
The Impacts of Air Temperature on Accidental Casualties in Beijing, China



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Statistical Analysis
3. Results
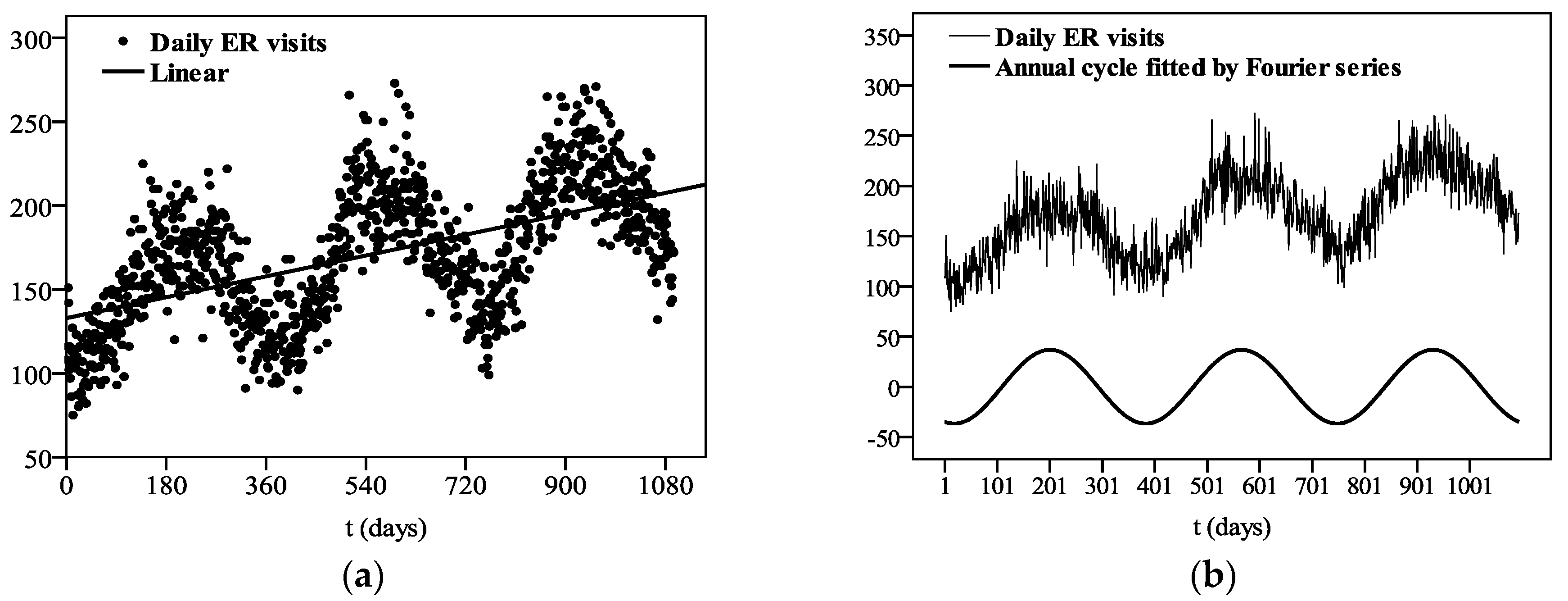
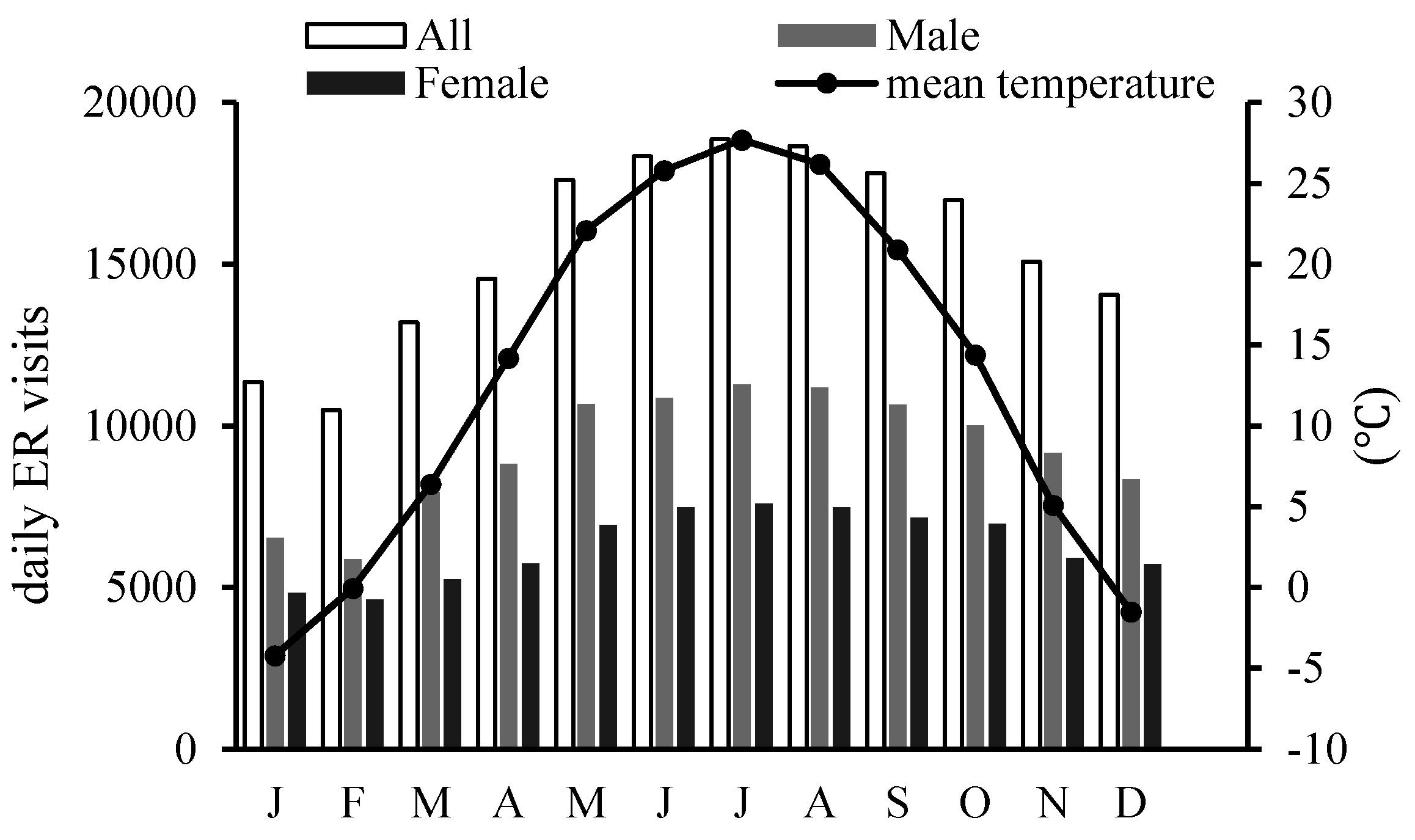
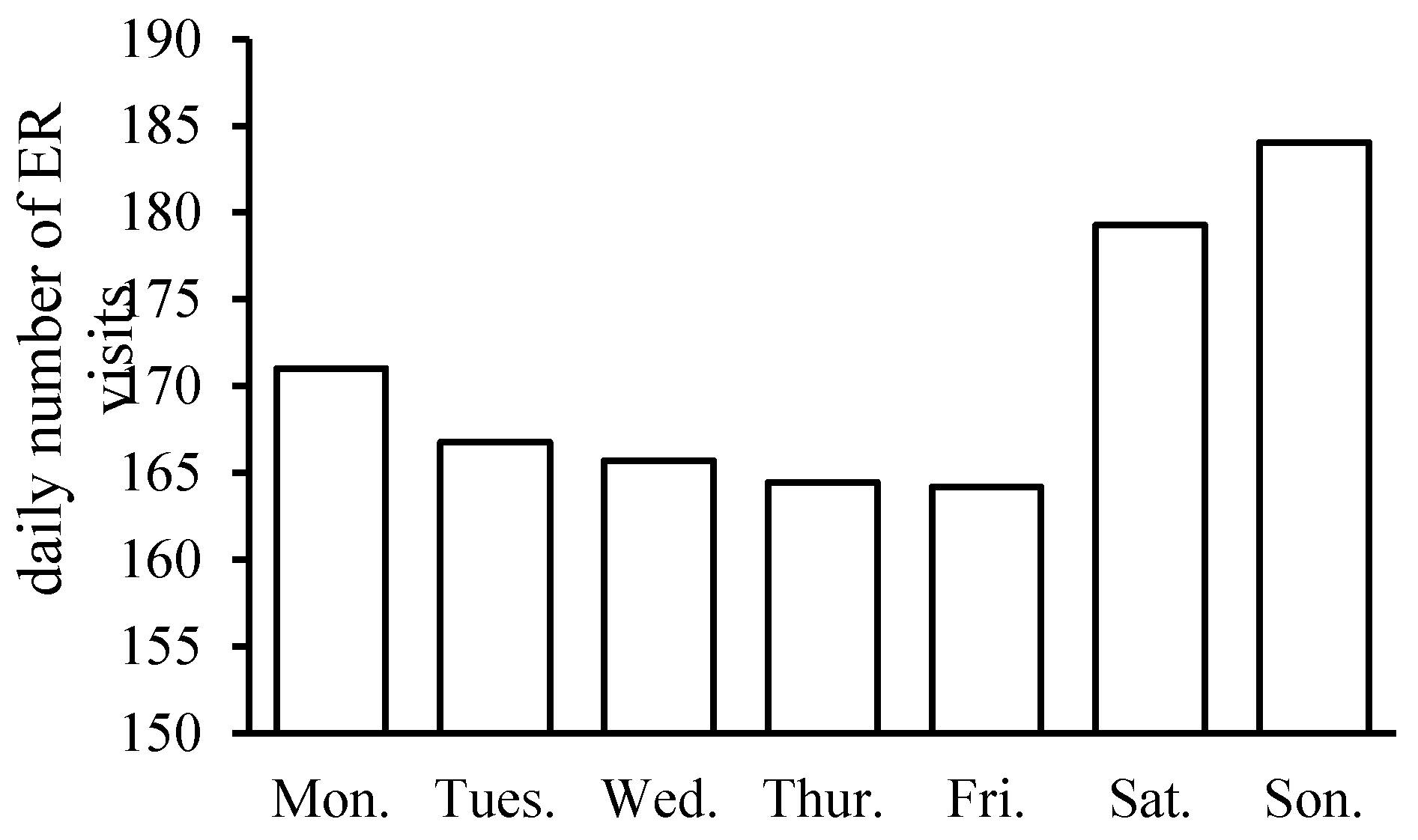
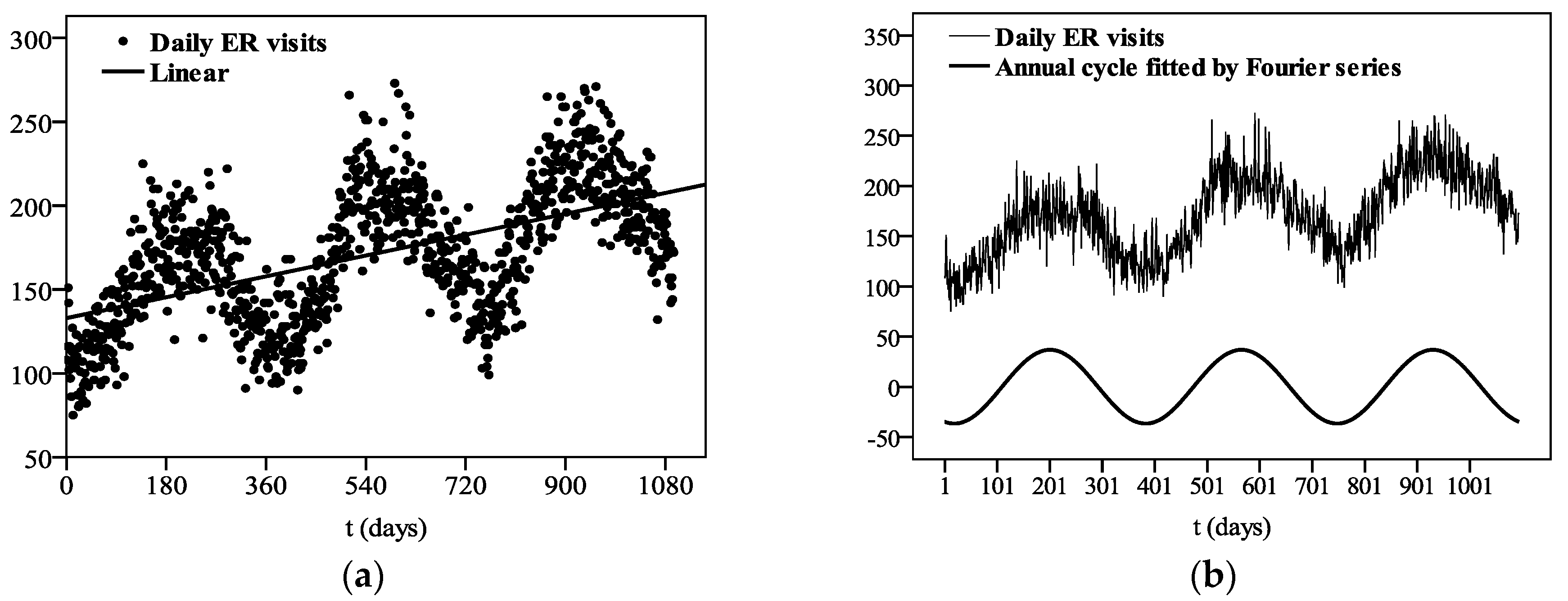
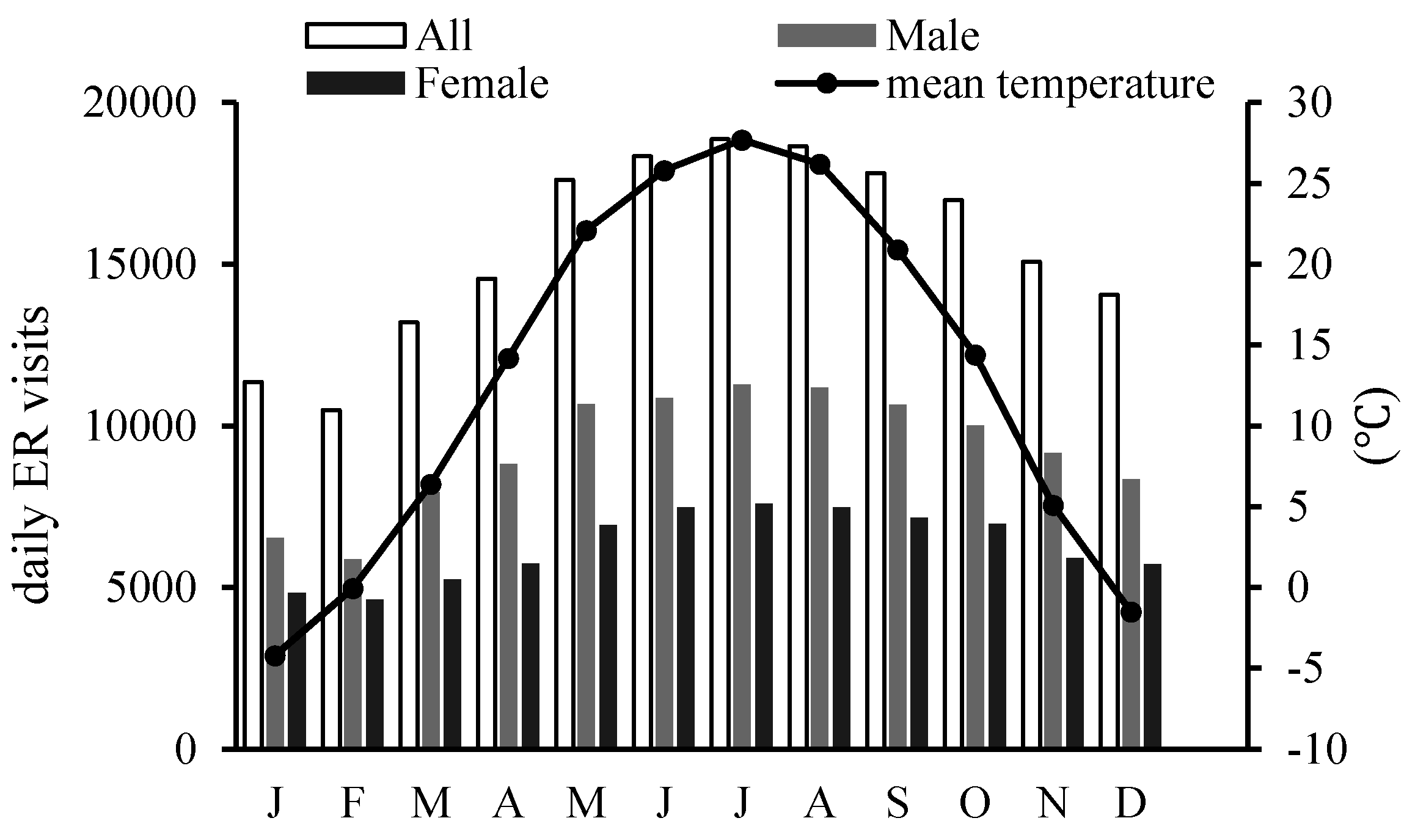
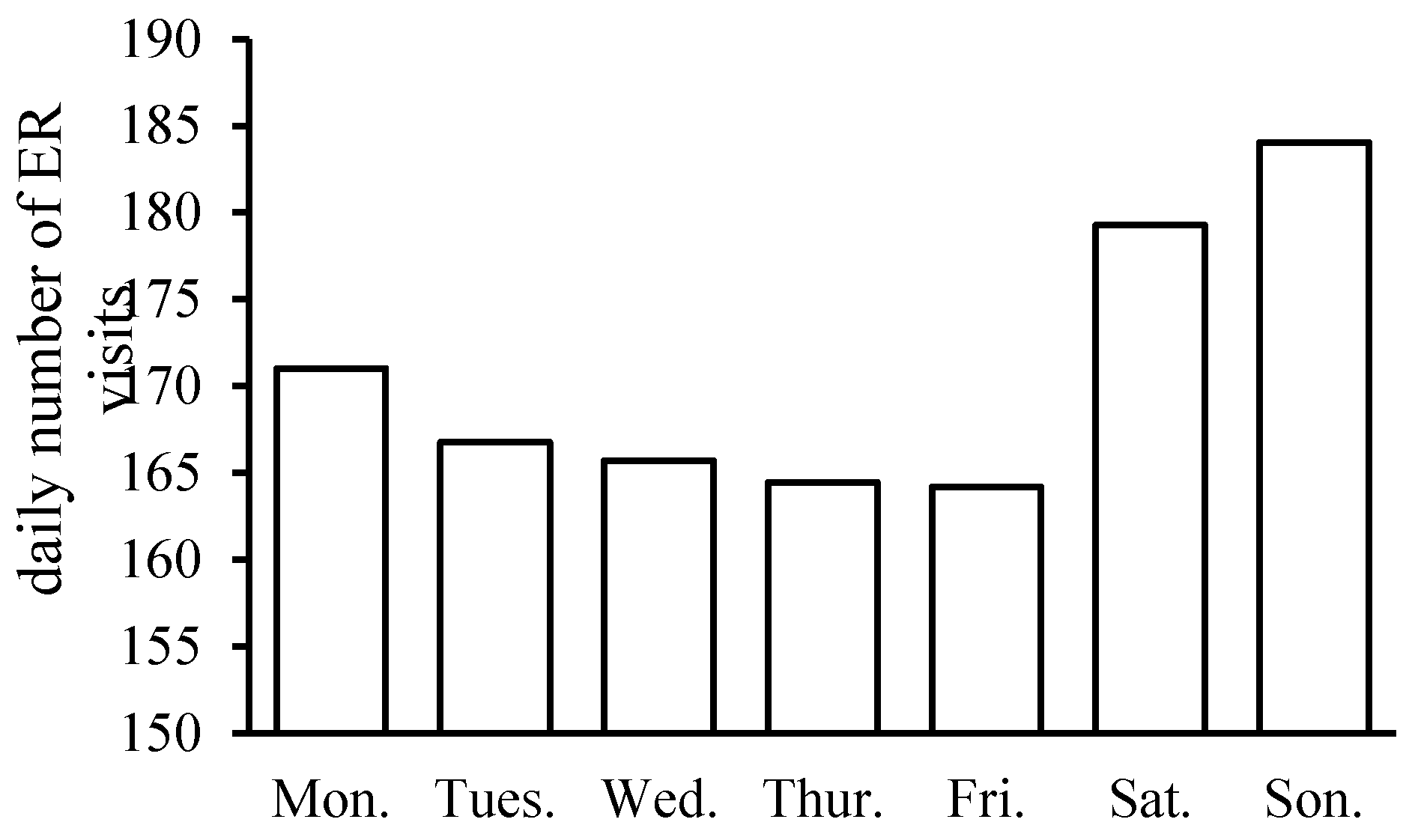
3.1. Descriptive Statistics of Variables
3.2. Correlation Analysis
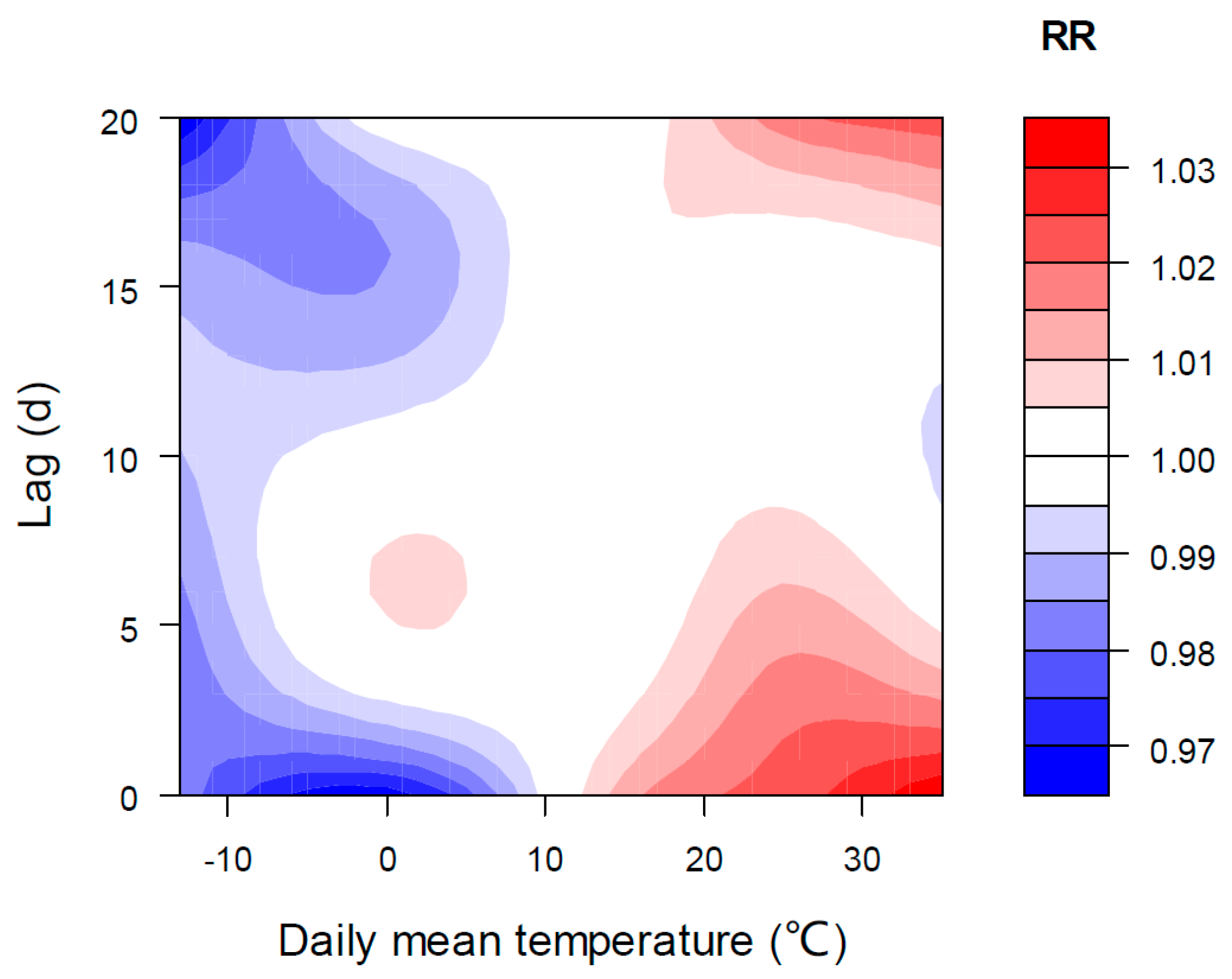
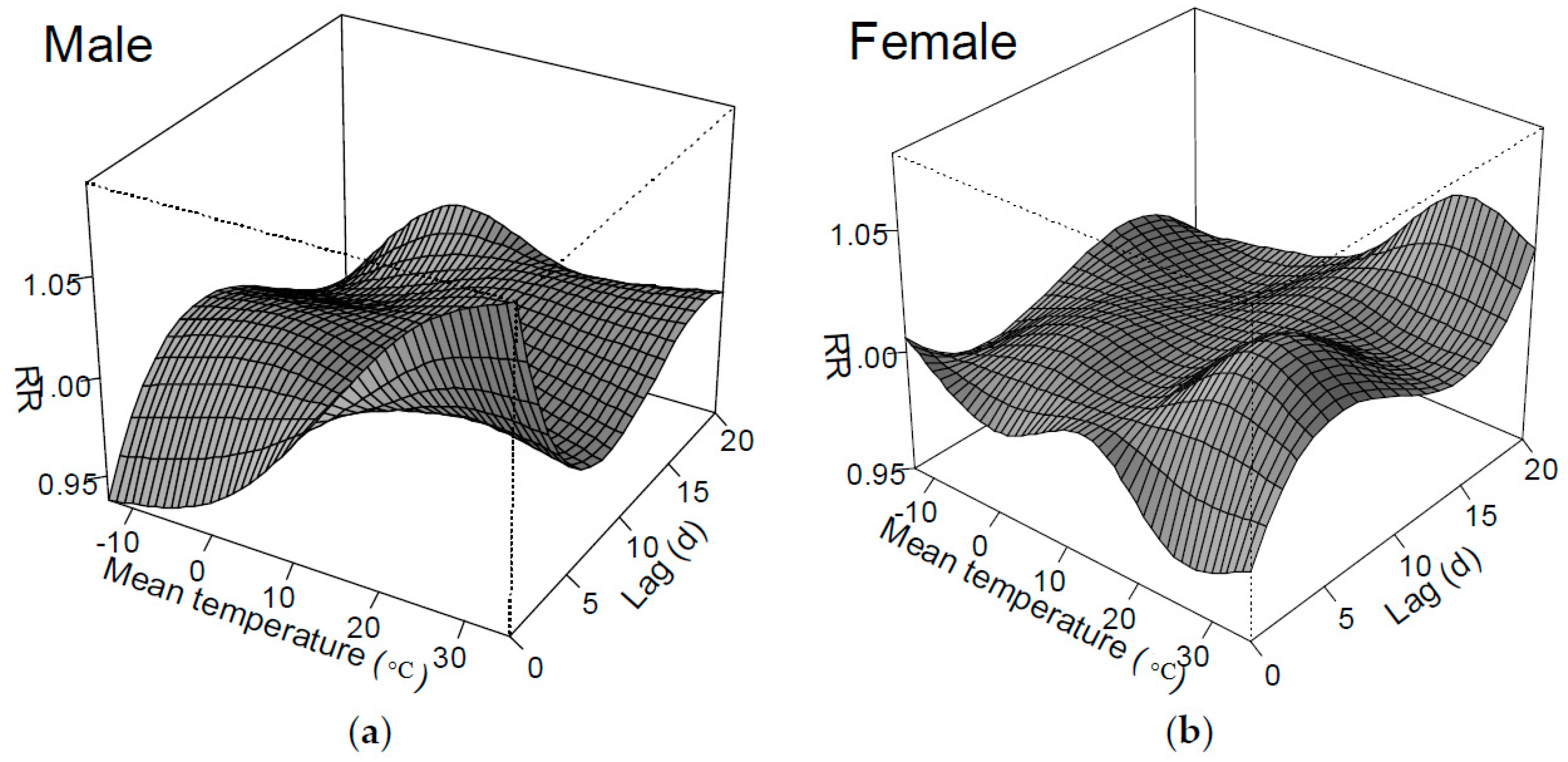
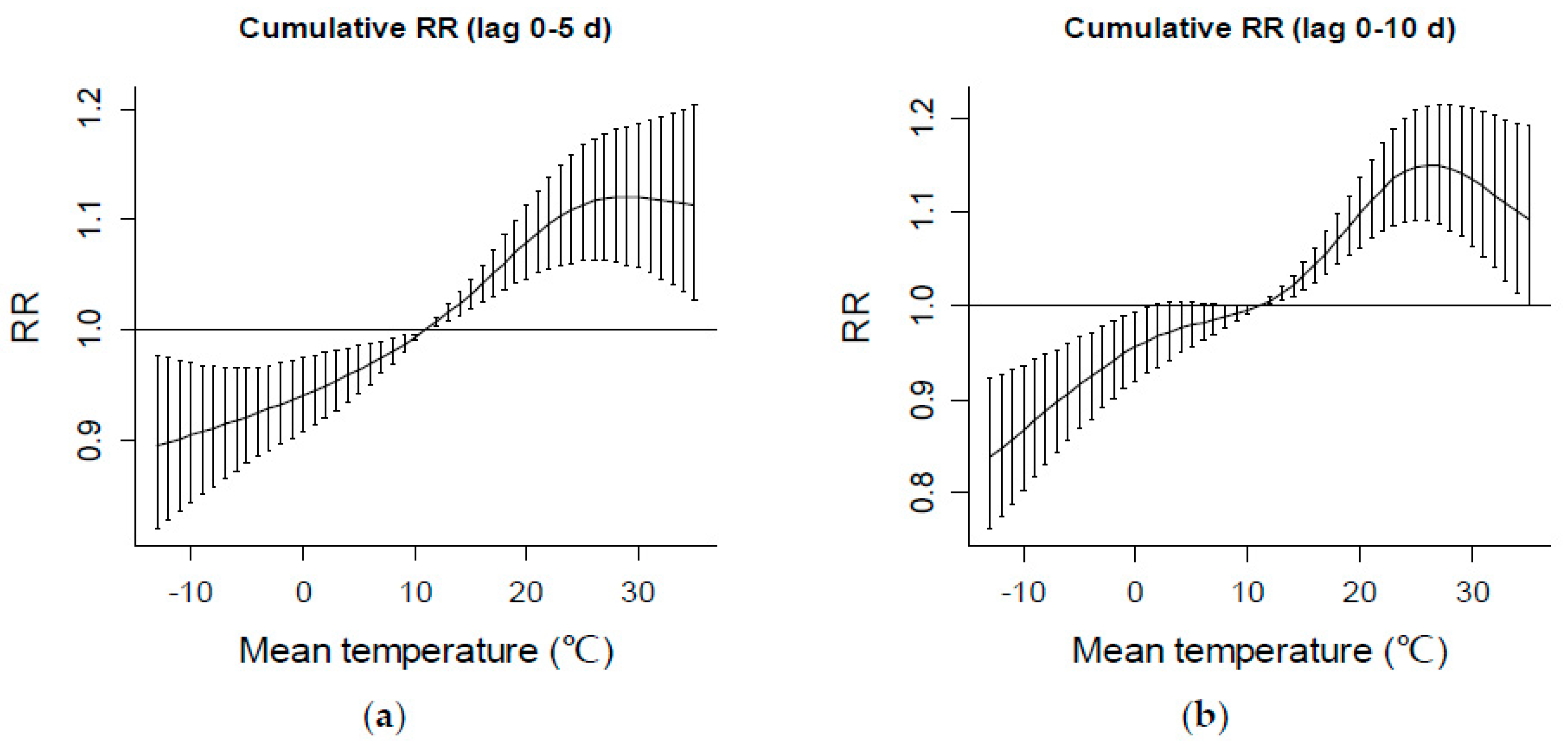
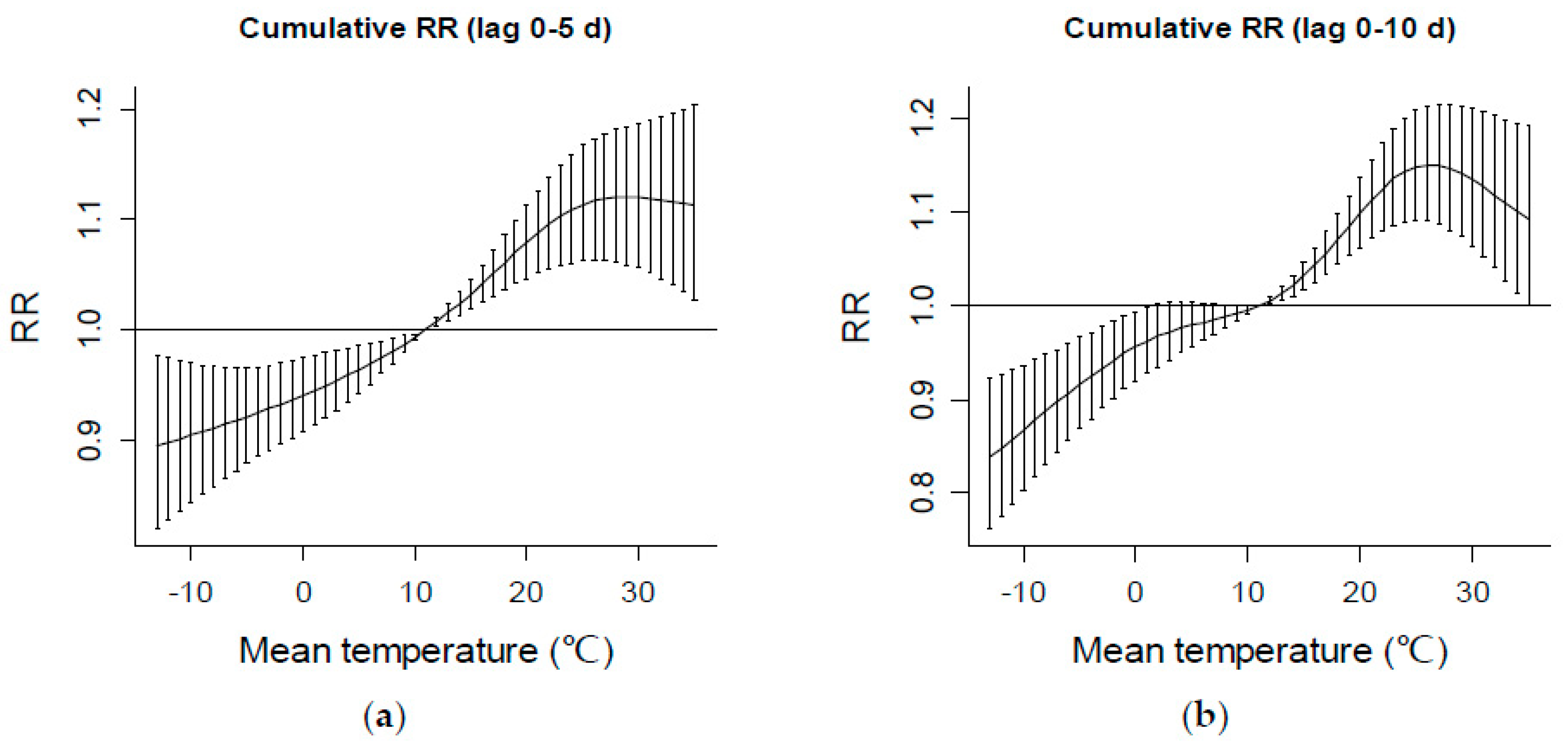
3.3. The Relationship between Temperature and Number of ER Visits
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

References
- Woodward, A.; Smith, K.R.; Campbell-Lendrum, D.; Chadee, D.D.; Honda, Y.; Liu, Q.; Olwoch, J.; Revich, B.; Sauerborn, R.; Chafe, Z.; et al. Climate change and health: On the latest IPCC report. Lancet 2014, 383, 1185–1189. [Google Scholar] [CrossRef]
- Huang, C.; Barnett, A.G.; Wang, X.; Tong, S. The impact of temperature on years of life lost in Brisbane, Australia. Nat. Clim. Chang. 2012, 2, 265–270. [Google Scholar] [CrossRef]
- Hondula, D.M.; Vanos, J.K.; Gosling, S.N. The SSC: A decade of climate-health research and future directions. Int. J. Biometeorol. 2013, 58, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, S.J.; Kovats, R.S.; Armstrong, B.G. Global diarrhoea morbidity, weather and climate. Clim. Res. 2007, 34, 119–127. [Google Scholar] [CrossRef]
- Hanna, A.F.; Yeatts, K.B.; Xiu, A.; Zhu, Z.; Smith, R.L.; Davis, N.N.; Talgo, K.D.; Arora, G.; Robinson, P.J.; Meng, Q.; et al. Associations between ozone and morbidity using the Spatial Synoptic Classification system. Environ. Health 2010, 10, 49. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems; World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- Imre, F.; Balázs, K.P.; Márta, J.; Andrea, F. The air temperature may affect ophthalmologic emergency attendances. Acta Ophthalmol. 2014, 93, e311–e313. [Google Scholar]
