Effects of Group Counseling Programs, Cognitive Behavioral Therapy, and Sports Intervention on Internet Addiction in East Asia: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
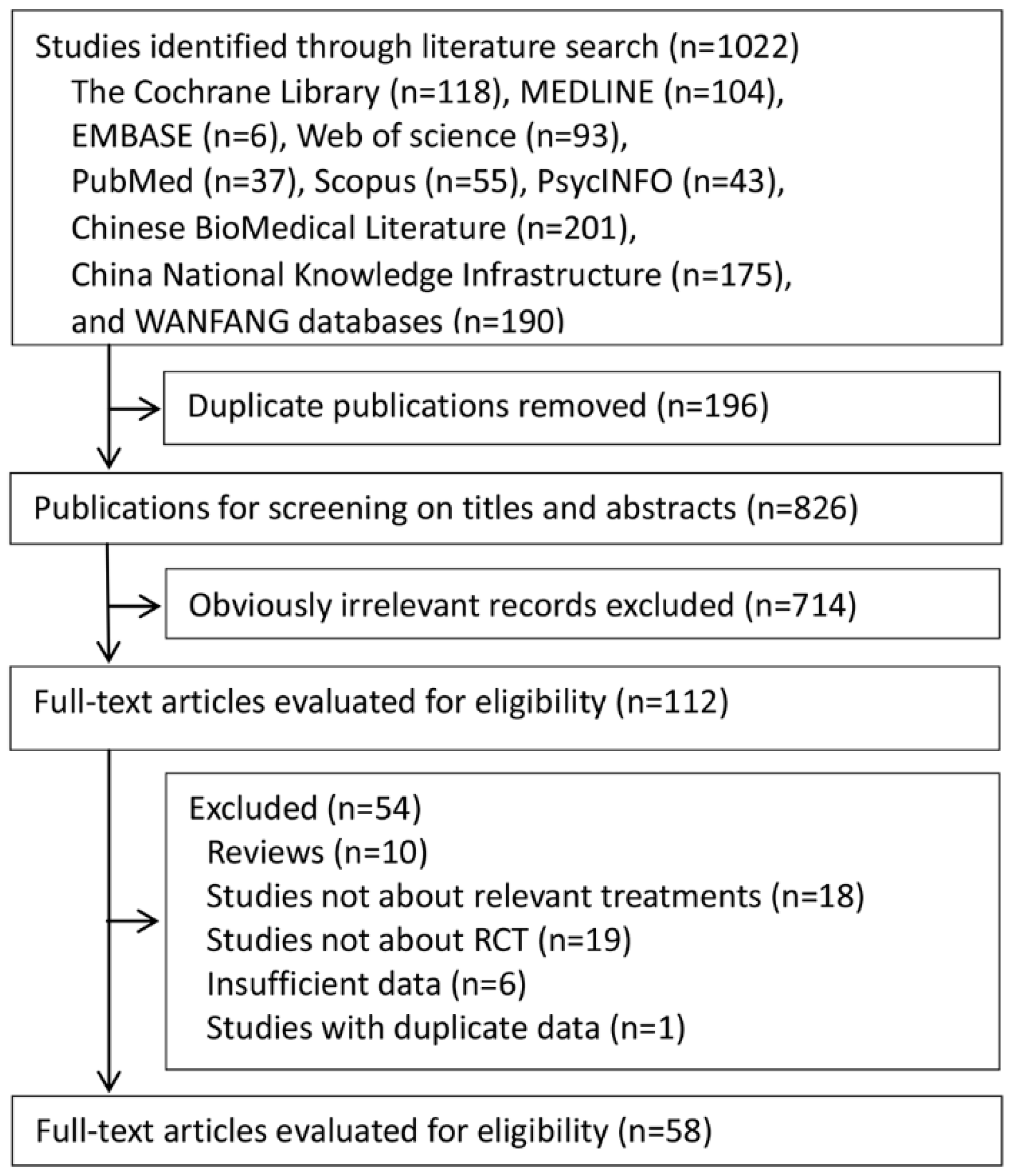
