Stress-Induced Hyperglycemia, but Not Diabetic Hyperglycemia, Is Associated with Higher Mortality in Patients with Isolated Moderate and Severe Traumatic Brain Injury: Analysis of a Propensity Score-Matched Population


 ,
,
Abstract
:1. Introduction
2. Methods
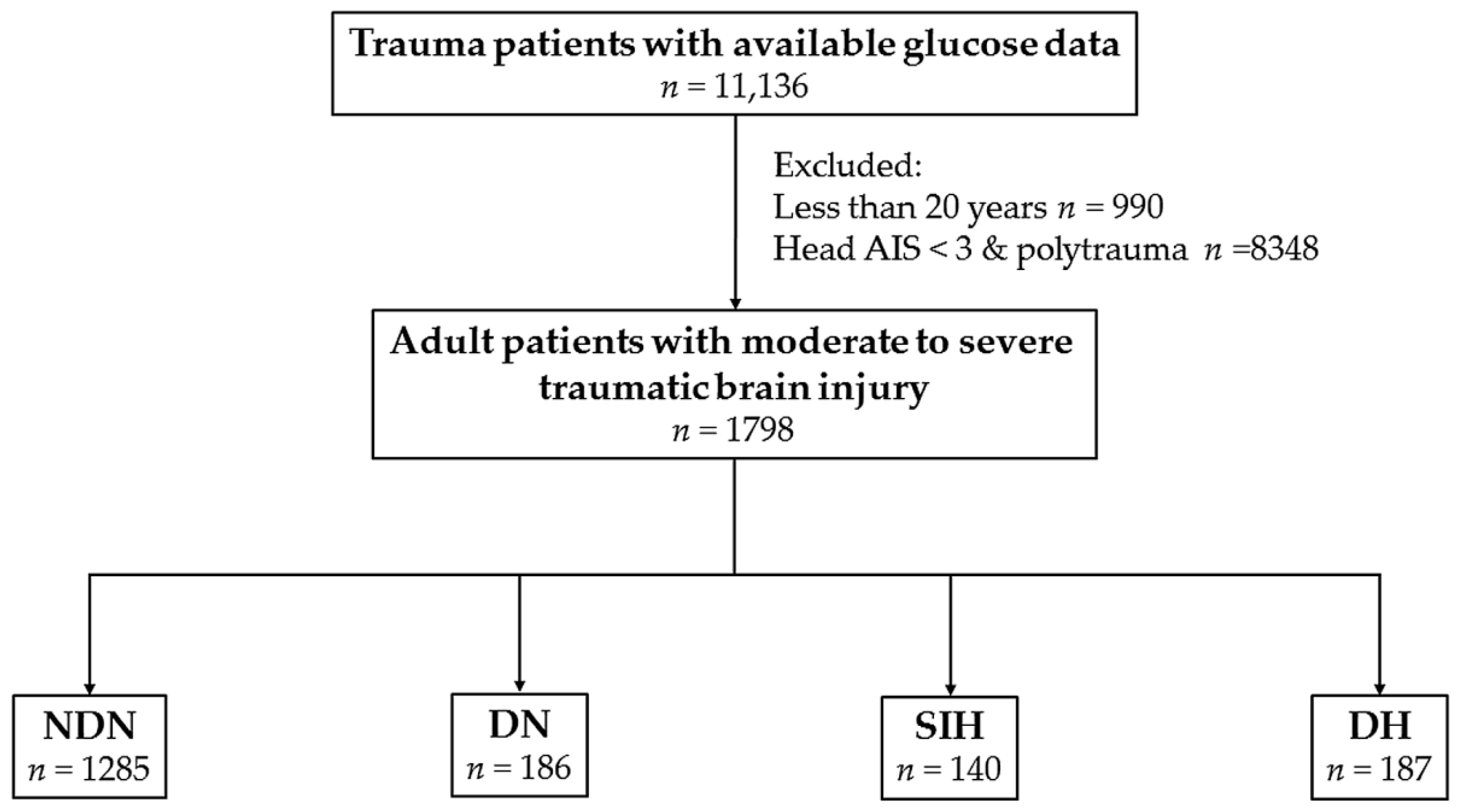
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Characteristics and Outcomes of Patients with SIH
3.2. Characteristics and Outcomes of Patients with DH
3.3. Adjusted Outcomes of Patients with SIH and with DH
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Alexiou, G.A.; Lianos, G.; Fotakopoulos, G.; Michos, E.; Pachatouridis, D.; Voulgaris, S. Admission glucose and coagulopathy occurrence in patients with traumatic brain injury. Brain Inj. 2014, 28, 438–441. [Google Scholar] [CrossRef] [PubMed]
- Prisco, L.; Iscra, F.; Ganau, M.; Berlot, G. Early predictive factors on mortality in head injured patients: A retrospective analysis of 112 traumatic brain injured patients. J. Neurosurg. Sci. 2012, 56, 131–136. [Google Scholar] [PubMed]
- Salim, A.; Hadjizacharia, P.; Dubose, J.; Brown, C.; Inaba, K.; Chan, L.S.; Margulies, D. Persistent hyperglycemia in severe traumatic brain injury: An independent predictor of outcome. Am. Surg. 2009, 75, 25–29. [Google Scholar] [PubMed]
- Khajavikhan, J.; Vasigh, A.; Kokhazade, T.; Khani, A. Association between Hyperglycaemia with Neurological Outcomes Following Severe Head Trauma. J. Clin. Diagn. Res. JCDR 2016, 10. [Google Scholar] [CrossRef] [PubMed]
- Bosarge, P.L.; Shoultz, T.H.; Griffin, R.L.; Kerby, J.D. Stress-induced hyperglycemia is associated with higher mortality in severe traumatic brain injury. J. Trauma Acute Care Surg. 2015, 79, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, K. Traumatic brain injury: Pathophysiology for neurocritical care. J. Intensiv. Care 2016, 4, 29. [Google Scholar] [CrossRef] [PubMed]
- Gauglitz, G.G.; Herndon, D.N.; Jeschke, M.G. Insulin resistance postburn: Underlying mechanisms and current therapeutic strategies. J. Burn Care Res. Off. Publ. Am. Burn Assoc. 2008, 29, 683–694. [Google Scholar] [CrossRef] [PubMed]
- Smit, J.W.; Romijn, J.A. Acute insulin resistance in myocardial ischemia: Causes and consequences. Semin. Cardiothorac. Vasc. Anesth. 2006, 10, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Ray, B.; Ludwig, A.; Yearout, L.K.; Thompson, D.M.; Bohnstedt, B.N. Stress-Induced Hyperglycemia after Spontaneous Subarachnoid Hemorrhage and Its Role in Predicting Cerebrospinal Fluid Diversion. World Neurosurg. 