- Cashman, J.P.; Green, C.J.; Mcellistrem, B.; Masterson, E.; Condon, F. The effect of inclement weather on trauma orthopaedic workload. Ir. J. Med. Sci. 2011, 180, 679–682. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, T.; Millham, F.H. Relationship between weather and seasonal factors and trauma admission volume at a level I trauma center. J. Trauma Acute Care Surg. 2001, 51, 118–122. [Google Scholar] [CrossRef]
- Atherton, W.G.; Harper, W.M.; Abrams, K.R. A year’s trauma admissions and the effect of the weather. Injury 2005, 36, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Macgregor, D.M. Effect of weather on attendance with injury at a paediatric emergency department. Emerg. Med. J. 2003, 20, 204–205. [Google Scholar] [CrossRef] [PubMed]
- Stomp, W.; Fidler, V.; ten Duis, H.J.; Nijsten, M.W. Relation of the weather and the lunar cycle with the incidence of trauma in the Groningen region over a 36-year period. J. Trauma Acute Care Surg. 2009, 67, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Cervellin, C.; Comelli, I.; Lippi, G.; Comelli, D.; Rastelli, G.; Ossola, P.; Marchesi, C. The number of emergency department visits for psychiatric emergencies is strongly associated with mean temperature and humidity variations. Results of a nine years survey. Emerg. Care J. 2014, 10, 431–435. [Google Scholar] [CrossRef]
- Salib, E.; Gray, N. Weather conditions and fatal self-harm in North Cheshire 1989–1993. Br. J. Psychiatry J. Ment. Sci. 1997, 171, 473–477. [Google Scholar] [CrossRef]
- Burkart, K.; Breitner, S.; Schneider, A.; Khan, M.M.; Krämer, A.; Endlicher, W. An analysis of heat effects in different subpopulations of Bangladesh. Int. J. Biometeorol. 2014, 58, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, B. Models for the relationship between ambient temperature and daily mortality. Epidemiology 2006, 17, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Parsons, K.C. Human Thermal Environments: The Effects of Hot, Moderate, and Cold Environments on Human Health, Comfort and Performance; Taylor & Francis: London, UK; New York, NY, USA, 2003. [Google Scholar]
- Anderson, G.B.; Dominici, F.; Wang, Y.; Mccormack, M.C.; Bell, M.L.; Peng, R.D. Heat-related emergency hospitalizations for respiratory diseases in the medicare population. Am. J. Respir. Crit. Care Med. 2013, 177, 1098–1103. [Google Scholar] [CrossRef] [PubMed]
