
Possible Correlation between Mucin Gene Expression and Symptoms of Dry Eye Syndrome Secondary to Sjogren’s Disease

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Recruitment
2.2. Clinical Assessment of Patients
2.2.1. Tear Stability Test
2.2.2. Tear Production Assessment
2.2.3. OS Damage Assessment
2.2.4. Dry Eye Symptom Assessment
2.3. Obtention of the Conjunctival Samples
2.4. Messenger RNA (mRNA) Extraction Method
2.5. Gene Expression by qRT-PCR
2.6. Statistical Analysis
3. Results
3.1. Patient Population and Analysis of the Ocular Surface
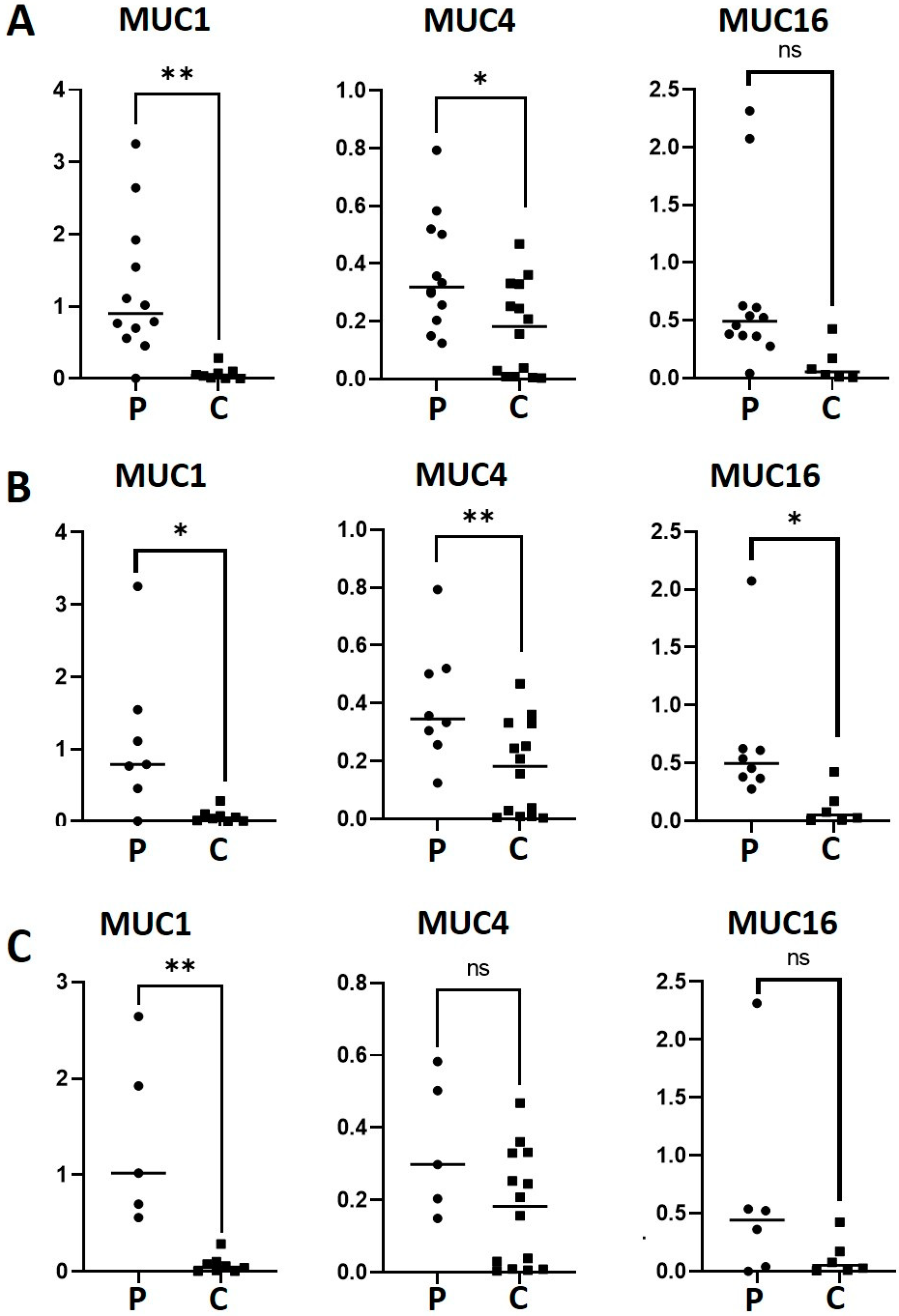
3.2. Gene Expression of MUC1, MUC4 and MUC16 in Conjunctival Impression Samples in Patients with SS-DED versus Healthy Controls
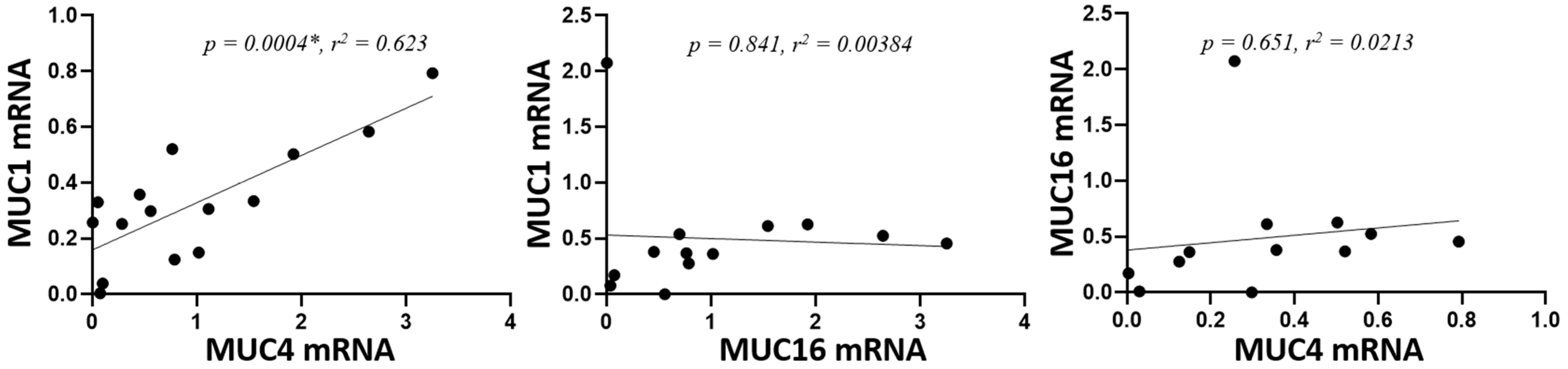
3.3. Correlation of the Expression of MUC1, MUC4 and MUC16 in SS-DED and Controls
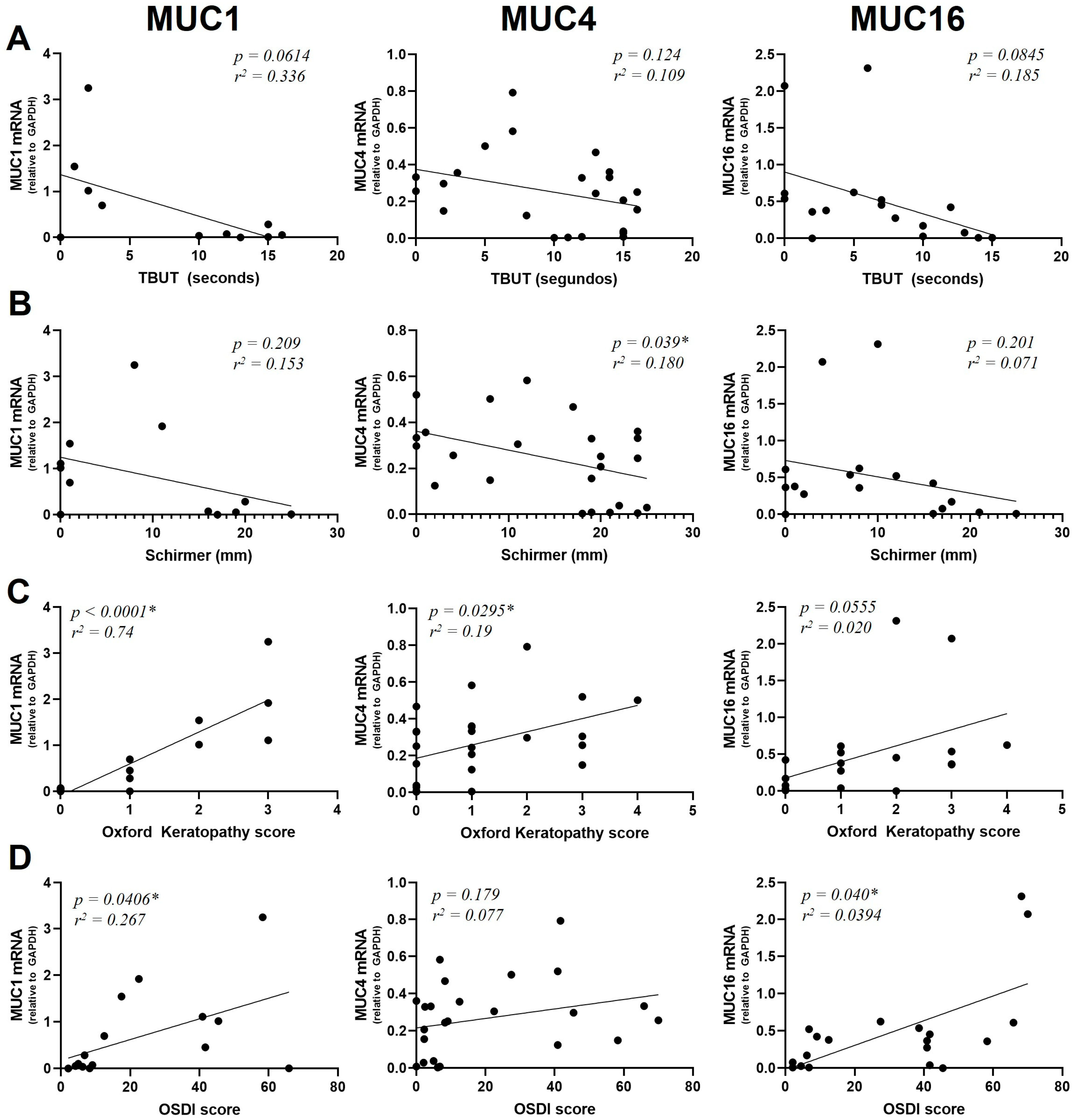
3.4. Relationship between Mucin Gene Expression and Clinical Parameters of DED
3.4.1. TBUT and Mucin Expression
3.4.2. Schirmer I Test and Mucin Expression
3.4.3. Superficial Keratopathy and Mucin Expression
3.4.4. OSDI Score and Mucin Expression
3.5. Expression of IL-17 and IL-22 in SS-DED
3.6. Correlation of IL-17 and IL-22 with Clinical Parameters of Patients with SS-DED
4. Discussion
