
Health Profile of Construction Workers in Hong Kong



Abstract
:1. Introduction
2. Participants and Methods
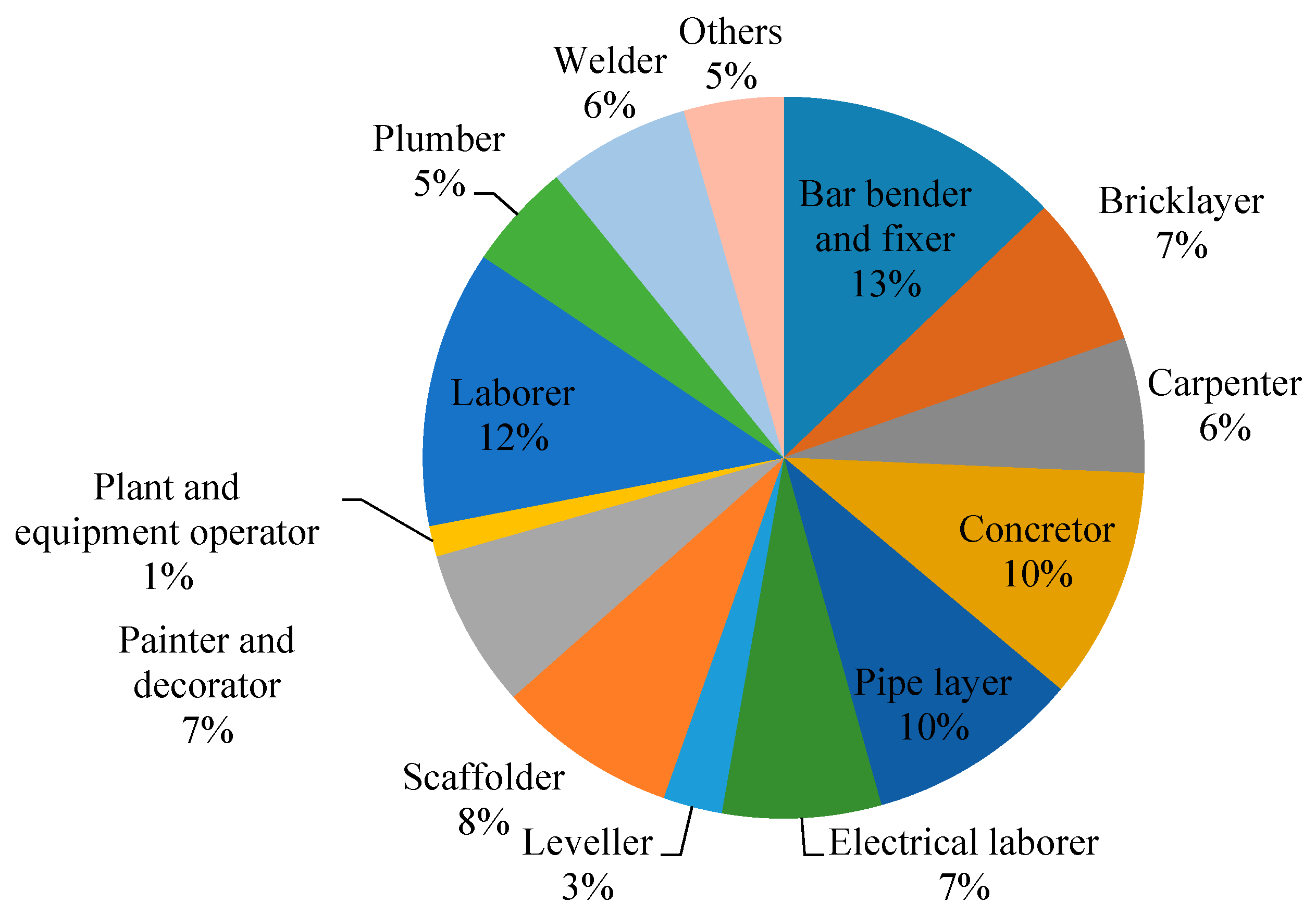
2.1. Participants
2.2. Individual Characteristics and Work-Related Factors
2.3. Clinical Examination
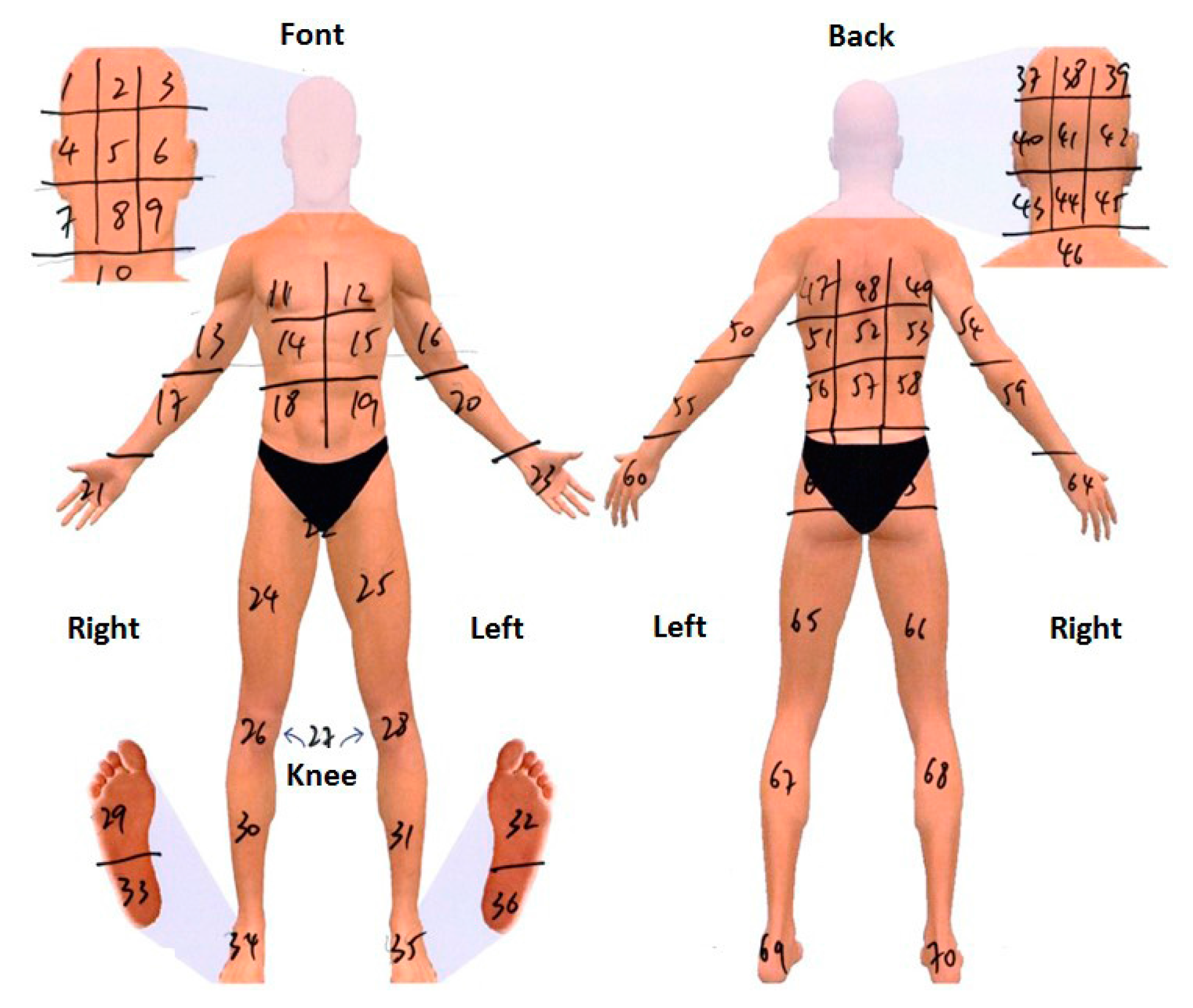
2.4. Musculoskeletal Pain Assessment
2.5. Statistical Analysis
3. Results
3.1. Demographic Details
3.2. Health Condition
3.2.1. Blood Pressure and RHR
3.2.2. Blood Glucose
3.2.3. Liver Function
3.2.4. Urea
3.2.5. Cholesterol
3.2.6. Uric Acid
3.3. Musculoskeletal Pain
3.3.1. Pain Experience
