
The Influence of Urbanization Modes on the Spatial Circulation of Flaviviruses within Ouagadougou (Burkina Faso)

 , ,
, ,
Abstract
:1. Introduction
2. Methods
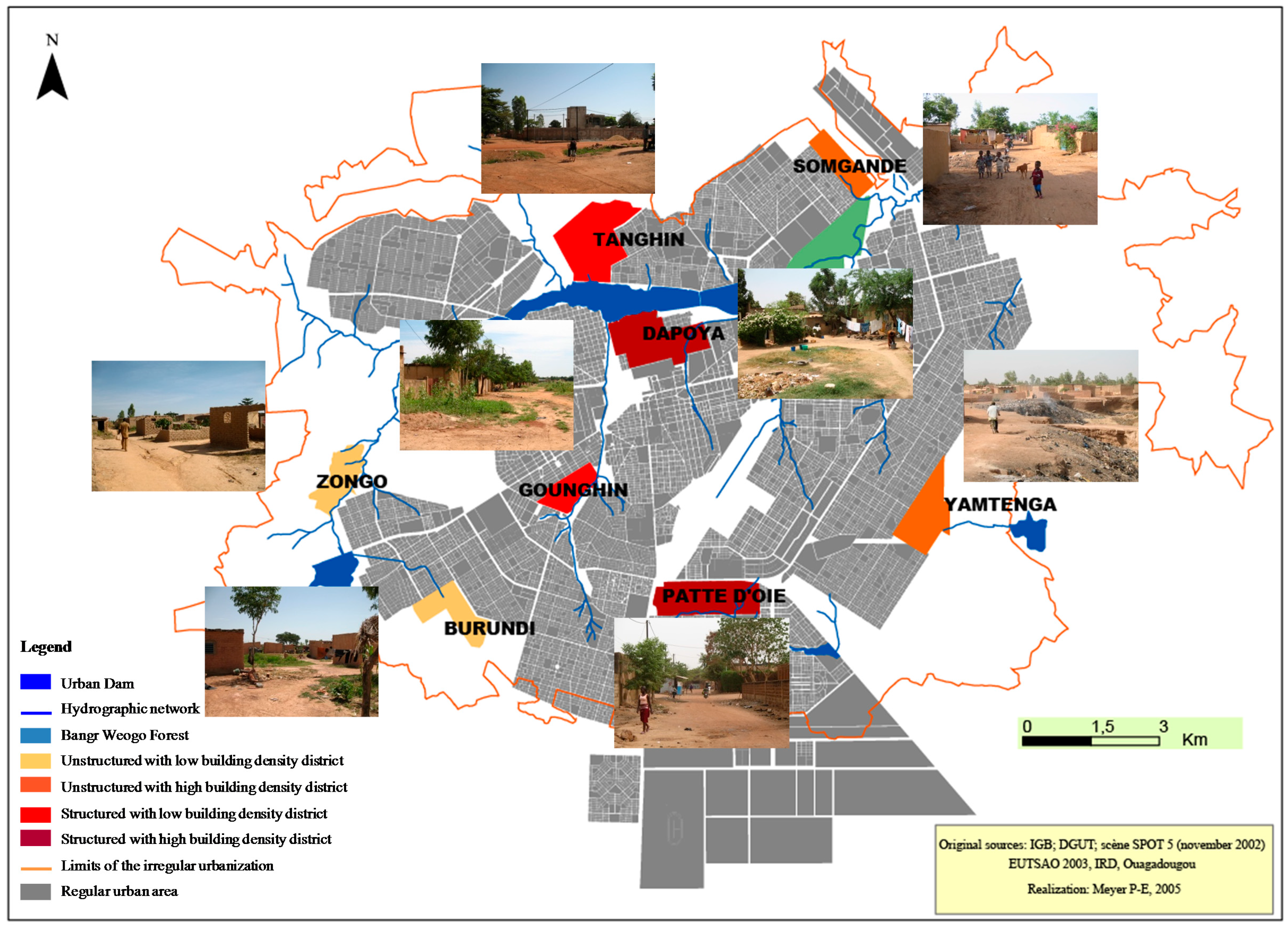
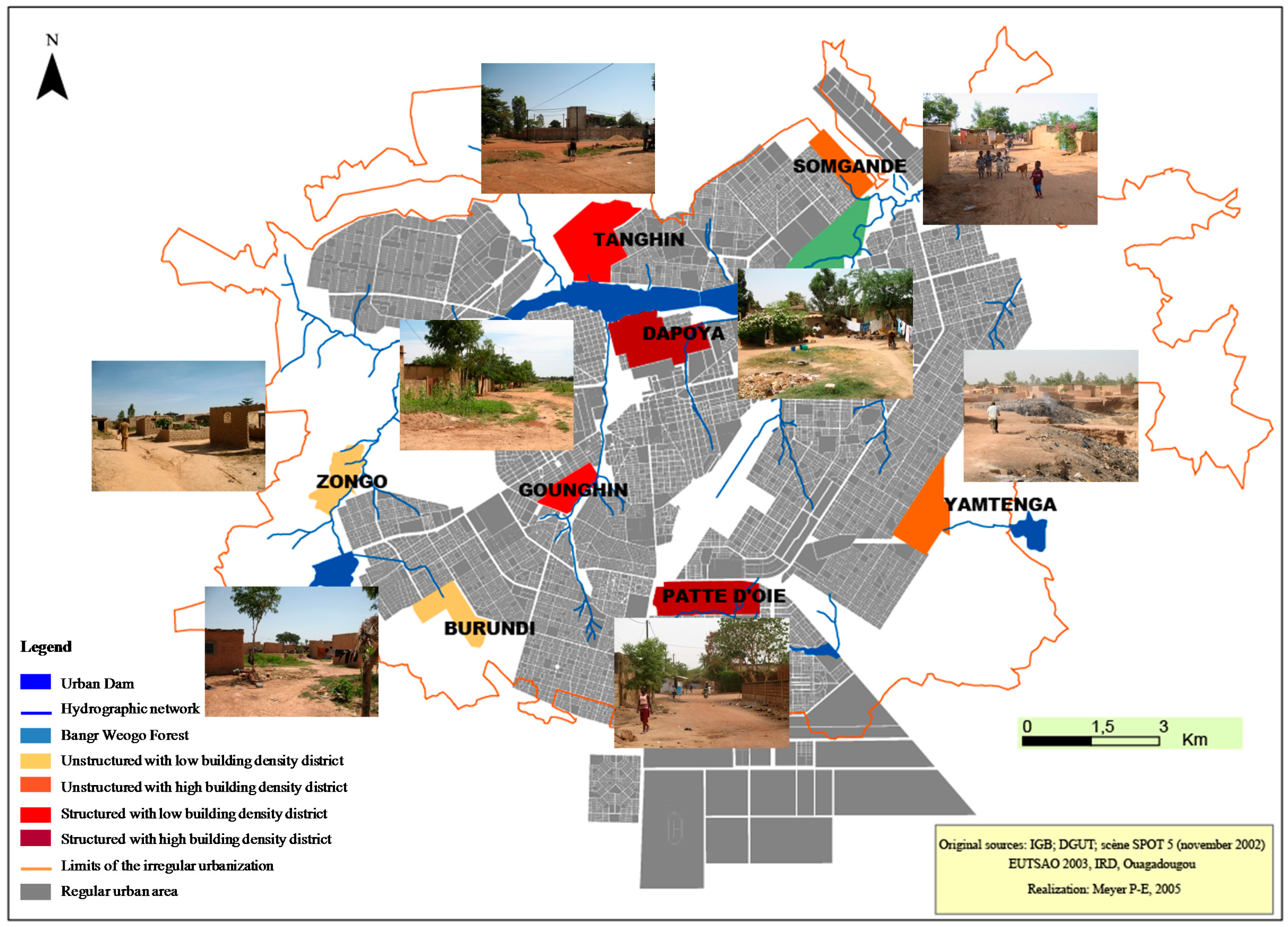
2.1. Study Area
2.2. Sampling Strategy
2.3. Sample Design and Studied Population
2.4. Data Collection
2.5. Laboratory Analysis
2.6. Statistical Analysis
2.7. Ethics
3. Results
3.1. Anti-Flavivirus Antibody Seroprevalence
3.2. Individual and Environmental Factors Associated with Flavivirus Seroprevalence
4. Discussion
5. Limitations of the Study
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Downs, W.G. Malaria: The Great Umbrella. Bull. N. Y. Acad. Med. 1975, 51, 984–990. [Google Scholar] [PubMed]
- Franco, L.; Di Caro, A.; Carletti, F.; Vapalahti, O.; Renaudat, C.; Zeller, H.; Tenorio, A. Recent expansion of dengue virus serotype 3 in West Africa. Eurosurveillance 2010, 15, 5–8. [Google Scholar]
- Jentes, E.S.; Robinson, J.; Johnson, B.W.; Conde, I.; Sakouvougui, Y.; Iverson, J.; Beecher, S.; Bah, M.A.; Diakite, F.; Coulibaly, M.; et al. Acute Arboviral Infections in Guinea, West Africa, 2006. Am. J. Trop. Med. Hyg. 2010, 83, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Stoler, J.; al Dashti, R.; Anto, F.; Fobil, J.N.; Gordon, A.; Awandare, G.A. Deconstructing “malaria”: West Africa as the next front for dengue fever surveillance and control. Acta Trop. 2014, 134, 58–65. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Yellow fever surveillance and outbreak response: Revision of case definitions, October 2010. Wkly. Epidemiol. Rec. 2010, 19, 465–472. [Google Scholar]
- World Health Organization. Yellow fever in the WHO African and American Regions. Wkly. Epidemiol. Rec. 2010, 34, 365–376. [Google Scholar]
- World Health Organization. DengueNet: Global Surveillance of Dengue and Dengue Haemorrhagic Fever; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Département International, Institut de Veille Sanitaire (InVS). Bilan Epidémiologique et Grande Tendance, Dengue; InVS: Saint-Maurice Cedex, France, 2011. [Google Scholar]
