
Survey of WBSNs for Pre-Hospital Assistance: Trends to Maximize the Network Lifetime and Video Transmission Techniques


Abstract
:
1. Introduction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Injury | Rate of Men | Rate of Women | Total Rate |
|---|---|---|---|
| Homicides | 41 | 4.8 | 23.3 |
| Traffic accidents | 22.2 | 6.1 | 14.4 |
| Suicides | 7.8 | 1.9 | 4.9 |
| Falls | 3.2 | 0.8 | 2 |
| Drowning | 3.2 | 0.6 | 1.9 |
| Burns | 0.8 | 0.3 | 0.5 |
| Poisonings | 1.8 | 0.5 | 1.2 |
| Total injuries | 80 | 15 | 48.3 |

Emergency Scenario

2. Literature Review
3. Physiological Signal Monitoring and WBSNs Overall System
3.1. Vital Signs
- Electrocardiography (ECG): An electrical recording of the heart signal to detect anomalies.
- Electroencephalography (EEG): the electrical recording of the brain’s activity.
- Pulse: Measurement of the heart rate, that is, the number of times the heart beats during a determined period.
- Respiratory Rate: Inspiration and expiration activity within a specific time interval.
- Blood pressure: Pressure of the heart pushing blood, to distribute it against arteries resistance.
- Temperature: Measure of the body's ability to generate and get rid of heat.
- Oxygen saturation: Measure of the oxygen levels in the blood.
3.2. Compression of Physiological Signals
3.3. Security on Medical Information
3.4. WBSN
- Continuing and improper communication between devices.
- Housing resources and memory.
- Inefficient use of battery supply.
- Excessive traffic data and other types of information such as video and audio in real time.
- Interference and a large number of retransmissions.
- Inefficient network design that reduce power consumption of each node.
- Energy consumption of sensors according to the measured physiological parameter.
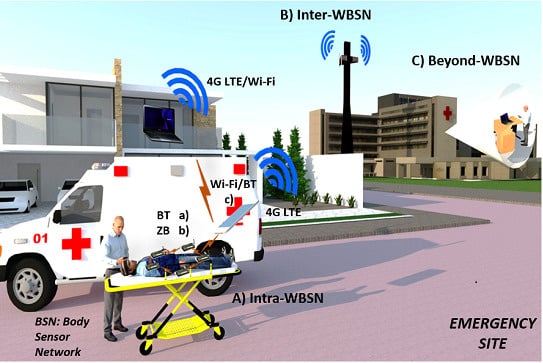
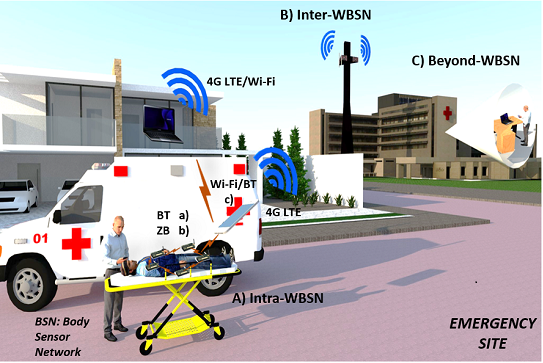
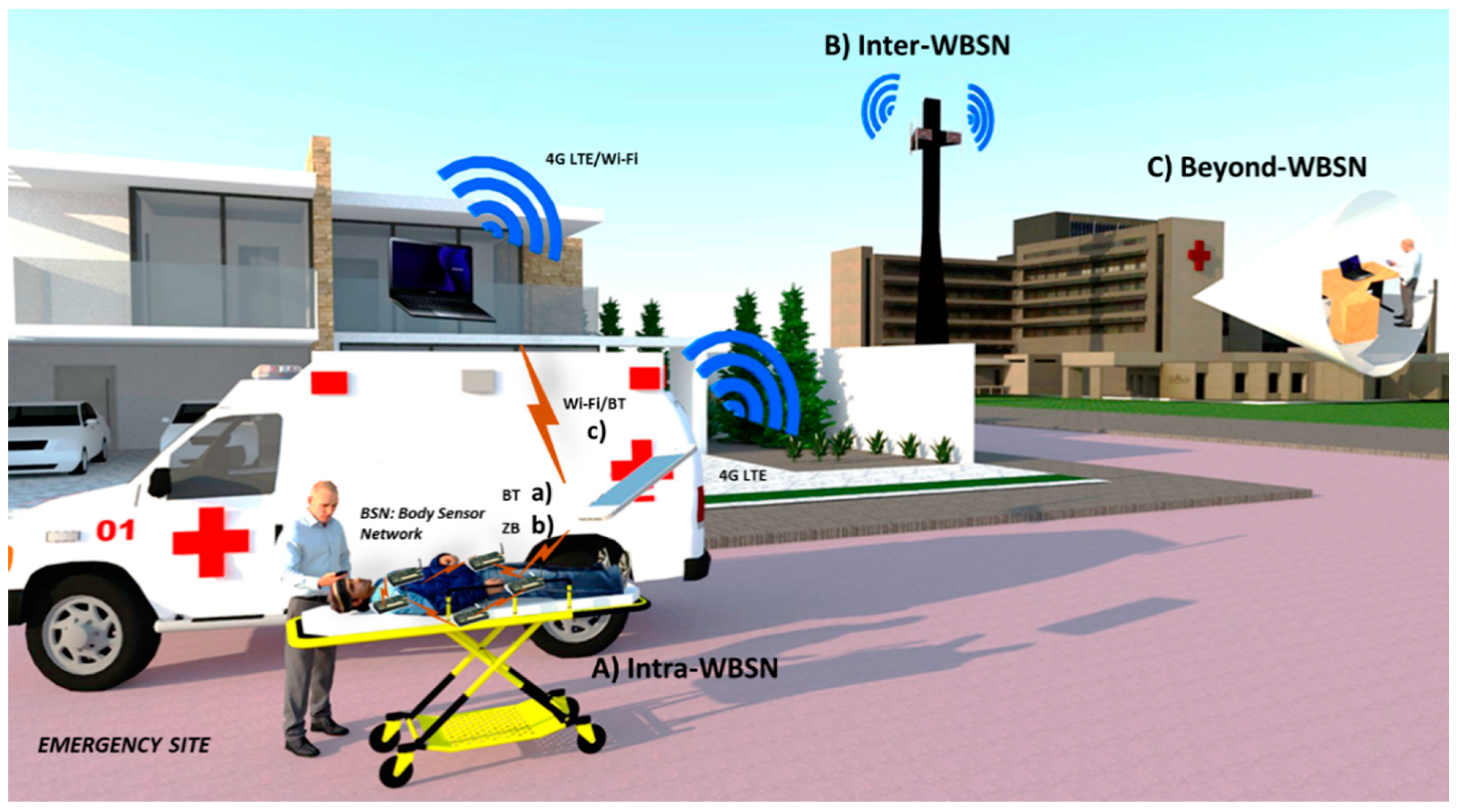
3.5. WBSN System Architecture