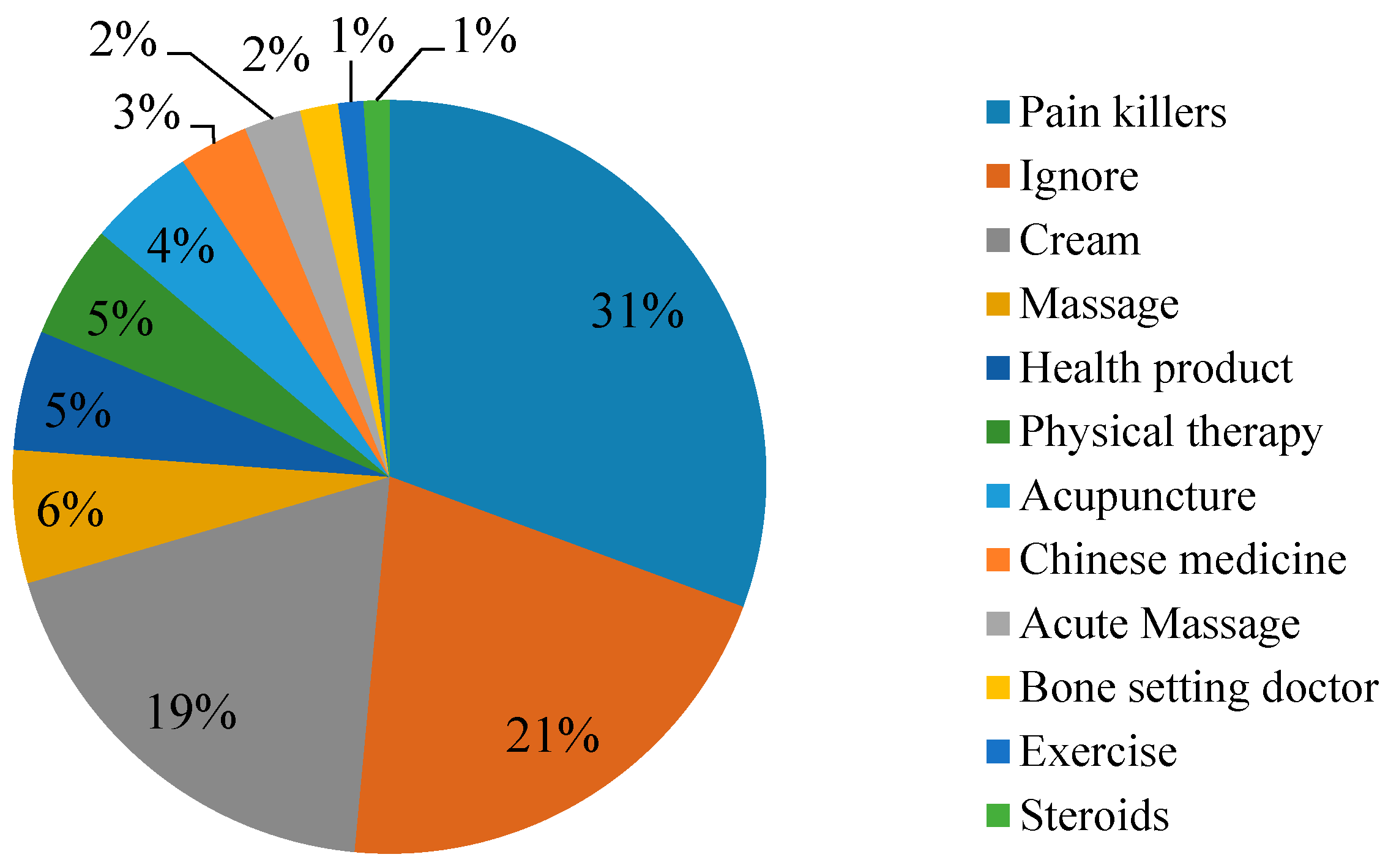
3.3.2. Pain Treatment
3.3.3. Impacts of Pain on Daily Life
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lingard, H. Occupational health and safety in the construction industry. Constr. Manag. Econ. 2013, 31, 505–514. [Google Scholar] [CrossRef]
- Yi, W.; Chan, A.P.C. Which environmental indicator is better able to predict the effects of heat stress on construction workers? J. Manag. Eng. 2004, 31, 04014063. [Google Scholar] [CrossRef]
- Yi, W.; Chan, A.P.C.; Wang, X.; Wang, J. Development of an early-warning system for site work in hot and humid environments: A case study. Autom. Constr. 2006, 62, 101–113. [Google Scholar] [CrossRef]
- Hallowell, M.R.; Gambatese, J.A. Construction safety risk mitigation. J. Constr. Eng. Manag. 2009, 135, 1316–1323. [Google Scholar] [CrossRef]
- International Labour Organization (ILO). Facts on Safety at Work; International Labour Office: Geneva, Switzerland, 2005. [Google Scholar]
- U.S. Bureau of Labour Statistics. Revisions to the 2012 Census of Fatal Occupational Injuries (CFIO) Counts. Available online: http://www.bls.gov/iif/oshwc/cfoi/cfoi_revised12.pdf (accessed on 31 March 2016).
