


Hematol. Rep. 2024, 16(2), 295-298; https://doi.org/10.3390/hematolrep16020029 - 9 May 2024
Abstract
►
Show Figures
Heparin products are frequently used in the inpatient setting to prevent and treat venous thromboembolism, but they simultaneously put patients at risk of developing heparin-induced thrombocytopenia (HIT). The 4Ts score determines the pretest probability of HIT. Diagnosis is made with a screening antiplatelet
[...] Read more.
Heparin products are frequently used in the inpatient setting to prevent and treat venous thromboembolism, but they simultaneously put patients at risk of developing heparin-induced thrombocytopenia (HIT). The 4Ts score determines the pretest probability of HIT. Diagnosis is made with a screening antiplatelet factor (PF4) immunoassay and the serotonin-release assay (SRA) as a confirmatory test. Anti-PF4 assays have high sensitivity (98%) but lower specificity (50%) and result in frequent false-positive tests. We present a rare case from our institution of a patient with anti-PF4–Polyanion ELISA-negative, SRA-positive HIT and describe the challenges in making a timely diagnosis in this case.
Full article
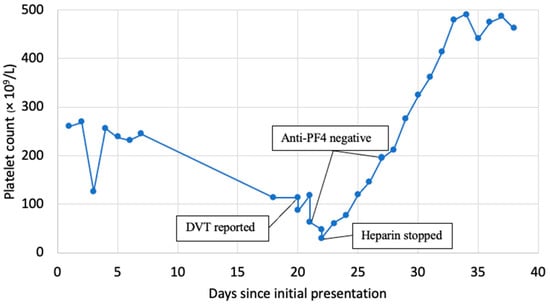
Figure 1






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}