
Development of Portable Digital Radiography System with a Device for Monitoring X-ray Source-Detector Angle and Its Application in Chest Imaging

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
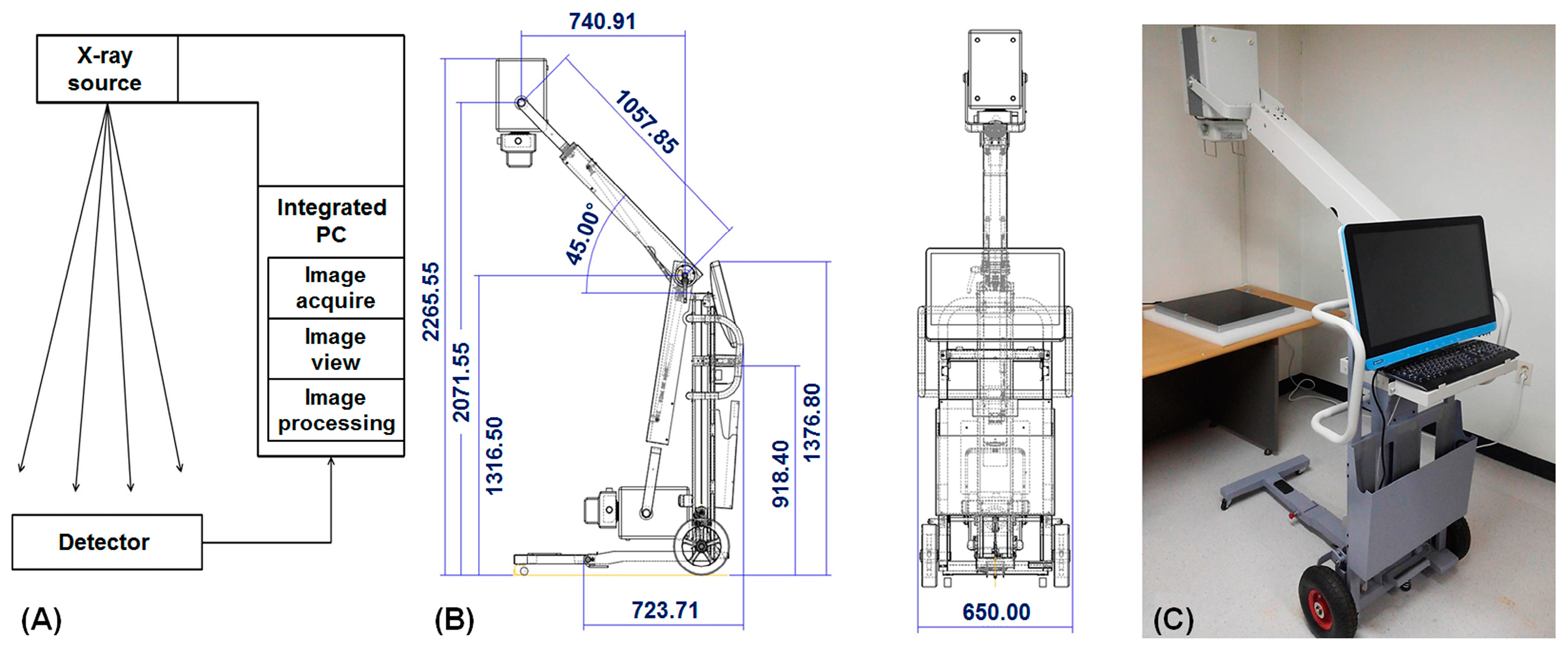
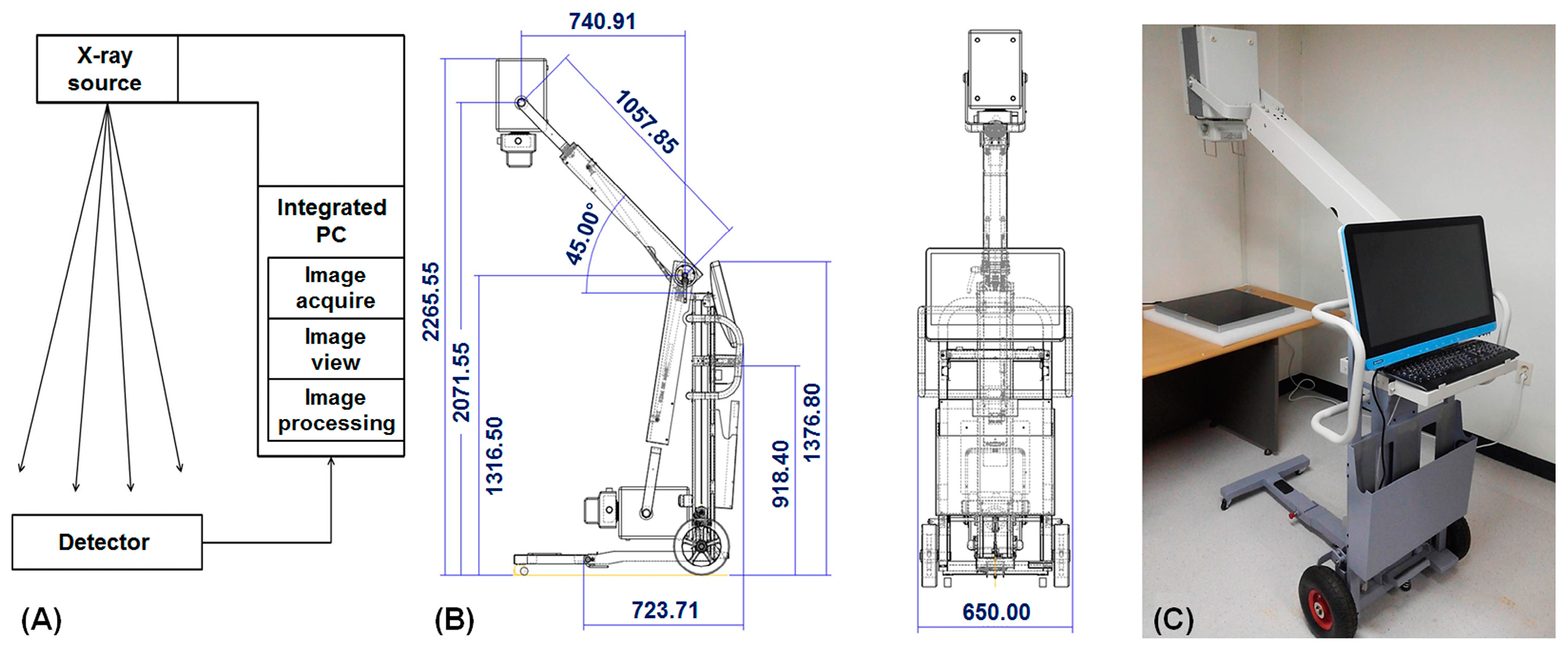
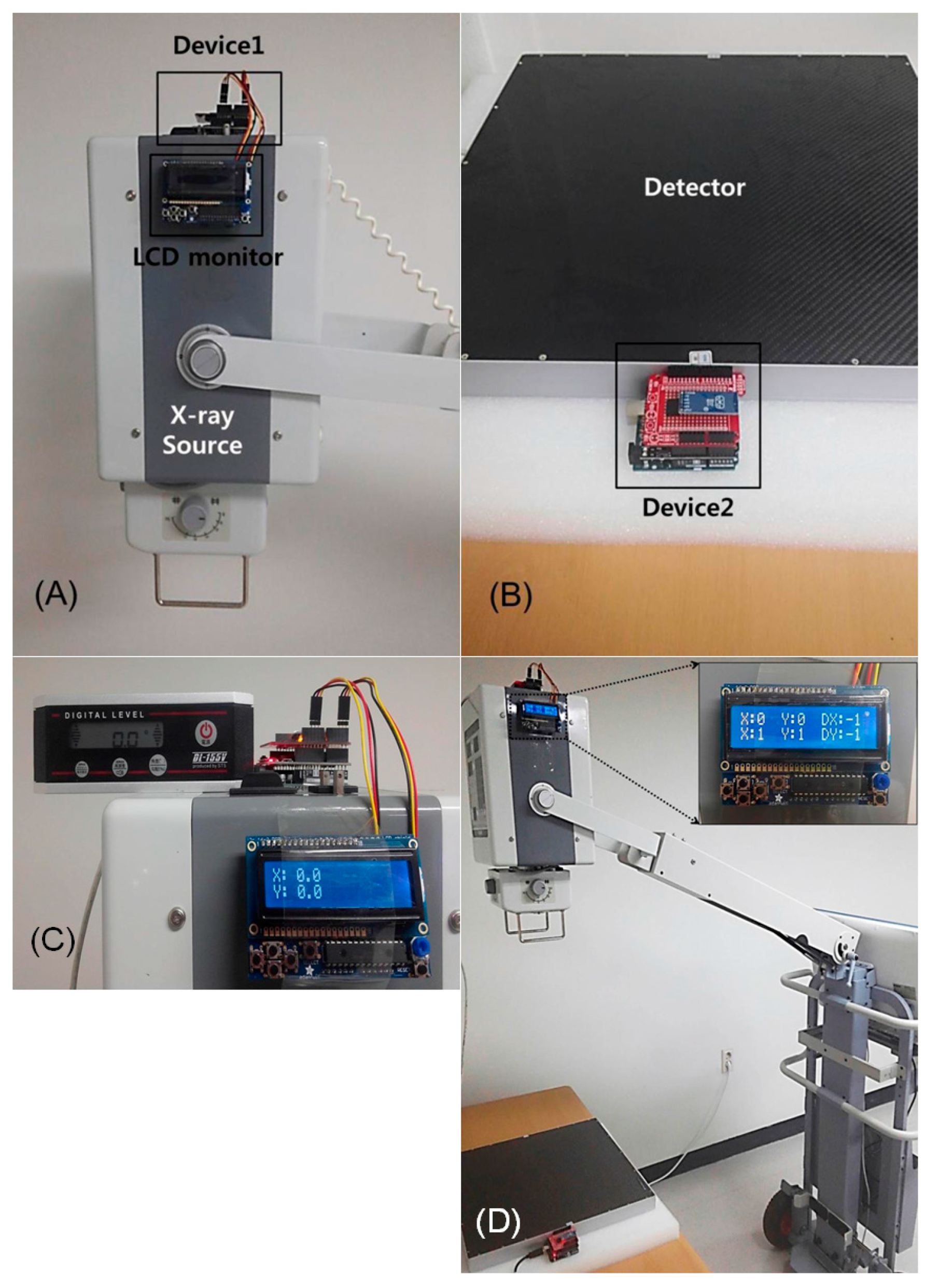
2.1. Portable Digital Radiography System
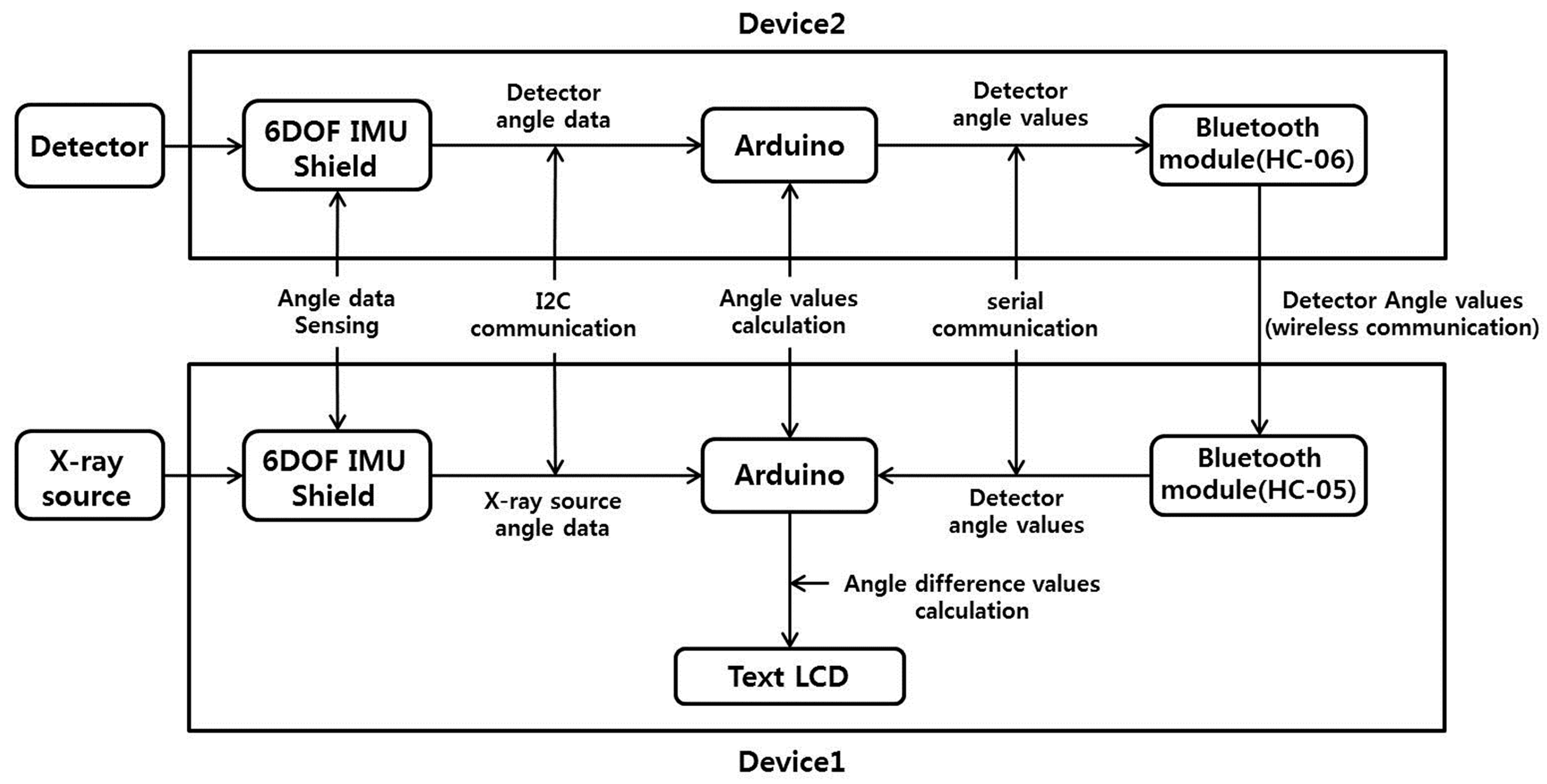
2.2. Internal Processing of Portable Digital Radiography
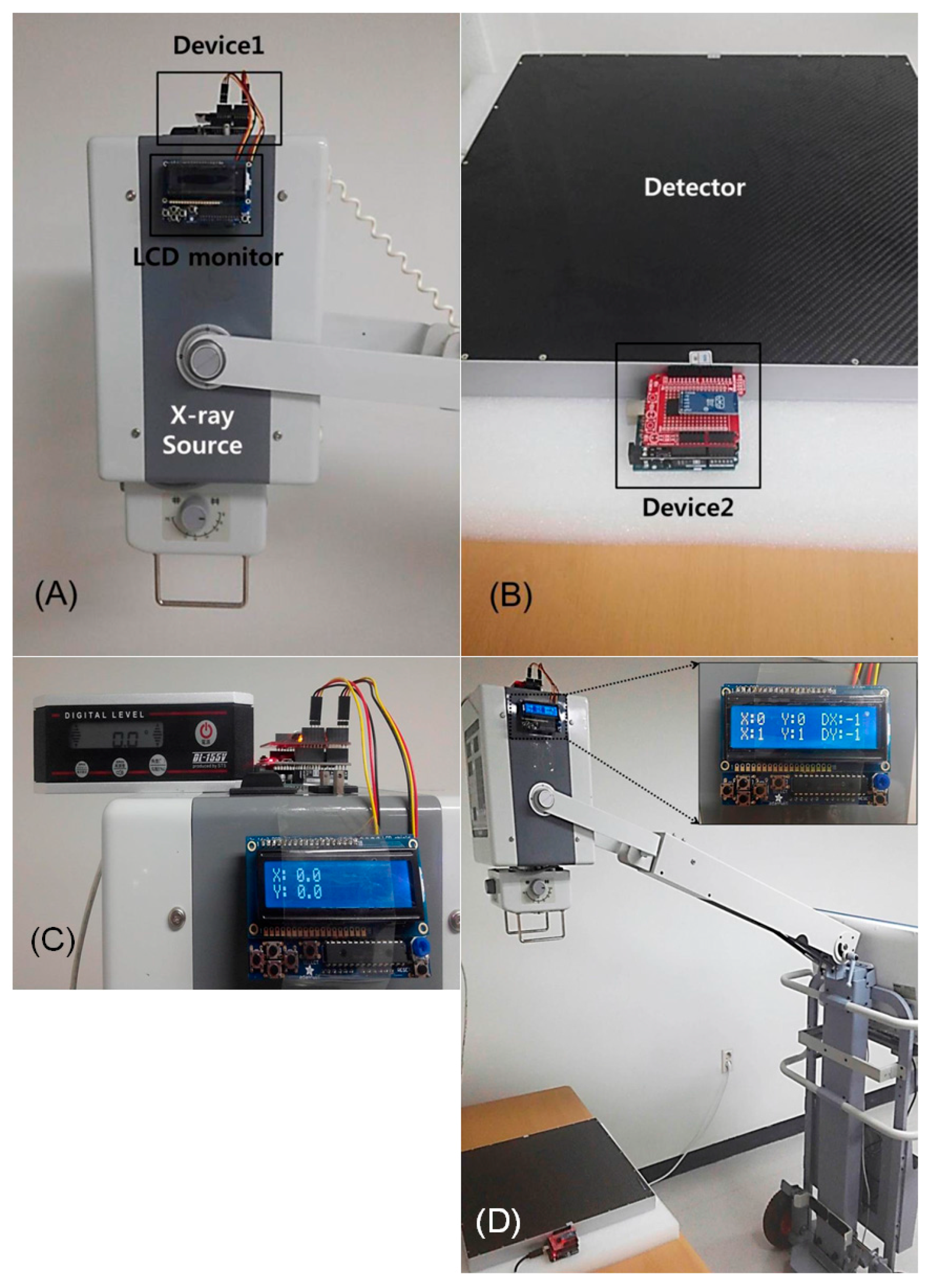
2.3. Development and Performance Test of X-ray SDA Device
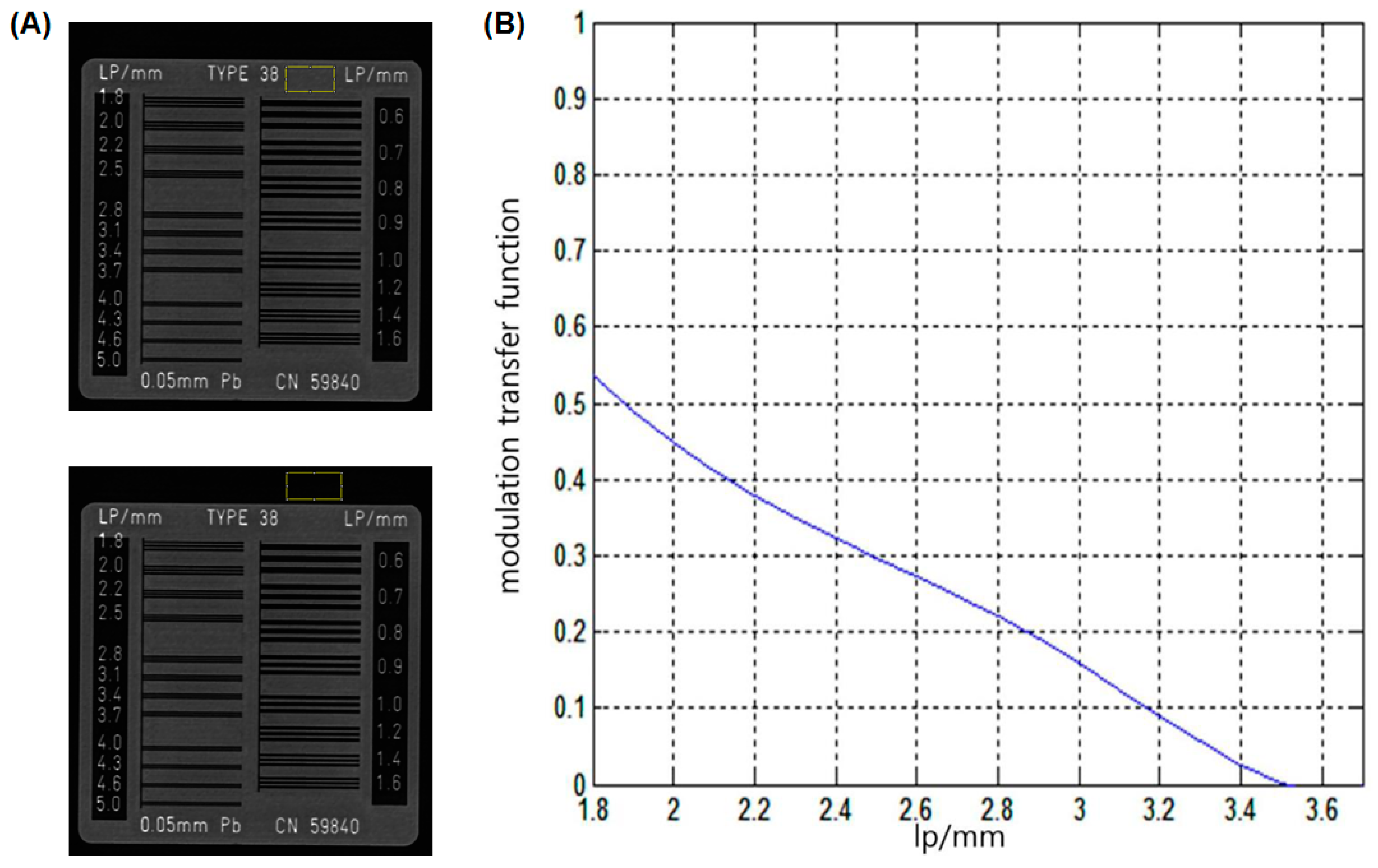
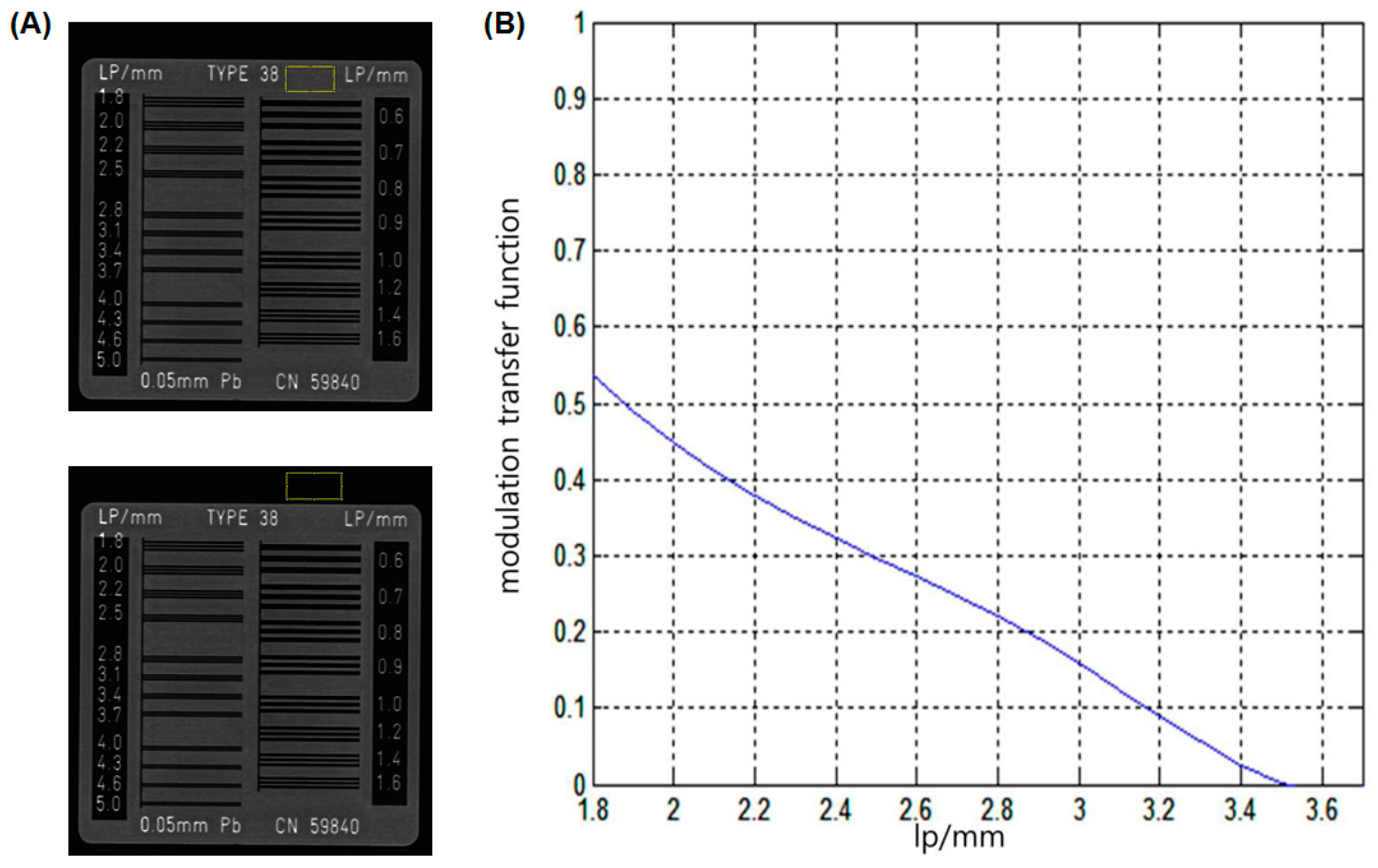
2.4. Measurements of Image Quality and Radiation Dose
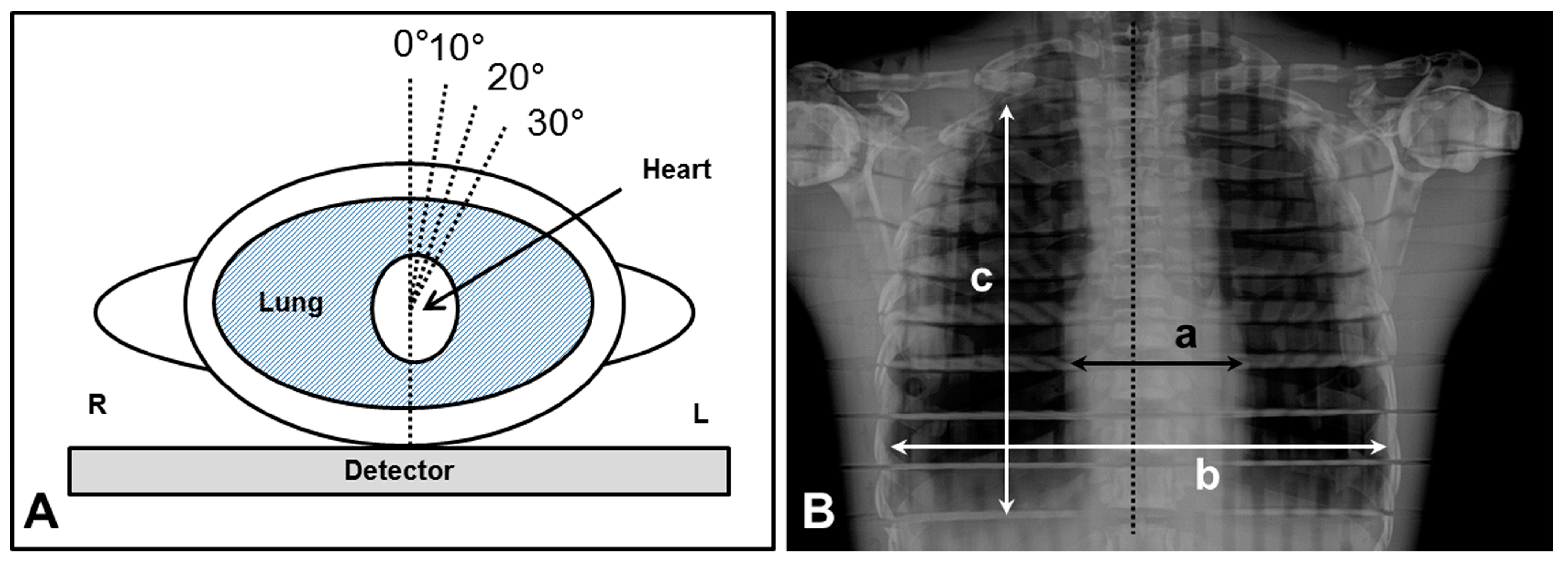
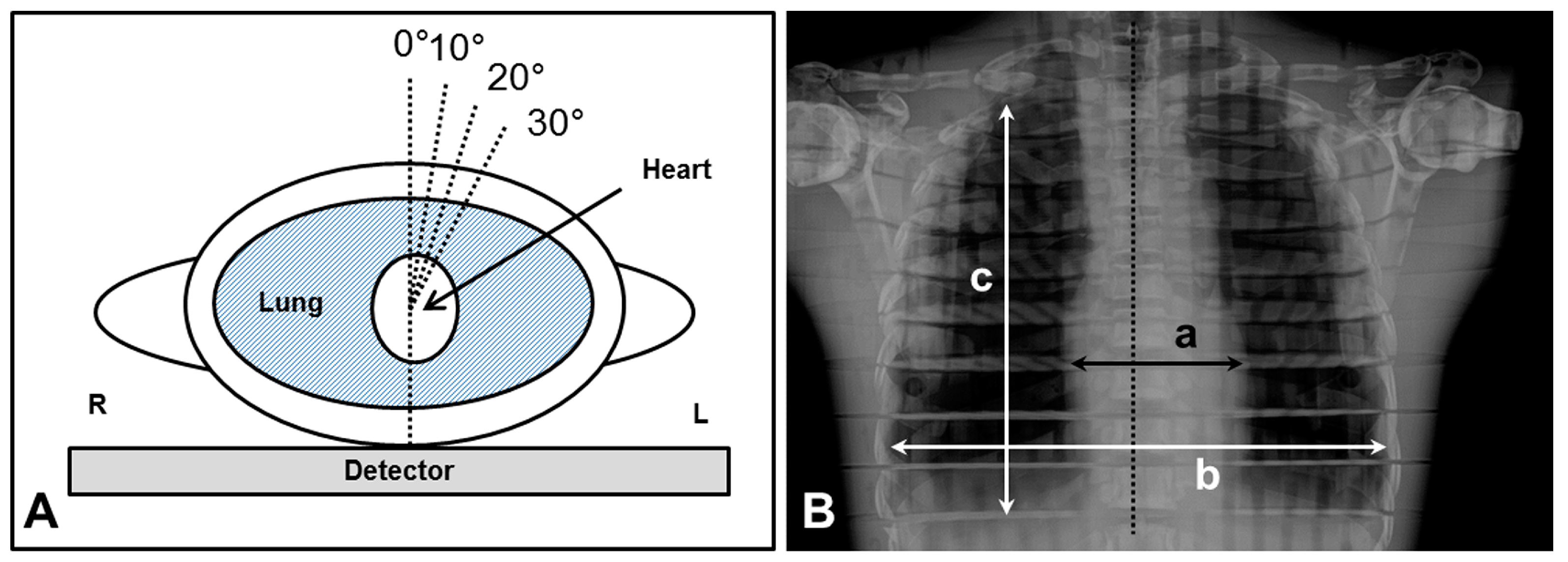
2.5. Chest Radiography According to Different Angle Degrees
2.6. Statistical Analysis
3. Results
3.1. Development and Performances of PDR
3.2. Performance of the SDA Device
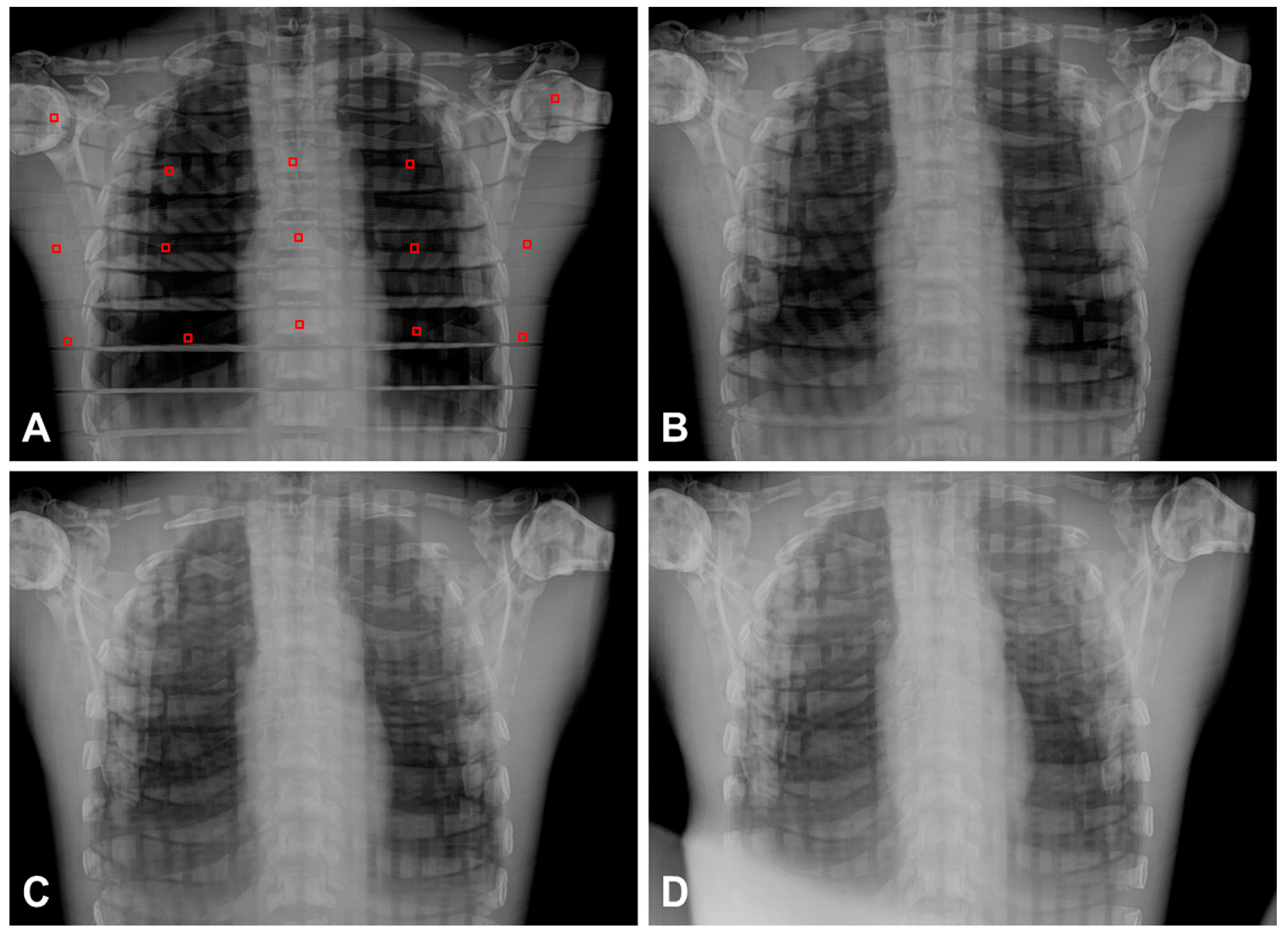
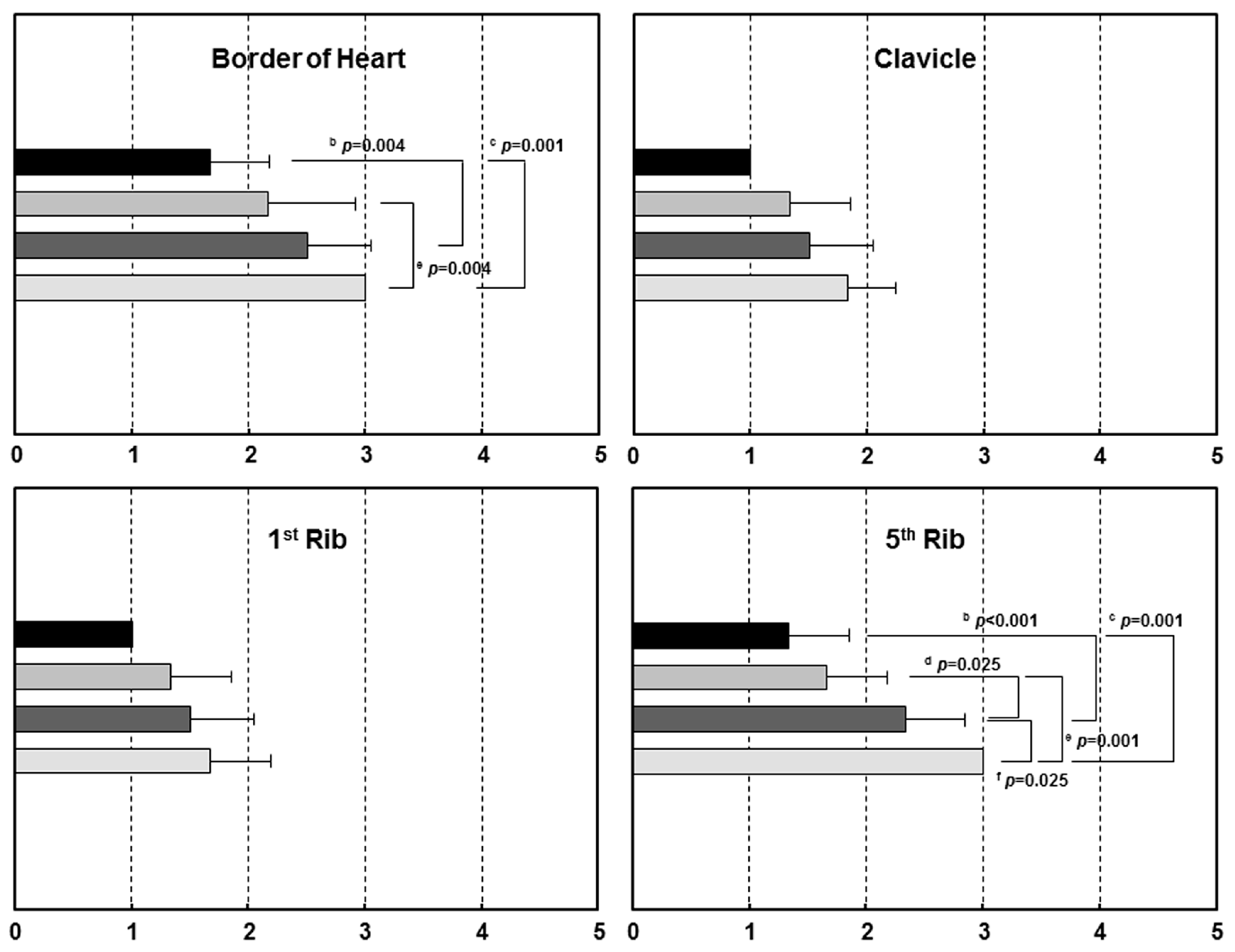
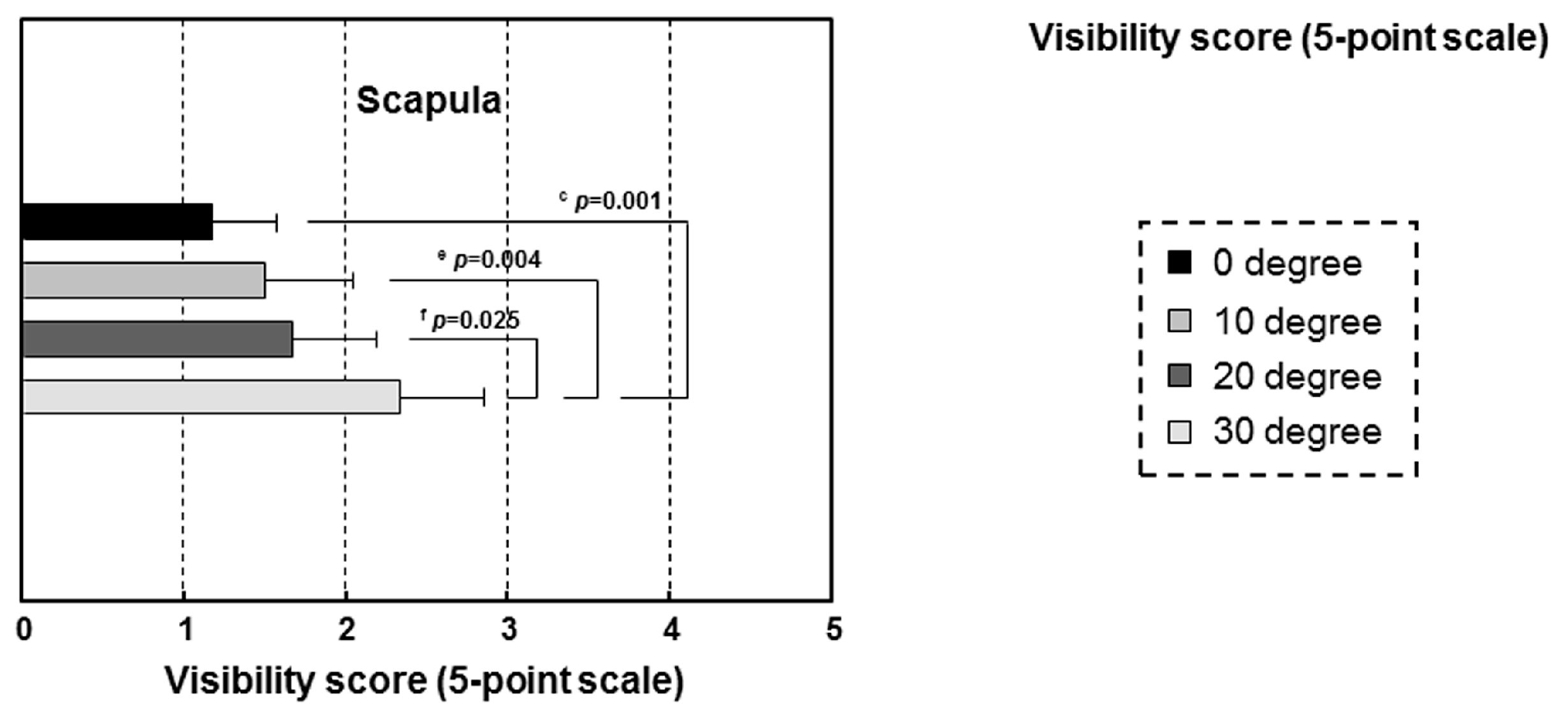
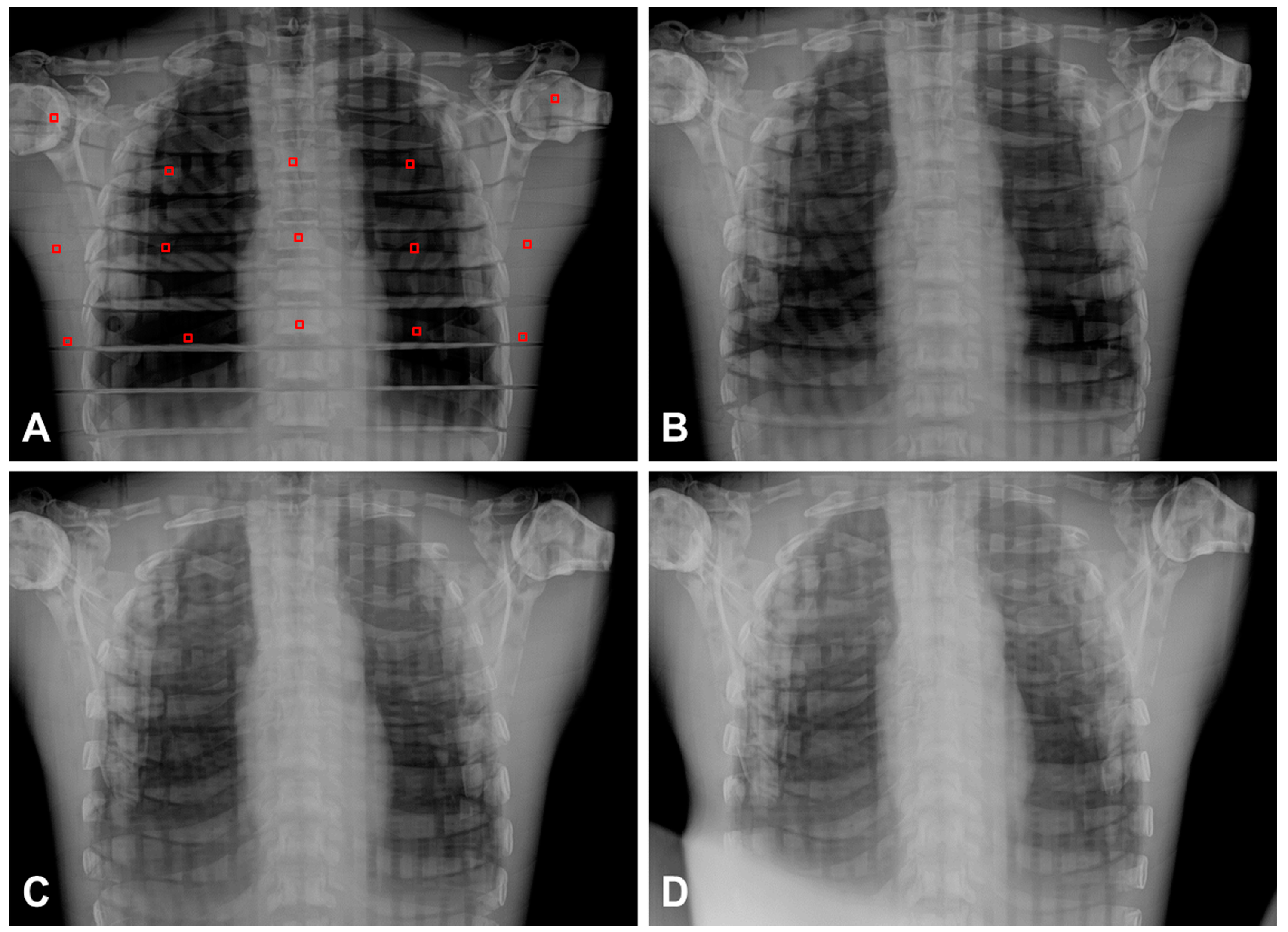
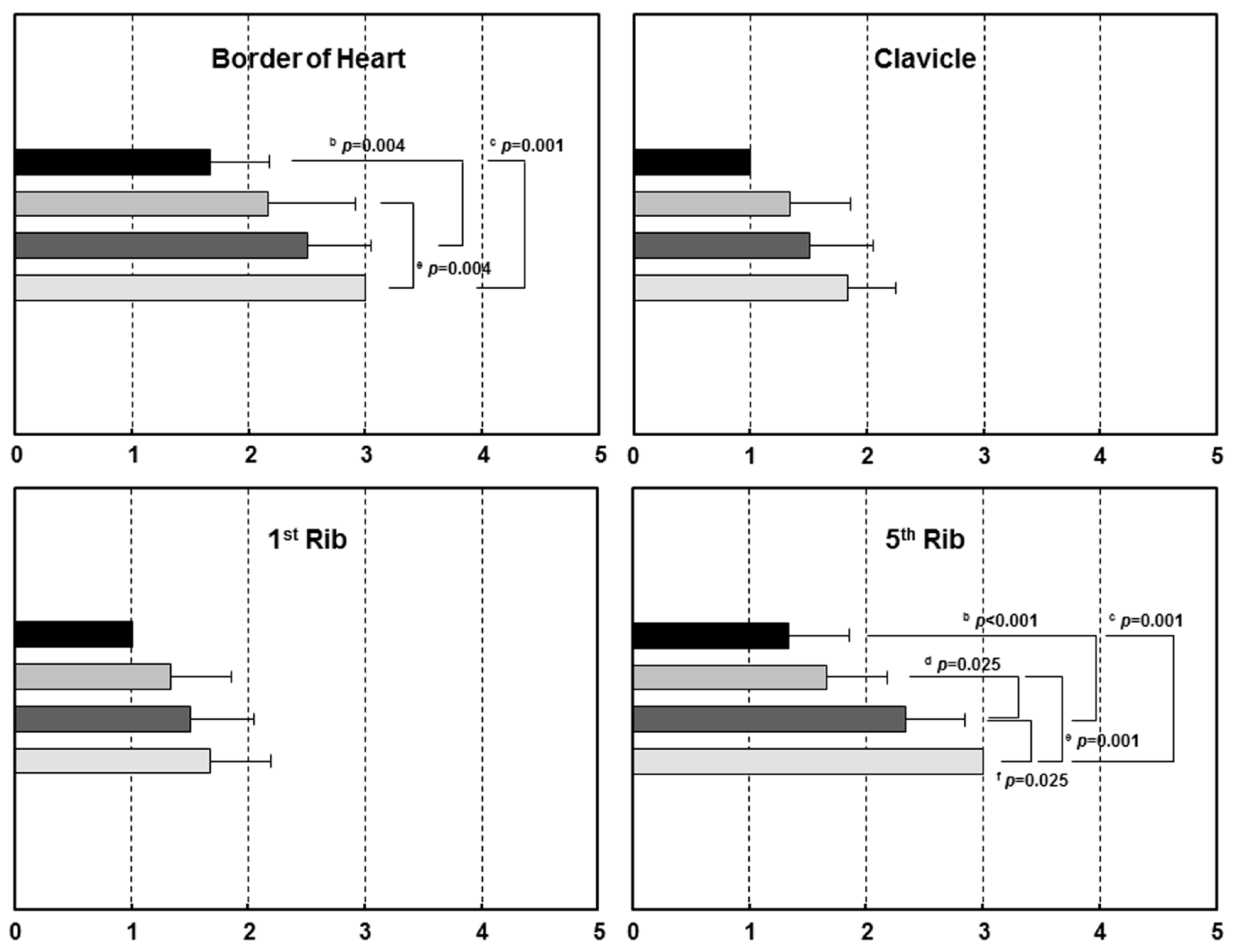
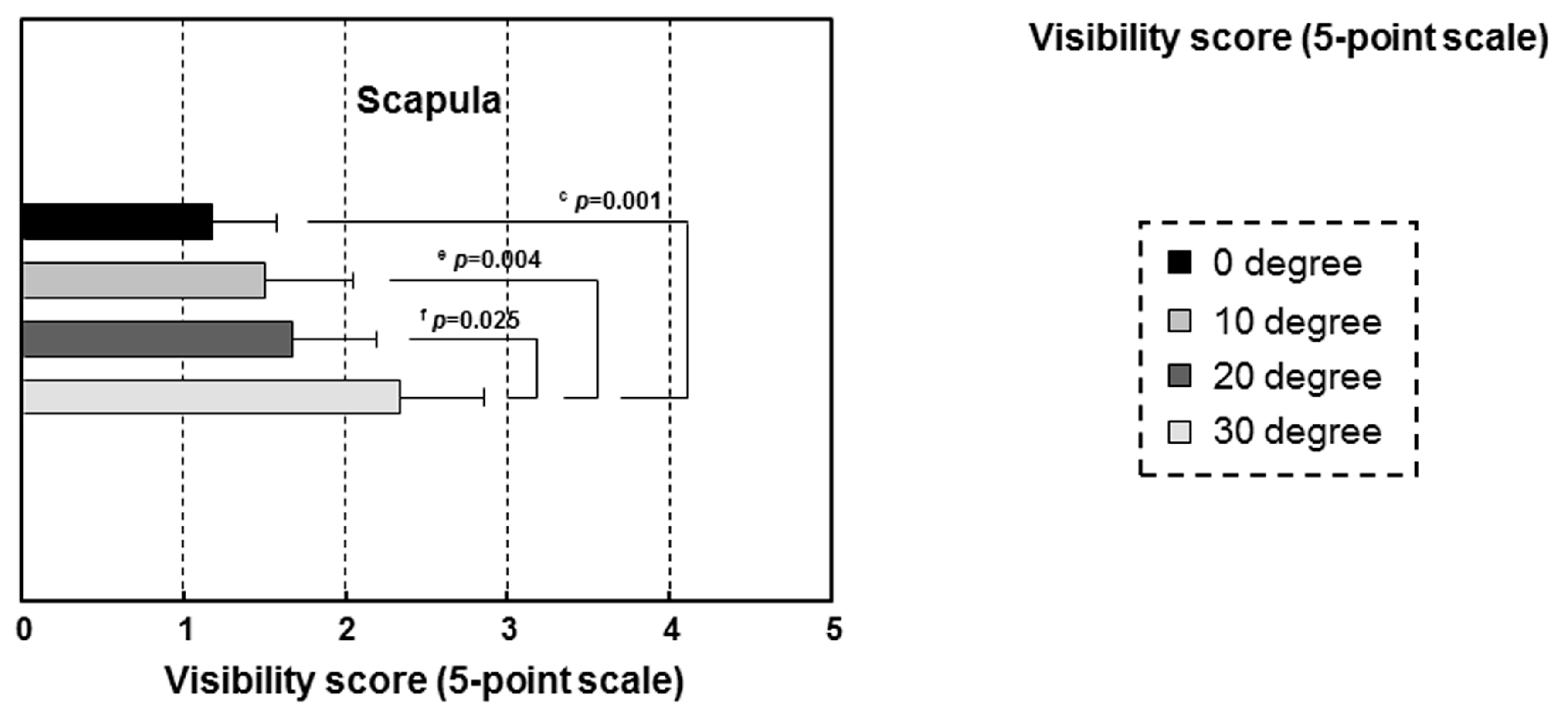
3.3. Chest Radiographic Study According to Different Angles for Clinical Application
4. Discussion and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| ALARA | as low as reasonably achievable |
