

Uranium and Radium in Groundwater and Incidence of Colorectal Cancer in Georgia Counties, USA: An Ecologic Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Datasets
2.2. Spatial Clustering Analysis
2.3. Spatial Regression Analysis
3. Results
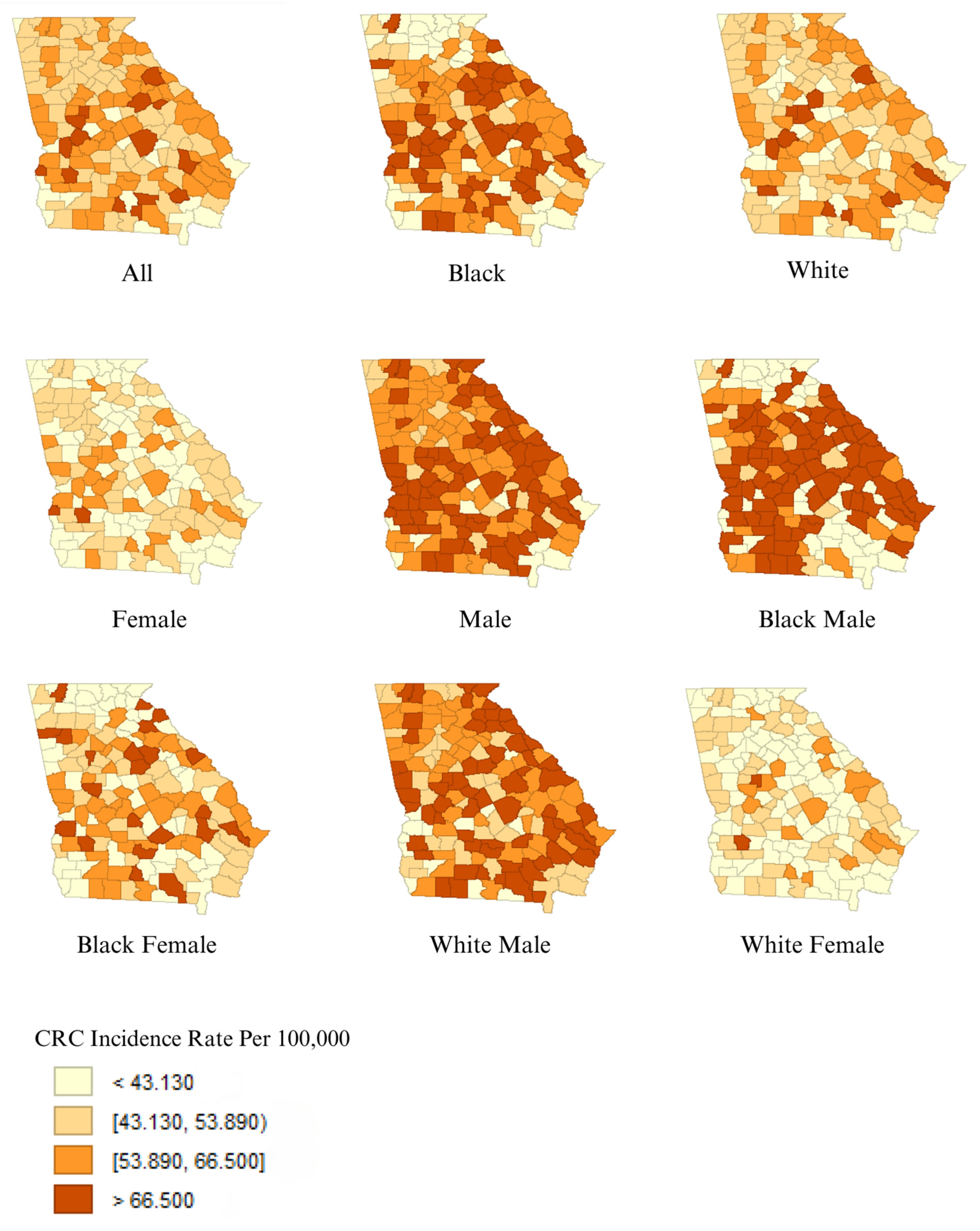
3.1. Descriptive Findings
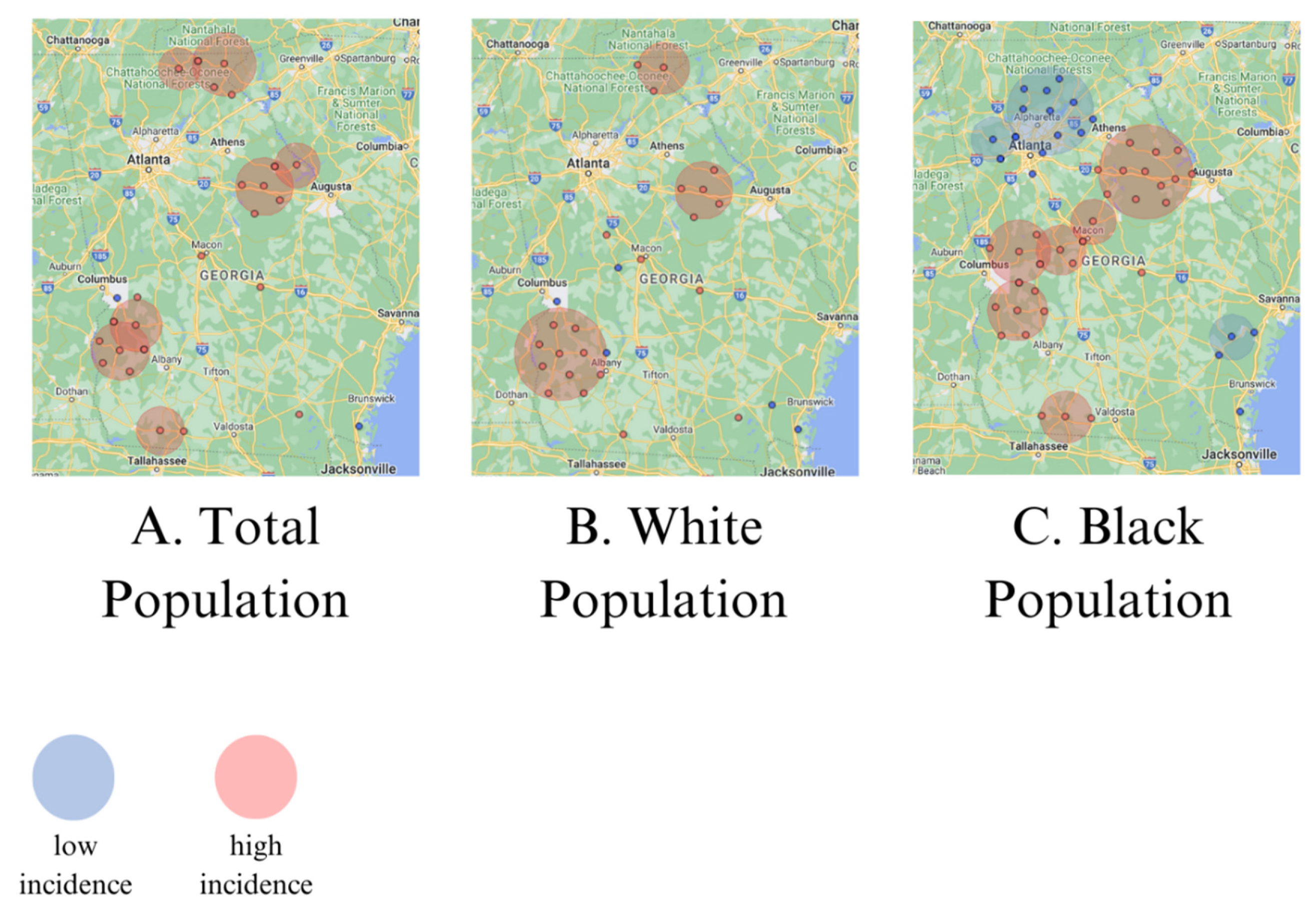
3.2. Spatial Clusters of CRC Incidence
3.3. Linear Regression between Radionuclides and CRC Incidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alzahrani, S.M.; Al Doghaither, H.A.; Al-Ghafari, A.B. General insight into cancer: An overview of colorectal cancer (Review). Mol. Clin. Oncol. 2021, 15, 271. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, T.; Ruszkowska, M.; Danielewicz, A.; Niedźwiedzka, E.; Arłukowicz, T.; Przybyłowicz, K.E. A Review of Colorectal Cancer in Terms of Epidemiology, Risk Factors, Development, Symptoms and Diagnosis. Cancers 2021, 13, 2025. [Google Scholar] [CrossRef] [PubMed]
- CDC. USCS Data Visualizations. Gis.cdc.gov. June 2021. Available online: https://gis.cdc.gov/Cancer/USCS/#/AtAGlance/ (accessed on 15 July 2024).
