
The Pleth Variability Index as a Guide to Fluid Therapy in Dogs Undergoing General Anesthesia: A Preliminary Study

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Anesthetic Management
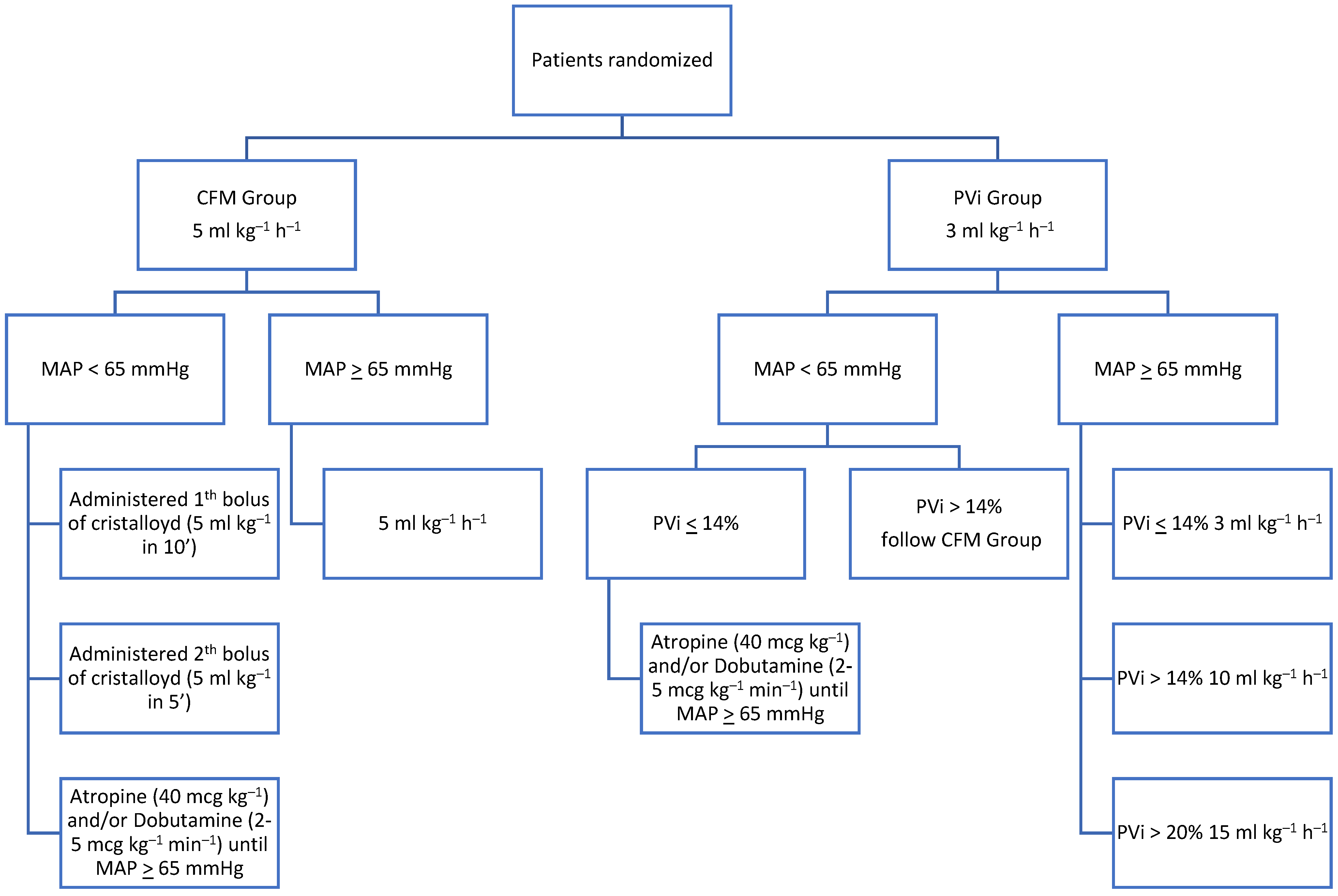
2.3. Study Protocol
2.4. Statistical Analysis
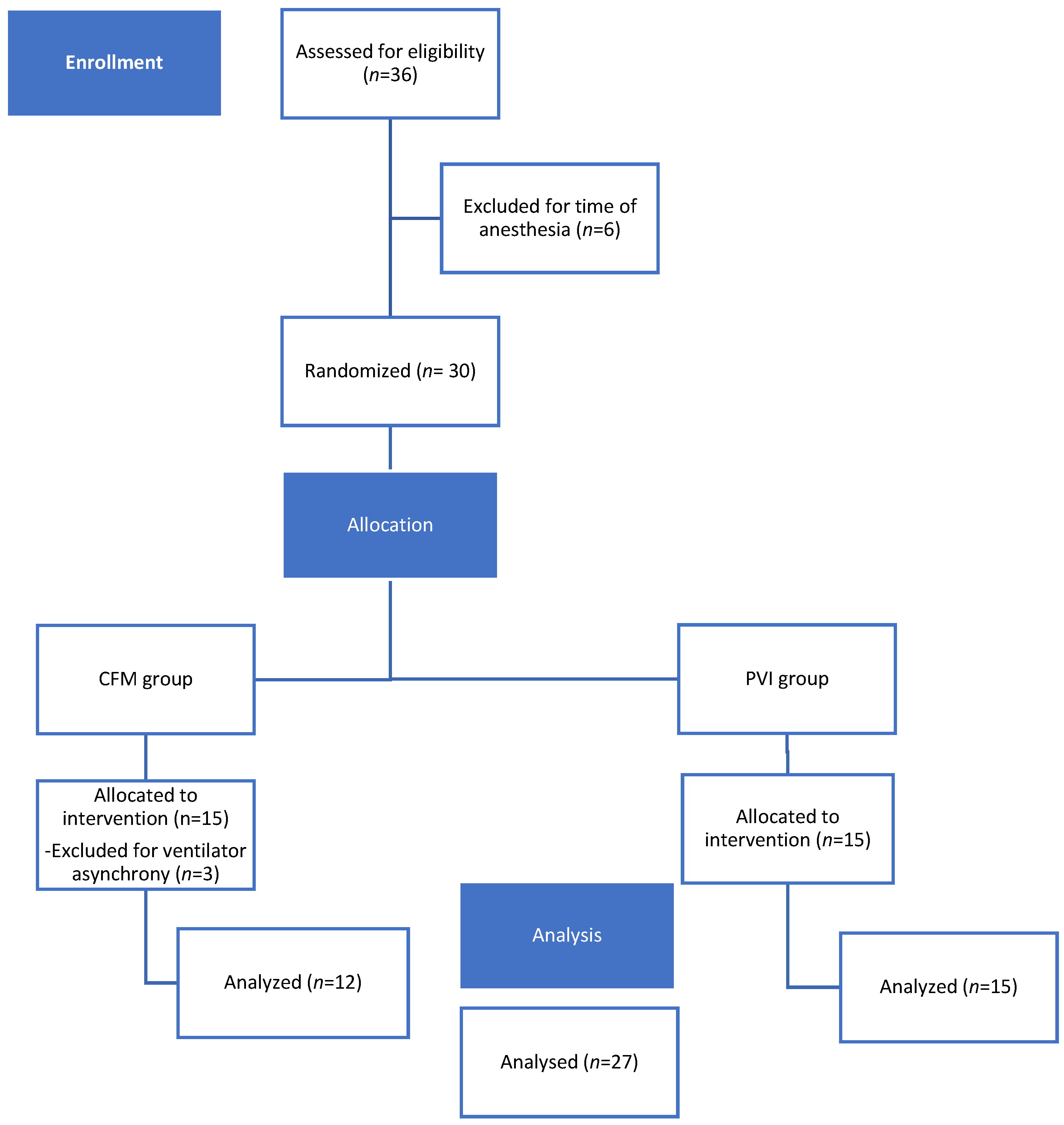
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Ghamdi, A. Intraoperative Fluid Management: Past and Future, Where Is the Evidence? Saudi J. Anaesth. 2018, 12, 311. [Google Scholar] [CrossRef] [PubMed]
- Le Manach, Y.; Hofer, C.K.; Lehot, J.-J.; Vallet, B.; Goarin, J.-P.; Tavernier, B.; Cannesson, M. Can Changes in Arterial Pressure Be Used to Detect Changes in Cardiac Output during Volume Expansion in the Perioperative Period? Anesthesiology 2012, 117, 1165–1174. [Google Scholar] [CrossRef]
- Marik, P.E.; Cavallazzi, R. Does the Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and a Plea for Some Common Sense. Crit. Care Med. 2013, 41, 1774–1781. [Google Scholar] [CrossRef] [PubMed]
- McDermid, R.C. Controversies in Fluid Therapy: Type, Dose and Toxicity. WJCCM 2014, 3, 24. [Google Scholar] [CrossRef]
- Hofer, C.K.; Cannesson, M. Monitoring Fluid Responsiveness. Acta Anaesthesiol. Taiwanica 2011, 49, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Pinsky, M.R. Heart–Lung Interactions. Curr. Opin. Crit. Care 2007, 13, 528–531. [Google Scholar] [CrossRef]
- Cannesson, M.; Attof, Y.; Rosamel, P.; Desebbe, O.; Joseph, P.; Metton, O.; Bastien, O.; Lehot, J.-J. Respiratory Variations in Pulse Oximetry Plethysmographic Waveform Amplitude to Predict Fluid Responsiveness in the Operating Room. Anesthesiology 2007, 106, 1105–1111. [Google Scholar] [CrossRef]