- Urban, A.; Davídkovová, H.; Kyselý, J. Heat- and cold-stress effects on cardiovascular mortality and morbidity among urban and rural populations in the Czech Republic. Int. J. Biometeorol. 2014, 58, 1057–1068. [Google Scholar] [CrossRef] [PubMed]
- Baccini, M.; Biggeri, A.; Accetta, G.; Kosatsky, T.; Katsouyanni, K.; Analitis, A.; Anderson, H.R.; Bisanti, L.; D’Ippoliti, D.; Danova, J.; et al. Heat effects on mortality in 15 European cities. Epidemiology 2008, 19, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Basu, R. High ambient temperature and mortality: A review of epidemiologic studies from 2001 to 2008. Environ. Health 2009, 8, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Attinger, E.O.; Anne, A.; McDonald, D.A. Use of Fourier series for the analysis of biological systems. Biophys J. 1966, 6, 291. [Google Scholar]
- Zhou, C.F.; Gong, R.Z.; Xiao, G.A. Research on natural disasters loss prediction model based on Fourier series: A case study of Hunan province. China Saf. Sci. J. 2009, 19, 5–9. (In Chinese) [Google Scholar]
- Gasparrini, A.; Armstrong, B. Time series analysis on the health effects of temperature: Advancements and limitations. Environ. Res. 2010, 110, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Barnett, A.G.; Pan, X.; Yu, W.; Tong, S. The impact of temperature on mortality in Tianjin, China: A case-crossover design with a distributed lag nonlinear model. Environ. Health Perspect. 2011, 119, 1719–1725. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A. Distributed lag linear and nonlinear models in R: The package dlnm. J. Stat. Softw. 2011, 43, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Gu, S.; Huang, C.; Bai, L.; Chu, C.; Liu, Q. Heat-related illness in China, summer of 2013. Int. J. Biometeorol. 2016, 60, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Hastie, T.; Tibshirani, R. Generalized additive models for medical research. Stat. Med. 1995, 4, 187–196. [Google Scholar] [CrossRef]
- Zhang, J.; Kai, F.Y. What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA 1998, 280, 1690–1691. [Google Scholar] [CrossRef] [PubMed]