| CNR | contrast-to noise |
| CTD | cardiac transverse diameter |
| CV | coefficient of variance |
| DICOM | Digital Imaging and Communications in Medicine |
| DOF | degree of freedom |
| DR | digital radiography |
| ESD | entrance surface dose |
| FPD | flat-panel detector ratio |
| ICT | information and communication technologies |
| IMU | inertial measurement unit |
| MTF | modulation transfer function |
| PDR | portable digital radiography |
| rmANOVA | repeated-measures analysis of variance |
| SDA | X-ray source-detector angle |
| SDD | X-ray source-detector distance |
| SNR | signal-to-noise ratio |
| TFT | thin-film transistor |
| TLD | thoracic longitudinal diameter |
| TTD | thoracic transverse diameter |
References
- Korner, M.; Weber, C.H.; Wirth, S.; Pfeifer, K.J.; Reiser, M.F.; Treitl, M. Advances in digital radiography: Physical principles and system overview. Radiographics 2007, 27, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Lança, L.; Silva, A. Digital radiography detectors—A technical overview: Part 1. Radiography 2009, 15, 58–62. [Google Scholar] [CrossRef]
- Cho, H.S.; Jeong, M.H.; Han, B.S.; Kim, S.; Lee, B.S.; Kim, H.K.; Lee, S.C. Development of a portable digital radiographic system based on FOP-coupled CMOS image sensor and its performance evaluation. IEEE Trans. Nucl. Sci. 2005, 52, 1766–1772. [Google Scholar] [CrossRef]