- Intra-WBSN Communication: This layer considers communication between sensors and personal servers (usually less than 10 m away). Sensors have a direct wireless communication with PS through ZB or BT (star topology). The PS has capacity to take video of the patient’s condition, and collect and/or compress the physiological signals. The PS can directly transmit the video and physiological data, e.g., via 4G LTE to the second layer, but if the PS do not have this technology, the PS transmits the information to an ambulance via Wi-Fi or BT, and later the ambulance rebroadcasts the information via 4G LTE or Wi-Fi (modem enabled). According to [32], this tier should fulfill some hardware and software requirements. In terms of hardware, sensors must be lightweight, easy to use and comfortable for the patient, with high degree of accuracy. For the software, proper communication protocols, energy efficiency and handling of collected data are important considerations to make. Among these requirements, there are quality standards that must be implemented in the development of the system like: availability of data; usability (wearable or implantable); security/privacy, according to HIPPA; and QoS, for service guarantee.
- Inter-WBSN Communication: This tier corresponds to the communication between the PS to the internet or between PS and one or more RPs and then to the internet. If the signal drops, data could be sent to an RP/PC server (inside the ambulance) and afterwards, the information will be sent wirelessly (Wi-Fi) to the data base server. At this level, a gateway, PDA, PC, or 4G antennas are the link between de Intra-BAN and Beyond-WBSN layers. This tier needs some hardware and software requirements due to the specifications of the device, in terms of developing friendly user interfaces, and collecting and processing efficiently the sensors’ data in real-time [32].
- Beyond-WBSN Communication: This is the final layer which facilitates the real time medical attention. Medical staff could handle through internet video conference or mobile calls an emergency situation of an accident. With the help of a database server, all patient data collected will be stored to create the patient health profile, which could be consulted at any time needed. The inclusion of this tier depends on the application of the platform for a specific situation [32]. Some specifications are needed to implement the data server with respect to high capacity and processing, and should be located in the medical institution.

