E.G. Cutaneous Syncytial Myoepithelioma Is Characterized by Recurrent EWSR1-PBX3 Fusions. Am. J. Surg. Pathol. 2019, 43, 1349–1354. [Google Scholar]
- Pizzi, M.; Facchin, F.; Kohlscheen, E.; Sartore, L.; Salmaso, R.; Bassetto, F. Cutaneous syncytial myoepithelioma: Clinico-pathological features and differential diagnosis. Pathol. Res. Pract. 2016, 212, 954–956. [Google Scholar]
- Guillen-Climent, S.; Vazquez, B.; Pinazo, M.I.; Monteagudo, C. Painful Cutaneous Syncytial Myoepithelioma: From Nonspecific Symptoms to Histopathologic Diagnosis. Actas Dermosifiliogr. 2020, 111, 173–175. [Google Scholar]
- Plaza, J.A.; Brenn, T.; Chung, C.; Salim, S.; Linos, K.D.; Jour, G.; Duran Rincon, J.; Wick, M.; Sangueza, M.; Gru, A.A. Histomorphological and immunophenotypical spectrum of cutaneous myoepitheliomas: A series of 35 cases. J. Cutan. Pathol. 2021, 48, 847–855. [Google Scholar]
- Nagayasu, M.A.; Tanaka, H.; Nogami, K.; Kukita, Y.; Nakamura, H.; Motoi, T.; Manabe, T.; Kataoka, H. Cutaneous syncytial myoepithelioma with folliculocentric growth and EWSR1 gene rearrangement: A case report. J. Cutan. Pathol. 2023, 50, 400–404. [Google Scholar]
- Sidney, L.E.; Branch, M.J.; Dunphy, S.E.; Dua, H.S.; Hopkinson, A. Concise review: Evidence for CD34 as a common marker for diverse progenitors. Stem Cells 2014, 32, 1380–1389. [Google Scholar]
- Flint, A.; Weiss, S.W. CD-34 and keratin expression distinguishes solitary fibrous tumor (Fibrous mesothelioma) of pleura from desmoplastic mesothelioma. Hum. Pathol. 1995, 26, 428–431. [Google Scholar]
- Bhargava, R.; Shia, J.; Hummer, A.J.; Thaler, H.T.; Tornos, C.; Soslow, R.A. Distinction of endometrial stromal sarcomas from «hemangiopericytomatous» tumors using a panel of immunohistochemical stains. Mod. Pathol. 2005, 18, 40–47. [Google Scholar] [CrossRef]
- Lee, J.; Nguyen, P.T.; Shim, H.S.; Hyeon, S.J.; Im, H.; Choi, M.-H.; Chung, S.; Kowall, N.W.; Lee, S.B.; Ryu, H. EWSR1, a multifunctional protein, regulates cellular function and aging via genetic and epigenetic pathways. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2019, 1865, 1938–1945. [Google Scholar] [CrossRef]
- Morgan, R.; Pandha, H.S. PBX3 in Cancer. Cancers 2020, 12, 431. [Google Scholar] [CrossRef]
- Antonescu, C.R.; Zhang, L.; Shao, S.Y.; Mosquera, J.-M.; Weinreb, I.; Katabi, N.; Fletcher, C.D.M. Frequent PLAG1 gene rearrangements in skin and soft tissue myoepithelioma with ductal differentiation. Genes Chromosom. Cancer 2013, 52, 675–682. [Google Scholar] [PubMed]
- Alomari, A.K.; Brown, N.; Andea, A.A.; Betz, B.L.; Patel, R.M. Cutaneous syncytial myoepithelioma: A recently described neoplasm which may mimic nevoid melanoma and epithelioid sarcoma. J. Cutan. Pathol. 2017, 44, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Kao, E.Y.; Kernig, M.L. Neurothekeoma. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: http://www.ncbi.nlm.nih.gov/books/NBK519525/ (accessed on 24 June 2023).