- Health and Safety Executive. Health and Safety in Construction in Great Britain, 2014. Available online: http://www.hse.gov.uk/statistics/industry/construction/construction.pdf (accessed on 1 April 2016).
- Labour Department, Hong Kong. Occupational Safety and Health Statistics Bulletin Issue No. 15 (August 2015). Occupational Safety and Health Branch, Labour Department, Hong Kong Government. Available online: http://www.labour.gov.hk/eng/osh/pdf/Bulletin2014.pdf (accessed on 3 May 2016).
- Ministry of Labour and Immigration, Spain, under Secretary of Labour and Social Affairs Statistics of Industrial Accidents and Occupational Diseases. Available online: http://www.mtas.es/Estadisticas/EAT/welcome.htm (accessed on 15 September 2008).
- Reese, C.D.; Eidson, J.V. Handbook of OSHA Construction Safety and Health, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2006. [Google Scholar]
- Kawai, N.; Kawai, T.; Kawai, K. Ultrasonic and laboratory studies on fatty liver in white collar workers. Jpn. J. Gastroenterol. 1995, 92, 1058–1065. [Google Scholar]
- Choi, Y.Y.; Kim, K.Y. Effects of physical examination and diet consultation on serum cholesterol and health-behavior in the Korean pilots employed in commercial airline. Ind. Health 2013, 51, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Haldiya, K.R.; Mathur, M.L.; Sachdev, R.; Saiyed, H.N. Risk of high blood pressure in salt workers working near salt milling plants: A cross-sectional and interventional study. Environ. Health 2005, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, S.; Kuramatani, N.; Arimoto, A.; Ichihara, G. Time course of blood parameters in printing workers with cholangiocarcinoma. J. Occup. Health 2014, 56, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Punnett, L.; Wegman, D.H. Work-related musculoskeletal disorders: The epidemiologic evidence and the debate. J. Electromyogr. Kinesiol. 2004, 14, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Leung, M.Y.; Chan, I.Y.S.; Yu, J. Preventing construction worker injury incidents through the management of personal stress and organizational stressors. Accid. Anal. Prev. 2012, 48, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Goldsheyder, D.; Weinera, S.S.; Nordin, M.; Hiebert, R. Musculoskeletal symptom survey among cement and concrete workers. Work 2004, 23, 111–121. [Google Scholar] [PubMed]
- Hanklang, S.; Kaewboonchoo, O.; Silpasuwan, P.; Mungarndee, S.S. Musculoskeletal disorders among Thai women in construction-related work. Asia-Pac. J. Public Health 2014, 26, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Alberta Construction Safety Association (ACSA). Lost-Time Claims, Disabling Injury Claims and Claim Rates—2004 to 2008. Available online: http://employment.alberta.ca/documents/WHS/WHS-PUB-2009-data-analysis.pdf (accessed on 15 September 2016).
- Hong Kong Construction Industry Council (HKCIC). The Construction Industry Council Launches Pilot Medical Examination Scheme for Construction Workers. Available online: https://www.cic.hk/cic_data/pdf/about_cic/news_and_update/whats_new/eng/20140326_Announcement_BodyCheck_e.pdf (accessed on 15 August 2016).