- Desebbe, O.; Cannesson, M. Using Ventilation-Induced Plethysmographic Variations to Optimize Patient Fluid Status. Curr. Opin. Anaesthesiol. 2008, 21, 772–778. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Feibicke, T.; Keyl, C.; Prasser, C.; Moritz, S.; Graf, B.M.; Wiesenack, C. Accuracy of Stroke Volume Variation Compared with Pleth Variability Index to Predict Fluid Responsiveness in Mechanically Ventilated Patients Undergoing Major Surgery. Eur. J. Anaesthesiol. 2010, 27, 555–561. [Google Scholar] [CrossRef]
- Michard, F.; Giglio, M.T.; Brienza, N. Perioperative Goal-Directed Therapy with Uncalibrated Pulse Contour Methods: Impact on Fluid Management and Postoperative Outcome. Br. J. Anaesth. 2017, 119, 22–30. [Google Scholar] [CrossRef]
- Davis, H.; Jensen, T.; Johnson, A.; Knowles, P.; Meyer, R.; Rucinsky, R.; Shafford, H. 2013 AAHA/AAFP Fluid Therapy Guidelines for Dogs and Cats. J. Am. Anim. Hosp. Assoc. 2013, 49, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, Z.U.; Mullenheim, J.W. Predicting Fluid Responsiveness. Trends Anaesth. Crit. Care 2012, 2, 15–19. [Google Scholar] [CrossRef]
- Forget, P.; Lois, F.; De Kock, M. Goal-Directed Fluid Management Based on the Pulse Oximeter–Derived Pleth Variability Index Reduces Lactate Levels and Improves Fluid Management. Anesth. Analg. 2010, 111, 910–914. [Google Scholar] [CrossRef]
- Tsuchiya, M.; Yamada, T.; Asada, A. Pleth Variability Index Predicts Hypotension during Anesthesia Induction. Acta Anaesthesiol. Scand. 2010, 54, 596–602. [Google Scholar] [CrossRef]
- Skouropoulou, D.; Lacitignola, L.; Di Bella, C.; Stabile, M.; Acquafredda, C.; Brienza, N.; Grasso, S.; Crovace, A.; Iarussi, F.; Staffieri, F. Intraoperative Assessment of Fluid Responsiveness in Normotensive Dogs under Isoflurane Anaesthesia. Vet. Sci. 2021, 8, 26. [Google Scholar] [CrossRef]
- Dwan, K.; Li, T.; Altman, D.G.; Elbourne, D. CONSORT 2010 Statement: Extension to Randomised Crossover Trials. BMJ 2019, 366, l4378. [Google Scholar] [CrossRef] [PubMed]