4. Energy Efficient Protocols, and Scheduling in WBSNs
- ANT+: It is an expanded version of the original ANT protocol to make the devices interoperable in a managed network. It was developed by the sensor company Dynastream in 2004 and it is considered a low power wireless technology. This protocol operates in the 2.4 GHz spectrum. ANT was created with the objective to communicate sports and fitness sensors with a display unit [33], which encourages its application in healthcare and telemedicine areas. Up to 64,000 members could participate in an ANT+ network; in ANT technology, the frequency channel is divided into many communication channels partitioned by time, allowing the sensors to remain in sleep mode for prolonged periods of time achieving important energy savings [34].
- NFC: NFC is for short-range wireless links operating at 13.56 MHz in the high-frequency (HF) band. His range of operation is approximately 4 cm and for this reason and its higher energy consumption compared with other low power wireless technologies (BLE or ANT+), it cannot be considered a direct competitor [34]. NFC involves two devices: an initiator (active) and a target (passive); the initiator actively generates an RF field that can power a passive target. Since passive targets do not require energy source, they can take different forms as tags, stickers, key fobs, or cards. In addition, peer to peer communication is possible, provided that both devices are powered (e.g., data exchange between two smartphones) [35].
- Nike+: It is a wireless technology created by Nike and Apple in 2006, (it will only work with devices of these brands) and operates in the 2.4 GHz spectrum supporting 250 Kbps or 1 Mbps transmission rates [36]. It was developed to monitor user’s physical exercise. Nike+ consists on a sensor attached to the body and a receiver, for example, a wrist band, watch or smartphone.
- ZigBee: It is a low power wireless protocol based on standard 802.15.4.2003, that was developed for applications that need network flexibility, security, high reliability, low cost, and simplicity. It is an ad hoc self-organizing network, and it was created for short range large-scale networks (over 65,000 for a ZigBee star network [37]) with low duty cycle and secure networking, but with smaller throughput needs and for low data rate applications. There are several covering areas for ZigBee such as: home automation, industrial, medicine, smart energy, telecom services, etc. For healthcare, ZigBee provides secure and reliable remote patient monitoring and management, with maintained freedom of mobility [33]. Some medical devices like glucometers, pulse oximeters, electrocardiographs and weight scales support ZigBee protocol.
- Wi-Fi: Wi-Fi is based on the IEEE 802.11 standards, letting users surf the Internet at broadband speeds when connected to an access point (AP) or in ad hoc mode. It is ideally suited for large data transfers, but unfortunately, it needs large batteries [33]. Wireless local area networks provide high-speed wireless connectivity and support information access anytime anywhere, allowing video-conferencing, voice calls, and video streaming. An important advantage is that all smartphones, tablets and laptops have Wi-Fi integrated, and the main disadvantage for Wi-Fi is high energy consumption even if its throughput is reduced.
- Long Term Evolution (4G LTE): 4G LTE is a technology that optimizes communications with transmission speeds of 100 Mbit/s for high mobility and 1 Gbit/s for low mobility. This technology uses transmission with Multiple Input-Multiple Output (MIMO) and Orthogonal Frequency Division Multiplexing (OFDM) techniques, transmitting more data in the same time period. On the negative side, 4G LTE is less power efficient than 3G and Wi-Fi for small data transfers, while for bulk data transfer is more power efficient than 3G [38].
- Bluetooth Low Energy (BLE): BLE was adopted and developed by the Bluetooth Special Interest Group aimed at novel applications in healthcare, fitness, security, and home entertainment industries [39]. The most important fact that guarantees Bluetooth presence in the market is its support by every major operating system. In the latest BLE improvement, a new stack protocol was proposed to offer energy efficiency, latency, piconet size, and throughput parameters. In the medical device area, BLE has the advantage that is implemented in majority of medical devices.