2017, 100, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.J.; Liao, W.I.; Wang, J.C.; Tsai, C.L.; Lee, J.T.; Peng, G.S.; Lee, C.H.; Hsu, C.W.; Tsai, S.H. Usefulness of glycated hemoglobin A1c-based adjusted glycemic variables in diabetic patients presenting with acute ischemic stroke. Am. J. Emerg. Med. 2017, 35, 1240–1246. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.; Bochicchio, G.V.; Joshi, M.; Bochicchio, K.; Tracy, K.; Scalea, T.M. Admission hyperglycemia is predictive of outcome in critically ill trauma patients. J. Trauma 2005, 59, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Richards, J.E.; Kauffmann, R.M.; Zuckerman, S.L.; Obremskey, W.T.; May, A.K. Relationship of hyperglycemia and surgical-site infection in orthopaedic surgery. J. Bone Jt. Surg. Am. 2012, 94, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Richards, J.E.; Kauffmann, R.M.; Obremskey, W.T.; May, A.K. Stress-induced hyperglycemia as a risk factor for surgical-site infection in nondiabetic orthopedic trauma patients admitted to the intensive care unit. J. Orthop. Trauma 2013, 27, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Mraovic, B.; Suh, D.; Jacovides, C.; Parvizi, J. Perioperative hyperglycemia and postoperative infection after lower limb arthroplasty. J. Diabetes Sci. Technol. 2011, 5, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Leto, R.; Desruelles, D.; Gillet, J.B.; Sabbe, M.B. Admission hyperglycaemia is associated with higher mortality in patients with hip fracture. Eur. J. Emerg. Med. 2015, 22, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Oddo, M.; Schmidt, J.M.; Mayer, S.A.; Chiolero, R.L. Glucose control after severe brain injury. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Zygun, D.A.; Steiner, L.A.; Johnston, A.J.; Hutchinson, P.J.; Al-Rawi, P.G.; Chatfield, D.; Kirkpatrick, P.J.; Menon, D.K.; Gupta, A.K. Hyperglycemia and brain tissue pH after traumatic brain injury. Neurosurgery 2004, 55, 877–881, discussion 882. [Google Scholar] [CrossRef] [PubMed]
- Rostami, E.; Bellander, B.M. Monitoring of glucose in brain, adipose tissue, and peripheral blood in patients with traumatic brain injury: A microdialysis study. J. Diabetes Sci. Technol. 2011, 5, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Bonizzoli, M.; Zagli, G.; Lazzeri, C.; Degl’Innocenti, S.; Gensini, G.; Peris, A. Early insulin resistance in severe trauma without head injury as outcome predictor? A prospective, monocentric pilot study. Scand. J. Trauma Resusc. Emerg. Med. 2012, 20, 69. [Google Scholar] [CrossRef] [PubMed]