- Schaefer-Prokop, C.M.; De Boo, D.W.; Uffmann, M.; Prokop, M. DR and CR: Recent advances in technology. Eur. J. Radiol. 2009, 72, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.H.; Freckleton, M.W. Digital radiography for the field: A portable prototype. J. Digit. Imaging 2002, 15 (Suppl. 1), 194–197. [Google Scholar] [CrossRef] [PubMed]
- Lehnert, T.; Naguib, N.N.; Ackermann, H.; Schomerus, C.; Jacobi, V.; Balzer, J.O.; Vogl, T.J. Novel, portable, cassette-sized, and wireless flat-panel digital radiography system: Initial workflow results versus computed radiography. AJR Am. J. Roentgenol. 2011, 196, 1368–1371. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, W.S.; Kuo, K.M.; Liu, C.F.; Yao, H.C.; Chen, C.Y.; Lin, H.W. Managing repeat digital radiography images—A systematic approach and improvement. J. Med. Syst. 2012, 36, 2697–2704. [Google Scholar] [CrossRef] [PubMed]
- Chida, K.; Kaga, Y.; Haga, Y.; Takeda, K.; Zuguchi, M. Quality control phantom for flat panel detector X-ray systems. Health Phys. 2013, 104, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Poletti, J.L.; McLean, D. The effect of source to image-receptor distance on effective dose for some common X-ray projections. Br. J. Radiol. 