4.1. Differential Mucin Gene Expression in SS-DED
4.2. IL-17 and IL-22 Expression in SS-DED
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Papas, E.B. The global prevalence of dry eye disease: A Bayesian view. Ophthalmic Physiol. Opt. 2021, 41, 1254–1266. [Google Scholar] [CrossRef] [PubMed]
- Mehra, D.; Galor, A. Digital screen use and dry eye: A review. Asia-Pac. J. Ophthalmol. 2020, 9, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Mandell, J.T.; Idarraga, M.; Kumar, N.; Galor, A. Impact of Air Pollution and Weather on Dry Eye. J. Clin. Med. 2020, 9, 3740. [Google Scholar] [CrossRef]
- Akpek, E.K.; Amescua, G.; Farid, M.; Garcia-Ferrer, F.J.; Lin, A.; Rhee, M.K.; Varu, D.M.; Musch, D.C.; Dunn, S.P.; Mah, F.S. Dry Eye Syndrome Preferred Practice Pattern®. Ophthalmology 2019, 126, P286–P334. [Google Scholar] [CrossRef]
- Brito-Zerón, P.; Baldini, C.; Bootsma, H.; Bowman, S.J.; Jonsson, R.; Mariette, X.; Sivils, K.; Theander, E.; Tzioufas, A.; Ramos-Casals, M. Sjogren syndrome. Nat. Rev. Dis. Primers 2016, 2, 16047. [Google Scholar] [CrossRef]
- Mantelli, F.; Argüeso, P. Functions of ocular surface mucins in health and disease. Curr. Opin. Allergy Clin. Immunol. 2008, 8, 477–483. [Google Scholar] [CrossRef] [PubMed]