- Bosarge, P.L.; Kerby, J.D. Stress-induced hyperglycemia: Is it harmful following trauma? Adv. Surg. 2013, 47, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Kerby, J.D.; Griffin, R.L.; MacLennan, P.; Rue, L.W., 3rd. Stress-induced hyperglycemia, not diabetic hyperglycemia, is associated with higher mortality in trauma. Ann. Surg. 2012, 256, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Differences between the sexes in motorcycle-related injuries and fatalities at a Taiwanese level I trauma center. Biomed. J. 2017, 40, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Liu, H.T.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Motorcycle-related hospitalizations of the elderly. Biomed. J. 2017, 40, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Savitsky, B.; Givon, A.; Rozenfeld, M.; Radomislensky, I.; Peleg, K. Traumatic brain injury: It is all about definition. Brain Inj. 2016, 30, 1194–1200. [Google Scholar] [CrossRef] [PubMed]
- Butcher, N.; Balogh, Z.J. AIS > 2 in at least two body regions: A potential new anatomical definition of polytrauma. Injury 2012, 43, 196–199. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2012, 35, S64–S71. [Google Scholar]
- Rau, C.S.; Wu, S.C.; Chen, Y.C.; Chien, P.C.; Hsieh, H.Y.; Kuo, P.J.; Hsieh, C.H. Higher Mortality in Trauma Patients Is Associated with Stress-Induced Hyperglycemia, but Not Diabetic Hyperglycemia: A Cross-Sectional Analysis Based on a Propensity-Score Matching Approach. Int. J. Environ. Res. Public Health 2017, 14, 1161. [Google Scholar] [CrossRef] [PubMed]
- Rovlias, A.; Kotsou, S. The influence of hyperglycemia on neurological outcome in patients with severe head injury. Neurosurgery 2000, 46, 335–342, discussion 342–343. [Google Scholar] [CrossRef] [PubMed]
- Young, B.; Ott, L.; Dempsey, R.; Haack, D.; Tibbs, P. Relationship between admission hyperglycemia and neurologic outcome of severely brain-injured patients. Ann. Surg. 1989, 210, 466–473. [Google Scholar] [CrossRef] [PubMed]
- McCowen, K.C.; Malhotra, A.; Bistrian, B.R. Stress-induced hyperglycemia. Crit. Care Clin. 2001, 17, 107–124. [Google Scholar] [CrossRef]
- Marik, P.E.; Bellomo, R. Stress hyperglycemia: An essential survival response! Crit. Care Med. 2013, 41, e93–e94. [Google Scholar] [CrossRef] [PubMed]
- Cherian, L.; Hannay, H.J.; Vagner, G.; Goodman, J.C.; Contant, C.F.; Robertson, C.S. Hyperglycemia increases neurological damage and behavioral deficits from post-traumatic secondary ischemic insults. J. Neurotrauma 1998, 15, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.; Zhao, J.; Dash, P.K. High blood glucose does not adversely affect outcome in moderately brain-injured rodents. J. Neurotrauma 2010, 27, 1439–1448. [Google Scholar] [CrossRef] [PubMed]
