Assessment of the Health Impacts of Climate Change in Kiribati

Abstract
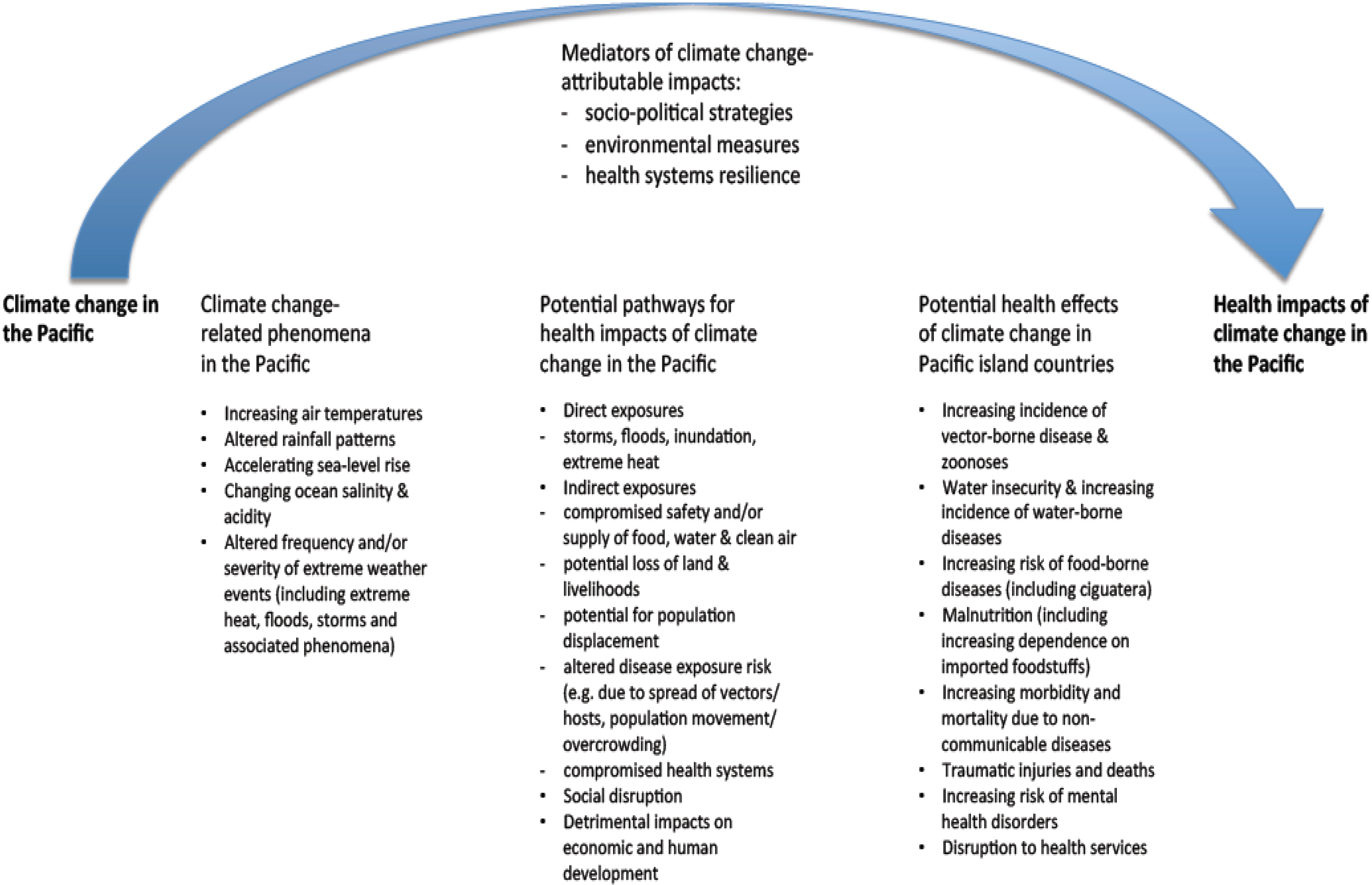
:1. Introduction
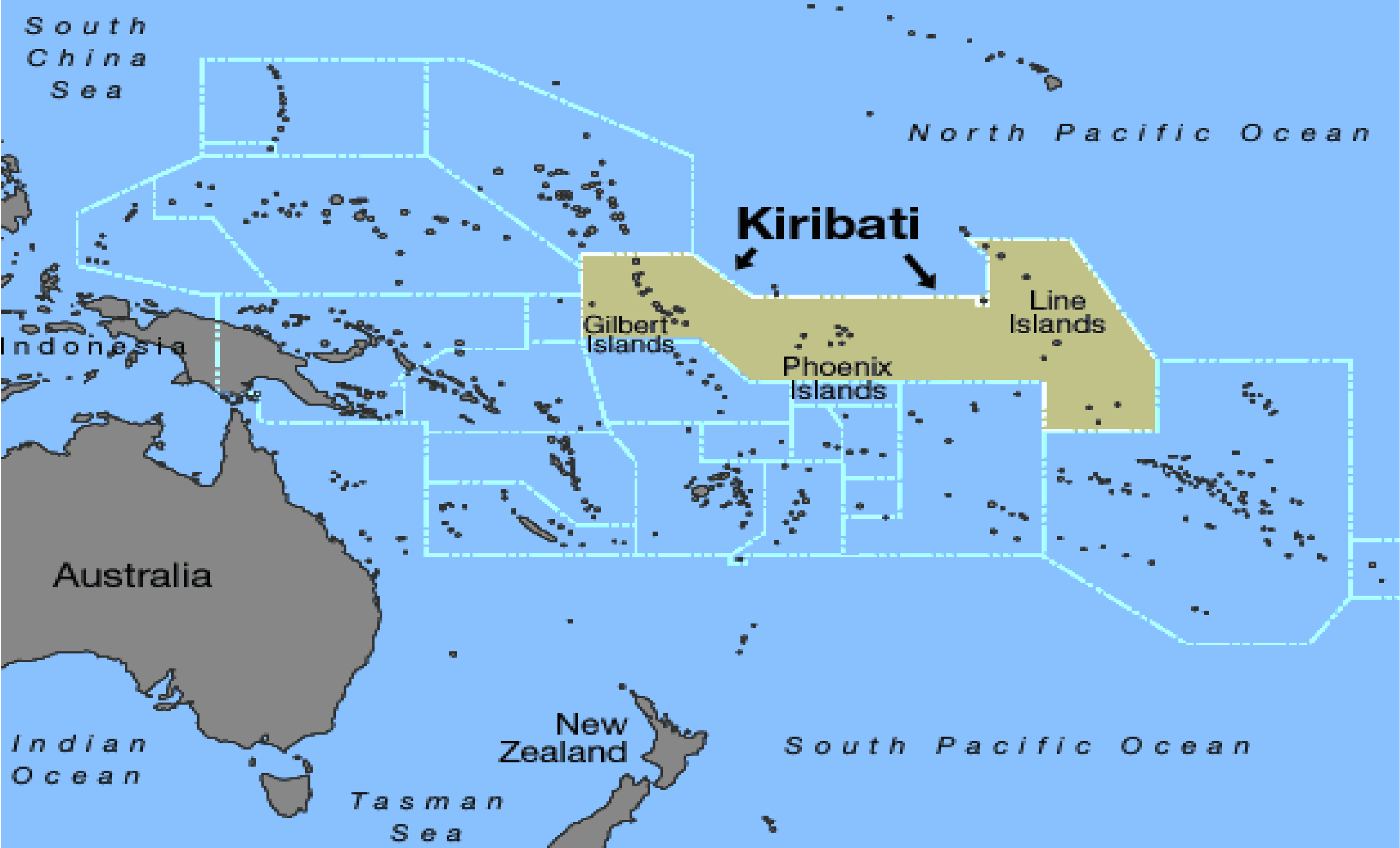
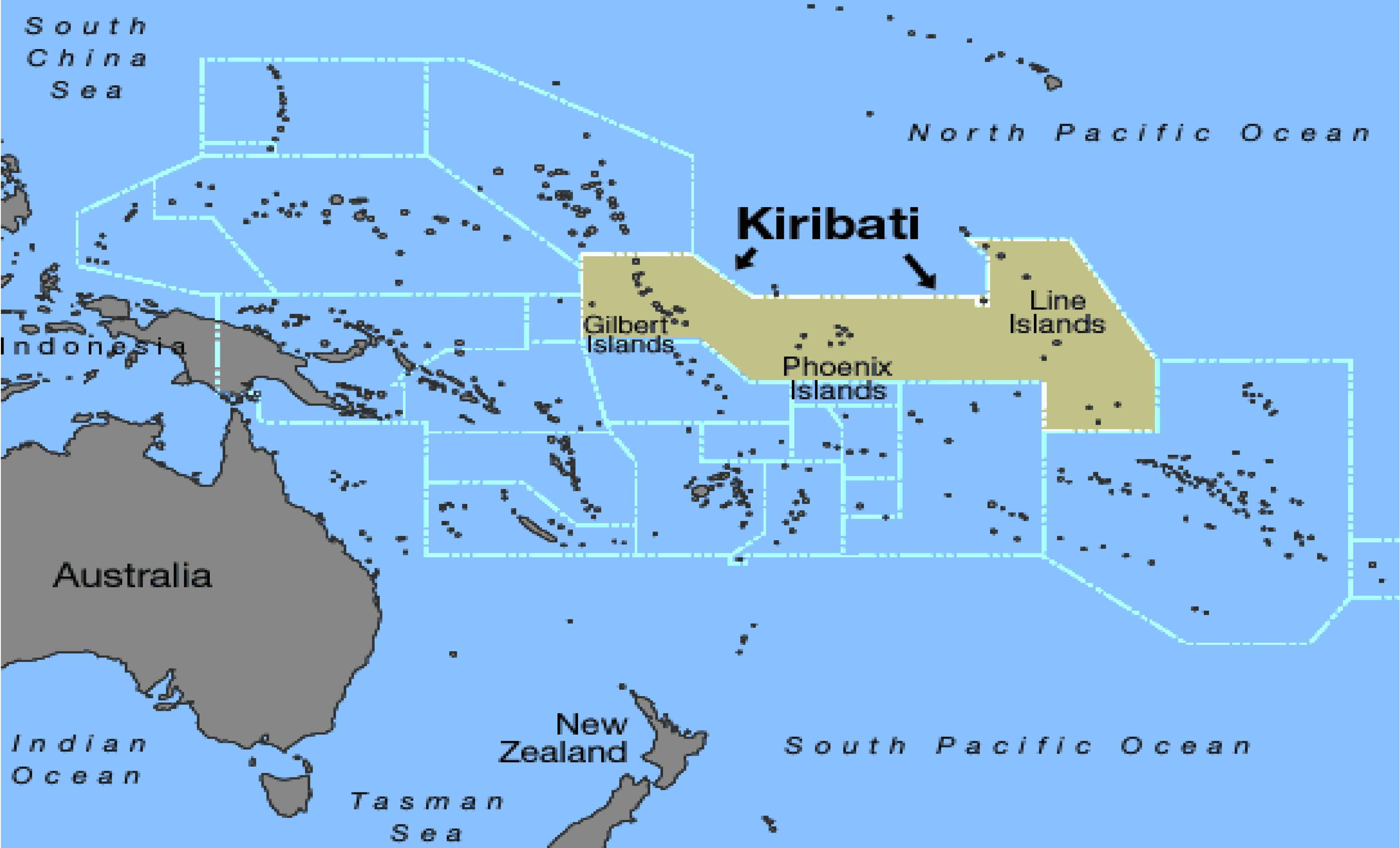
1.1. Background to Climate Change in Kiribati
1.2. Rationale for Assessment of Climate Change and Health in Kiribati
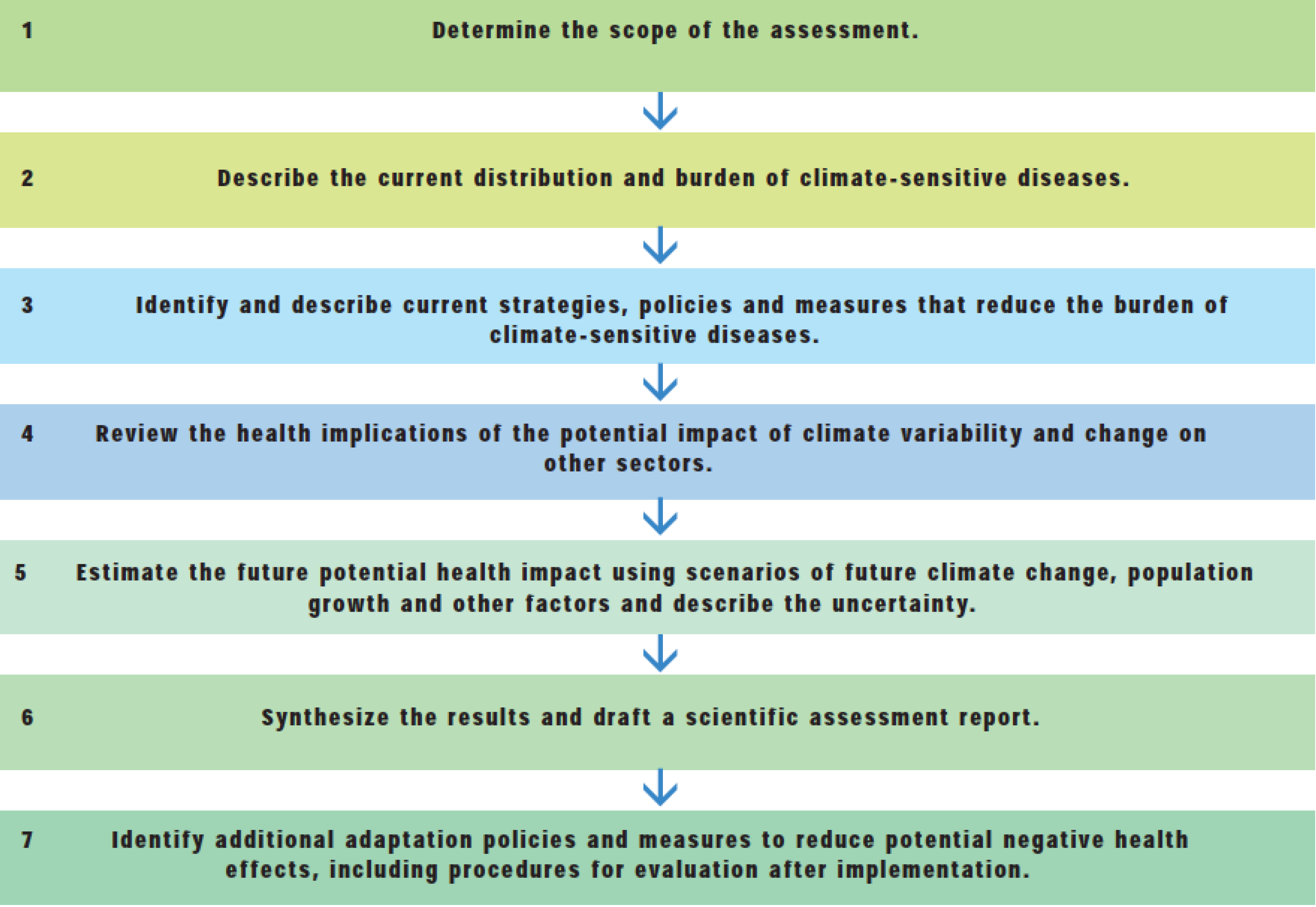
2. Methodology
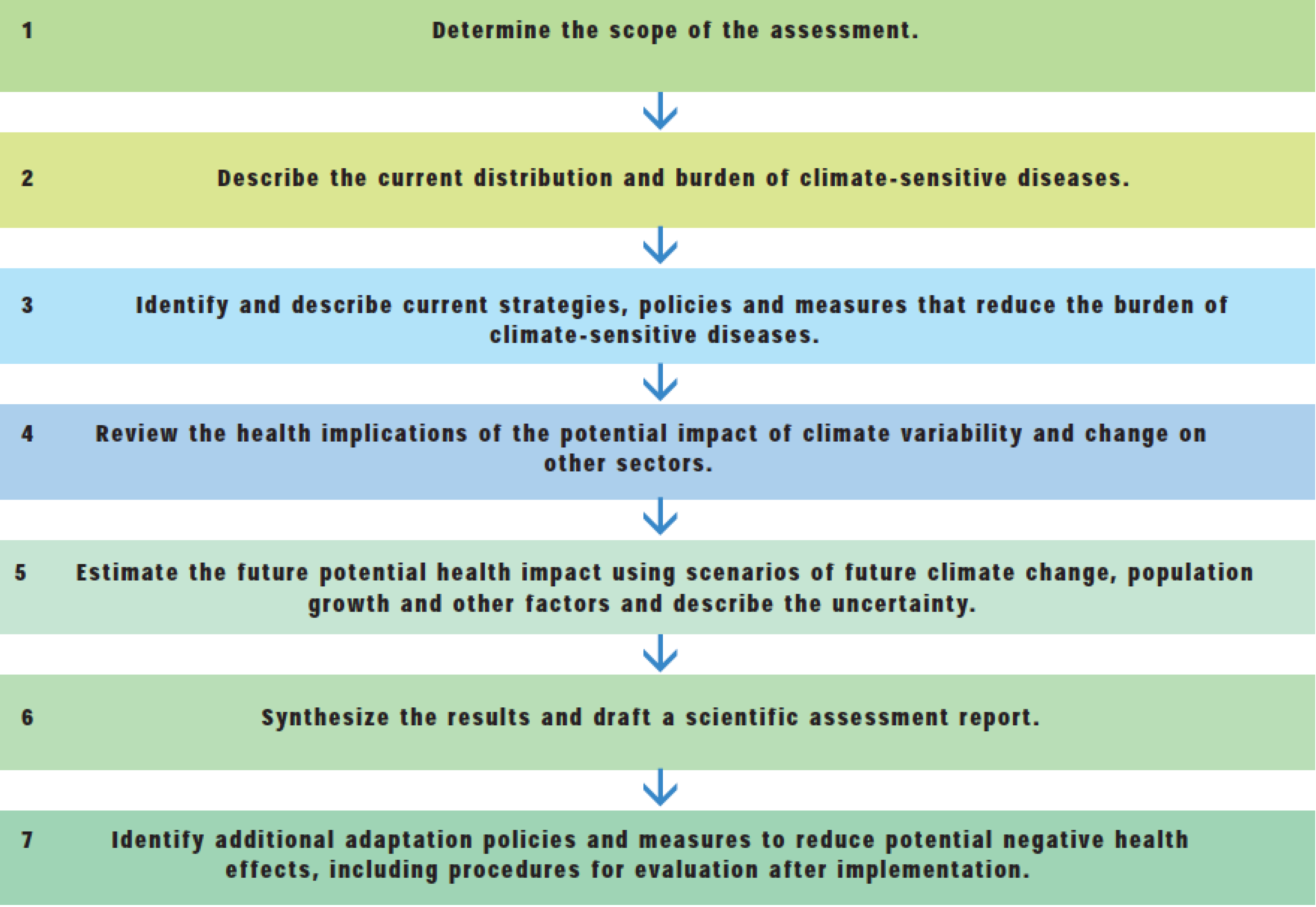
2.1. Determining the Scope of the Assessment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Likelihood | Impact (Considering Consequence and Coping Capacity) | ||||
|---|---|---|---|---|---|
| Insignificant | Minor | Moderate | Major | Catastrophic | |
| Almost Certain | Medium | Medium | High | Extreme | Extreme |
| Likely | Low | Medium | High | High | Extreme |
| Possible | Low | Medium | Medium | High | High |
| Unlikely | Low | Low | Medium | Medium | Medium |
| Rare | Low | Low | Low | Low | Medium |