2005, 78, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Bontrager, K.L.; Lampignano, J. Textbook of Radiographic Positioning and Related Anatomy, 8th ed.; Elsevier/Mosby: St. Louis, MO, USA, 2014. [Google Scholar]
- Lin, P.J.; Schueler, B.A.; Balter, S.; Strauss, K.J.; Wunderle, K.A.; LaFrance, M.T.; Kim, D.S.; Behrman, R.H.; Shepard, S.J.; Bercha, I.H. Accuracy and calibration of integrated radiation output indicators in diagnostic radiology: A report of the AAPM Imaging Physics Committee Task Group 190. Med. Phys. 2015, 42, 6815–6829. [Google Scholar] [CrossRef] [PubMed]
- Alkatout, I. Communicative and ethical aspects of physician-patient relationship in extreme situations. Wien. Med. Wochenschr. 2015, 165, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Rinkel, J.; Gerfault, L.; Esteve, F.; Dinten, J.M. A new method for X-ray scatter correction: First assessment on a cone-beam CT experimental setup. Phys. Med. Biol. 2007, 52, 4633–4652. [Google Scholar] [CrossRef] [PubMed]
- D’Ausilio, A. Arduino: A low-cost multipurpose lab equipment. Behav. Res. Methods 2012, 44, 305–313. [Google Scholar] [CrossRef] [PubMed]
- McCarron, B. Low-Cost IMU Implementation via Sensor Fusion Algorithms in the Arduino Environment; California Polytechnic State University: San Luis Obispo, CA, USA, 2013. [Google Scholar]