- Ridde, V.; Agier, I.; Bonnet, E.; Carabali, M.; Dabire, K.R.; Fournet, F.; Ly, A.; Meda, I.B.; Parra, B. Presence of three dengue serotypes in Ouagadougou (Burkina Faso): Research and public health implications. Infect. Dis. Poverty 2016, 5, 23. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Dengue in Africa: Emergence of DENV-3, Côte d’Ivoire, 2008. Wkly. Epidemiol. Rec. 2009, 84, 85–88. [Google Scholar]
- Higa, Y. Dengue Vectors and their Spatial Distribution. Trop. Med. Health 2011, 39, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, J.P.; Du Saussay, C.; Gautun, J.C.; McCormick, J.B.; Mouchet, J. La dengue au Burkina Faso (ex Haute-Volta): Epidémies saisonnières en milieu urbain à Ouagadougou. Bull. Soc. Pathol. Exot. 1985, 78, 7–14. [Google Scholar]
- Yaro, S.; Zango, A.; Rouamba, J.; Diabaté, A.; Dabiré, R.; Kambiré, C.; Tiendrebeogo, S.M.R.; Yonli, T.; Ouango, J.G.; Diagbouga, S.P. Situation épidémiologique de la fièvre jaune au Burkina Faso de 2003 à 2008. Bull. Soc. Pathol. Exot. 2010, 103, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Niakara, A.; Fournet, F.; Gary, J.; Harang, M.; Nebie, L.V.A.; Salem, G. Hypertension, urbanization, social and spatial disparities: A cross-sectional population-based survey in a West African urban environment (Ouagadougou, Burkina Faso). Trans. R. Soc. Trop. Med. Hyg. 2007, 101, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Ouedraogo, H.Z.; Fournet, F.; Martin-Prével, Y.; Gary, J.; Henry, M.C.; Salem, G. Socio-spatial disparities of obesity among adults in the urban setting of Ouagadougou, Burkina Faso. Public Health Nutr. 2008, 11, 1280–1287. [Google Scholar] [CrossRef] [PubMed]
- Baragatti, M.; Fournet, F.; Henry, M.C.; Assi, S.; Ouedraogo, H.; Rogier, C.; Salem, G. Social and environmental malaria risk factors in urban areas of Ouagadougou, Burkina Faso. Malar. J. 2009, 8, 13. [Google Scholar] [CrossRef] [PubMed]
- United Nations Population Fund. State of World Population 2009. Facing a Changing World: Women, Population and Climate; United Nations Population Fund: New York, NY, USA, 2009. [Google Scholar]
- Institut National de la Statistique et de la Démographie (INSD). Analyse des Résultats du Recensement Général de la Population et de l’Habitation de 1996; INSD: Ouagadougou, Burkina Faso, 2000. [Google Scholar]
- Fournet, F.; Meunier-Nikiema, A.; Salem, G. Ouagadougou: Des Processus D’urbanisation Aux Inégalités Spatiales, Géographie D’une Capitale; Collection Petits Atlas Urbains, IRD: Paris, France, 2008. [Google Scholar]