- Butcavage, K. Glycemic control and intensive insulin protocols for neurologically injured patients. J. Neurosci. Nurs. 2012, 44, E1–E9. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.H.; Roberts, D.J.; Zygun, D.A. Optimal glycemic control in neurocritical care patients: A systematic review and meta-analysis. Crit. Care (Lond. Engl.) 2012, 16, R203. [Google Scholar] [CrossRef] [PubMed]
- Scalea, T.M.; Bochicchio, G.V.; Bochicchio, K.M.; Johnson, S.B.; Joshi, M.; Pyle, A. Tight glycemic control in critically injured trauma patients. Ann. Surg. 2007, 246, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Patrone, C.; Eriksson, O.; Lindholm, D. Diabetes drugs and neurological disorders: New views and therapeutic possibilities. Lancet Diabetes Endocrinol. 2014, 2, 256–262. [Google Scholar] [CrossRef]


{kind=link}
| Variables | SIH n = 140 | NDN n = 1285 | Odds Ratio (95% CI) | p |
|---|---|---|---|---|
| Sex | 0.984 | |||
| Female, n (%) | 50 (35.7) | 460 (35.8) | 1.0 (0.69–1.43) | |
| Male, n (%) | 90 (64.3) | 825 (64.2) | 1.0 (0.70–1.44) | |
| Age (years) | 52.4 ± 18.7 | 54.3 ± 19.8 | - | 0.297 |
| Hemorrhage type | ||||
| EDH, n (%) | 45 (32.1) | 273 (21.2) | 1.8 (1.20–2.57) | 0.003 |
| SDH, n (%) | 90 (64.3) | 688 (53.5) | 1.6 (1.09–2.25) | 0.015 |
| SAH, n (%) | 76 (54.3) | 634 (49.3) | 1.2 (0.86–1.73) | 0.266 |
| ICH, n (%) | 30 (21.4) | 137 (10.7) | 2.3 (1.47–3.55) | <0.001 |
| Co-morbidity | ||||
| HTN, n (%) | 36 (25.7) | 326 (25.4) | 1.0 (0.68–1.52) | 0.929 |
| CAD, n (%) | 4 (2.9) | 42 (3.3) | 0.9 (0.31–2.47) | 1.000 |
| CHF, n (%) | 2 (1.4) | 8 (0.6) | 2.3 (0.49–11.00) | 0.257 |
| CVA, n (%) | 2 (1.4) | 55 (4.3) | 0.3 (0.08–1.34) | 0.102 |
| ESRD, n (%) | 0 (0.0) | 2 (0.2) | - | 1.000 |
| GCS | 7.7 ± 4.7 | 12.4 ± 3.8 | - | <0.001 |
| ≤8 | 89 (63.6) | 255 (19.8) | 7.0 (4.87–10.21) | <0.001 |
| 9–12 | 18 (12.9) | 157 (12.2) | 1.1 (0.63–1.79) | 0.827 |
| ≥13 | 33 (23.6) | 873 (67.9) | 0.1 (0.10–0.22) | <0.001 |
| ISS, median (IQR) | 20 (16–25) | 16 (13–20) | - | <0.001 |
| <16 | 23 (16.4) | 466 (36.3) | 0.3 (0.22–0.55) | <0.001 |
| 16–24 | 65 (46.4) | 678 (52.8) | 0.8 (0.55–1.10) | 0.154 |
| ≥25 | 52 (37.1) | 141 (11.0) | 4.8 (3.26–7.05) | <0.001 |
| Hospital LOS (days) | 14.4 ± 21.1 | 12.2 ± 12.5 | - | 0.236 |
| ICU admission, n (%) | 117 (83.6) | 853 (66.4) | 2.6 (1.62–4.09) | <0.001 |
| Mortality, n (%) | 58 (41.4) | 93 (7.2) | 9.1 (6.10–13.48) | <0.001 |
| Variables | DH n = 187 | NDN n = 1285 | Odds Ratio (95% CI) | p |