- Ryu, J.H.; Kim, T.H.; Jeong, C.W.; Jun, H.Y.; Heo, D.W.; Lee, J.; Kim, K.W.; Yoon, K.H. Dedicated mobile volumetric cone-beam computed tomography for human brain imaging: A phantom study. J. X-ray Sci. Technol. 2015, 23, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Fujita, H.; Tsai, D.Y.; Itoh, T.; Doi, K.; Morishita, J.; Ueda, K.; Ohtsuka, A. A simple method for determining the modulation transfer function in digital radiography. IEEE Trans. Med. Imaging 1992, 11, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Eckerman, K.; Harrison, J.; Menzel, H.G.; Clement, C.H. ICRP Publication 119: Compendium of Dose Coefficients based on ICRP Publication 60. Ann. ICRP 2012, 41 (Suppl. 1). [Google Scholar] [CrossRef] [PubMed]
- Rapp-Bernhardt, U.; Roehl, F.W.; Esseling, R.; Lenzen, H.; Schiborr, M.; Theobald-Hormann, I.; Heindel, W.; Bernhardt, T.M. Portable flat-panel detector for low-dose imaging in a pediatric intensive care unit: Comparison with an asymmetric film-screen system. Investig. Radiol. 2005, 40, 736–741. [Google Scholar] [CrossRef]
- Bruton, A.; Conway, J.H.; Holgate, S.T. Reliability: What is it, and how is it measured? Physiotherapy 2000, 86, 94–99. [Google Scholar] [CrossRef]