4.1. Energy Efficient Protocols in MAC Layer
| PROTOCOL | BLE | ZIGBEE | WIFI | 4G LTE | ANT+ | NFC | NIKE+ |
|---|---|---|---|---|---|---|---|
| PROS |
|
|
|
|
|
| |
| CONS |
|
|
|
|
|
| |
| STANDARD RANGE [33,35,42] | 1 to 100 m | 10 to 100 m | ~100 m | 1–10 miles | ~30 m | <0.2 m | ~10 m |
| TOPOLOGY [33,34,42] | Star-bus | Mesh, Star, Point to Point | Star, Point to Point. | Ring, Star, chain, mixed. | Peer to Peer, Mesh | Point to Point | Point to Point |
| EFFICIENCY [33] | 0.153 µW/bit | 185.9 µW/bit | 0.00525 µW/bit | 0.011 µW/bit | 0.71 µW/bit | Not specified | 2.48 µW/bit |
| LATENCY [33,39,42] | <3 ms | <5 ms (beaconless mode, at 250 kbps) | 1.5 ms | 10 ms | Zero | Polled typically every second | ~1 s |
| USES FOR WBSNs | Intra-BAN Communication: glucose, Blood pressure, SPO2, Temperature, Heart Rate, ECG, watches and smartphones | Intra-BAN Communication: glucose, Blood pressure, SPO2, Temperature, Heart Rate and ECG. | Inter-BAN and Beyond-BAN Communication: Smartphones, wireless modems, tablets, laptops. | Inter-BAN and Beyond BAN Communication: Smartphones, wireless usb modems, tablets. | Intra-BAN communication: Heart Rate, Temperature, Blood pressure, glucose and smartphones. | Not applications for BAN’s | Intra-BAN communication: Heart Rate, smartphones, wrist bands and watches. |
| PROTOCOLS | MAC OPERATION | ADVANTAGES | DISADVANTAGES | COMMENTS |
|---|---|---|---|---|
| BodyMAC [44] | TDMA | Flexible bandwidth allocation. Nodes and gateway synchronized allowing sleep mode. Good for periodic data sensing and event reporting. | Unsuitable scheme for collision avoidance. | Star topology and MICAz mote specification are used. |
| MEDMAC [45] | ADAPTIVE TDMA | Maximize energy efficiency through dynamical adjustments for QoS requirements. Good for low rate (Class 0) and medium data rate (Class 1) medical applications. | Low performance for high data rate applications. | Star topology. TDMA synchronization. Energy efficiency optimized by dynamically adjusting QoS requirements. |
| NEW IMPROVED LEACH [43] | TDMA/ Clustering | Distributed protocol, control information from the base station is not required. MD node is introduced to allow sleep mode periodically. | Extra overhead for dynamic clustering. | A clustering topology is used. Efficiency is increased 50% than LEACH protocol. |
| POWER EFFICIENT MAC [46] | TDMA/superframe enabled | Better performance in energy saving and delay compared to WiseMAC, ZigBee, B-MAC, and X-MAC protocols Wakeup mechanism enabled to reduce energy consumption with sleep mode. | No existing evaluation for security and QoS parameters. Nodes must wake up to receive the beacon. | Network lifetime is increased thanks to an overhead reduction. Two priorities for traffic: periodic or normal, and random or emergency. |
| HIGHLY RELIABLE ENERGY-SAVING MAC [20] | Distributed Queuing Body Area Network. Superframe is proposed | Qos parameters are considered. A Cross-layer fuzzy logic scheduler is used. By using Energy-aware radio-activation policies, sensors transmit at lowest possible level specified in 802.15.4. | Nodes must wake up to receive the beacon. | Star topology for BSN under two different realistic hospital scenarios. Matlab simulations are carried out using the CC2420 transmitter-receiver. |
| EQ-MAC [47] | Hybrid TDMA and CSMA schemes | Efficient node’s battery usage and support for QoS based on the service differentiation concept (data prioritization traffic levels). | Data redundancy in the sensor network. Low performance for low data rates. High latency without traffic prioritization. | Sensor Simulator is used for large-scale networks. EQ-MAC outperforms Q-MAC and S-MAC protocols. |
- Class 0: Low grade data (e.g., respiratory, pulse and temperature sensor).
- Class 1: Medium grade data (e.g., ECG, EEG, blood pressure, Sp02).
- Class 2: High grade data (video, medical imaging, EMG, capsule endoscope).
4.2. Minimizing Scheduling Conflicts
5. Energy Consumption and System Optimization in WBSNs
| Operation | Energy Consumption |
|---|---|
| Data sensing | = |
| Data register | = |
| TX and RX | = |
| State shifting | = |
5.1. Constraints
5.2. Cost Function
6. Video Technology in M-Health Systems
6.1. Video and Physiological Data Platforms
6.2. Video and Physiological Signal Synchronization
7. Discussion and Open Research Issues
- Scheduling: Design a transmission scheduling for the WBSN in relation to the transfer rate of each vital sign. Characteristics of a model in monitoring and data transmission must be provided. We know that sampling frequency of each sensor, required bandwidth and amount of data are very particular according to the vital sign measured.
- Adaptability: A WBSN must be dynamic and adaptive. Each patient according to his/her condition, shall imply different priorities in terms of the energy consumption, the collection and transmission of data from each sensor.
- Communication: wireless communication is an important factor to evaluate. Each sensor can communicate wirelessly with other sensors or with the base station, however, there are factors that can influence this communication to be successful to optimize energy consumption:
- a)
- Collisions if two sensors try to transmit at the same time (inefficient communication).