- Dos Santos, S. Accès à l’eau et enjeu socio-sanitaire à Ouagadougou. Espace Popul. Soc. 2006, 2–3, 271–285. [Google Scholar] [CrossRef]
- Vallée, J.; Fournet, F.; Meyer, P.E.; Harang, M.; Pirot, F.; Salem, G. Stratification de la ville de Ouagadougou (Burkina Faso) à partir d’une image panchromatique Spot 5: Une première étape à la mise en place d’une enquête de santé. Espace Popul. Soc. 2007, 2–3, 393–401. [Google Scholar] [CrossRef]
- Sobngwi, E.; Mbanya, J.C.; Unwin, N.C.; Porcher, R.; Kengne, A.P.; Fezeu, L.; Minkoulou, E.M.; Tournoux, C.; Gautier, J.F.; Aspray, T.J.; et al. Exposure over the life course to an urban environment and its relation with obesity, diabetes, and hypertension in rural and urban Cameroon. Int. J. Epidemiol. 2004, 33, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Seubsman, S.; Sleigh, A.; The Thai Cohort Study Team. Timing of Urbanisation and Cardiovascular Risks in Thailand: Evidence from 51,936 Members of the Thai Cohort Study, 2005–2009. J. Epidemiol. 2014, 24, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, M.G.; Costa, M.C.; Coelho, G.; Barreto, M.L. Recent shift in age pattern of dengue hemorrhagic fever, Brazil. Emerg. Infect. Dis. 2008, 14, 1663. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.P.; Cubitt, W.D. The use of the dried blood spot sample in epidemiological studies. J. Clin. Pathol. 1999, 52, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Kuno, G.; Gomez, I.; Gubler, D.J. An ELISA procedure for the diagnosis of dengue infections. J. Virol. Methods 1991, 33, 101–113. [Google Scholar] [CrossRef]
- Tuntaparsat, W.; Barbazan, P.; Nitatpattana, N.; Rongsryam, Y.; Yoksan, S.; Gonzalez, J.P. Seroepidemiological survey among schoolchildren during the 2000–2001 dengue outbreak of Ratchaburi Province, Thailand. Southeast Asian J. Trop. Med. Public Health 2003, 34, 564–568. [Google Scholar]
- Hosmer, D.; Lemeshow, S. Applied Logistic Regression; Wiley Interscience: New York, NY, USA, 2000. [Google Scholar]
- Meunier-Nikiema, A. Géographie d’une ville à travers la gestion des déchets: Ouagadougou (Burkina Faso). Mappemonde 2007, 87, 1–15. [Google Scholar]
- Demanou, M.; Grandadam, M.; Rogier, C.; Tolou, H.; Hervé, J.-P.; Paupy, C.; Rousset, D. Séroprévalence de la dengue en milieu urbain au Cameroun. Méd. Trop. 2009, 69, 363–364. [Google Scholar]