- Makri, T.; Yakoumakis, E.; Papadopoulou, D.; Gialousis, G.; Theodoropoulos, V.; Sandilos, P.; Georgiou, E. Radiation risk assessment in neonatal radiographic examinations of the chest and abdomen: A clinical and Monte Carlo dosimetry study. Phys. Med. Biol. 2006, 51, 5023–5033. [Google Scholar] [CrossRef] [PubMed]
- European Commission. EUR 16261—European Guidelines on Quality Criteria for Diagnostic Radiographic Images in Paediatrics; Office for Official Publications of the European Communities: Brussels, Belgium; Luxembourg, 1996. [Google Scholar]
- American College of Radiology (ACR); Society for Pediatric Radiology (SPR). ACR–SPR Practice Parameter for the Performance of Chest Radiography Res. 56-2011, Amended 2014 (Res. 39). 2013. Available online: http://www.acr.org/~/media/ACR/Documents/PGTS/guidelines/Chest_Radiography.pdf (accessed on 22 January 2015).
- American College of Radiology (ACR); Society for Pediatric Radiology (SPR). ACR–SPR Practice Parameter for the Performance of Portable (Mobile Unit) Chest Radiography Res. 55-2011, Amended 2014 (Res. 39). 2013. Available online: http://www.acr.org/~/media/ACR/Documents/PGTS/guidelines/Portable_Chest.pdf (accessed on 14 July 2014).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Degree (°) | Digital Angle Meter (A, Mean ± SD) | Developed SDA Device (B, Mean ± SD) | Angle Difference (B-A) |
|---|---|---|---|
| 0 | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.00 |
| 5 | 5.00 ± 0.00 | 5.30 ± 0.08 | 0.30 |