- b)
- Retransmissions caused by collisions or loss of information with direct impact on the energy consumption.
- c)
- Mobility of patient: when a patient is moving within different areas in a hospital (Emergency room, laboratory, X-ray, etc.) data loss or retransmissions could occur if protocol is not designed with mobility support.
- d)
- External factors such as a monitoring environment with heavy traffic information (external devices are transmitting information) or geographic areas that prevent proper communication between network devices.
- e)
- The need to guarantee access to the transmission channel for each sensor according to the priority that involves each of the scenarios for monitoring.
- Quality of service: It is of utmost importance in the monitoring and vital sign transmission; data must be available at the right time, without errors and in real time, so reliability of the network is not affected.
- Security: The security and privacy of patient-related data are two relevant components for the system security of the WBSN. By data security, it means the protection of information from unauthorized users while data being stored and transferred and data privacy means right of individuals to control the collection and use of personal information. Security and privacy issues are raised automatically when the data is created, transferred, stored and processed. The Health Insurance Portability and Accountability Act (HIPAA) mandates that, as the sensors in WBSN collect the wearer’s health data (which is regarded as personal information), care needs to be taken to protect it from unauthorized access and tampering [27].
- Critical time parameters: For diagnosis, it is very important that health data (vital signs) of patients arrive within the expected time to accurately indicate the actual health condition of the patient. Delay, packet errors, and packet losses are some factors that could alter the correct medical diagnosis. If one of the vital sign parameters gets lost, arrives with delay or in a different time slot, a critical condition could be ignored. So, these factors are needed to evaluate a WBSNs through critical time parameters [60].
8. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Estadísticas sanitarias mundiales 2012. Organización mundial de la salud (WorldHealthOrganization). Available online: http://www.who.int/gho/publications/world_health_statistics/ES_WHS2012_Full.pdf (accessed on 16 February 2014).
- Población. Esperanza de vida. Available online: http://cuentame.inegi.org.mx/poblacion/esperanza.aspx?tema=P (accessed on 16 February 2014).
- The graying of America. Available online: http://thesocietypages.org/socimages/2010/03/08/the-graying-of-americ (accessed on 16 February 2014).
- Rendición de cuentas en salud 2011. Available online: http://dgdif.salud.gob.mx/pdf/cuentas2011.pdf (accessed on 16 February 2014).
- ERPHA. Latin America and Caribbean Collaborative ICT Research. Available online: http://www.laccir.org/sites/r1209lac001/Project.aspx (accessed on 16 February 2014).
- Istepanian, R.S.H.; Jovanov, E.; Zhang, Y.T. Guest editorial introduction to the special section on m-health: Beyond seamless mobility and global wireless health-care connectivity. IEEE Trans. Inf. Technol. Biomed. 2004, 8, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Aquino-Santos, R.; González Potes, A.; Rangel-Licea, V.; García-Ruiz, M.A.; Villaseñor-González, L.A.; Edwards-Block, A. Wireless communication protocol based on EDF for wireless body sensor networks. J. Appl. Res. Technol. 2008, 6, 120–128. [Google Scholar]
- Amisha, N.; Kumar, S. A secure health care management system. Int. J. Adv. Res. Comput. Sci. Technol. 2014, 2, 31–35. [Google Scholar]
- Lu, X.; Chen, X.; Li, Y.; Jin, D.; Zhang, L.; Rashvand, H.F. ZebraBAN: A heterogeneous high-performance energy efficient wireless body sensor network. IET Wirel. Sens. Syst. J. 2013, 3, 247–254. [Google Scholar] [CrossRef]
- Crosby, G.V.; Ghosh, T.; Murimi, R.; Chin, C.A. Wireless body area network for healthcare: A survey. Int. J. Ad hoc Sens. Ubiquitous Comput. 2012, 3. [Google Scholar] [CrossRef]