- De Paiva, C.S.; Leger, A.J.S.; Caspi, R.R. Mucosal immunology of the ocular surface. Mucosal Immunol. 2022, 15, 1143–1157. [Google Scholar] [CrossRef]
- Argüeso, P.; Balaram, M.; Spurr-Michaud, S.; Keutmann, H.T.; Dana, M.R.; Gipson, I.K. Decreased levels of the goblet cell mucin MUC5AC in tears of patients with Sjögren syndrome. Investig. Ophthalmol. Vis. Sci. 2002, 43, 1004–1011. [Google Scholar]
- Caffery, B.; Heynen, M.L.; Joyce, E.; Jones, L.; Ritter, R., III; Senchyna, M. MUC1 expression in Sjogren’s syndrome, KCS, and control subjects. Mol. Vis. 2010, 16, 1720–1727. [Google Scholar]
- Caffery, B.; Joyce, E.; Heynen, M.L.; Jones, L.; Ritter, R., III; Gamache, D.A.; Senchyna, M. MUC16 expression in Sjogren’s syndrome, KCS, and control subjects. Mol. Vis. 2008, 14, 2547–2555. [Google Scholar]
- Jones, D.T.; Monroy, D.; Ji, Z.; Pflugfelder, S.C. Alterations of ocular surface gene expression in Sjögren’s syndrome. Adv. Exp. Med. Biol. 1998, 438, 533–536. [Google Scholar]
- Na, K.-S.; Hwang, K.-Y.; Lee, H.-S.; Chung, S.-H.; Mok, J.W.; Joo, C.-K. Wakayama symposium: Interface between innate and adaptive immunity in dry eye disease. BMC Ophthalmol. 2015, 15, 159. [Google Scholar] [CrossRef] [PubMed]
- Chivasso, C.; Sarrand, J.; Perret, J.; Delporte, C.; Soyfoo, M.S. The Involvement of Innate and Adaptive Immunity in the Initiation and Perpetuation of Sjögren’s Syndrome. Int. J. Mol. Sci. 2021, 22, 658. [Google Scholar] [CrossRef]