- Portier, K.; Ida, K.K. The ASA Physical Status Classification: What Is the Evidence for Recommending Its Use in Veterinary Anesthesia?—A Systematic Review. Front. Vet. Sci. 2018, 5, 204. [Google Scholar] [CrossRef]
- Reed, R.; Doherty, T. Minimum Alveolar Concentration: Key Concepts and a Review of Its Pharmacological Reduction in Dogs. Part 1. Res. Vet. Sci. 2018, 117, 266–270. [Google Scholar] [CrossRef]
- Felisberto, R.; Gonzalez, A.G.; Flaherty, D.; Casoria, V.; Auckburally, A. Validation of Oscillometric Blood Pressure Measurement Using a Datex S/5 Compact Multiparameter Monitor in Anaesthetized Adult Dogs. Vet. Anaesth. Analg. 2022, 49, 156–164. [Google Scholar] [CrossRef]
- Sedgwick, S.; Lorenzutti, A.M.; Araos, J.B.; Gleed, R.D.; Martin-Flores, M. Evaluation of an Oscillometric Blood Pressure Monitor in Anesthetized Dogs: Agreement with Direct Measurements and Ability to Detect Hypotension. Res. Vet. Sci. 2021, 135, 162–166. [Google Scholar] [CrossRef]
- Acierno, M.J.; Brown, S.; Coleman, A.E.; Jepson, R.E.; Papich, M.; Stepien, R.L.; Syme, H.M. ACVIM Consensus Statement: Guidelines for the Identification, Evaluation, and Management of Systemic Hypertension in Dogs and Cats. Vet. Intern. Medicne 2018, 32, 1803–1822. [Google Scholar] [CrossRef] [PubMed]
- Doherty, M.; Buggy, D.J. Intraoperative Fluids: How Much Is Too Much? Br. J. Anaesth. 2012, 109, 69–79. [Google Scholar] [CrossRef]
- Holte, K.; Sharrock, N.E.; Kehlet, H. Pathophysiology and Clinical Implications of Perioperative Fluid Excess. Br. J. Anaesth. 2002, 89, 622–632. [Google Scholar] [CrossRef]
- Chong, M.A.; Wang, Y.; Berbenetz, N.M.; McConachie, I. Does Goal-Directed Haemodynamic and Fluid Therapy Improve Peri-Operative Outcomes?: A Systematic Review and Meta-Analysis. Eur. J. Anaesthesiol. 2018, 35, 469–483. [Google Scholar] [CrossRef] [PubMed]