- Chan, O. Meeting Challenges of HK’s Construction Industry. Available online: http://www.chinadaily.com.cn/hkedition/2012-12/14/content_16016231.htm (accessed on 15 August 2016).
- Construction Workers Registration Board. Total Number of Valid Registered Workers in Designated Trades. Available online: http://cwr.hkcic.org/information/total.asp (accessed on 15 September 2016).
- Watson, J. How to Determine A Sample Size: Tipsheet #60, Penn State Cooperative Extension. Available online: http://extension.psu.edu/evaluation/pdf/TS60.pdf (accessed on 15 September 2016).
- Kanazawa, M.; Yoshiike, N.; Osaka, T.; Numba, Y.; Zimmet, P.; Inoue, S. Criteria and classification of obesity in Japan and Asia-Oceania. World Rev. Nutr. Diet. 2005, 94, 1–12. [Google Scholar] [PubMed]
- Tung Wah Group of Hospitals. eBACCalc—Alcohol Prevention and Treatment Service. Available online: http://www.apkmonk.com/app/org.tungwah.atp.ebaccalc/ (accessed on 8 February 2016).
- Tse, M.M.Y.; Wan, V.T.C.; Ho, S.S.K. Profile of pain and use of pharmacological and non-pharmacological methods for relieving pain in older persons in nursing homes. J. Pain Manag. 2010, 3, 309–317. [Google Scholar]
- Tse, M.; Wan, V.T.; Wong, A.M. Pain and pain-related situations surrounding community-dwelling older persons. J. Clin. Nurs. 2013, 22, 1870–1879. [Google Scholar] [CrossRef] [PubMed]
- Poulter, N.R.; Prabhakaran, D.; Causlfield, M. Hypertension. Lancet 2015, 386, 801–812. [Google Scholar] [CrossRef]
- American Heart Association. All About Heart Rate (Pulse). Available online: http://www.heart.org/HEARTORG/Conditions/More/MyHeartandStrokeNews/All-About-Heart-Rate-Pulse_UCM_438850_Article.jsp#.V-OSIHpxur0 (accessed on 3 May 2016).
- Renard, E. Monitoring glycemic control: The importance of self-monitoring of blood glucose. Am. J. Med. 2005, 118 (Suppl. 9), S12–S19. [Google Scholar] [CrossRef]
- Pincus, M.R.; Abraham, N.Z. Interpreting laboratory results. In Henry’s Clinical Diagnosis and Management by Laboratory Methods, 22nd ed.; McPherson, R.A., Pincus, M.R., Eds.; Elsevier Saunders: Philadelphia, PA, USA, 2011. [Google Scholar]
- Nyblom, H.; Björnsson, E.; Simrén, M.; Aldenborg, F.; Almer, S.; Olsson, R. The AST/ALT ratio as an indicator of cirrhosis in patients with PBC. Liver Int. 2006, 26, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Hosten, A.O. BUN and Creatinine. Clinical Methods: The History, Physical, and Laboratory Examinations, 3rd ed.; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworths: Boston, MA, USA, 1990. [Google Scholar]
- Mann, S.; Beedie, C.; Jimenez, A. Differential effects of aerobic exercise, resistance training and combined exercise modalities on cholesterol and the lipid profile: review, synthesis and recommendation. Sports Med. 2014, 44, 211–222. [Google Scholar] [CrossRef] [PubMed]
- National Health Service (2015a). Uric Acid/Urate. Available online: http://www.gloshospitals.nhs.uk/en/Wards-and-Departments/Departments/Pathology/Pathology-Samples-and-Tests/Search/Chemical-Pathology/Urate--Uric-Acid-Blood/ (accessed on 13 August 2016).
- National Health Service (2015b). High Cholesterol. Available online: http://www.nhs.uk/Conditions/cholesterol/Pages/Introduction.aspx (accessed on 13 August 2016).
- Angelopoulos, T.J.; Lowndes, J.; Zukley, L.; Melanson, K.J.; Nguyen, V.; Huffman, A.; Rippe, J.M. The effect of high-fructose corn syrup consumption on triglycerides and uric acid. J. Nutr. 2009, 139, 1242–1245. [Google Scholar] [CrossRef] [PubMed]
- Census and Statistics Department. Body Mass Index (BMI) Distribution Based on Classification of Weight Status for Chinese Adults in Hong Kong by Sex. Available online: http://www.censtatd.gov.hk/FileManager/EN/Content_1149/T07_08.xls (accessed on 15 September 2016).