- Reiskind, M.H.; Baisley, K.J.; Calampa, C.; Sharp, T.W.; Watts, D.M.; Wilson, M.L. Epidemiological and ecological characteristics of past dengue virus infection in Santa Clara, Peru. Trop. Med. Int. Health 2001, 6, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Guha-Sapir, D.; Schimmer, B. Dengue fever: New paradigms for a changing epidemiology. Emerg. Themes Epidemiol. 2005, 2, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilon, M.; Wayack, M. La démocratisation de l’enseignement au Burkina Faso: Que peut-on en dire aujourd’hui? Cah. d’Études Afr. 2003, 43, 63–86. [Google Scholar] [CrossRef]
- Grossman, M. The correlation between health and education. In Household Production and Consumption; Terleckyj, N., Ed.; Columbia University Press: New York, NY, USA, 1975. [Google Scholar]
- Bartley, L.M.; Carabin, H.; Vinh Chau, N.; Ho, V.; Luxemburger, C.; Hien, T.T.; Garnett, G.P.; Farrar, J. Assessment of the factors associated with flavirus seroprevalence in a population in Southern Vietnam. Epidemiol. Infect. 2002, 128, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Christophers, S.R. Aedes aegypti (L.) the Yellow Fever Mosquito. Its Life History Bionomics and Structure; Cambridge University Press: London, UK, 1960. [Google Scholar]
- Gubler, D.J.; Clark, G.G. Dengue/dengue hemorrhagic fever: The emergence of a global health problem. Emerg. Infect. Dis. 1995, 1, 55–57. [Google Scholar] [CrossRef] [PubMed]
- Déverin-Kouanda, Y. De la fertilité rurale a la nuisance urbaine. Les difficiles variations culturelles du Tampuure (tas d’ordures) en pays Mossi (Région de Ouagadougou-Burkina Faso). Géogr. Cult. 1993, 6, 121–134. [Google Scholar]
- Arunachalam, N.; Tana, S.; Espino, F.; Kittayapong, P.; Abeyewickreme, W.; Wai, K.T.; Tyagi, B.K.; Kroeger, A.; Sommerfeld, J.; Petzold, M. Eco-bio-social determinants of dengue vector breeding: A multicountry study in urban and periurban Asia. Bull. World Health Organ. 2010, 88, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Kamgang, B.; Happi, J.Y.; Boisier, P.; Njiokou, F.; Hervé, J.P.; Simard, F.; Paupy, C. Geographic and ecological distribution of the dengue and chikungunya virus vectors Aedes aegypti and Aedes albopictus in three major Cameroonian towns. Med. Vet. Entomol. 2010, 24, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.; Grillet, M.E.; Ramos, O.M.; Amador, M.; Barrera, R. Habitat segregation of dengue vectors along an urban environmental gradient. Am. J. Trop. Med. Hyg. 2007, 76, 820–826. [Google Scholar] [PubMed]