- Alimian, M.; Mohseni, M.; Moradi Moghadam, O.; Seyed Siamdoust, S.A.; Moazzami, J. Effects of Liberal Versus Restrictive Fluid Therapy on Renal Function Indices in Laparoscopic Bariatric Surgery. Anesth. Pain Med. 2020, 10, e95378. [Google Scholar] [CrossRef]
- Noel-Morgan, J.; Muir, W.W. Anesthesia-Associated Relative Hypovolemia: Mechanisms, Monitoring, and Treatment Considerations. Front. Vet. Sci. 2018, 5, 53. [Google Scholar] [CrossRef] [PubMed]
- Fantoni, D.; Shih, A.C. Perioperative Fluid Therapy. Vet. Clin. N. Am. Small Anim. Pract. 2017, 47, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Bundgaard-Nielsen, M.; Jørgensen, C.C.; Secher, N.H.; Kehlet, H. Functional Intravascular Volume Deficit in Patients before Surgery. Acta Anaesthesiol. Scand. 2010, 54, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Bennett, V.; Cecconi, M. Perioperative Fluid Management: From Physiology to Improving Clinical Outcomes. Indian J. Anaesth. 2017, 61, 614. [Google Scholar] [CrossRef]
- Miller, T.E.; Roche, A.M.; Mythen, M. Fluid Management and Goal-Directed Therapy as an Adjunct to Enhanced Recovery After Surgery (ERAS). Can. J. Anesth. 2015, 62, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Aditianingsih, D.; George, Y.W.H. Guiding Principles of Fluid and Volume Therapy. Best Pract. Res. Clin. Anaesthesiol. 2014, 28, 249–260. [Google Scholar] [CrossRef]
- Cecconi, M.; Parsons, A.K.; Rhodes, A. What Is a Fluid Challenge? Curr. Opin. Crit. Care 2011, 17, 290–295. [Google Scholar] [CrossRef]
- Araos, J.; Kenny, J.-E.S.; Rousseau-Blass, F.; Pang, D.S. Dynamic Prediction of Fluid Responsiveness during Positive Pressure Ventilation: A Review of the Physiology Underlying Heart–Lung Interactions and a Critical Interpretation. Vet. Anaesth. Analg. 2020, 47, 3–14. [Google Scholar] [CrossRef]