2.2. Describing the Current Distribution and Burden of Climate-Sensitive Diseases
2.3. Identifying and Describing Current Strategies, Policies and Measures that Reduce the Burden of Climate-Sensitive Diseases
2.4. Reviewing the Health Implications of the Potential Impact of Climate Variability and Change on other Sectors
2.5. Estimating the Future Potential Health Impact Using Scenarios of Future Climate Change, Population Growth and Other Factors, and Describing the Related Uncertainty
2.6. Synthesizing the Results and Drafting a Scientific Assessment Report
2.7. Identifying Additional Adaptation Policies and Measures to Reduce Potential Negative Health Effects, Including Procedures for Evaluation Following Implementation
| Type/Source of Information Reviewed and Consulted | Name/Description of Source and Information Obtained |
|---|---|
| Data | notifiable disease surveillance data from MHMS (Health Information Unit) annual reports from MHMS historical climate data from Kiribati Meteorology Service climate change data (historical trends and predictions) from Pacific Climate Change Science Program quality of household sanitation and water supplies, information obtained from the 2010 national census population data (2010 census) |
| Stakeholders | Office of Te Beretitenti (Office of the President) Ministry of Health and Medical Services Ministry of Public Works and Utilities Ministry of Internal and Social Affairs Ministry of Fisheries and Marine Resources Development Ministry of Environment, Lands and Agricultural Development Ministry of Commerce, Industries and Cooperatives Kiribati Port Authority Overseas Environmental Cooperation Centre Secretariat for the Pacific Community (including the South Pacific Applied Geosciences Commission) Kiribati Association of Non-Government Organizations Community members (during health promotion workshops) World Health Organization |
| Previous/current activities related to climate change adaptation | National Adaptation Programme of Action (NAPA) Kiribati Adaptations Plans (I-III) Climate Change Adaptation Plan and Strategy National Framework for Climate Change Adaptation Second National Communication (to the United Nations Framework Convention on Climate Change) Kiribati Development Plan Kiribati National Development Strategies |
| Previous/current activities related to public health | Ministry of Health and Medical Services’ Strategic Plan National Population Policy National Disaster Risk Management Plan National Sanitation Implementation Plan |
3. Results
- (a)
- have been shown to be strongly linked to changes in climate (based on empirical epidemiological evidence and expert judgement);
- (b)
- would likely add substantially to the burden of disease in Kiribati; and
- (c)
- could be reduced by feasible public and environmental health interventions.