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Uranium; USDHHS: Atlanta, GA, USA, 2013. [Google Scholar]
- Kim, S.B.; Bozeman, R.G.; Kaisani, A.; Kim, W.; Zhang, L.; Richardson, J.A.; Wright, W.E.; Shay, J.W. Radiation promotes colorectal cancer initiation and progression by inducing senescence-associated inflammatory responses. Oncogene 2016, 35, 3365–3375. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, C.M.; Espinosa, A.; Gracia-Lavedan, E.; Vlaanderen, J.; Vermeulen, R.; Molina, A.J.; Amiano, P.; Gómez-Acebo, I.; Castaño-Vinyals, G.; Vineis, P.; et al. Exposure to widespread drinking water chemicals, blood inflammation markers, and colorectal cancer. Environ. Int. 2021, 157, 106873. [Google Scholar] [CrossRef] [PubMed]
- Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Radium; US Public Health Service & USEPA: Atlanta, GA, USA, 1990. [Google Scholar]
- Eisenbud, M. Natural radioactivity. In Environmental Radioactivity; Academic Press: New York, NY, USA, 1973; pp. 159–174. [Google Scholar]
- Wagner, S.E.; Burch, J.B.; Bottai, M.; Puett, R.; Porter, D.; Bolick-Aldrich, S.; Temples, T.; Wilkerson, R.C.; Vena, J.E.; Hébert, J.R. Groundwater uranium and cancer incidence in South Carolina. Cancer Causes Control 2011, 22, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Radespiel-Tröger, M.; Meyer, M. Association between drinking water uranium content and cancer risk in Bavaria, Germany. Int. Arch. Occup. Environ. Health 2013, 86, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.G.; Klug, M.G.; Rundquist, B.C. An exploration of colorectal cancer incidence rates in North Dakota, USA, via structural equation modeling. Int. J. Color. Dis. 2019, 34, 1571–1576. [Google Scholar] [CrossRef] [PubMed]
- Albertson, P.N. Naturally occurring radionuclides in Georgia water supplies: Implications for community water systems. In Proceedings of the 2003 Georgia Water Resources Conference, Athens, GA, USA, 23–24 April 2003; Hatcher, K.J., Ed.; [Google Scholar]
- United States Census. Profile of Selected Economic Characteristics: 2000. DP3. 2024. Available online: https://data.census.gov/table/DECENNIALDPSF32000.DP3?q=2000%20georgia%20county%20median%20household%20income&g=040XX00US13$0500000 (accessed on 15 July 2024).
- Georgia Department of Community Health. Georgia Rural Counties Map. 2021. Available online: https://dch.georgia.gov/divisionsoffices/state-office-rural-health/sorh-maps-georgia (accessed on 15 July 2024).
- Anselin, L. Exploring Spatial Data with GeoDa: A Workbook. 2005. Available online: https://geodacenter.github.io/documentation.html (accessed on 15 July 2024).
- American Cancer Society. Colorectal Cancer Facts & Figures 2008–2010. Atlanta, GA. 2008. Available online: www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/colorectal-cancer-facts-and-figures/colorectal-cancer-facts-and-figures-2008-2010.pdf (accessed on 15 July 2024).