|---|---|---|---|---|
| Sex | <0.001 | |||
| Female, n (%) | 92 (49.2) | 460 (35.8) | 1.7 (1.28–2.37) | |
| Male, n (%) | 95 (50.8) | 825 (64.2) | 0.6 (0.42–0.78) | |
| Age (years) | 65.6 ± 12.0 | 54.3 ± 19.8 | - | <0.001 |
| Hemorrhage type | ||||
| EDH, n (%) | 25 (13.4) | 273 (21.2) | 0.6 (0.37–0.89) | 0.012 |
| SDH, n (%) | 104 (55.6) | 688 (53.5) | 1.1 (0.80–1.48) | 0.595 |
| SAH, n (%) | 78 (41.7) | 634 (49.3) | 0.7 (0.54–1.00) | 0.051 |
| ICH, n (%) | 22 (11.8) | 137 (10.7) | 1.1 (0.69–1.80) | 0.650 |
| Co-morbidity | ||||
| HTN, n (%) | 116 (62.0) | 326 (25.4) | 4.8 (3.49–6.63) | <0.001 |
| CAD, n (%) | 20 (10.7) | 42 (3.3) | 3.5 (2.03–6.18) | <0.001 |
| CHF, n (%) | 4 (2.1) | 8 (0.6) | 3.5 (1.04–11.70) | 0.055 |
| CVA, n (%) | 14 (7.5) | 55 (4.3) | 1.8 (0.99–3.32) | 0.053 |
| ESRD, n (%) | 0 (0.0) | 2 (0.2) | - | 1.000 |
| GCS | 12.1 ± 4.2 | 12.4 ± 3.8 | - | 0.320 |
| ≤8 | 44 (23.5) | 255 (19.8) | 1.2 (0.86–1.79) | 0.242 |
| 9–12 | 19 (10.2) | 157 (12.2) | 0.8 (0.49–1.34) | 0.418 |
| ≥13 | 124 (66.3) | 873 (67.9) | 0.9 (0.67–1.29) | 0.656 |
| ISS, median (IQR) | 16 (14–20) | 16 (13–20) | - | 0.183 |
| <16 | 50 (26.7) | 466 (36.3) | 0.6 (0.46–0.90) | 0.011 |
| 16–24 | 108 (57.8) | 678 (52.8) | 1.2 (0.90–1.67) | 0.201 |
| ≥25 | 29 (15.5) | 141 (11.0) | 1.5 (0.97–2.30) | 0.070 |
| Hospital LOS (days) | 13.3 ± 12.0 | 12.2 ± 12.5 | - | 0.296 |
| ICU admission, n (%) | 134 (71.7) | 853 (66.4) | 1.3 (0.91–1.80) | 0.151 |
| Mortality, n (%) | 27 (14.4) | 93 (7.2) | 2.2 (1.37–3.42) | 0.001 |
| Variables | Propensity Score-Matched Cohort | ||||
|---|---|---|---|---|---|
| SIH n = 122 | NDN n = 122 | Odds Ratio (95% CI) | p | Standardized Difference | |
| Sex | 1.000 | ||||
| Female, n (%) | 40 (32.8) | 40 (32.8) | 1.0 (0.59–1.71) | 0.00% | |
| Male, n (%) | 82 (67.2) | 82 (67.2) | 1.0 (0.59–1.71) | 0.00% | |
| Age (years) | 50.9 ± 18.7 | 51.0 ± 17.9 | - | 0.992 | −0.13% |
| Co-morbidity | |||||
| HTN, n (%) | 25 (20.5) | 25 (20.5) | 1.0 (0.54–1.86) | 1.000 | 0.00% |
| CAD, n (%) | 1 (0.8) | 1 (0.8) | 1.0 (0.06–16.17) | 1.000 | 0.00% |
| CHF, n (%) | 0 (0.0) | 0 (0.0) | - | - | - |
| CVA, n (%) | 1 (0.8) | 1 (0.8) | 1.0 (0.06–16.17) | 1.000 | 0.00% |
| ESRD, n (%) | 0 (0.0) | 0 (0.0) | - | - | - |
| EDH, n (%) | 42 (34.4) | 42 (34.4) | 1.0 (0.59–1.70) | 1.000 | 0.00% |
| SDH, n (%) | 83 (68.0) | 83 (68.0) | 1.0 (0.58–1.71) | 1.000 | 0.00% |
| SAH, n (%) | 63 (51.6) | 63 (51.6) | 1.0 (0.61–1.65) | 1.000 | 0.00% |
| ICH, n (%) | 21 (17.2) | 21 (17.2) | 1.0 (0.51–1.94) | 1.000 | 0.00% |
| ISS, median (IQR) | 17 (16–25) | 17 (16–25) | - | 0.898 | 0.00% † |