| Health Issue Likely to be Affected by Climate Change | Priority |
|---|---|
| Water safety and water-borne diseases | High |
| Food safety and food-borne diseases | High |
| Vector-borne diseases | High |
| Disease surveillance | High |
| Respiratory diseases | Low |
| Malnutrition | Low |
| Non-communicable diseases and heat-related illness | Low |
| Ciguatera | Low |
| Mental health | Low |
| Reproductive health | Low |
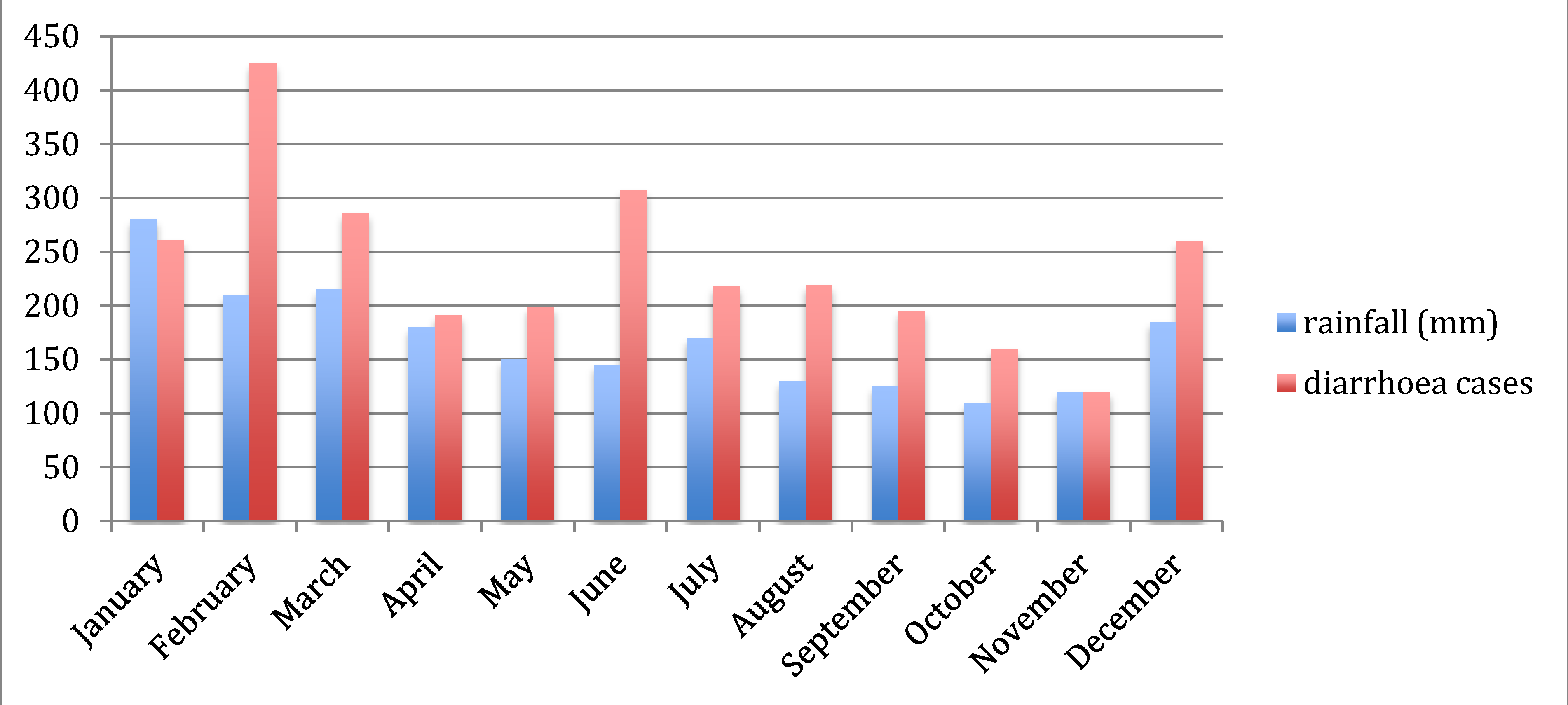
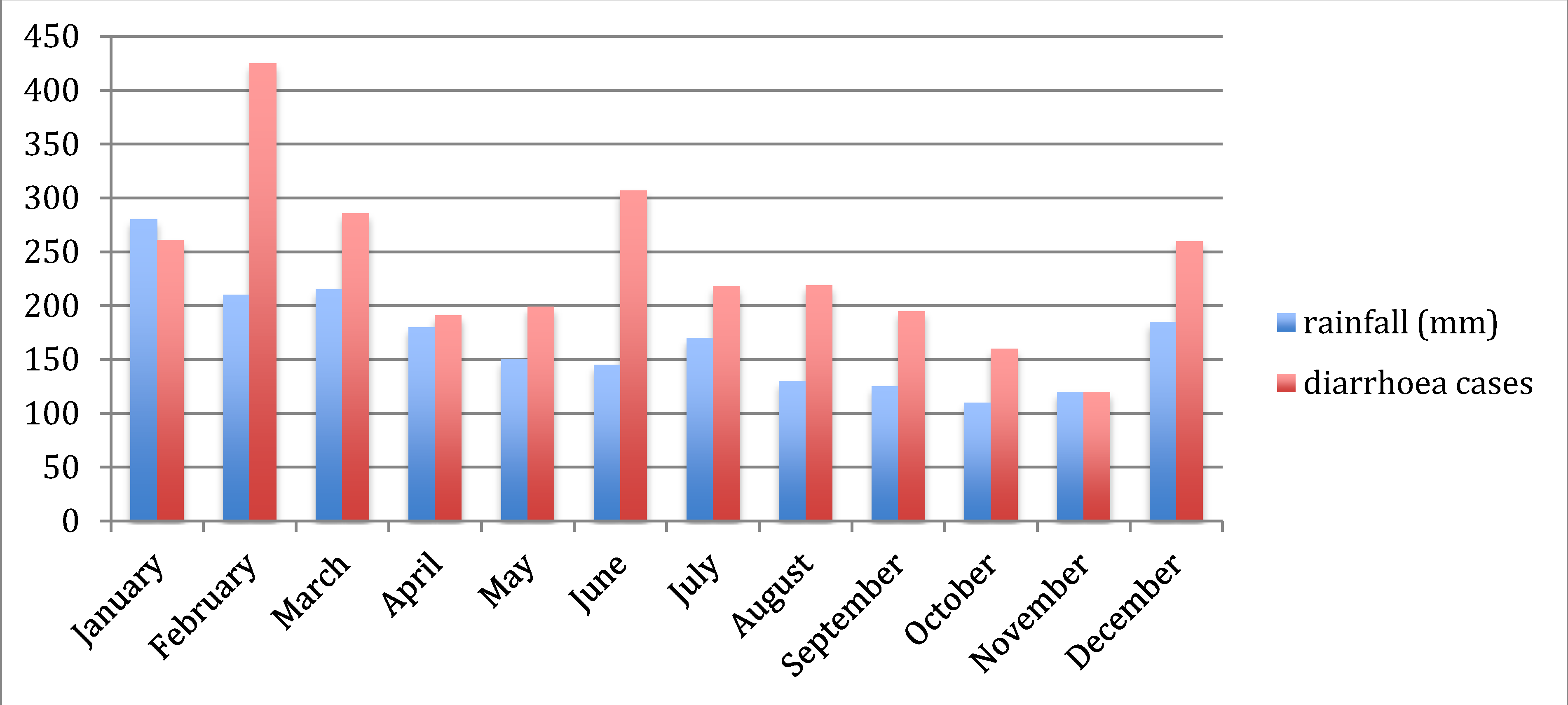
3.1. Water Safety and Water-borne Diseases
3.2. Food Safety and Food-borne Diseases
3.3. Vector-borne Diseases
3.4. Disease Surveillance
3.5. Respiratory Diseases
3.6. Malnutrition
3.8. Ciguatera
3.9. Mental Health
3.10. Reproductive Health
3.11. Vulnerable Groups
4. Discussion
4.1. Innovations and Challenges in the Vulnerability Assessment and Adaptation Planning Process in Kiribati
4.2. Future Direction of Climate Change and Health Adaptation in Kiribati
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ministry of Finance and Economic Planning 2010; Census of Population and Housing, National Statistics Office: Bairiki, Tarawa, Republic of Kiribati, 2012.