- Fine, D.M.; Durham, H.E., Jr.; Rossi, N.F.; Spier, A.W.; Selting, K.; Rubin, L.J. Echocardiographic Assessment of Hemodynamic Changes Produced by Two Methods of Inducing Fluid Deficit in Dogs. J. Vet. Intern. Med. 2010, 24, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Urhan, G.; Demirel, İ.; Deniz, A.; Aksu, A.; Altun, A.Y.; Bolat, E.; Beştaş, A.; Altuntaş, G. Comparison of Dynamic Measures in Intraoperative Goal-Directed Fluid Therapy of Patients with Morbid Obesity Undergoing Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2024, 34, 1600–1607. [Google Scholar] [CrossRef]
- Cannesson, M.; Desebbe, O.; Rosamel, P.; Delannoy, B.; Robin, J.; Bastien, O.; Lehot, J.-J. Pleth Variability Index to Monitor the Respiratory Variations in the Pulse Oximeter Plethysmographic Waveform Amplitude and Predict Fluid Responsiveness in the Operating Theatre. Br. J. Anaesth. 2008, 101, 200–206. [Google Scholar] [CrossRef]
- Coeckelenbergh, S.; Delaporte, A.; Ghoundiwal, D.; Bidgoli, J.; Fils, J.-F.; Schmartz, D.; Van Der Linden, P. Pleth Variability Index versus Pulse Pressure Variation for Intraoperative Goal-Directed Fluid Therapy in Patients Undergoing Low-to-Moderate Risk Abdominal Surgery: A Randomized Controlled Trial. BMC Anesth. 2019, 19, 34. [Google Scholar] [CrossRef]
- Mathew, P.J.; Sharma, S.; Bhardwaj, N.; Ashok, V.; Malik, M.A. Goal-Directed Fluid Therapy Guided by Plethysmographic Variability Index (PVI) versus Conventional Liberal Fluid Administration in Children during Elective Abdominal Surgery: A Randomized Controlled Trial. J. Pediatr. Surg. 2023, 58, 735–740. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CFM-Group (n = 12) (95% CI) | PVI-Group (n = 15) (95% CI) | p | |
|---|---|---|---|
| Sex (female/male; n) | 7/5 | 5/10 | 0.212 |