- Groeneveld, I.F.; Proper, K.I.; van der Beek, A.J.; van Duivenbooden, C.; van Mechelen, W. Design of a RCT evaluating the (cost-) effectiveness of a lifestyle intervention for male construction workers at risk for cardiovascular disease: The health under construction study. BMC Public Health 2008, 8, 1. [Google Scholar] [CrossRef] [PubMed]
- Claessen, H.; Arndt, V.; Drath, C.; Brenner, H. Overweight, obesity and risk of work disability: A cohort study of construction workers in Germany. Occup. Environ. Med. 2009, 66, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Census and Statistics Department. Hypertension. Available online: http://www.chp.gov.hk/en/content/9/25/35390.html (accessed on 15 September 2016).
- South China Morning Post. Almost Half of Hongkongers Have Unhealthy BMI and Cholesterol, Study Suggests (even Those Who Look Slim). Available online: http://www.scmp.com/news/hong-kong/health-environment/article/2001360/hong-kongs-men-less-healthy-women-study-suggests (accessed on 15 September 2016).
- Gray, B.J.; Bracken, R.M.; Turner, D.; Morgan, K.; Mellalieu, S.D.; Thomas, M. Prevalence of undiagnosed cardiovascular risk factors and 10-year CVD risk in male steel industry workers. J. Occup. Environ. Med. 2014, 56, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Phonrat, B.; Pongpaew, P.; Tungtrongchitr, R.; Horsawat, V.; Supanaranond, W.; Vutikes, S.; Vudhivai, N.; Schelp, F.P. Risk factors for chronic diseases among road sweepers in Bangkok. Southeast Asian J. Trop. Med. Public Health 1997, 28, 36–45. [Google Scholar] [PubMed]
- Beevers, D.G.; MacGregor, G.A. Hypertension in Practice, 3rd ed.; CRC Press: Boca Raton, FL, USA, 1999. [Google Scholar]
- Ong, J.J.; Sharma, V.K. High serum total cholesterol levels as a risk factor of ischemic stroke in Asian individuals. Aging Health 2012, 8, 239–242. [Google Scholar] [CrossRef]
- Mancino, L.; Kuchler, F. Offsetting behavior in reducing high cholesterol: Substitution of medication for diet and lifestyle changes. J. Choice Model. 2009, 2, 51–64. [Google Scholar] [CrossRef]
- Ranade, V. Cholesterol detection, diagnosis and evaluation. Int. J. Clin. Pharmacol. Ther. Toxicol. 1993, 31, 313–321. [Google Scholar] [PubMed]
- Brunner, E.J.; Thorogood, M.; Rees, K.; Hewitt, G. Dietary advice for reducing cardiovascular risk: Cochrane systematic review. Int. J. Epidemiol. 2006, 35, 538–539. [Google Scholar]
- Dong, X.S.; Wang, X.; Daw, C.; Ringen, K. Chronic diseases and functional limitations among older construction workers in the United States. J. Occup. Environ. Med. 2011, 53, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Construction Workers Registration Board. Total Number of Valid Registered Workers in Designated Trades. Available online: http://cwr.hkcic.org/download/Chi_Age_Distribution_by%20alphabetical%20order.pdf (accessed on 1 July 2016).