- Climate Change in the Pacific: Scientific Assessment and New Research—Country Report for Kiribati; Pacific Climate Change Science Program, Australian Bureau of Meteorology and the Commonwealth Scientific Industrial and Research Organisation: Canberra, Australia, 2011.
- Aung, T.; Singh, A.; Prasad, A. A study of sea-level changes in the Kiribati area for the last 16 years. Weather 2009, 64, 203–206. [Google Scholar] [CrossRef]
- McMichael, T.; Montgomery, H.; Costello, A. Health risks, present and future, from global climate change. BMJ 2012, 344. [Google Scholar] [CrossRef]
- Haines, A.; Kovats, R.S.; Campbell-Lendrum, D.; Corvalan, C. Climate change and human health: Impacts, vulnerability and public health. Public Health 2006, 120, 585–596. [Google Scholar] [CrossRef]
- Singh, S.; Mushtaq, U.; Holm-Hansen, C.; Milan, D.; Cheung, A.; Watts, N. The importance of climate change to health. Lancet 2011, 378, 29–30. [Google Scholar]
- Patz, J.A.; Campbell-Lendrum, D.; Holloway, T.; Foley, J.A. Impact of regional climate change on human health. Nature 2005, 438, 310–317. [Google Scholar] [CrossRef]
- Kovats, R.S.; Menne, B.; McMichael, A.J.; Corvalan, C.; Bertollini, R. Climate Change and Human Health: Impact and Adaptation; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Woodward, A.; Hales, S.; Weinstein, P. Climate change and human health in the Asia Pacific region: Who will be most vulnerable? Clim. Res. 1998, 11, 31–38. [Google Scholar] [CrossRef]
- Lovell, S.A. Health governance and the impact of climate change on Pacific small island developing states. IHDP Update 2011, 1, 50–55. [Google Scholar]
- Singh, R.B.; Hales, S.; de Wet, N.; Raj, R.; Hearnden, M.; Weinstein, P. The influence of climate variation and change on diarrheal disease in the Pacific Islands. Environ. Health Perspect. 2001, 109, 155–159. [Google Scholar] [CrossRef]
- Ebi, K.L.; Lewis, N.D.; Corvalan, C.; Lucia, S. Climate variability and change and their potential health effects in small island states: Information for adaptation planning in the health sector. Environ. Health Perspect. 2006, 114, 1957–1963. [Google Scholar]
- Spickett, J.T.; Katscherian, D.; McIver, L. Health impacts of climate change in Vanuatu: An assessment and adaptation action plan. Glob. J. Health Sci. 2013, 5, 42–53. [Google Scholar]
- WHO and Secretariat for the Pacific Community Madang Commitment; WHO and Secretariat for the Pacific Community: Geneva, Switzerland, 2009; pp. 13–14.
- Regional Framework for Action to Protect Human Health from Effects of Climate Change in the Asia-Pacific Region; World Health Organization, Western Pacific Regional Office: Manila, Philippines, 2007; pp. 1–4.
- National Adaptation Programme of Action (NAPA); Ministry of Environment, Land and Agricultural Development: Tarawa, Republic of Kiribati, 2007.
- Campbell-Lendrum, D.; Woodruff, R. Climate Change: Quantifying the Health Impact at National and Local Levels. 2007. Available online: http://whqlibdoc.who.int/publications/2007/9789241595674_eng.pdf?ua=1 (accessed on 7 May 2014).
- Ebi, K.L.; Kovats, R.S.; Menne, B. An approach for assessing human health vulnerability and public health interventions to adapt to climate change. Environ. Health Perspect. 2006, 114, 1930–1934. [Google Scholar]
- Spickett, J.T.; Brown, H.L.; Katscherian, D. Adaptation strategies for health impacts of climate change in Western Australia: Application of a health impact assessment framework. Environ. Impact Assess. Rev. 2011, 31, 297–300. [Google Scholar] [CrossRef]
- Kovats, S.; Ebi, K.; Menne, B. Methods of Assessing Human Health Vulnerability and Public Health Adaptation to Climate Change. Available online: http://www.euro.who.int/__data/assets/pdf_file/0009/91098/E81923.pdf (accessed on 7 May 2014).
- Prüss-Ustün, A.; Corvalán, C. How much disease burden can be prevented by environmental interventions? Epidemiology 2007, 18, 167–178. [Google Scholar] [CrossRef]
- Bank, World. In Kiribati Adaptation Program—Phase III Project Appraisal Document; East Asia and Pacific Region, World Bank Sustainable Development: Washington DC, USA, 2011.