- Micek, J.; Kochlan, M. Energy-efficient Communication Systems of Wireless Sensor Networks. Stud. Inform. Universalis 2014, 11, 69–86. [Google Scholar]
- Latré, B.; Braem, B.; Moerman, I.; Blondia, C. A survey on wireless body area networks. J. Wirel. Netw. 2011, 17, 1–18. [Google Scholar] [CrossRef]
- Chen, M.; Gonzalez, S.; Vasilakos, A.; Cao, H.; Leung, V.C.M. Body area networks: A survey. Mob. Netw. Appl. 2011, 16, 171–193. [Google Scholar] [CrossRef]
- Bangas, J.I.; Abdullah, A.H.; Anisi, M.H.; Khan, A.W. A survey of routing protocols in wireless body sensor networks. Sensors 2014, 14, 1322–1357. [Google Scholar] [CrossRef] [PubMed]
- Cao, H.; Leung, V.; Chow, C.; Chan, H. Enabling technologies for wireless body area networks: A survey and outlook. IEEE Commun. Mag. 2009, 47, 84–93. [Google Scholar] [CrossRef]
- Movassaghi, S.; Abolhasan, M.; Lipman, J.; Smith, D.; Jamalipour, A. Wireless body area networks: A survey. IEEE Commun. Surv. Tutor. 2013, 1–29. [Google Scholar]
- Ko, J.; Lim, J.H.; Chen, Y.; Musaloiu-E., R.; Terzis, A.; Masson, G.M.; Gao, T.; Destler, W.; Selavo, L.; Dutton, R.P. MEDISN: Medical Emergency Detection in Sensor Networks. ACM Trans. Embed. Comput. Syst. (TECS) 2010, 10. [Google Scholar] [CrossRef]
- Halgamuge, M.N.; Zukerman, M.; Ramamohanarao, K. An estimation of sensor energy consumption. Prog. Electromagn. Res. B 2009, 12, 259–295. [Google Scholar] [CrossRef]
- Chen, S.-L.; Lee, H.-Y.; Chen, C.-A.; Huang, H.-Y.; Luo, C.-H. Wireless body sensor network with adaptive low-power design for biometrics and healthcare applications. IEEE Syst. J. 2009, 3, 398–409. [Google Scholar] [CrossRef]
- Otal, B.; Alonso, L.; Verikoukis, C. Highly reliable energy-saving MAC for wireless body sensor networks in healthcare systems. IEEE J. Sel. Areas Commun. 2009, 27, 553–565. [Google Scholar] [CrossRef]
- Pourmohseni, B.; Eshghi, M. Reliable Energy-Efficient Dynamic-TDMA MAC Protocol for Wireless Body Area Networks. Int. J. Appl. Innov. Eng. Manag. 2013, 2, 393–402. [Google Scholar]
- Silva Thotahewa, K.; Redoute, J.M.; Yuce, R.M. MAC Protocols for UWB-Based WBAN Applications. In Ultra Wideband Wireless Body Area Networks; Springer International Publishing: Cham, Switzerland, 2014; pp. 19–35. [Google Scholar]
- Kimura, N.; Latifi, S. A survey on data compression in wireless sensor networks. In Proceedings of the International Conference on Information Technology: Coding and Computing, Las Vegas, NV, USA, 4–6 April 2005; pp. 8–13.
- Agarwal, R.; Sonkusale, S.R. Input-feature correlated asynchronous analog to information converter for ECG monitoring. IEEE Trans. Biomed. Circuits Syst. 2011, 5, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Zarei, S.; Farokhi, F. Data reduction in body sensor networks using wavelet principal components analysis. In Proceedings of 2011 International Conference on Intelligent Computation and Bio-Medical Instrumentation (ICBMI), Wuhan, China, 14–17 December 2011; pp. 183–187.
- Pesovic, U.; Randic, S.; Stamenkovic, Z. A wireless ECG sensor node based on huffman data encoder. In Proceedings of IEEE 14th International Symposium on Design and Diagnostics of Electronic Circuits & Systems (DDECS), Cottbus, Germany, 13–15 April 2011; pp. 411–412.
- Scholl, M.A.; Stine, K.M.; Hash, J.; Bowen, P.; Johnson, L.A.; Smith, C.D.; Steinberg, D.I. An Introductory Resource Guide for Implementing the Health Insurance Portability and Accountability Act (HIPAA) Security Rule; Tech. Rep. SP-800-66 Rev. 1; NIST: Gaithersburg, MD, USA, October 2008. [Google Scholar]
- Ramli, S.N.; Ahmad, R. Surveying the wireless body area network in the realm of wireless communication. In Proceedings of 7th International Conference on Information Assurance and Security (IAS), Melaka, Malaysia, 5–8 December 2011; pp. 58–61.
- Jovanov, E.; Price, J.; Raskovic, D.; Kavi, K.; Martin, T.; Adhami, R. Wireless Personal Area Network in Telemedical Environment. In Proceedings of the 2000 IEEE EMBS International Conference on Information Technology Applications in Biomedicine, Arlington, VA, USA, 9–10 November 2000; pp. 22–27.