2.1. Literature Search
2.2. Study Selection
2.3. Outcome Measurement
2.4. Data Abstraction and Quality Assessment
2.5. Statistical Analysis
3. Results
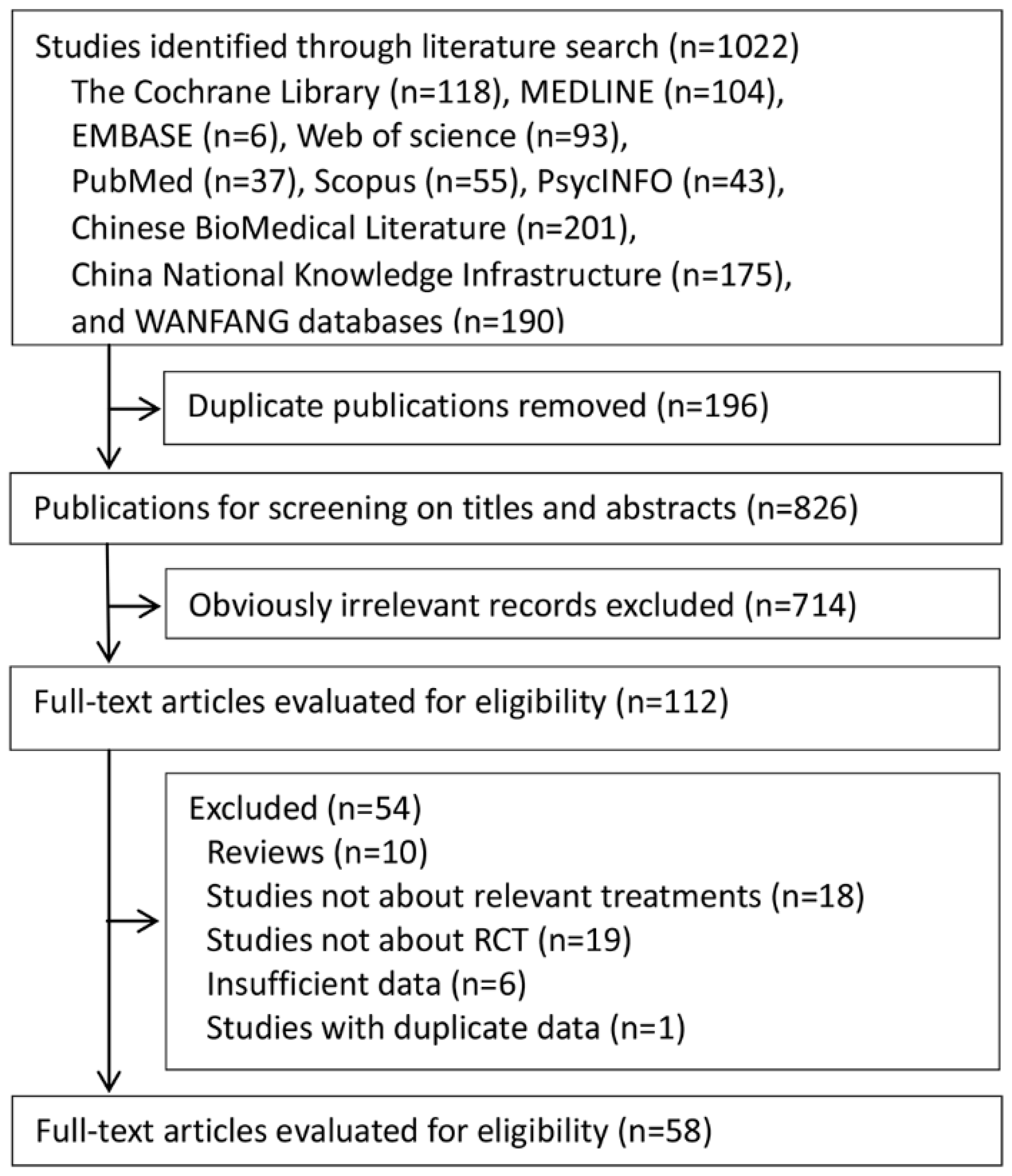