- Braks, M.A.; Honorio, N.A.; Lourenco-De-Oliveira, R.; Juliano, S.A.; Lounibos, L.P. Convergent habitat segregation of Aedes aegypti and Aedes albopictus (Diptera: Culicidae) in southeastern Brazil and Florida. J. Med. Entomol. 2003, 40, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Carbajo, A.E.; Curto, S.I.; Schweigmann, N.J. Spatial distribution pattern of oviposition in the mosquito Aedes aegypti in relation to urbanization in Buenos Aires: Southern fringe bionomics of an introduced vector. Med. Vet. Entomol. 2006, 20, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Hayes, E.B. Zika virus outside Africa. Emerg. Infect. Dis. 2009, 15, 1347–1350. [Google Scholar] [CrossRef] [PubMed]
- Institut de Veille Sanitaire (InVS). Bulletin Hebdomadaire International N°151 6–12 Août 2008; InVS: Saint-Maurice Cedex, France, 2008; p. 4. [Google Scholar]
- Russell, P.K.; Nisalak, A.; Sukhavachana, P.; Vivona, S. A plaque reduction test for dengue virus neutralizing antibodies. J. Immunol. 1967, 99, 285–290. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Variable | UHBD | ULBD | SHBD | SLBD | Total | |
|---|---|---|---|---|---|---|---|
| Child | Sex | Male | 448 (51.2) * | 422 (51.3) | 286 (49.1) | 351 (47.8) | 1485 (49.3) |
| Female | 427 (48.8) | 400 (48.7) | 297 (50.9) | 384 (52.2) | 1530 (50.7) | ||
| Age | 0–4 years | 328 (37.5) | 296 (36.0) | 207 (35.5) | 230 (31.3) | 1061 (35.2) | |
| 4–10 years | 434 (49.6) | 406 (49.4) | 266 (45.6) | 367 (49.9) | 1473 (48.9) | ||
| 10–12 years | 113 (12.9) | 120 (14.6) | 110 (18.9) | 138 (18.8) | 481 (16.0) | ||
| Householder | Householder Education | Yes | 359 (41.0) | 427 (51.9) | 363 (62.3) | 343 (46.7) | 1492 (49.5) |
| No | 516 (59.0) | 395 (48.1) | 220 (37.7) | 392 (53.3) | 1523 (50.5) | ||
| Socioeconomic level | Low | 656 (75.0) | 603 (73.4) | 190 (32.6) | 373 (50.7) | 1822 (60.0) | |
| Medium | 187 (21.4) | 197 (24.0) | 103 (17.7) | 200 (27.2) | 687 (23.0) | ||
| High | 32 (3.6) | 22 (2.6) | 290 (49.7) | 162 (22.1) | 506 (17.0) | ||