- Chu, Y.; Ganz, A. WISTA: A wireless transmission system for disaster patient care. Mob. Network Appl. J. 2007, 12, 201–214. [Google Scholar] [CrossRef]
- Tarannum, S. Energy Conservation Challenges in Wireless Sensor Network: A Comprehensive Study. Wirel. Sens. Netw. J. 2010, 2, 483–491. [Google Scholar] [CrossRef]
- Bandar, A; Fouchal, H. A mobile wireless body area network platform. J. Comput. Sci. 2014, 5, 664–674. [Google Scholar] [CrossRef]
- Smith, P. Comparing Low-Power Wireless Technologies; Tech. Rep. CS-213199-AN; CSR PLC: Cambridge, UK, 24 May 2001. [Google Scholar]
- Hong, L. Wearables-Smart protocols for smart technology. M2M J. 2014, 22, 16–17. [Google Scholar]
- Neeraj, C. Comparative Analysis of Different Wireless Technologies. Int. J. Sci. Res. Netw. Secur. Commun. 2013, 5, 13–17. [Google Scholar]
- Nike+iPod reverse engineering. Available online: http://dmitry.gr/index.php?r=05.Projects&proj=05.%20Nike%20plus%20iPod (accessed on 28 March 2015).
- Vivek, N.K. Comparative Analysis and Interpretation of Various Short-Range Wireless Technologies. Int. J. Sci. Eng. Res. 2012, 3, 1–5. [Google Scholar]
- Huang, J.; Qian, F.; Gerber, A.; Mao, Z.M.; Sen, S.; Spatscheck, O. A close examination of performance and power characteristics of 4G LTE networks. In Proceedings of the 10th International Conference on Mobile Systems, Applications, and Services, Low Wood Bay, UK, 25–29 June 2012; pp. 225–238.
- Gomez, C.; Oller, J.; Paradells, Josep. Overview and Evaluation of Bluetooth Low Energy: An Emerging Low-Power Wireless Technology. Sens. J. 2012, 12, 11734–11753. [Google Scholar] [CrossRef]
- Otal, B.; Alonso, L.; Verikoukis, C. Energy-efficiency analysis of a distributed queuing medium access control protocol for biomedical wireless sensor networks in saturation conditions. Sensors 2011, 11, 1277–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suhonen, J.; Kohvakka, M.; Kaseva, V.; Hamalainen, T.D.; Hannikainen, M. Low-Power Wireless Sensor Network Platforms. In Handbook of Signal Processing Systems; Springer: New York, NY, USA, 2010; pp. 123–160. [Google Scholar]
- Rohan, T.; Adel, B.M.; Farid, T.; Abdulaziz, M.G. A Comparative Analysis of BLE and 6LoWPAN for U-HealthCare Applications. In Proceeding of IEEE GCC Conference and Exhibition, Doha, Qatar, 17–20 November 2013; pp. 286–291.
- Yassein, M.B.; Mistareehi, H. Improvement on the lifetime of the WSN using energy efficiency saving of leach protocol. Sens. Transducers J. 2011, 130, 142–154. [Google Scholar]
- Fang, G.; Dutkiewicz, E. BodyMAC: Energy efficient TDMA-based MAC protocol for wireless body area networks. In Proceedings of 9th International Symposium on Communications and Information Technology, Icheon, Korea, 28–30 September 2009; pp. 1455–1459.
- Timmons, N.F.; Scanlon, W.G. An adaptive energy efficient mac protocol for the medical body area network. In Proceedings of 1st International Conference on Wireless Communication, Vehicular Technology, Information Theory and Aerospace & Electronic Systems Technology, Aalborg, the Netherlands, 17–20 May 2009; pp. 587–593.
- Al Ameen, M.; Ullah, N.; Chowdhury, M.S.; Islam, S.R.; Kwak, K. A power efficient mac protocol for wireless body area networks. EURASIP J. Wirel. Commun. Netw. 2012, 2012. [Google Scholar] [CrossRef]
- Yahya, B.; Ben-Othman, J. Energy efficient and QoS aware medium access control for wireless sensor networks. Concurrency Comput. Pract. Exper. 2010, 22, 1252–1266. [Google Scholar] [CrossRef]
- Bernard, T.; Fouchal, H. Slot scheduling for wireless sensor networks. J. Comput. Methods Sci. Eng. 2012, 12, 1–12. [Google Scholar]
- Nabar, S.; Walling, J.; Poovendran, R. Minimizing energy consumption in body sensor networks via convex optimization. In Proceedings of International Conference on Body Sensor Networks (BSN), Singapore, 7–9 June 2010; pp. 62–67.