3.1. Identification and Characteristics of Eligible Studies
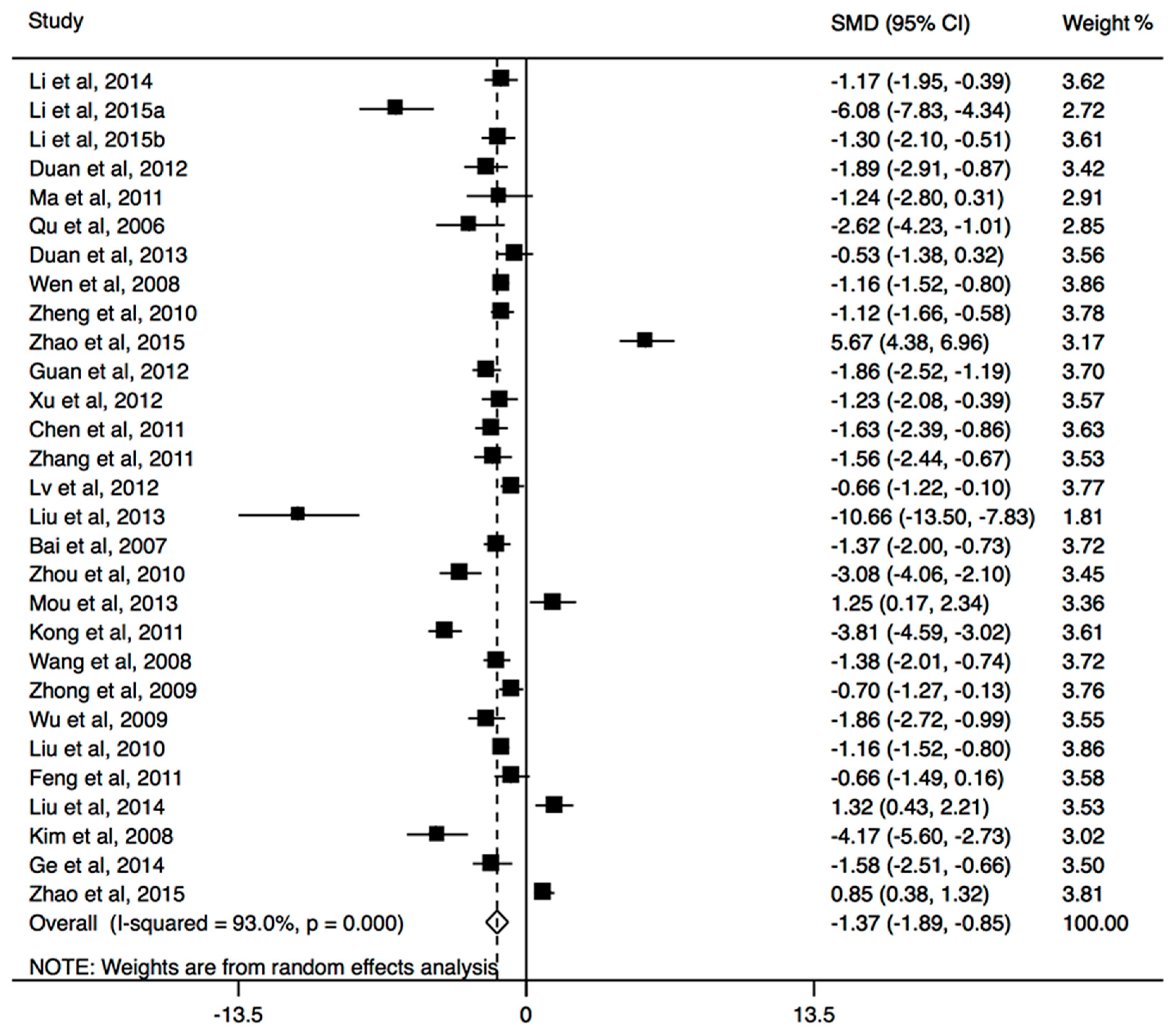
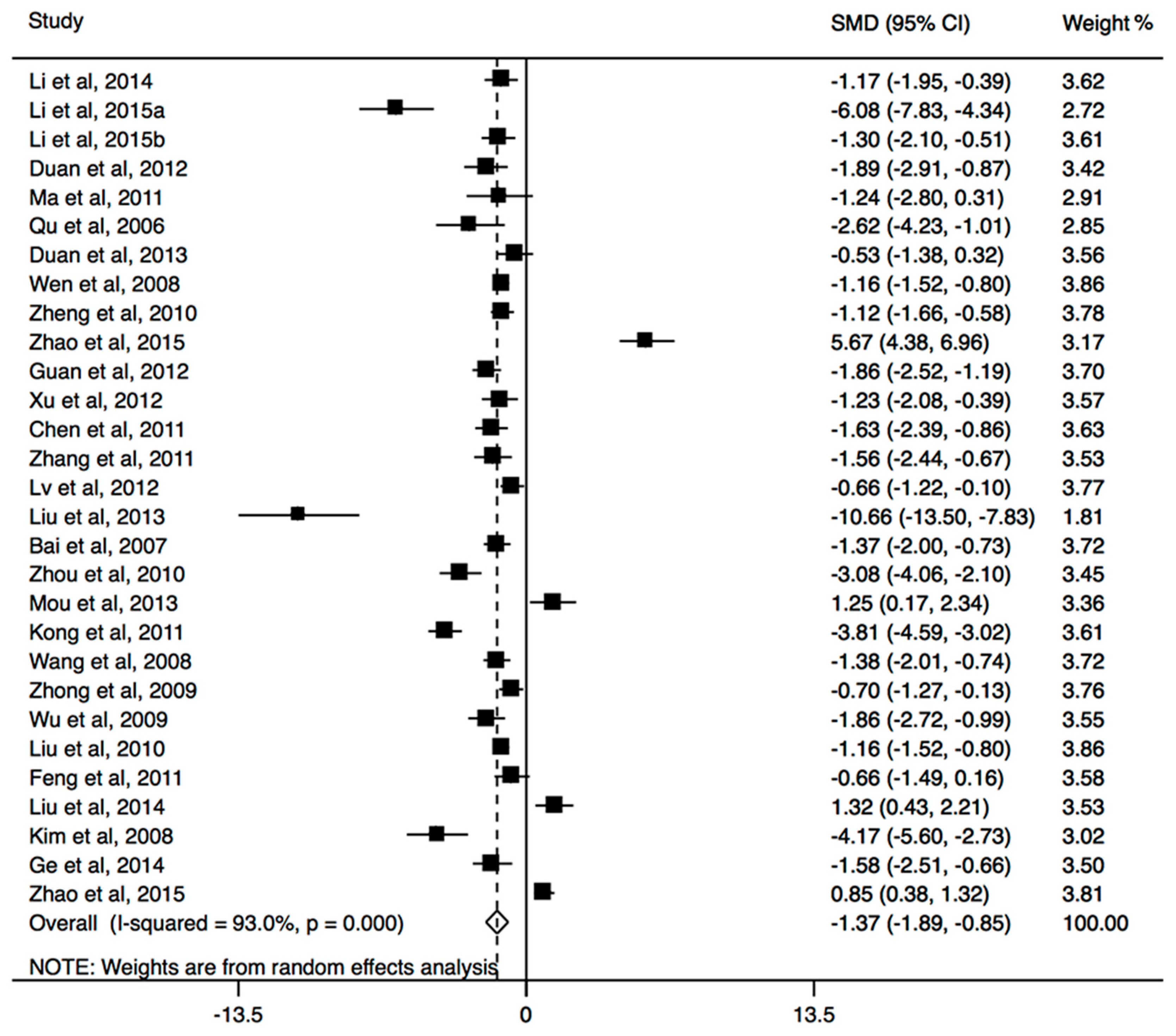
3.2. Effects of Group Counseling Programs
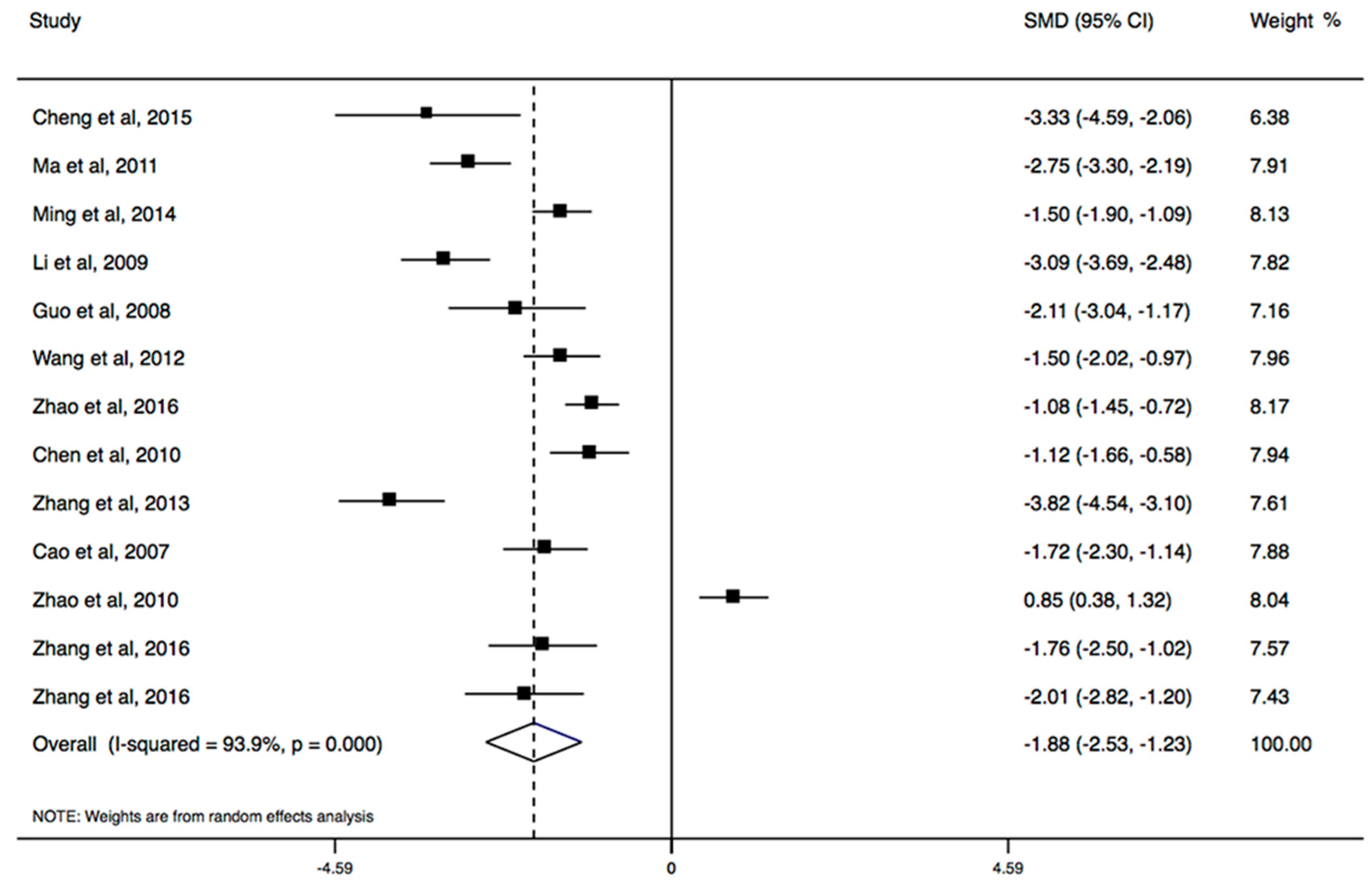