- Rising, W.R.; O’Daniel, J.A.; Roberts, C.S. Correlating weather and trauma admissions at a level I trauma center. J. Trauma Acute Care Surg. 2006, 60, 1096–1100. [Google Scholar] [CrossRef] [PubMed]
- Tomkinson, A.; Bremmer-Smith, A.; Craven, C.; Roblin, D.G. Hospital epistaxis admission rate and ambient temperature. Clin. Otolaryngol. 1995, 20, 239–240. [Google Scholar] [CrossRef] [PubMed]
- Rutkove, S.B.; Do, M.J.K.; Shefner, J.M. Nerve, muscle, and neuromuscular junction electrophysiology at high temperature. Muscle Nerve 1997, 20, 431–436. [Google Scholar] [CrossRef]
- Tham, K.W.; Willem, H.C. Room air temperature affects occupants’ physiology, perceptions and mental alertness. Build. Environ. 2010, 45, 40–44. [Google Scholar] [CrossRef]
- Bazille, C.; Megarbane, B.; Bensimhon, D.; Lavergne-Slove, A.; Baglin, A.C.; Loirat, P.; Woimant, F.; Mikol, J.; Gray, F. Brain damage after heat stroke. J. Neuropathol. Exp. Neurol. 2005, 64, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Li, T.T.; Horton, R.M.; Kinney, P.L. Projections of seasonal patterns in temperature related deaths for Manhattan, New York. Nat. Clim. Chang. 2013, 3, 717–721. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Y.; Barnett, A.G.; Hu, W.; Tong, S. Temperature variation and emergency hospital admissions for stroke in Brisbane, Australia, 1996–2005. Int. J. Biometeorol. 2009, 53, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Xu, X.; Peng, L.; Kan, H. Impact of extreme temperature on hospital admission in Shanghai, China. Sci. Total Environ. 2011, 409, 3634–3637. [Google Scholar] [CrossRef] [PubMed]
- McGeehin, M.A.; Mirabelli, M. The potential impacts of climate variability and change on temperature-related morbidity and mortality in the United States. Environ. Health Perspect. 2001, 109, 185. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Ding, G.; Gu, S.; Bi, P.; Su, B.; Qin, D.; Xu, G.; Liu, Q. The effects of summer temperature and heat waves on heat-related illness in a coastal city of China, 2011–2013. Environ. Res. 2014, 132, 212–219. [Google Scholar] [CrossRef] [PubMed]