| 10 | 10.00 ± 0.00 | 10.70 ± 0.08 | 0.70 |
| 15 | 15.00 ± 0.00 | 15.50 ± 0.08 | 0.50 |
| 20 | 20.00 ± 0.00 | 20.87 ± 0.04 | 0.87 |
| 25 | 25.00 ± 0.00 | 25.80 ± 0.08 | 0.80 |
| 30 | 30.00 ± 0.00 | 30.70 ± 0.08 | 0.70 |
| 35 | 35.00 ± 0.00 | 35.77 ± 0.04 | 0.77 |
| 40 | 40.00 ± 0.00 | 40.77 ± 0.12 | 0.77 |
| 45 | 45.00 ± 0.00 | 45.77 ± 0.04 | 0.77 |
| 50 | 50.00 ± 0.00 | 50.80 ± 0.08 | 0.80 |
| 55 | 55.00 ± 0.00 | 55.77 ± 0.04 | 0.77 |
| 60 | 60.00 ± 0.00 | 60.73 ± 0.04 | 0.73 |
| p-value * | 0.865 | 0.71 ± 0.15 | |
| Angle Degree | 0° | 10° | 20° | 30° | p-Value * | |
|---|---|---|---|---|---|---|
| Value | ||||||
| SNR | 408.7 ± 160.0 | 408.8 ± 157.8 | 428.0 ± 176.3 | 463.4 ± 155.9 | 0.082 | |
| CNR | 82.3 ± 23.0 | 100.0 ± 30.9 | 102.8 ± 33.1 | 98.2 ± 28.8 | 0.114 | |
| Distortion † | ||||||
| CTD (size, mm) | 101.9 ± 0.3 | 104.4 ± 0.3 | 106.6 ± 0.4 | 107.5 ± 0.3 | <0.001 abcdef | |
| (deformity, %) | (100.0%) | (102.5%) | (104.6%) | (105.5%) | ||
| TTD (mm) | 278.0 ± 0.3 | 278.5 ± 0.1 | 278.7 ± 0.1 | 279.4 ± 0.3 | <0.001 abcdef | |
| (%) | (100.0%) | (100.2%) | (100.3%) | (100.5%) | ||
| TLD (mm) | 250.2 ± 1.0 | 260.7 ± 1.3 | 266.3 ± 1.3 | 273.7 ± 1.4 | <0.001 abcdef | |
| (%) | (100.0%) | (104.2%) | (106.4%) | (109.4%) | ||
| Visibility ‡ | ||||||
| Border of Heart | 1.67 ± 0.52 | 2.17 ± 0.75 | 2.50 ± 0.55 | 3.00 ± 0.00 | 0.044 bce | |