3.3. Effects of CBT
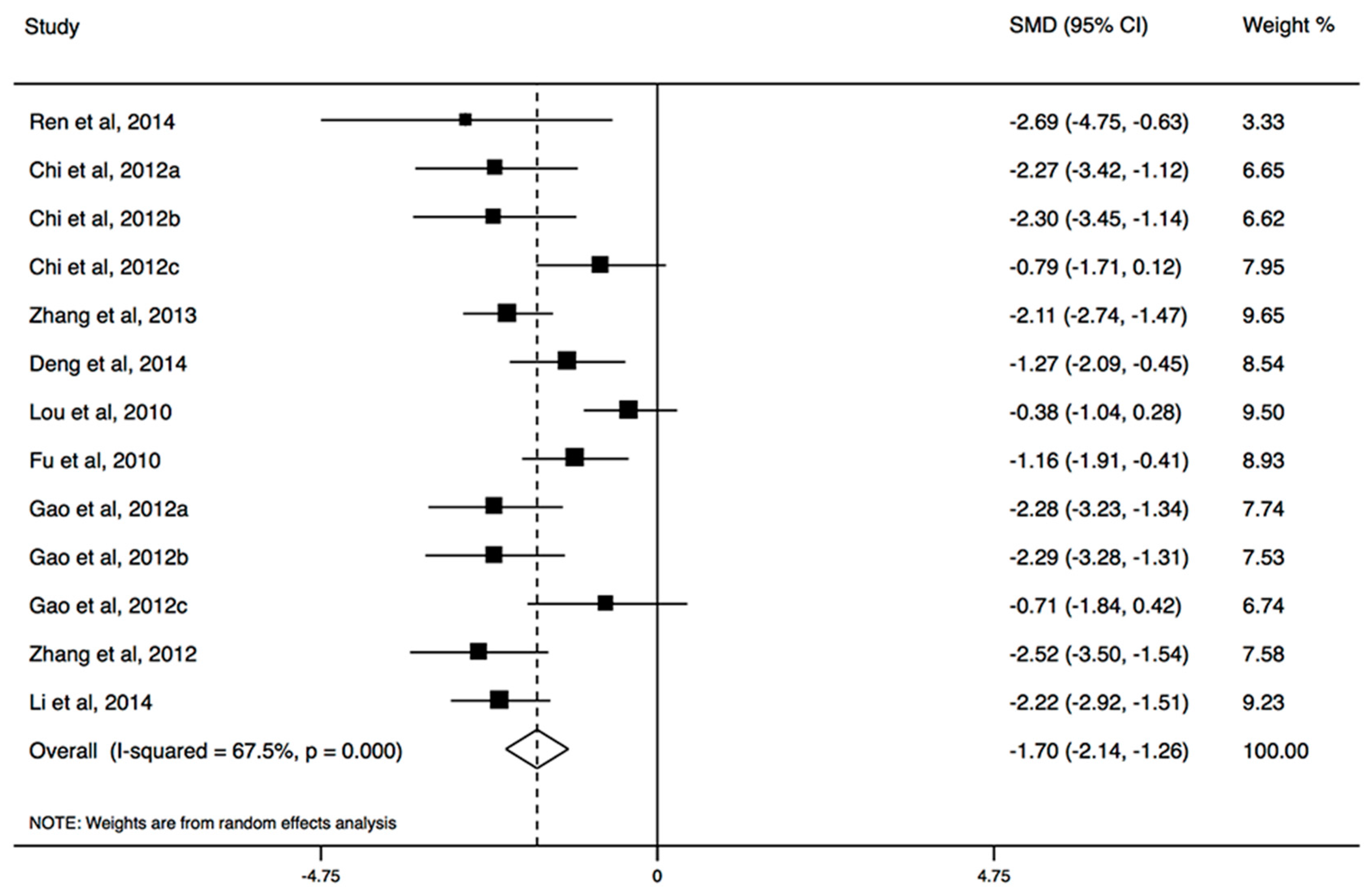
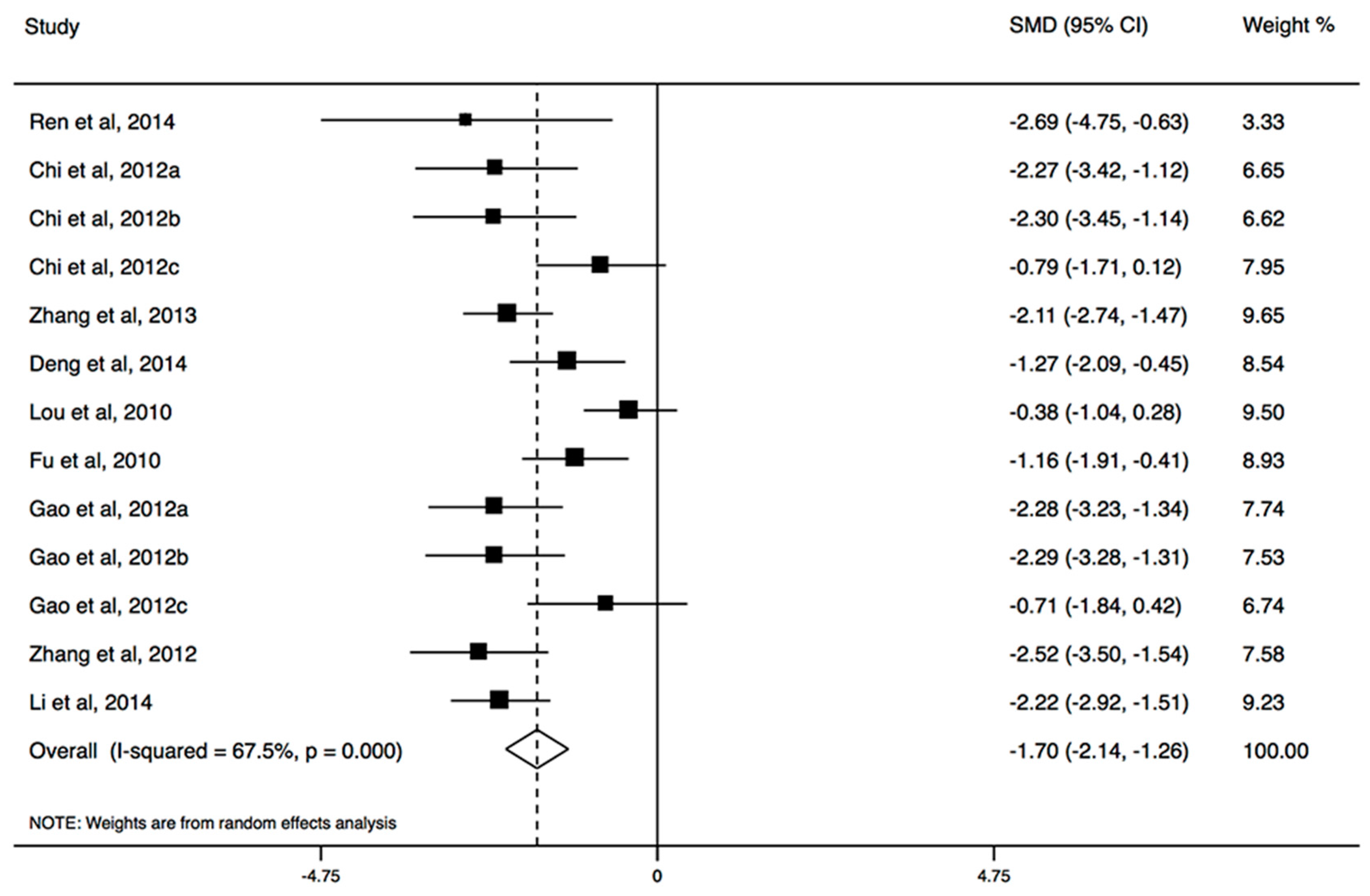
3.4. Effects of Sports Intervention
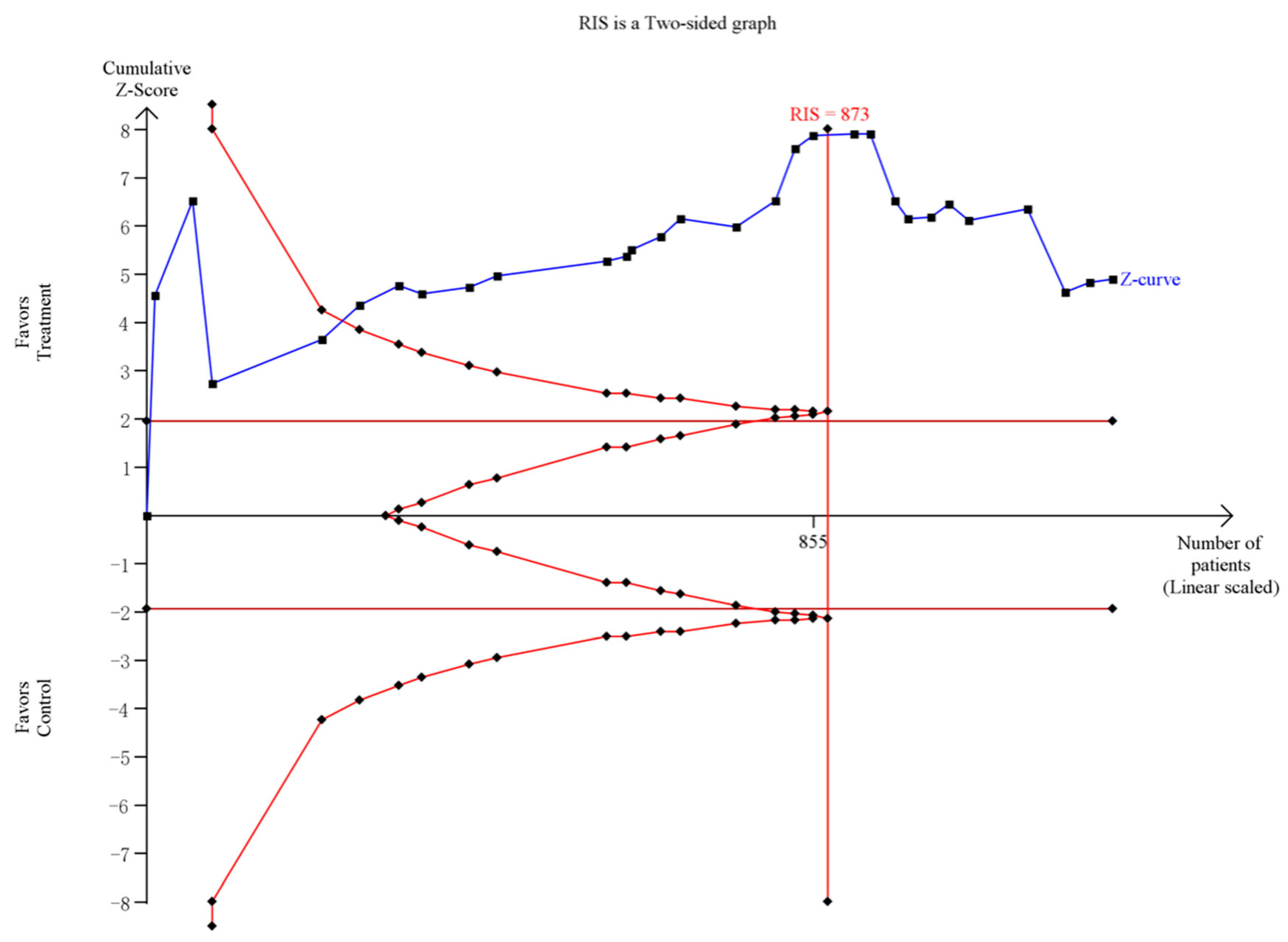
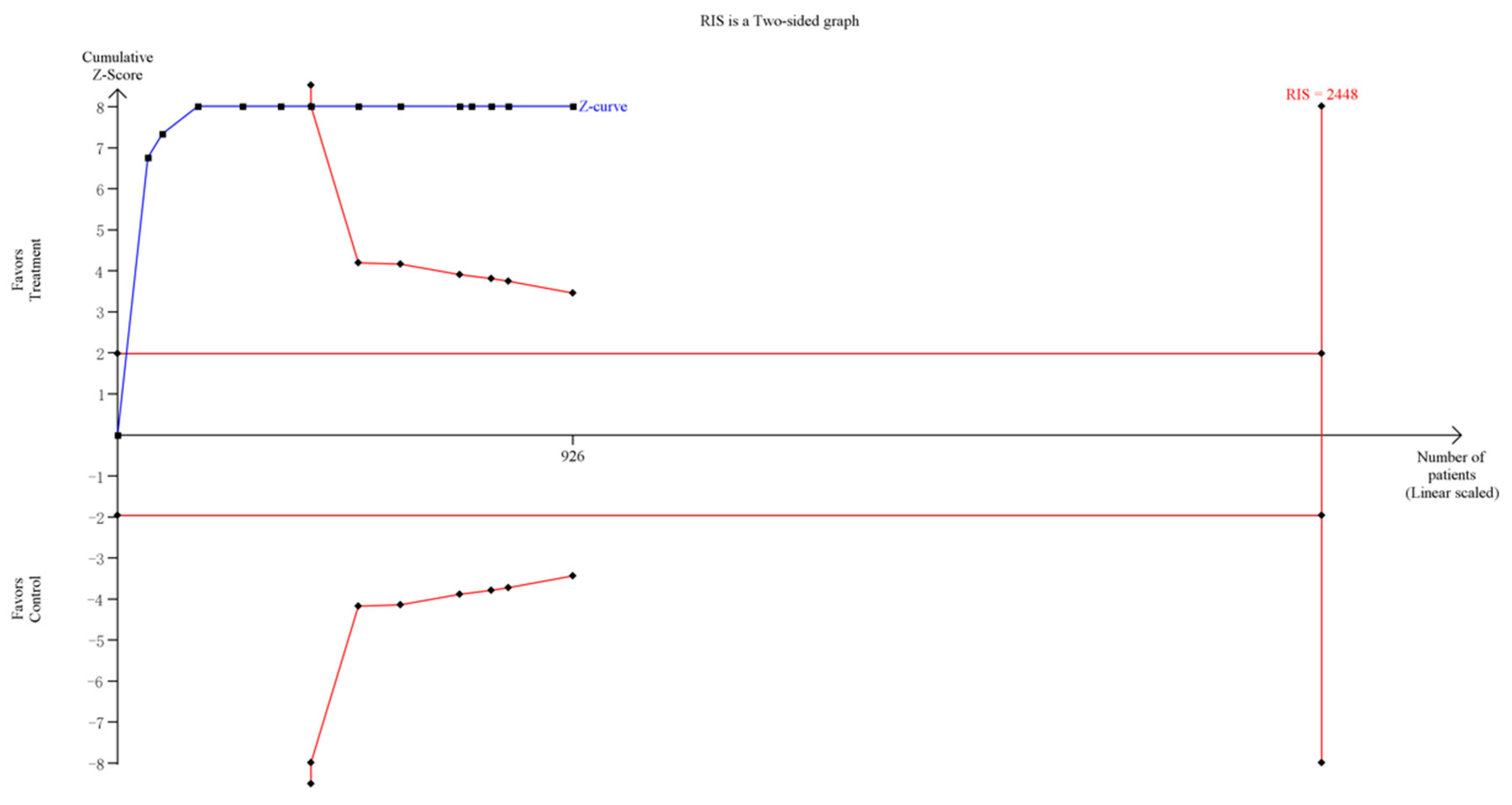