- John, L.C.; Charles, W.L., Jr.; Charles, W.L., Jr. Age and sex differences among adolescent participants in nine outdoor recreation activities. Res. Quart. 1979, 50, 589–598. [Google Scholar]
- Nielsen, G.; Pfister, G.; Andersen, L.B. Gender differences in the daily physical activities of Danish school children. Eur. Phys. Educ. Rev. 2011, 17, 69–90. [Google Scholar] [CrossRef]
- Lottrup, L.; Stigsdotter, U.K.; Meilby, H.; Corazon, S.S. Associations between use, activities and characteristics of the outdoor environment at workplaces. Urban For. Urban Green. 2012, 11, 159–168. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean | Standard Deviation | Variance | Minimum | Maximum | Percentile | ||
|---|---|---|---|---|---|---|---|---|
| 25 | 50 | 75 | ||||||
| IPEC-classified ER visits | 170.78 | 39.34 | 1547.75 | 75 | 273 | 141 | 172 | 200 |
| Male | 101.69 | 24.882 | 619.14 | 38 | 179 | 83 | 102 | 120 |
| Female | 69.09 | 17.11 | 292.59 | 26 | 120 | 56 | 68 | 81 |
| Air pressure (hPa) | 1012.38 | 10.25 | 105.0 | 990 | 1037 | 1004.1 | 1011.8 | 1020.6 |
| Temperature (°C) | 13.15 | 11.54 | 133.22 | −13 | 35 | 1.8 | 14.9 | 24.2 |
| Maximum temperature (°C) | 18.3 | 11.74 | 137.76 | −9 | 41 | 7.5 | 20.5 | 29.1 |
| Minimum temperature (°C) | 8.45 | 11.40 | 130.0 | −17 | 29 | −2.2 | 9.4 | 19.2 |
| Wind speed (m/s) | 2.23 | 0.938 | 0.879 | 0 | 6 | 1.5 | 2.1 | 2.7 |
| Sunshine duration (h) | 6.74 | 3.99 | 15.89 | 0 | 14 | 3.6 | 7.7 | 9.8 |
| Daily temperature range (°C) | 9.85 | 3.58 | 12.78 | 1 | 22 | 7.3 | 9.7 | 12.1 |
| Vapor pressure (hPa) | 9.99 | 8.289 | 68.69 | 0 | 33 | 3.1 | 7 | 16.1 |
| Relative humidity (%) | 50.38 | 19.79 | 391.50 | 9 | 92 | 33 | 51 | 67 |
| SO2 (μg/m3) | 30.65 | 30.01 | 900.69 | 4.82 | 201.64 | 10 | 19.1 | 40.09 |
| NO2 (μg/m3) | 54.51 | 23.38 | 546.49 | 9 | 167.36 | 38.89 | 50.09 | 64.41 |
| PM10 (μg/m3) | 116.03 | 76.44 | 5842.4 | 6.4 | 801.55 | 63.86 | 101.91 | 146.95 |
| Pressure (hPa) | Wind Speed (m/s) | Sunshine Duration (Hour) | Relative Humidity (%) | Mean Temperature (°C) | SO2 (μg/m3) | NO2 (μg/m3) | PM10 (μg/m3) | ||
|---|---|---|---|---|---|---|---|---|---|
| All | R | −0.543 ** | −0.059 | 0.114 ** | 0.275 ** | 0.693 ** | −0.528 ** | −0.115 ** | 0.009 |
| P | 0.000 | 0.051 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.764 | |