- Dungan, L.S.; Mills, K.H. Caspase-1-processed IL-1 family cytokines play a vital role in driving innate IL-17. Cytokine 2011, 56, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, T.T.; Monteleone, G. Immunity, inflammation, and allergy in the gut. Science 2005, 307, 1920–1925. [Google Scholar] [CrossRef]
- Dudakov, J.A.; Hanash, A.M.; van den Brink, M.R. Interleukin-22: Immunobiology and pathology. Annu. Rev. Immunol. 2015, 33, 747–785. [Google Scholar] [CrossRef]
- Tan, X.; Sun, S.; Liu, Y.; Zhu, T.; Wang, K.; Ren, T.; Wu, Z.; Xu, H.; Zhu, L. Analysis of Th17-associated cytokines in tears of patients with dry eye syndrome. Eye 2014, 28, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wu, C. The relationship between intestinal goblet cells and the immune response. Biosci. Rep. 2020, 40, BSR20201471. [Google Scholar] [CrossRef]
- Oxford Grading System. Available online: https://www.aao.org/education/image/oxford-grading-system (accessed on 1 December 2023).
- Leanne Spiegle. How to Use Dry Eye Questionnaires in Your Practice. Available online: https://www.reviewofoptometry.com/article/how-to-use-dry-eye-questionnaires-in-your-practice (accessed on 1 December 2023).