| Environment | Waste management | Improper | 281 (32.1) | 304 (37.0) | 103 (17.7) | 302 (41.1) | 1517 (50.3) |
| Adequate | 594 (67.9) | 518 (63.0) | 480 (82.3) | 433 (58.9) | 1498 (49.7) | ||
| Water supply | Tap | 37 (4.2) | 17 (2.1) | 331 (56.8) | 240 (32.6) | 625 (20.7) | |
| Pump | 766 (87.5) | 639 (77.7) | 240 (41.2) | 465 (63.3) | 2110 (70.0) | ||
| Well | 72 (8.3) | 166 (20.2) | 12 (2.0) | 30 (4.1) | 280 (9.3) | ||
| House appearance | Good | 162 (18.5) | 347 (42.2) | 229 (39.3) | 170 (23.1) | 908 (30.1) | |
| Not good | 713 (81.5) | 475 (57.8) | 354 (60.7) | 565 (76.9) | 2107 (69.9) | ||
| Total | 875 | 822 | 583 | 735 | 3015 | ||
| Independent Variables | %FLAV IgG + (95% CI) | p | |
|---|---|---|---|
| Sex * | Male | 20.7 (22.4–26.7) | 0.015 |
| Female | 24.4 (18.7–22.8) | ||
| Age * | 0–4 years | 11.8 (9.8–13.7) | <0.001 |
| 4–10 years | 25.9 (23.7–28.2) | ||
| 10–12 years | 36.4 (32.3–40.9) | ||
| Education of the householder * | Yes | 21.6 (19.5–23.7) | 0.15 |
| No | 24.3 (22.0–26.6) | ||
| Duration of residence of the householder | <10 years | 27.4 (21.6–33.3) | 0.41 |
| 10 to 20 years | 22.6 (19.4–25.7) | ||
| ≥20 years | 22.2 (20.4–23.9) | ||
| Socioeconomic level * | Low | 22.4 (20.5–24.4) | 0.003 |
| Medium | 26.5 (23.2–29.8) | ||
| High | 18.2 (14.8–21.5) | ||
| Water supply * | Tap | 22.2 (19.0–25.5) | 0.03 |
| Pump | 21.9 (20.2–23.7) | ||
| Well | 28.9 (23.6–34.2) | ||
| Waste management * | Improper | 24.1 (22.0–26.3) | 0.05 |
| Adequate | 21.2 (19.1–23.2) | ||
| House appearance * | Good | 24.4 (20.1–23.6) | 0.12 |
| Not good | 21.9 (21.7–27.2) | ||
| Strata | UHBD | 20.2 (17.6–22.9) | <0.001 |
| ULBD | 25.0 (22.1–28.0) | ||
| SHBD | 16.8 (13.6–19.7) | ||
| SLBD | 27.8 (24.4–30.9) | ||
| Districts | Somgandé | 29.7 (25.2–34.3) | <0.001 |
| Yamtenga | 12.7 (9.6–15.5) | ||
| Zongo | 31.2 (26.6–35.5) | ||
| Pissy | 18.8 (15.2–22.8) | ||
| Dapoya | 15.5 (11.7–19.5) | ||
| Patte d’Oie | 18.4 (13.3–22.7) | ||
| Gounghin | 37.3 (31.7–42.1) | ||
| Tanghin | 19.9 (15.9–23.7) | ||
| Building density | High | 18.9 (16.8–20.8) | <0.001 |
| Low | 26.3 (24.1–28.5) | ||
| Area structuration | Yes | 23.1 (20.5–25.0) | 0.97 |
| No | 22.5 (20.6–24.6) | ||
| Total | 22.7 (21.2–24.1) | ||
| Variables | UHBD | ULBD | SHBD | SLBD | |
|---|---|---|---|---|---|
| Age | 0–4 years | 1 | 1 | 1 | 1 |