| Male | R | −0.539 ** | −0.043 | 0.109 ** | 0.262 ** | 0.687 ** | −0.501 ** | −0.104 ** | 0.041 |
| P | 0.000 | 0.151 | 0.000 | 0.000 | 0.000 | 0.000 | 0.001 | 0.180 | |
| Female | R | −0.465 ** | −0.077 * | 0.099 ** | 0.252 ** | 0.594 ** | −0.486 ** | −0.113 ** | −0.035 |
| P | 0.000 | 0.011 | 0.001 | 0.000 | 0.000 | 0.000 | 0.000 | 0.244 | |
| Air Pressure (hPa) | R | - | −0.048 | −0.087 ** | −0.334 ** | −0.858 ** | 0.433 ** | 0.100 ** | −0.246 ** |
| P | - | 0.110 | 0.004 | 0.000 | 0.000 | 0.000 | 0.001 | 0.000 | |
| Wind Speed (m/s) | R | −0.048 | - | 0.321 ** | −0.465 ** | 0.029 | −0.158 ** | −0.446 ** | −0.150 ** |
| P | 0.110 | - | 0.000 | 0.000 | 0.338 | 0.000 | 0.000 | 0.000 | |
| Sunshine Duration (h) | R | −0.087 ** | 0.321 ** | - | −0.590 ** | 0.182 ** | −0.278 ** | −0.297 ** | −0.324 ** |
| P | 0.004 | 0.000 | - | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| Daily Temperature Range (°C) | R | −0.117 ** | −0.033 | 0.643 ** | −0.368 ** | 0.093 ** | 0.028 | 0.122 ** | 0.010 |
| P | 0.000 | 0.274 | 0.000 | 0.000 | 0.002 | 0.359 | 0.000 | 0.749 | |
| Vapor Pressure (hPa) | R | −0.787 ** | −0.181 ** | −0.138 ** | 0.706 ** | 0.900 ** | −0.541 ** | −0.046 | 0.211 ** |
| P | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.126 | 0.000 | |
| Relative Humidity (%) | R | −0.334 ** | −0.465 ** | −0.590 ** | - | 0.346 ** | −0.127 ** | 0.268 ** | 0.309 ** |
| P | 0.000 | 0.000 | 0.000 | - | 0.000 | 0.000 | 0.000 | 0.000 | |
| Mean Temperature (°C) | R | −0.858 ** | 0.029 | 0.182 ** | 0.346 ** | - | −0.633 ** | −0.201 ** | 0.116 ** |
| P | 0.000 | 0.338 | 0.000 | 0.000 | - | 0.000 | 0.000 | 0.000 | |
| Maximum Temperature (°C) | R | −0.858 ** | 0.028 | 0.261 ** | 0.293 ** | 0.987 ** | −0.608 ** | −0.178 ** | 0.118 ** |
| P | 0.000 | 0.356 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| Minimum Temperature (°C) | R | −0.836 ** | 0.024 | 0.045 | 0.437 ** | 0.979 ** | −0.638 ** | −0.211 ** | 0.129 ** |
| P | 0.000 | 0.429 | 0.132 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| SO2 (μg/m3) | R | 0.433 ** | −0.158 ** | −0.278 ** | −0.127 ** | −0.633 ** | - | - | - |
| P | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | - | - | - | |
| NO2 (μg/m3) | R | 0.100 ** | −0.446 ** | −0.297 ** | 0.268 ** | −0.201 ** | 0.617 ** | - | - |
| P | 0.001 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | - | - | |
| PM10 (μg/m3) | R | −0.246 ** | −0.150 ** | −0.324 ** | 0.309 ** | 0.116 ** | 0.457 ** | 0.605 ** | - |
| P | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | - | |
| T Percentiles | Lag 0 d | Lag 2 d | Lag 4 d | Lag 6 d | Lag 8 d |
| 5th (−4.7 °C) | 0.957 (0.935–0.978) | 0.984 (0.975–0.993) | 0.999 (0.991–1.008) | 1.004 (1.001–1.013) | 1.001 (0.999 –1.009) |
| 10th (−2.9 °C) | 0.956 (0.936–0.976) | 0.985 (0.978–0.993) | 1.001 (0.994–1.009) | 1.007 (0.998–1.015) | 1.004 (0.996–1.012) |
| 25th (1.8 °C) | 0.960 (0.950–0.980) | 0.989 (0.985–0.996) | 1.004 (0.998–1.009) | 1.009 (1.002–1.015) | 1.006 (1.000–1.011) |
| 14 °C | 1.003 (1.002–1.004) | 1.001 (1.001–1.002) | 1.000 (1.000–1.001) | 1.000 (1.000–1.001) | 1.000 (1.000–1.000) |
| 50th (14.9 °C) | 1.006 (1.004–1.009) | 1.003 (1.002–1.004) | 1.001 (1.000–1.002) | 1.000 (0.999–1.002) | 1.000 (0.999–1.001) |
| 75th (24.2 °C) | 1.022 (1.005–1.039) | 1.021 (1.014–1.027) | 1.017 (1.011–1.023) | 1.013 (1.006–1.019) | 1.007 (1.002–1.013) |
| 90th (27.2 °C) | 1.025 (1.006–1.045) | 1.023 (1.015–1.030) | 1.018 (1.012–1.025) | 1.013 (1.005–1.020) | 1.007 (1.000–1.013) |
| 95th (28.7 °C) | 1.026 (1.005–1.048) | 1.023 (1.014–1.031) | 1.017 (1.010–1.024) | 1.011 (1.003–1.019) | 1.005 (0.998–1.012) |
| Tmax/Percentiles | Lag 0 d | Lag 2 d | Lag 4 d | Lag 6 d | Lag 8 d |
| 5th (−3 °C) | 0.969 (0.939–1.001) | 0.981 (0.972–0.991) | 0.992 (0.980–1.004) | 0.999 (0.990–1.008) | 1.001 (0.992–1.009) |
| 10th (1.76 °C) | 0.966 (0.941–0.991) | 0.983 (0.975–0.986) | 0.997 (0.987–1.008) | 1.006 (0.999–1.014) | 1.008 (1.001–1.015) |
| 25th (7.5 °C) | 0.970 (0.950–0.990) | 0.986 (0.970–0.993) | 1.001 (0.992–1.009) | 1.009 (1.002–1.015) | 1.010 (1.005 –1.016) |
| 50th (20.5 °C) | 1.006 (1.003–1.009) | 1.003 (1.002–1.004) | 1.001 (1.000–1.002) | 1.000 (0.999–1.001) | 1.000 (0.999–1.001) |
| 75th (29.1 °C) | 1.030 (1.009–1.052) | 1.017 (1.010–1.024) | 1.012 (1.003–1.020) | 1.010 (1.004–1.016) | 1.009 (1.004–1.015) |