- Kyriacou, E.; Pattichis, M.S.; Pattichis, C.S.; Panayides, A.; Pitsillides, A. M-health e-emergency systems: Current status and future directions. IEEE Antennas Propag. Mag. 2007, 49, 216–231. [Google Scholar]
- Skorin-Kapov, L.; Matijasevic, M. Analysis of QoS requirements for e-health services and mapping to evolved packet system QoS classes. Int. J. Telemed. Appl. 2010, 2010. [Google Scholar] [CrossRef]
- Richardson, I. The H.264 Advanced Video Compression Standard, 2nd ed.; Wiley: West Sussex, UK, 2010; pp. 81–98. [Google Scholar]
- Kim, Y.-H.; Lim, I.L.; Lee, J.-K. Efficient remote medical support system design on using H.264/AVC. In Proceedings of the 5th International Conference on Ubiquitous Information Technologies and Applications (CUTE), Sanya, China, 16–18 December 2010; pp. 1–6.
- Rivera-Rodríguez, R.; Serrano-Santoyo, A.; Tamayo-Fernández, R.; Armenta-Ramade, A. Sistema móvil de teleasistencia médica para la atención en tiempo real de casos de urgencia. Ing. Investig. Technol. 2012, 13, 1–8. [Google Scholar]
- Gallego, J.R.; Hernandez-Solana, A.; Canales, M.; Lafuente, J.; Valdovinos, A.; Fernandez-Navajas, J. Performance analysis of multiplexed medical data transmission for mobile emergency care over the umts channel. IEEE Trans. Inf. Technol. Biomed. 2005, 9, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Vouyioukas, D.; Maglogiannis, I.; Komnakos, D. Emergency m-health services through high-speed 3G systems: Simulation and performance evaluation. Simulation 2007, 83, 329–345. [Google Scholar] [CrossRef]
- Weinger, M.B.; Gonzales, D.C.; Slagle, J.; Syeed, M. Video capture of clinical care to enhance patient safety. Qual. Saf. Health Care 2004, 13, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Banno, K.; Kryger, M.H. Use of polysomnography with synchronized digital video recording to diagnose pediatric sleep breathing disorders. Can. Med. Assoc. J. 2005, 173, 28–30. [Google Scholar] [CrossRef]
- Bhattacharyya, S.; Roy, A.; Dogra, D.P.; Biswas, A.; Mukherjee, J.; Majumdar, A.K.; Majumdar, B.; Mukherjee, S.; Singh, A.K. Summarization of neonatal video EEG for seizure and artifact detection. In Proceedings of 3th National Conference on Computer Vision, Pattern Recognition, Image Processing and Graphics (NCVPRIPG), Hubli, Karnataka, 15–17 December 2011; pp. 134–137.
- Balasubramanian, V. Critical time parameters for evaluation of Body Area Wireless Sensor Networks in a Healthcare Monitoring Application. In Proceedings of IEEE Ninth International Conference on Intelligent Sensors, Sensors Networks and Information Processing, Singapore, 21–24 April 2014; pp. 1–6.
- Xiaoyin, Q.; Mianshu, C.; Hexin, C. A CAVLC embedded method for audio-video synchronization coding based on H.264. In Proceedings of International Conference on Multimedia Technology (ICMT), Hangzhou, China, 26–28 July 2011; pp. 16–19.
- Li, X.; Chen, H.; Wang, D.; Qi, X. Audio-video synchronous coding based on mode selection in H.264. In Proceedings of 4th International Congress on Image and Signal Processing (CISP), Shanghai, China, 15–17 October 2011; pp. 113–117.
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzalez, E.; Peña, R.; Vargas-Rosales, C.; Avila, A.; De Cerio, D.P.-D. Survey of WBSNs for Pre-Hospital Assistance: Trends to Maximize the Network Lifetime and Video Transmission Techniques. Sensors 2015, 15, 11993-12021. https://doi.org/10.3390/s150511993
Gonzalez E, Peña R, Vargas-Rosales C, Avila A, De Cerio DP-D. Survey of WBSNs for Pre-Hospital Assistance: Trends to Maximize the Network Lifetime and Video Transmission Techniques. Sensors. 2015; 15(5):11993-12021. https://doi.org/10.3390/s150511993
Chicago/Turabian StyleGonzalez, Enrique, Raul Peña, Cesar Vargas-Rosales, Alfonso Avila, and David Perez-Diaz De Cerio. 2015. "Survey of WBSNs for Pre-Hospital Assistance: Trends to Maximize the Network Lifetime and Video Transmission Techniques" Sensors 15, no. 5: 11993-12021. https://doi.org/10.3390/s150511993