| Age (months) | 42.5 ± 34.25 (20.73–64.26) | 85.66 ± 37.71 (64.78–106.55) | 0.005 * |
| Body weight (kg) | 35.22 ± 13.77 (26.47–43.97) | 29.13 ± 13.13 (21.86–36.40) | 0.252 |
| CFM-Group (95% CI) | PVI-Group (95% CI) | p | |
|---|---|---|---|
| MAP at the beginning (mmHg) | 85.16 ± 19.74 | 94.2 ± 23.92 | 0.303 |
| Duration of anesthesia (min) | 151.66 ± 86.21 (96.88–206.44) | 134.66 ± 66.24 (97.98–171.35) | 0.562 |
| Duration of surgery (min) | 76.25 ± 82.11 (24.07–128.42) | 53.66 ± 38.27 (32.47–74.86) | 0.351 |
| Duration of PVi study (min) | 82.08 ± 62.33 (42.48–121.68) | 73 ± 41.78 (49.86–96.13) | 0.654 |
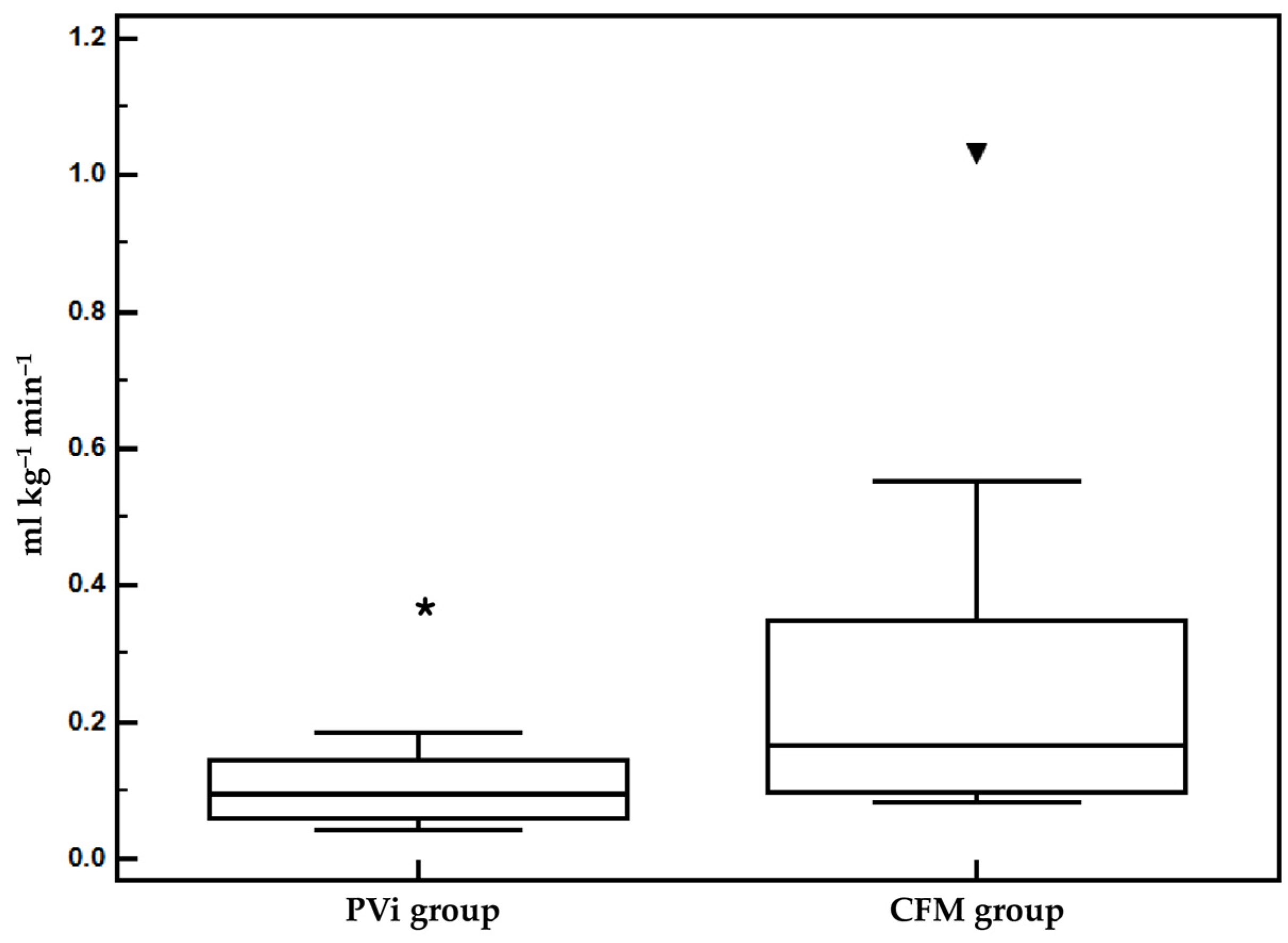
| Amount of fluids (mL kg−1 min−1) | 0.132 ± 0.115 (0.058–0.20) | 0.056 ± 0.27 (0.04–0.07) | 0.022 * |
| CFM-Group (95% CI) | PVI-Group (95% CI) | p | |
|---|---|---|---|
| HR (beats/min) | |||
| T0 | 76.41 ± 26.56 (59.53–93.29) | 83.26 ± 19.62 (72.40–94.13) | 0.443 |
| T1/2 | 78.25 ± 25.88 (61.80–94.69) | 70.13 ± 13.17 (72.40–94.13) | 0.296 |
| Tend | 85.08 ± 25.51 (68.87–101.29) | 74.86 ± 13.22 (67.54–82.18) | 0.197 |
| SAP (mmHg) | |||
| T0 | 109.91 ± 17.54 (98.76–121.06) | 119.71 ± 17.95 (109.78–129.67) | 0.164 |
| T1/2 | 108.41 ± 17.40 (97.36–119.47) | 115.86 ± 16.15 (106.91–124.81) | 0.262 |
| Tend | 115.83 ± 16.40 (105.41–126.25) | 115.6 ± 10.73 (109.65–121.54) | 0.963 |
| MAP (mmHg) | |||
| T0 | 73.25 ± 15.11 (63.64–82.85) | 85.13 ± 16.67 (75.90–94.36) | 0.067 |
| T1/2 | 74.083 ± 9.2 (68.22–79.94) | 84.66 ± 14.70 (76.52–92.81) | 0.039 * |
| Tend | 75.167 ± 6.68 (70.91–79.41) | 84 ± 10.13 (78.38–89.61) | 0.015 * |
| DAP (mmHg) | |||
| T0 | 61.08 ± 12.24 (53.30–68.86) | 70.93 ± 14.94 (62.65–79.21) | 0.078 |
| T1/2 | 66.08 ± 15.79 (56.04–76.12) | 71.6 ± 15.58 (62.96–80.23) | 0.372 |
| Tend | 66.58 ± 14.89 (57.11–76.04) | 69.8 ± 12.13 (63.08–76.51) | 0.542 |