| 90th (32.4 °C) | 1.033 (1.009–1.057) | 1.019 (1.011–1.027) | 1.013 (1.004–1.021) | 1.011 (1.004–1.012) | 1.009 (1.003–1.010) |
| 95th (34.2 °C) | 1.032 (1.007–1.058) | 1.019 (1.011–1.027) | 1.012 (1.003–1.022) | 1.010 (1.002–1.017) | 1.008 (1.001–1.014) |
| Tmin/Percentiles | Lag 0 d | Lag 2 d | Lag 4 d | Lag 6 d | Lag 8 d |
| 5th (−9.2 °C) | 0.964 (0.933–0.996) | 0.982 (0.972–0.993) | 0.990 (0.977–1.004) | 0.992 (0.981–1.002) | 0.989 (0.979–0.999) |
| 10th (−6.7 °C) | 0.975 (0.948–1.004) | 0.985 (0.968–0.994) | 0.992 (0.976–0.995) | 0.995 (0.978–1.000) | 0.993 (0.981–1.004) |
| 25th (−2.2 °C) | 0.988 (0.966–1.011) | 0.990 (0.978–0.999) | 0.994 (0.982–0.998) | 0.998 (0.983–1.001) | 0.998 (0.985–1.004) |
| 50th (9.4 °C) | 1.001 (1.000–1.002) | 1.001 (1.000–1.001) | 1.000 (1.000–1.001) | 1.000 (1.000–1.001) | 1.000 (1.000–1.001) |
| 75th (19.2 °C) | 1.038 (1.016–1.061) | 1.017 (1.014–1.036) | 1.011 (1.010–1.024) | 1.010 (1.005–1.020) | 1.010 (1.002–1.019) |
| 90th (23.14 °C) | 1.045 (1.016–1.075) | 1.016 (1.013–1.041) | 1.008 (1.007–1.025) | 1.008 (1.000–1.020) | 1.009 (0.998–1.018) |
| 95th (24.4 °C) | 1.045 (1.014–1.077) | 1.015 (1.011–1.042) | 1.007 (1.005–1.025) | 1.007 (0.998–1.020) | 1.009 (0.996–1.018) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, P.; Wang, S.; Fan, X.; Li, T. The Impacts of Air Temperature on Accidental Casualties in Beijing, China. Int. J. Environ. Res. Public Health 2016, 13, 1073. https://doi.org/10.3390/ijerph13111073
Ma P, Wang S, Fan X, Li T. The Impacts of Air Temperature on Accidental Casualties in Beijing, China. International Journal of Environmental Research and Public Health. 2016; 13(11):1073. https://doi.org/10.3390/ijerph13111073
Chicago/Turabian StyleMa, Pan, Shigong Wang, Xingang Fan, and Tanshi Li. 2016. "The Impacts of Air Temperature on Accidental Casualties in Beijing, China" International Journal of Environmental Research and Public Health 13, no. 11: 1073. https://doi.org/10.3390/ijerph13111073
APA StyleMa, P., Wang, S., Fan, X., & Li, T. (2016). The Impacts of Air Temperature on Accidental Casualties in Beijing, China. International Journal of Environmental Research and Public Health, 13(11), 1073. https://doi.org/10.3390/ijerph13111073