- Wollina, U.; Hansel, G.; Schönlebe, J.; Haroske, G. Myxoid neurothekeoma—A painful case in a less common location. Dermatol. Online J. 2009, 15, 3. [Google Scholar] [CrossRef] [PubMed]
- Mizuta, H.; Takahashi, A.; Namikawa, K.; Ogata, D.; Yamazaki, N. Association between prognosis and complete resection in primary cutaneous myoepithelial carcinoma: Two case presentations and literature review. Dermatol. Ther. 2020, 33, e13485. [Google Scholar] [CrossRef]
- Hornick, J.L.; Fletcher, C.D.M. Myoepithelial tumors of soft tissue: A clinicopathologic and immunohistochemical study of 101 cases with evaluation of prognostic parameters. Am. J. Surg. Pathol. 2003, 27, 1183–1196. [Google Scholar] [CrossRef]
- Kacerovska, D.; Michal, M.; Kazakov, D.V. Hybrid Epithelioid Schwannoma/Perineurioma. Am. J. Dermatopathol. 2016, 38, e90–e92. [Google Scholar] [CrossRef]
- Luzar, B.; Calonje, E. Cutaneous fibrohistiocytic tumours—An update. Histopathology 2010, 56, 148–165. [Google Scholar] [CrossRef]
- Armah, H.B.; Parwani, A.V. Epithelioid sarcoma. Arch. Pathol. Lab. Med. 2009, 133, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Bains, A.; Parham, D.M. Langerhans cell histiocytosis preceding the development of juvenile xanthogranuloma: A case and review of recent developments. Pediatr. Dev. Pathol. 2011, 14, 480–484. [Google Scholar] [CrossRef] [PubMed]
- Fetsch, J.F.; Miettinen, M. Sclerosing perineurioma: A clinicopathologic study of 19 cases of a distinctive soft tissue lesion with a predilection for the fingers and palms of young adults. Am. J. Surg. Pathol. 1997, 21, 1433–1442. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.; Davey, J.; Gharpuray-Pandit, D.; Plaza, J.A.; Billings, S.D.; Balogh, P.; Tchrakian, N.; Selvan, S.; Wiedemeyer, K.; Hornick, J.L.; et al. Cutaneous Myoepithelial Neoplasms on Acral Sites Show Distinctive and Reproducible Histopathologic and Immunohistochemical Features. Am. J. Surg. Pathol. 2022, 46, 1241–1249. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ariasi, C.; Romanò, C.; Ghini, I.; Licata, G.; Rubelli, L.; Artelli, G.L.; Calzavara-Pinton, P.; Arisi, M. Cutaneous Syncytial Myoepithelioma with Positive CD34 Immunohistochemical Staining: An Unusual Tumor and a Challenging Diagnosis. Dermatopathology 2023, 10, 259-265. https://doi.org/10.3390/dermatopathology10030034
Ariasi C, Romanò C, Ghini I, Licata G, Rubelli L, Artelli GL, Calzavara-Pinton P, Arisi M. Cutaneous Syncytial Myoepithelioma with Positive CD34 Immunohistochemical Staining: An Unusual Tumor and a Challenging Diagnosis. Dermatopathology. 2023; 10(3):259-265. https://doi.org/10.3390/dermatopathology10030034
Chicago/Turabian StyleAriasi, Cesare, Carola Romanò, Iacopo Ghini, Gaetano Licata, Luca Rubelli, Grazia Linda Artelli, Piergiacomo Calzavara-Pinton, and Mariachiara Arisi. 2023. "Cutaneous Syncytial Myoepithelioma with Positive CD34 Immunohistochemical Staining: An Unusual Tumor and a Challenging Diagnosis" Dermatopathology 10, no. 3: 259-265. https://doi.org/10.3390/dermatopathology10030034
APA StyleAriasi, C., Romanò, C., Ghini, I., Licata, G., Rubelli, L., Artelli, G. L., Calzavara-Pinton, P., & Arisi, M. (2023). Cutaneous Syncytial Myoepithelioma with Positive CD34 Immunohistochemical Staining: An Unusual Tumor and a Challenging Diagnosis. Dermatopathology, 10(3), 259-265. https://doi.org/10.3390/dermatopathology10030034