| Clavicle | 1.00 ± 0.00 | 1.33 ± 0.52 | 1.50 ± 0.55 | 1.83 ± 0.41 | 0.110 | |
| 1st Rib (Rt-side) | 1.00 ± 0.00 | 1.33 ± 0.52 | 1.50 ± 0.55 | 1.67 ± 0.52 | 0.292 | |
| 5th Rib (Rt-side) | 1.33 ± 0.52 | 1.67 ± 0.52 | 2.33 ± 0.52 | 3.00 ± 0.00 | <0.001 bcdef | |
| Scapula | 1.17 ± 0.41 | 1.50 ± 0.55 | 1.67 ± 0.52 | 2.33 ± 0.52 | 0.032 cef | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, T.-H.; Heo, D.-W.; Jeong, C.-W.; Ryu, J.-H.; Jun, H.Y.; Han, S.-J.; Ha, T.; Yoon, K.-H. Development of Portable Digital Radiography System with a Device for Monitoring X-ray Source-Detector Angle and Its Application in Chest Imaging. Sensors 2017, 17, 531. https://doi.org/10.3390/s17030531
Kim T-H, Heo D-W, Jeong C-W, Ryu J-H, Jun HY, Han S-J, Ha T, Yoon K-H. Development of Portable Digital Radiography System with a Device for Monitoring X-ray Source-Detector Angle and Its Application in Chest Imaging. Sensors. 2017; 17(3):531. https://doi.org/10.3390/s17030531
Chicago/Turabian StyleKim, Tae-Hoon, Dong-Woon Heo, Chang-Won Jeong, Jong-Hyun Ryu, Hong Young Jun, Seung-Jun Han, Taeuk Ha, and Kwon-Ha Yoon. 2017. "Development of Portable Digital Radiography System with a Device for Monitoring X-ray Source-Detector Angle and Its Application in Chest Imaging" Sensors 17, no. 3: 531. https://doi.org/10.3390/s17030531