- Boschman, J.S.; van der Molen, H.F.; Sluiter, J.K.; Frings-Dresen, M.H.W. Musculoskeletal disorders among construction workers: A one-year follow-up study. BMC Musculoskelet. Disord. 2012, 13, 196. [Google Scholar] [CrossRef] [PubMed]
- Deros, B.M.; Daruis, D.D.I.; Khamis, N.K.; Mohamad, D.; Daud, S.F.M.; Amdan, S.M.; Aziz, R.A.; Jamal, N. Prevalence of work related musculoskeletal disorders symptoms among construction workers: A case study in Malaysia. Iran. J. Public Health 2014, 43, 53–57. [Google Scholar]
- Holmström, E.B. Musculoskeletal disorders in construction workers related to physical, psychosocial, and individual factors. Acta Orthop. Scand. 1992, 63, S247. [Google Scholar] [CrossRef]
- Forde, M.S.; Punnett, L.; Wegman, D.H. Prevalence of musculoskeletal disorders in union ironworkers. J. Occup. Environ. Hyg. 2005, 2, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Holmström, E.; Engholm, G. Musculoskeletal disorders in relation to age and occupation in Swedish construction workers. Am. J. Ind. Med. 2003, 44, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Kuorinka, I. Tools and means of implementing participatory ergonomics. Int. J. Ind. Ergon. 1997, 19, 267–270. [Google Scholar] [CrossRef]
- NRC Panel on Musculoskeletal Disorders. Musculoskeletal Disorders and the Workplace, Low Back and Upper Extremities; National Research Council, National Academy Press: Washington, DC, USA, 2001; pp. 301–329. [Google Scholar]
- Vi, P. Reducing risk of musculoskeletal disorders through the use of rebar-tying machines. Appl. Occup. Environ. Hyg. 2003, 18, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Arcury, T.A.; O’Hara, H.; Grzywacz, J.G.; Isom, S.; Chen, H. Work safety climate, musculoskeletal discomfort, working while injured, and depression among migrant farmworkers in North Carolina. Am. J. Public Health 2012, 102 (Suppl. 2), S272–S278. [Google Scholar] [CrossRef] [PubMed]
- Fung, I.W.H.; Tam, V.W.Y.; Tam, C.M.; Wang, K. Frequency and continuity of work-related musculoskeletal symptoms for construction workers. J. Civ. Eng. Manag. 2008, 14, 183–187. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | N | Min | Max | Mean ± Standard Deviation (SD) | Percentage (%) |
|---|---|---|---|---|---|
| Age (years) | 942 | 17 | 70 | 45.1 ± 12.1 | - |
| Male | 818 | 17 | 70 | 44.3 ± 12.4 | - |
| Female | 124 | 28 | 66 | 50.5 ± 12.1 | - |
| Weight (kg) | 932 | 42 | 115 | 68.5 ± 11.6 | - |
| Height (cm) | 932 | 145 | 191 | 168.6 ± 8.0 | - |
| Body Mass Index (BMI) (kg/m2) | 932 | 13.3 | 36.8 | 24.3 ± 3.7 | - |
| Sleeping (hs) | 938 | 4 | 11 | 6.9 ± 1.2 | - |
| Smoking Habits | - | - | - | - | - |
| Non-Smoker (%) | 477 | - | - | - | 50.9 |
| Occasional Smoker (%) | 101 | - | - | - | 10.8 |
| Daily Smoker (%) | 360 | - | - | - | 38.4 |
| Alcohol Drinking Habit | - | - | - | - | - |
| Non-Alcohol Drinker (%) | 380 | - | - | - | 40.4 |
| Occasional Alcohol Drinker (%) | 494 | - | - | - | 52.7 |
| Problematic Alcohol Drinker (%) | 64 | - | - | - | 6.8 |
| Ethnicity | - | - | - | - | - |
| Hong Kong (%) | 839 | - | - | - | 89.4 |
| Mainland Chinese (%) | 87 | - | - | - | 9.3 |
| Pakistani (%) | 6 | - | - | - | 0.6 |
| Nepalese (%) | 6 | - | - | - | 0.6 |
| Working Experience in Construction (years) | 939 | 0.2 | 53 | 12.9 ± 10.9 | - |