| RR (breaths/min) | |||
| T0 | 14.5 ± 2.1106 (13.159–15.841) | 13.333 ± 3.2878 (11.513–15.154) | 0.297 |
| T1/2 | 15.333 ± 3.6013 (13.045–17.622) | 13 ± 2.9277 (11.379–14.621) | 0.074 |
| Tend | 15.583 ± 4.358 (12.814–18.352) | 13.333 ± 2.9921 (11.676–14.990) | 0.124 |
| PVi (%) | |||
| T0 | 15.33 ± 5.80 (11.64–19.02) | 17.53 ± 7.94 (13.12–21.93) | 0.431 |
| T1/2 | 12.75 ± 4.57 (9.84–15.65) | 15.2 ± 7.32 (11.14–19.25) | 0.322 |
| Tend | 12 ± 6.09 (8.13–15.87) | 11.8 ± 4.24 (9.44–14.15) | 0.921 |
| PI | |||
| T0 | 1.8 ± 1.6 (0.74–2.85) | 1.65 ± 1.50 (0.78–2.52) | 0.817 |
| T1/2 | 1.87 ± 1.19 (1.11–2.63) | 1.63 ± 0.94 (1.08–2.18) | 0.573 |
| Tend | 1.52 ± 0.97 (0.83–2.06) | 1.31 ± 0.91 (0.78–1.84) | 0.584 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vicenti, C.; Romagnoli, N.; Stabile, M.; Lambertini, C.; Piemontese, C.; Spaccini, F.; Foglia, A.; Lacitignola, L.; Crovace, A.; Staffieri, F. The Pleth Variability Index as a Guide to Fluid Therapy in Dogs Undergoing General Anesthesia: A Preliminary Study. Vet. Sci. 2024, 11, 396. https://doi.org/10.3390/vetsci11090396
Vicenti C, Romagnoli N, Stabile M, Lambertini C, Piemontese C, Spaccini F, Foglia A, Lacitignola L, Crovace A, Staffieri F. The Pleth Variability Index as a Guide to Fluid Therapy in Dogs Undergoing General Anesthesia: A Preliminary Study. Veterinary Sciences. 2024; 11(9):396. https://doi.org/10.3390/vetsci11090396
Chicago/Turabian StyleVicenti, Caterina, Noemi Romagnoli, Marzia Stabile, Carlotta Lambertini, Claudia Piemontese, Francesca Spaccini, Armando Foglia, Luca Lacitignola, Antonio Crovace, and Francesco Staffieri. 2024. "The Pleth Variability Index as a Guide to Fluid Therapy in Dogs Undergoing General Anesthesia: A Preliminary Study" Veterinary Sciences 11, no. 9: 396. https://doi.org/10.3390/vetsci11090396