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and Validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef]
- Bustos, N.A.; Ribbeck, K.; Wagner, C.E. The role of mucosal barriers in disease progression and transmission. Adv. Drug Deliv. Rev. 2023, 200, 115008. [Google Scholar] [CrossRef]
- Dhar, P.; McAuley, J. The Role of the Cell Surface Mucin MUC1 as a Barrier to Infection and Regulator of Inflammation. Front. Cell. Infect. Microbiol. 2019, 9, 117. [Google Scholar] [CrossRef]
- Xavier, R.J.; Podolsky, D.K. Unravelling the pathogenesis of inflammatory bowel disease. Nature 2007, 448, 427–434. [Google Scholar] [CrossRef]
- Karin, M.; Greten, F.R. NF-kappaB: Linking inflammation and immunity to cancer development and progression. Nat. Rev. Immunol. 2005, 5, 749–759. [Google Scholar] [CrossRef]
- Buisine, M.-P.; Devisme, L.; Copin, M.-C.; Durand-Réville, M.; Gosselin, B.; Aubert, J.-P.; Porchet, N. Developmental mucin gene expression in the human respiratory tract. Am. J. Respir. Cell Mol. Biol. 1999, 20, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Damera, G.; Xia, B.; Sachdev, G.P. IL-4 induced MUC4 enhancement in respiratory epithelial cells in vitro is mediated through JAK-3 selective signaling. Respir. Res. 2006, 7, 39. [Google Scholar] [CrossRef]
- Damera, G.; Xia, B.; Ancha, H.R.; Sachdev, G.P. IL-9 modulated MUC4 gene and glycoprotein expression in airway epithelial cells. Biosci. Rep. 2006, 26, 55–67. [Google Scholar] [CrossRef]
- Fischer, B.M.; Cuellar, J.G.; Diehl, M.L.; Defreytas, A.M.; Zhang, J.; Carraway, K.L.; Voynow, J.A. Neutrophil elastase increases MUC4 expression in normal human bronchial epithelial cells. Am. J. Physiol. Cell. Mol. Physiol. 2003, 284, L671–L679. [Google Scholar] [CrossRef]
- Das, S.; Rachagani, S.; Sheinin, Y.; Smith, L.M.; Gurumurthy, C.B.; Roy, H.K.; Batra, S.K. Mice deficient in Muc4 are resistant to experimental colitis and colitis-associated colorectal cancer. Oncogene 2016, 35, 2645–2654. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Li, L.; Luo, N.; Liu, Q.; Liu, L.; Chen, D.; Cheng, Z.; Xi, X. Inflammatory signals induce MUC16 expression in ovarian cancer cells via NF-κB activation. Exp. Ther. Med. 2021, 21, 163. [Google Scholar] [CrossRef] [PubMed]
- Paulsen, F.; Jäger, K.; Worlitzsch, D.; Bräuer, L.; Schulze, U.; Schäfer, G.; Sel, S. Regulation of MUC16 by inflammatory mediators in ocular surface epithelial cell lines. Ann. Anat. Anat. Anz. 2008, 190, 59–70. [Google Scholar] [CrossRef]
- Solomon, A.; Dursun, D.; Liu, Z.; Xie, Y.; Macri, A.; Pflugfelder, S.C. Pro- and anti-inflammatory forms of interleukin-1 in the tear fluid and conjunctiva of patients with dry-eye disease. Investig. Ophthalmol. Vis. Sci. 2001, 42, 2283–2292. [Google Scholar]
- Argüeso, P.; Tisdale, A.; Mandel, U.; Letko, E.; Foster, C.S.; Gipson, I.K. The cell-layer- and cell-type-specific distribution of GalNAc-transferases in the ocular surface epithelia is altered during keratinization. Investig. Ophthalmol. Vis. Sci. 2003, 44, 86–92. [Google Scholar] [CrossRef]
- Cheng, P.W.; Radhakrishnan, P. Mucin O-glycan branching enzymes: Structure, function, and gene regulation. Adv. Exp. Med. Biol. 2011, 705, 465–492. [Google Scholar]
- Hoşal, B.M.; Örnek, N.; Zilelioğlu, G.; Elhan, A.H. Morphology of corneal nerves and corneal sensation in dry eye: A preliminary study. Eye 2005, 19, 1276–1279. [Google Scholar] [CrossRef] [PubMed]
- Duan, H.; Yang, T.; Zhou, Y.; Ma, B.; Zhao, L.; Chen, J.; Qi, H. Comparison of mucin levels at the ocular surface of visual display terminal users with and without dry eye disease. BMC Ophthalmol. 2023, 23, 189. [Google Scholar] [CrossRef]