- Cheng, J.J.; Berry, P. Health co-benefits and risks of public health adaptation strategies to climate change: A review of current literature. Int. J. Public Health 2013, 58, 305–311. [Google Scholar] [CrossRef]
- Ganten, D.; Haines, A.; Souhami, R. Health co-benefits of policies to tackle climate change. Lancet 2010, 376, 1802–1804. [Google Scholar] [CrossRef]
- Parker, C.L. Health impacts of sea-level rise. Plan. Environ. Law 2014, 66, 8–12. [Google Scholar] [CrossRef]
- Hashizume, M.; Armstrong, B.; Hajat, S.; Wagatsuma, Y.; Faruque, A.S.G.; Hayashi, T.; Sack, D.A. Association between climate variability and hospital visits for non-cholera diarrhoea in Bangladesh: Effects and vulnerable groups. Int. J. Epidemiol. 2007, 36, 1030–1037. [Google Scholar] [CrossRef]
- Milojevic, A.; Armstrong, B.; Hashizume, M.; McAllister, K.; Faruque, A.; Yunus, M.; Streatfield, P.K.; Moji, K.; Wilkinson, P. Health effects of flooding in rural Bangladesh. Epidemiology 2012, 23, 107–115. [Google Scholar] [CrossRef]
- Funari, E.; Manganelli, M.; Sinisi, L. Impact of climate change on waterborne diseases. Ann. Ist. Super. Sanita 2012, 48, 473–487. [Google Scholar] [CrossRef]
- Cann, K.F.; Thomas, D.R.; Salmon, R.L.; Wyn-Jones, A.P.; Kay, D. Extreme water-related weather events and waterborne disease. Epidemiol. Infect. 2013, 141, 671–686. [Google Scholar] [CrossRef]
- Spini, L.; Adeel, Z.; Rosenberg, M.W. The nexus of water and human health in the context of global changes. Curr. Opin. Environ. Sustain. 2011, 3. [Google Scholar] [CrossRef]
- Fewtrell, L.; Kaufmann, R.; Kay, D. Water, sanitation, and hygiene interventions to reduce diarrhoea in less developed countries: A systematic review and meta-analysis. Lancet Infect. 2005, 5, 42–52. [Google Scholar] [CrossRef]
- Gunnarsdottir, M.J.; Gardarsson, S.M.; Elliott, M.; Sigmundsdottir, G.; Bartram, J. Benefits of water safety plans: Microbiology, compliance, and public health. Environ. Sci. Technol. 2012, 46, 7782–7789. [Google Scholar] [CrossRef]
- Markandya, A.; Chiabai, A. Valuing climate change impacts on human health: Empirical evidence from the literature. Int. J. Environ. Res. Public Health 2009, 6, 759–786. [Google Scholar] [CrossRef]
- El-Fadel, M.; Ghanimeh, S.; Maroun, R.; Alameddine, I. Climate change and temperature rise: Implications on food- and water-borne diseases. Sci. Total Environ. 2012, 437, 15–21. [Google Scholar] [CrossRef]
- Semenza, J.C.; Suk, J.E.; Estevez, V.; Ebi, K.L.; Lindgren, E. Mapping climate change vulnerabilities to infectious diseases in europe. Environ. Health Perspect. 2012, 120, 385–392. [Google Scholar]
- Rose, J.B.; Epstein, P.R.; Lipp, E.K.; Sherman, B.H.; Bernard, S.M.; Patz, J.A. Climate variability and change in the United States: Potential impacts on water- and foodborne diseases caused by microbiologic agents. Environ. Health Perspect. 2001, 109, 211–221. [Google Scholar] [CrossRef]
- Chowell, G.; Cazelles, B.; Broutin, H.; Munayco, C.V. The influence of geographic and climate factors on the timing of dengue epidemics in Perú, 1994–2008. BMC Infect. Dis. 2011, 11. [Google Scholar] [CrossRef]
- Thai, K.T.D.; Anders, K.L. The role of climate variability and change in the transmission dynamics and geographic distribution of dengue. Exp. Biol. Med. 2011, 236, 944–954. [Google Scholar] [CrossRef]
- Rosa-Freitas, M.G.; Schreiber, K.V.; Tsouris, P.; Weimann, E.T.D.S.; Luitgards-Moura, J.F. Associations between dengue and combinations of weather factors in a city in the Brazilian Amazon. Rev. Panam. Salud Publica 2006, 20, 256–267. [Google Scholar]
- Hunter, P.R. Climate change and waterborne and vector-borne disease. J. Appl. Microbiol. 2003, 94, S37–S46. [Google Scholar] [CrossRef]
- Hales, S.; de Wet, N.; Maindonald, J.; Woodward, A. Potential effect of population and climate changes on global distribution of dengue fever: An empirical model. Lancet 2002, 360, 830–834. [Google Scholar] [CrossRef]
- Guzman, M.G.; Halstead, S.B.; Artsob, H.; Buchy, P.; Farrar, J.; Gubler, D.J.; Hunsperger, E.; Kroeger, A.; Margolis, H.S.; Martínez, E.; et al. Dengue: A continuing global threat. Nat. Rev. Microbiol. 2010, 8, S7–S16. [Google Scholar] [CrossRef]
- Weiss, R.A.; McMichael, A.J. Social and environmental risk factors in the emergence of infectious diseases. Nat. Med. 2004, 10, S70–S76. [Google Scholar] [CrossRef]
- Lowe, R.; Bailey, T.C.; Stephenson, D.B.; Jupp, T.E.; Graham, R.J.; Barcellos, C.; Carvalho, M.S. The development of an early warning system for climate-sensitive disease risk with a focus on dengue epidemics in southeast Brazil. Stat. Med. 2013, 32, 864–883. [Google Scholar] [CrossRef]
- Chaves, L.F.; Pascual, M. Comparing models for early warning systems of neglected tropical diseases. PLoS Negl. Trop. Dis. 2007, 1. [Google Scholar] [CrossRef]
- Yu, H.-L.; Yang, S.J.; Yen, H.J.; Christakos, G. A spatio-temporal climate-based model of early dengue fever warning in southern Taiwan. Environ. Res. 2011, 25, 485–494. [Google Scholar]