- DeLancey, J.O.; Thun, M.J.; Jemal, A.; Ward, E.M. Recent trends in Black-White disparities in cancer mortality. Cancer Epidemiol. Biomark. Prev. 2008, 17, 2908–2912. [Google Scholar] [CrossRef] [PubMed]
- Lansdorp-Vogelaar, I.; Kuntz, K.M.; Knudsen, A.B.; van Ballegooijen, M.; Zauber, A.G.; Jemal, A. Contribution of screening and survival differences to racial disparities in colorectal cancer rates. Cancer Epidemiol. Biomark. Prev. 2012, 21, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Carson, T.L.; Byrd, D.A.; Smith, K.S.; Carter, D.; Gomez, M.; Abaskaron, M.; Little, R.B.; Holmes, S.T.; van Der Pol, W.J.; Lefkowitz, E.J.; et al. A case-control study of the association between the gut microbiota and colorectal cancer: Exploring the roles of diet, stress, and race. Gut Pathog. 2024, 16, 13. [Google Scholar] [CrossRef] [PubMed]
- Boice, J.D.; Cohen, S.S.; Mumma, M.T.; Dupree Ellis, E.; Eckerman, K.F.; Leggett, R.W.; Boecker, B.B.; Brill, A.B.; Henderson, B.E. Mortality among radiation workers at Rocketdyne (Atomics International), 1948–1999. Radiat. Res. 2006, 166 Pt 1, 98–115. [Google Scholar] [CrossRef] [PubMed]
- Lashner, B.A.; Epstein, S.S. Industrial risk factors for colorectal cancer. Int. J. Health Serv. 1990, 20, 459–483. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, H.; Misumi, M.; Brenner, A.; Grant, E.J.; Sakata, R.; Sadakane, A.; Utada, M.; Preston, D.L.; Mabuchi, K.; Ozasa, K. Radiation risk of incident colorectal cancer by anatomical site among atomic bomb survivors: 1958–2009. Int. J. Cancer 2020, 146, 635–645. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Med, IQR | No. of Counties | |
|---|---|---|
| No. of cases/county | 122 (61–224) | 159 |
| Age-adjusted population at risk/county | 227,000 (113,000–4,400,000) | 159 |
| Black–White incident rate ratio | 1.20 (1.04–1.40) | 159 |
| Black: White–incident rate difference * | 9.23 (2.14–19.40) | 159 |
| County HHI | 31,950 (27,873–38,782)1 | 159 |
| Water samples exceed uranium > 27 pCi/L | 31 | |
| Water samples exceed uranium > 270 pCi/L | 7 | |
| Water samples exceed radium > 5 pCi/L | 66 | |
| Urban counties | 51 |
| Radium > 5 pCi/L | Uranium > 27 pCi/L | Uranium > 270 pCi/L | ||||
|---|---|---|---|---|---|---|
| β | p-Value | Β | p-Value | β | p-Value | |
| All cases * | 0.27 | 0.004 | 0.12 | 0.33 | 0.13 | 0.52 |
| Black population * | 0.18 | 0.006 | 0.08 | 0.49 | −0.14 | 0.35 |
| White population * | 0.13 | 0.003 | 0.07 | 0.32 | 0.03 | 0.78 |
| Males | 0.12 | 0.004 | 0.06 | 0.34 | 0.06 | 0.59 |
| Females | 0.12 | 0.007 | 0.04 | 0.55 | 0.08 | 0.45 |
| Black males * | 0.20 | 0.005 | 0.14 | 0.23 | −0.12 | 0.46 |
| Black females * | 0.15 | 0.002 | 0.07 | 0.42 | 0.03 | 0.80 |
| White males * | 0.18 | 0.02 | 0.01 | 0.96 | −0.21 | 0.23 |
| White females * | 0.15 | 0.003 | 0.05 | 0.54 | 0.04 | 0.75 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rooney, T.; Soares, L.; Babalola, T.; Kensington, A.; Williams, J.; Meliker, J.R. Uranium and Radium in Groundwater and Incidence of Colorectal Cancer in Georgia Counties, USA: An Ecologic Study. Toxics 2024, 12, 705. https://doi.org/10.3390/toxics12100705
Rooney T, Soares L, Babalola T, Kensington A, Williams J, Meliker JR. Uranium and Radium in Groundwater and Incidence of Colorectal Cancer in Georgia Counties, USA: An Ecologic Study. Toxics. 2024; 12(10):705. https://doi.org/10.3390/toxics12100705
Chicago/Turabian StyleRooney, Taylor, Lissa Soares, Tesleem Babalola, Alex Kensington, Jennie Williams, and Jaymie R. Meliker. 2024. "Uranium and Radium in Groundwater and Incidence of Colorectal Cancer in Georgia Counties, USA: An Ecologic Study" Toxics 12, no. 10: 705. https://doi.org/10.3390/toxics12100705