- Verstappen, G.M.; Corneth, O.B.; Bootsma, H.; Kroese, F.G. Th17 cells in primary Sjögren’s syndrome: Pathogenicity and plasticity. J. Autoimmun. 2018, 87, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Vakrakou, A.G.; Polyzos, A.; Kapsogeorgou, E.K.; Thanos, D.; Manoussakis, M.N. Impaired anti-inflammatory activity of PPARγ in the salivary epithelia of Sjögren’s syndrome patients imposed by intrinsic NF-κB activation. J. Autoimmun. 2018, 86, 62–74. [Google Scholar] [CrossRef] [PubMed]
- Iwakura, Y.; Ishigame, H.; Saijo, S.; Nakae, S. Functional specialization of interleukin-17 family members. Immunity 2011, 34, 149–162. [Google Scholar] [CrossRef]
- Fogli, L.K.; Sundrud, M.S.; Goel, S.; Bajwa, S.; Jensen, K.; Derudder, E.; Sun, A.; Coffre, M.; Uyttenhove, C.; Van Snick, J.; et al. T Cell–Derived IL-17 Mediates Epithelial Changes in the Airway and Drives Pulmonary Neutrophilia. J. Immunol. 2013, 191, 3100–3111. [Google Scholar] [CrossRef]
- García-Posadas, L.; Hodges, R.R.; Li, D.; Shatos, M.A.; Storr-Paulsen, T.; Diebold, Y.; Dartt, D.A. Interaction of IFN-γ with cholinergic agonists to modulate rat and human goblet cell function. Mucosal Immunol. 2016, 9, 206–217. [Google Scholar] [CrossRef]
- De Paiva, C.S.; Raince, J.K.; McClellan, A.J.; Shanmugam, K.P.; Pangelinan, S.B.; Volpe, E.A.; Corrales, R.M.; Farley, W.J.; Corry, D.B.; Li, D.-Q.; et al. Homeostatic control of conjunctival mucosal goblet cells by NKT-derived IL-13. Mucosal Immunol. 2011, 4, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Henriksson, J.T.; Coursey, T.G.; Corry, D.B.; De Paiva, C.S.; Pflugfelder, S.C. IL-13 Stimulates Proliferation and Expression of Mucin and Immunomodulatory Genes in Cultured Conjunctival Goblet Cells. Investig. Ophthalmol. Vis. Sci. 2015, 56, 4186–4197. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Forward Primer | Reverse Primer |
|---|---|---|
| MUC1 | 5′-AGCGTGAGTGATGTGCCATT-3′ | 5′-AGCGCAACCAGAACACAGAC-3′ |
| MUC4 | 5′-GGTGGTGGAGGCGTTCTTAT-3′ | 5′-CTCACGTTCAGGGCTGTCAC-3′ |
| MUC16 | 5′-CCAACTCTTCCGAAACAGCA-3′ | 5′-GCCAGTGGCGAGAAGTTACA-3′ |
| GAPDH | 5′-ATGGGGAAGGTGAAGGTC G-3′ | 5′-GGGGTCATTGATGGCAACAATA-3′ |
| IL 17 | 5′-ACCTGAACATCCATAACCGGATAC-3′ | 5′-AGCGTTATGCAGCCCAAG-3′ |
| IL 22 | 5′-TGGGAAAGAAGGGCTGTCAG-3′ | 5′-GCGGTGACCCTGGCA-3′ |
| Parameter | Patients (n = 18) | Controls (n = 15) | p Value |
|---|---|---|---|
| Age (years) | 56.72 ± 11.73 (37–83) | 53.73 ± 11.11 (39–70) | 0.923 |
| Sex (M/F) | 0/18 | 0/15 | |
| OSDI score | 45.20 ± 19.25 *** | 4.395 ± 2.745 | 3.604 × 10−9 |
| TBUT (s) | 3.2 ± 2.6 *** | 13.5 ± 2.0 | 5.401 × 10−26 |
| Oxford Keratopathy Scale | 2.2 ± 1.0 *** | 0.3 ± 0.5 | 2.134 × 10−26 |
| Schirmer I test (mm) | 4.7 ± 4.0 *** | 20 ± 2.8 | 2.744 × 10−13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brossard-Barbosa, N.; Agoglia, M.; Vergara, M.E.; Costa, M.; Cairoli, E.; Freire, T. Possible Correlation between Mucin Gene Expression and Symptoms of Dry Eye Syndrome Secondary to Sjogren’s Disease. J. Clin. Transl. Ophthalmol. 2024, 2, 87-98. https://doi.org/10.3390/jcto2030008
Brossard-Barbosa N, Agoglia M, Vergara ME, Costa M, Cairoli E, Freire T. Possible Correlation between Mucin Gene Expression and Symptoms of Dry Eye Syndrome Secondary to Sjogren’s Disease. Journal of Clinical & Translational Ophthalmology. 2024; 2(3):87-98. https://doi.org/10.3390/jcto2030008
Chicago/Turabian StyleBrossard-Barbosa, Natalie, Matias Agoglia, Maria Elena Vergara, Monique Costa, Ernesto Cairoli, and Teresa Freire. 2024. "Possible Correlation between Mucin Gene Expression and Symptoms of Dry Eye Syndrome Secondary to Sjogren’s Disease" Journal of Clinical & Translational Ophthalmology 2, no. 3: 87-98. https://doi.org/10.3390/jcto2030008