- Paynter, S.; Ware, R.S.; Weinstein, P.; Williams, G.; Sly, P.D. Childhood pneumonia: A neglected, climate-sensitive disease? Lancet 2010, 376, 1804–1805. [Google Scholar] [CrossRef]
- Takaro, T. Climate change and respiratory health: Current evidence and knowledge gaps. Expert Rev. Resp. Med. 2013, 7, 349–361. [Google Scholar] [CrossRef]
- Ebi, K.L. Adaptation costs for climate change-related cases of diarrhoeal disease, malnutrition, and malaria in 2030. Global Health 2008, 4. [Google Scholar] [CrossRef]
- Friel, S.; Bowen, K.; Campbell-Lendrum, D.; Frumkin, H.; McMichael, A.J.; Rasanathan, K. Climate change, noncommunicable diseases, and development: The relationships and common policy opportunities. Annu. Rev. Public Health 2011, 32, 133–147. [Google Scholar] [CrossRef]
- Kjellstrom, T.; McMichael, A.J. Climate change threats to population health and well-being: The imperative of protective solutions that will last. Glob. Health Action 2013, 6, 1–9. [Google Scholar]
- Tawatsupa, B.; Dear, K.; Kjellstrom, T.; Sleigh, A. The association between temperature and mortality in tropical middle income Thailand from 1999 to 2008. Int. J. Biometeorol. 2014, 58, 203–215. [Google Scholar] [CrossRef]
- Lundgren, K.; Kuklane, K.; Gao, C.; Holmér, I. Effects of heat stress on working populations when facing climate change. Ind. Health 2013, 51, 3–15. [Google Scholar] [CrossRef]
- Hales, S.; Weinstein, P.; Woodward, A. Ciguatera (fish poisoning), El Niño, and Pacific Sea surface temperatures. Ecosyst. Health 1999, 5, 20–25. [Google Scholar] [CrossRef]
- Skinner, M.P.; Brewer, T.D.; Johnstone, R.; Fleming, L.E.; Lewis, R.J. Ciguatera fish poisoning in the Pacific Islands (1998 to 2008). Methods 2011, 5, 1–7. [Google Scholar]
- Llewellyn, L.E. Revisiting the association between sea surface temperature and the epidemiology of fish poisoning in the South Pacific: Reassessing the link between ciguatera and climate change. Toxicon 2010, 56, 691–697. [Google Scholar] [CrossRef]
- Berry, H.L.; Bowen, K.; Kjellstrom, T. Climate change and mental health: A causal pathways framework. Int. J. Public Health 2010, 55, 123–132. [Google Scholar] [CrossRef]
- Albrecht, G.; Sartore, G.; Connor, L.; Higginbotham, N.; Freeman, S.; Kelly, B.; Stain, H.; Tonna, A.; Pollard, G. Solastalgia: The distress caused by environmental change. 2007, 15, 95–98. [Google Scholar]
- Davidson, J.R.; McFarlane, A.C. The extent and impact of mental health problems after disaster. J. Clin. Psychiat. 2006, 67, 9–14. [Google Scholar] [CrossRef]
- Berry, H.; Bowen, K.; Kjellstrom, T. Climate change and mental health—A causal pathways framework. Int. J. Public Health 2010, 55, 123–132. [Google Scholar] [CrossRef]
- Obrien, L.V.; Berry, H.L.; Coleman, C.; Hanigan, I.C. Drought as a mental health exposure. Environ. Res. 2014, 131, 181–187. [Google Scholar] [CrossRef]
- Mcmichael, C.; Barnett, J.; Mcmichael, A.J. An ill wind? Climate change, migration, and health. Environ. Health Perspect. 2012, 120, 646–654. [Google Scholar] [CrossRef]
- Heltberg, R.; Siegel, P.B.; Jorgensen, S.L. Addressing human vulnerability to climate change: Toward a “no-regrets” approach. Glob. Environ. Chang. 2009, 19, 89–99. [Google Scholar] [CrossRef]
- Wardekker, J.A.; de Jong, A.; van Bree, L.; Turkenburg, W.C.; van der Sluijs, J.P. Health risks of climate change: An assessment of uncertainties and its implications for adaptation policies. Environ. Health 2012, 11. [Google Scholar] [CrossRef]
- Patz, J.; Campbell-Lendrum, D.; Gibbs, H.; Woodruff, R. Health impact assessment of global climate change: Expanding on comparative risk assessment approaches for policy making. Annu. Rev. Public Health 2008, 29, 27–39. [Google Scholar] [CrossRef]
- Chalabi, Z.; Kovats, S. Tools for developing adaptation policy to protect human health. Mitig. Adapt. Strateg. Glob. Change 2014, 19, 309–330. [Google Scholar] [CrossRef]
- Randolph, S.E. Is expert opinion enough? A critical assessment of the evidence for potential impacts of climate change on tick-borne diseases. Anim. Health Res. Rev. 2013, 14, 133–137. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
McIver, L.; Woodward, A.; Davies, S.; Tibwe, T.; Iddings, S. Assessment of the Health Impacts of Climate Change in Kiribati. Int. J. Environ. Res. Public Health 2014, 11, 5224-5240. https://doi.org/10.3390/ijerph110505224
McIver L, Woodward A, Davies S, Tibwe T, Iddings S. Assessment of the Health Impacts of Climate Change in Kiribati. International Journal of Environmental Research and Public Health. 2014; 11(5):5224-5240. https://doi.org/10.3390/ijerph110505224
Chicago/Turabian StyleMcIver, Lachlan, Alistair Woodward, Seren Davies, Tebikau Tibwe, and Steven Iddings. 2014. "Assessment of the Health Impacts of Climate Change in Kiribati" International Journal of Environmental Research and Public Health 11, no. 5: 5224-5240. https://doi.org/10.3390/ijerph110505224