| Mortality, n (%) | 49 (40.2) | 21 (17.2) | 6.6 (2.58–16.91) | <0.001 | |
| Variables | Propensity Score-Matched Cohort | ||||
|---|---|---|---|---|---|
| DH n = 163 | NDN n = 163 | Odds Ratio (95% CI) | p | Standardized Difference | |
| Sex | 1.000 | ||||
| Female, n (%) | 74 (45.4) | 74 (45.4) | 1.0 (0.65–1.55) | 0.00% | |
| Male, n (%) | 89 (54.6) | 89 (54.6) | 1.0 (0.65–1.55) | 0.00% | |
| Age (years) | 65.0 ± 12.3 | 65.3 ± 13.1 | - | 0.852 | −2.07% |
| Co-morbidity | |||||
| HTN, n (%) | 97 (59.5) | 97 (59.5) | 1.0 (0.64–1.56) | 1.000 | 0.00% |
| CAD, n (%) | 6 (3.7) | 6 (3.7) | 1.0 (0.32–3.17) | 1.000 | 0.00% |
| CHF, n (%) | 1 (0.6) | 1 (0.6) | 1.0 (0.06–16.13) | 1.000 | 0.00% |
| CVA, n (%) | 11 (6.7) | 11 (6.7) | 1.0 (0.42–2.38) | 1.000 | 0.00% |
| ESRD, n (%) | 0 (0.0) | 0 (0.0) | - | - | - |
| EDH, n (%) | 21 (12.9) | 21 (12.9) | 1.0 (0.52–1.91) | 1.000 | 0.00% |
| SDH, n (%) | 87 (53.4) | 87 (53.4) | 1.0 (0.65–1.55) | 1.000 | 0.00% |
| SAH, n (%) | 69 (42.3) | 69 (42.3) | 1.0 (0.64–1.55) | 1.000 | 0.00% |
| ICH, n (%) | 15 (9.2) | 15 (9.2) | 1.0 (0.47–2.12) | 1.000 | 0.00% |
| ISS, median (IQR) | 16 (13–20) | 16 (13–20) | - | 0.916 | 0.00% † |
| Mortality, n (%) | 23 (14.1) | 18 (11.0) | 1.4 (0.68–2.71) | 0.386 | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rau, C.-S.; Wu, S.-C.; Chen, Y.-C.; Chien, P.-C.; Hsieh, H.-Y.; Kuo, P.-J.; Hsieh, C.-H. Stress-Induced Hyperglycemia, but Not Diabetic Hyperglycemia, Is Associated with Higher Mortality in Patients with Isolated Moderate and Severe Traumatic Brain Injury: Analysis of a Propensity Score-Matched Population. Int. J. Environ. Res. Public Health 2017, 14, 1340. https://doi.org/10.3390/ijerph14111340
Rau C-S, Wu S-C, Chen Y-C, Chien P-C, Hsieh H-Y, Kuo P-J, Hsieh C-H. Stress-Induced Hyperglycemia, but Not Diabetic Hyperglycemia, Is Associated with Higher Mortality in Patients with Isolated Moderate and Severe Traumatic Brain Injury: Analysis of a Propensity Score-Matched Population. International Journal of Environmental Research and Public Health. 2017; 14(11):1340. https://doi.org/10.3390/ijerph14111340
Chicago/Turabian StyleRau, Cheng-Shyuan, Shao-Chun Wu, Yi-Chun Chen, Peng-Chen Chien, Hsiao-Yun Hsieh, Pao-Jen Kuo, and Ching-Hua Hsieh. 2017. "Stress-Induced Hyperglycemia, but Not Diabetic Hyperglycemia, Is Associated with Higher Mortality in Patients with Isolated Moderate and Severe Traumatic Brain Injury: Analysis of a Propensity Score-Matched Population" International Journal of Environmental Research and Public Health 14, no. 11: 1340. https://doi.org/10.3390/ijerph14111340