| Parameter | Mean ± SD |
|---|---|
| DBP (mmHg) | 77.7 ± 14.5 |
| SBP (mmHg) | 135.3 ± 17.2 |
| Resting Heart Rate (bpm) | 76.7 ± 12.1 |
| Glucose-Fasting (mmol/L) | 4.9 ± 1.4 |
| Glucose-Random (mmol/L) | 5.7 ± 2.2 |
| AST (U/L) | 30.2 ± 16.4 |
| ALT (U/L) | 33.3 ± 20.9 |
| Urea (nmol/L) | 5.7 ± 1.5 |
| Cholesterol | 4.9 ± 0.8 |
| Uric Acid | 360.3 ± 81.7 |
| Health Parameters | Mean | SD | F | Significance |
|---|---|---|---|---|
| Glucose (Fasting) (mmol/L) b | - | - | - | - |
| <35 years | 4.4 | 0.7 | 8.66 | 0.002 |
| 35–50 years | 4.9 | 1.5 | - | - |
| ≥50 years | 5.4 | 1.6 | - | - |
| Cholesterol (mmol/L) b | - | - | - | - |
| <35 years | 4.5 | 0.7 | 46.76 | 0.000 |
| 35–50 years | 4.8 | 0.9 | - | - |
| ≥50 years | 5.3 | 0.7 | - | - |
| Uric Acid (mmol/L) c | - | - | - | - |
| <35 years | 342.5 | 76.7 | 19.43 | 0.001 |
| 35–50 years | 374.1 | 78.2 | - | - |
| ≥50 years | 381.7 | 70.3 | - | - |
| Pain Severity | Male | Female | Pooled |
|---|---|---|---|
| Sample size | 312 | 57 | 369 |
| Most Intense Pain over the Past 24 h | 5.5 ± 2.6 | 4.9 ± 1.8 | 5.2 ± 2.5 |
| Slightest Pain over the Past 24 h | 2.1 ± 1.8 | 1.9 ± 2.0 | 2.0 ± 1.9 |
| Average Pain over the Past 24 h | 3.7 ± 2.2 | 4.2 ± 1.9 | 3.9 ± 2.0 |
| Present Pain | 2.5 ± 2.3 | 2.9 ± 2.1 | 2.6 ± 2.5 |
| Characteristic | Estimate | Standard Error | Significance |
|---|---|---|---|
| Age (years) | −0.14 | 0.003 | 0.000 |
| Working Experiences (years) | −1.17 | 0.054 | 0.023 |
| BMI | - | - | - |
| Underweight | Reference | 0.000 | 0.000 |
| Normal | 0.02 | 0.036 | 0.024 |
| Overweight | −0.48 | 0.067 | 0.009 |
| Obese | −0.94 | 0.065 | 0.003 |
| Alcohol Drinking Habit | - | - | - |
| Non-Drinker | Reference | 0.000 | 0.000 |
| Occasional Alcohol Drinker | −0.13 | 0.082 | 0.034 |
| Problematic Alcohol Drinker | −0.65 | 0.099 | 0.022 |
| Item | 1 | 2 | 3 | 4 | 5 | 6 | 7 | Mean ± SD |
|---|---|---|---|---|---|---|---|---|
| Strongly Disagree | Disagree | Somewhat Disagree | Neither Agree Nor Disagree | Somewhat Agree | Agree | Strongly Agree | ||
| Mood | 1 | 50 | 77 | 73 | 51 | 14 | 2 | 3.6 ± 1.2 |
| Walking Ability | 3 | 12 | 35 | 72 | 77 | 67 | 2 | 4.5 ± 1.2 |
| Work Productivity | 4 | 10 | 39 | 36 | 76 | 65 | 38 | 4.9 ± 1.5 |
| Relationship between Family, Friends, Partners | 41 | 80 | 57 | 46 | 32 | 9 | 3 | 2.9 ± 1.4 |
| Sleep | 7 | 26 | 23 | 34 | 75 | 78 | 25 | 4.8 ± 1.5 |
| Hobbies | 43 | 63 | 56 | 13 | 43 | 28 | 22 | 3.4 ± 1.9 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, W.; Chan, A. Health Profile of Construction Workers in Hong Kong. Int. J. Environ. Res. Public Health 2016, 13, 1232. https://doi.org/10.3390/ijerph13121232
Yi W, Chan A. Health Profile of Construction Workers in Hong Kong. International Journal of Environmental Research and Public Health. 2016; 13(12):1232. https://doi.org/10.3390/ijerph13121232
Chicago/Turabian StyleYi, Wen, and Albert Chan. 2016. "Health Profile of Construction Workers in Hong Kong" International Journal of Environmental Research and Public Health 13, no. 12: 1232. https://doi.org/10.3390/ijerph13121232
APA StyleYi, W., & Chan, A. (2016). Health Profile of Construction Workers in Hong Kong. International Journal of Environmental Research and Public Health, 13(12), 1232. https://doi.org/10.3390/ijerph13121232