| 4–10 years | 6.52 (3.85–11.01) *** | 2.64 (1.76–3.96) *** | 1.91 (1.10–3.31) ** | 1.64 (1.10–2.45) *** | |
| 10–12 years | 11.09 (5.97–20.58) *** | 5.52 (3.32–9.18) *** | 2.72 (1.45–5.11) *** | 2.71 (1.69–4.38) *** | |
| Sex | Male | 1 | 1 | 1 | 1 |
| Female | 0.92 (0.64–1.30) | 1.19 (0.85–1.67) | 1.83 (1.15–2.90) * | 1.25 (0.90–1.74) | |
| Education of the householder | Yes | 1 | 1 | 1 | 1 |
| No | 1.39 (0.95–2.01) | 1.44 (1.01–2.05) ** | 1.17 (0.71–1.92) | 1.23 (0.88–1.71) | |
| Socioeconomic level | High | 1 | 1 | 1 | 1 |
| Medium | 0.64 (0.24–1.66) | 1.65 (0.49–5.53) | 1.83 (0.99–3.39) * | 2.01 (1.21–3.33) ** | |
| Low | 0.47 (0.19–1.18) | 1.03 (0.39–4.31) | 1.20 (0.65–2.21) | 1.50 (0.91–2.47) | |
| Water supply | Tap | 1 | 1 | 1 | 1 |
| Pump | 0.55 (0.25–1.22) | 7.39 (0.93–58.07) * | 0.76 (0.45–1.32) | 0.84 (0.57–1.24) | |
| Well | 0.84 (0.32–2.23) | 10.27 (1.28–82.41) ** | 1.34 (0.31–5.75) | 1.22 (0.52–2.83) | |
| Waste management | Adequate | 1 | 1 | 1 | 1 |
| Improper | 1.56 (1.05–2.34) * | 1.17 (0.82–1.66) | 1.92 (1.11–3.34) ** | 0.90 (0.62–1.30) | |
| House appearance | Good | 1 | 1 | 1 | 1 |
| Not good | 0.79 (0.49–1.29) | 2.16 (1.53–3.04) *** | 0.56 (0.45–1.45) | 1.02 (0.68–1.53) | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fournet, F.; Rican, S.; Vaillant, Z.; Roudot, A.; Meunier-Nikiema, A.; Kassié, D.; Dabiré, R.K.; Salem, G. The Influence of Urbanization Modes on the Spatial Circulation of Flaviviruses within Ouagadougou (Burkina Faso). Int. J. Environ. Res. Public Health 2016, 13, 1226. https://doi.org/10.3390/ijerph13121226
Fournet F, Rican S, Vaillant Z, Roudot A, Meunier-Nikiema A, Kassié D, Dabiré RK, Salem G. The Influence of Urbanization Modes on the Spatial Circulation of Flaviviruses within Ouagadougou (Burkina Faso). International Journal of Environmental Research and Public Health. 2016; 13(12):1226. https://doi.org/10.3390/ijerph13121226
Chicago/Turabian StyleFournet, Florence, Stéphane Rican, Zoé Vaillant, Anna Roudot, Aude Meunier-Nikiema, Daouda Kassié, Roch K. Dabiré, and Gérard Salem. 2016. "The Influence of Urbanization Modes on the Spatial Circulation of Flaviviruses within Ouagadougou (Burkina Faso)" International Journal of Environmental Research and Public Health 13, no. 12: 1226. https://doi.org/10.3390/ijerph13121226