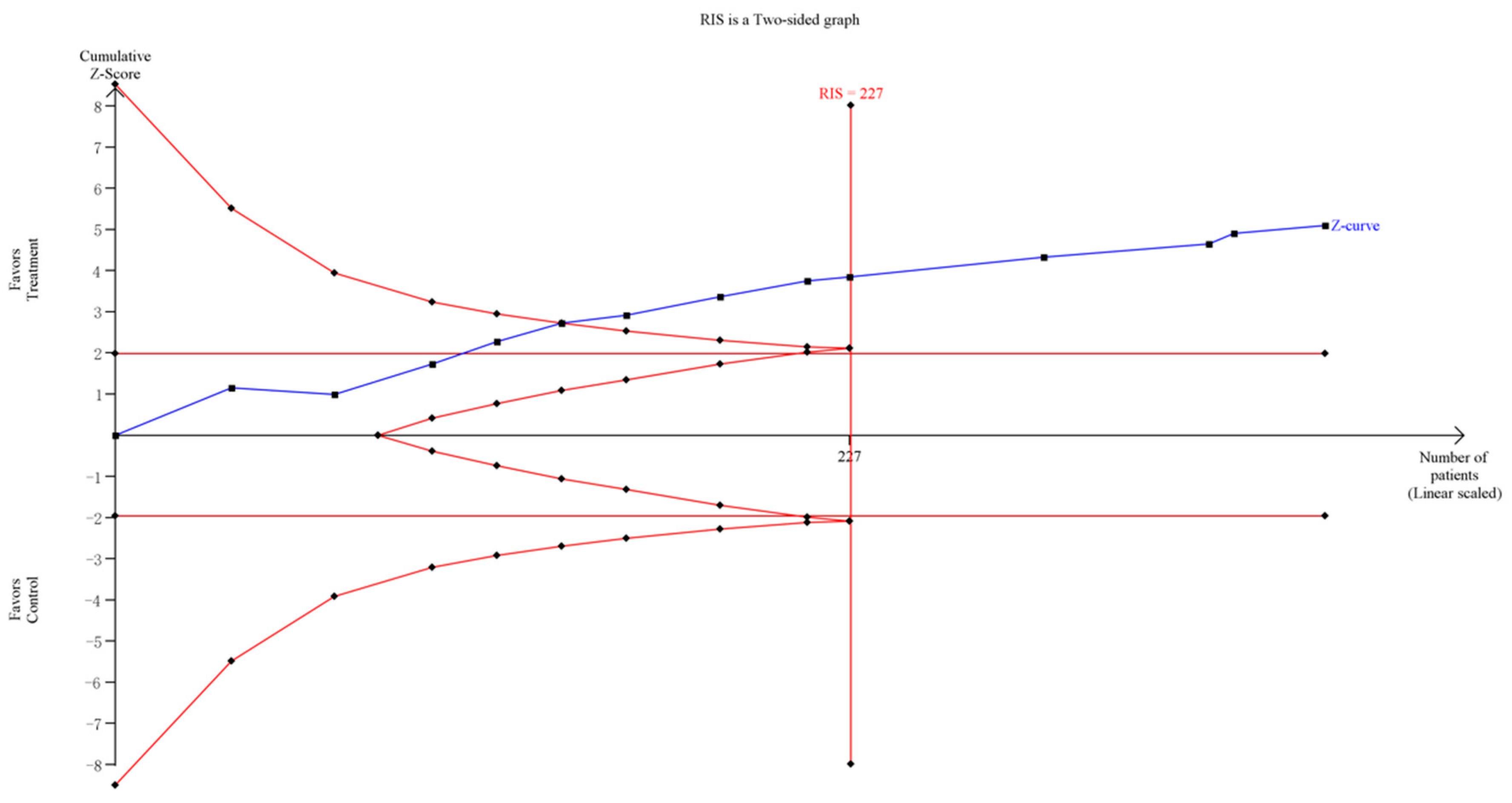
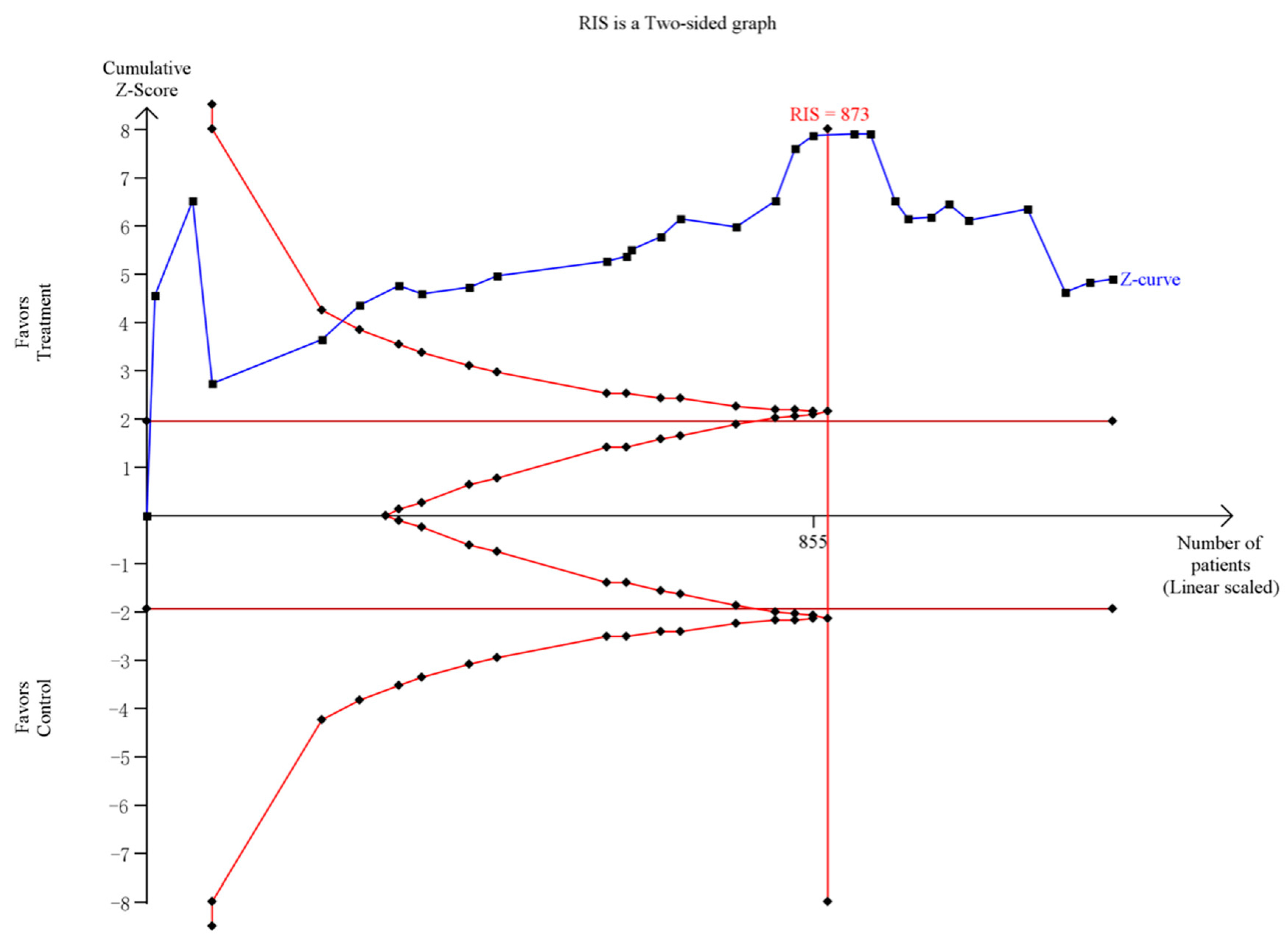
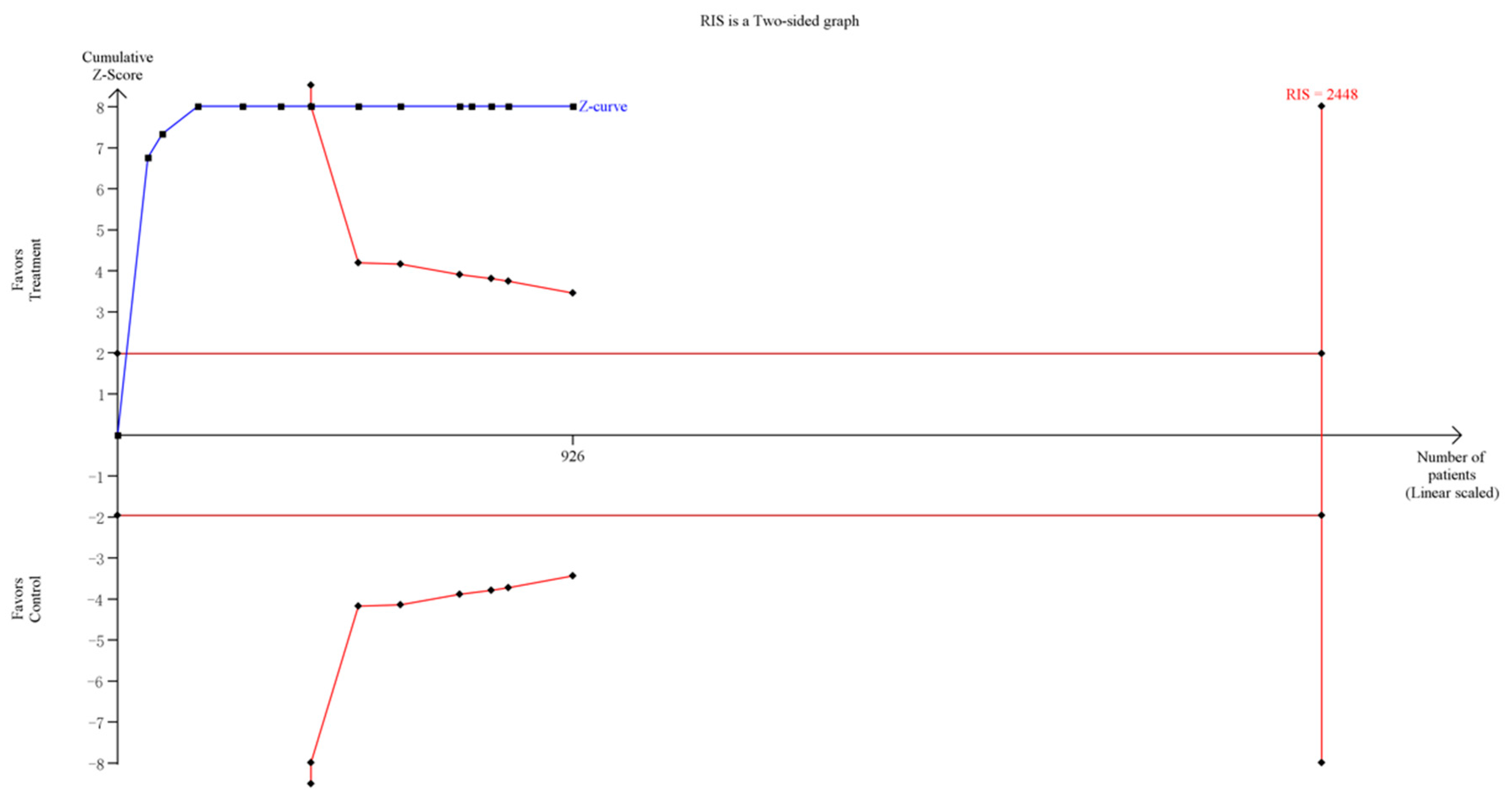
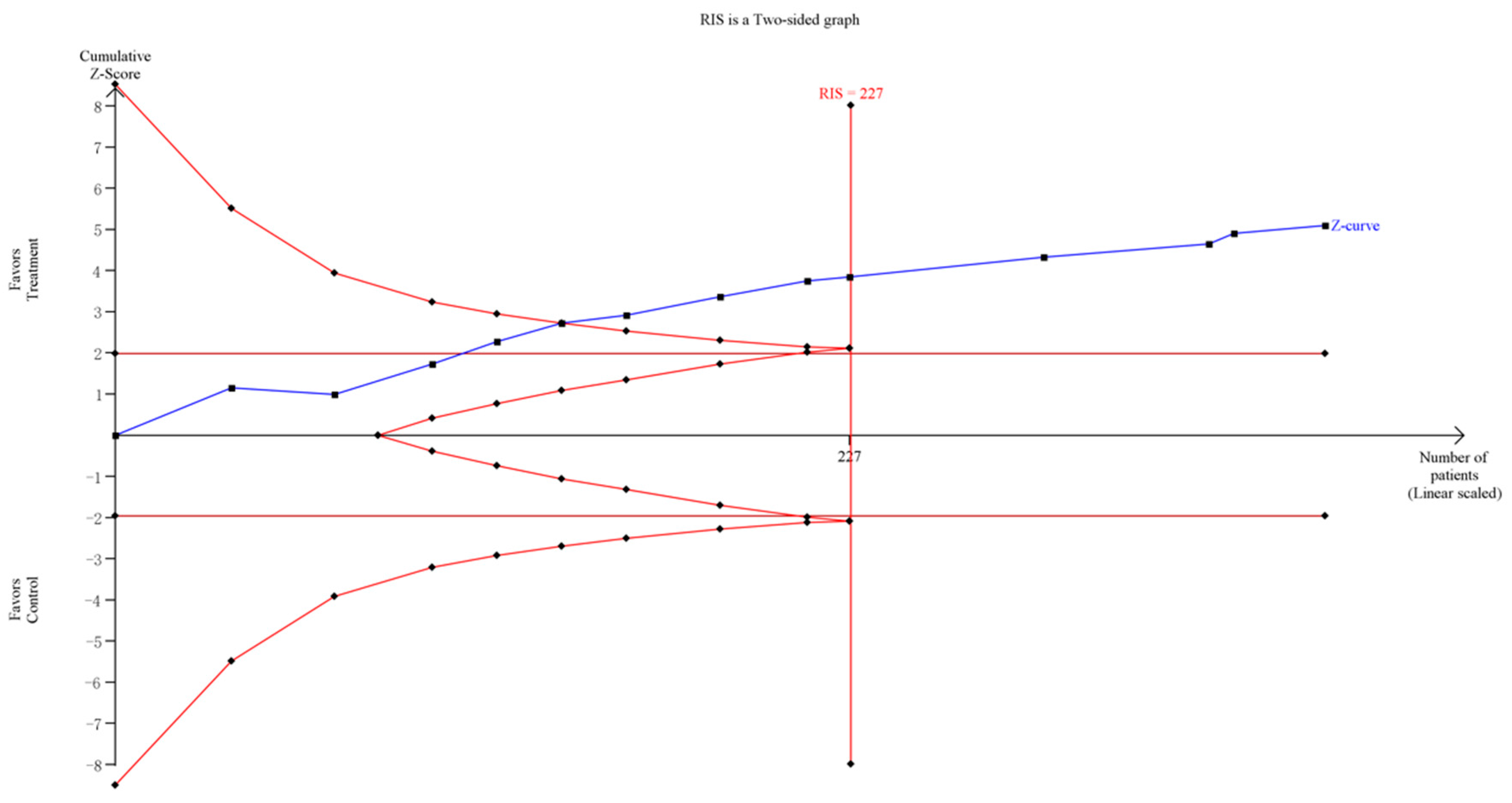
3.5. Trial Sequential Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Pontes, H.M.; Macur, M.; Griffiths, M.D. Internet Gaming Disorder among Slovenian Primary Schoolchildren: Findings From a Nationally Representative Sample of Adolescents. J. Behav. Addict. 2016, 5, 304–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammadbeigi, A.; Valizadeh, F.; Mirshojaee, S.R.; Ahmadli, R.; Mokhtari, M.; Ghaderi, E.; Ahmadi, A.; Rezaei, H.; Ansari, H. Self-rated Health and Internet Addiction in Iranian Medical Sciences Students, Prevalence, Risk Factors and Complications. Int. J. Biomed. Sci. 2016, 12, 65–70. [Google Scholar] [PubMed]
- Weinstein, A.; Lejoyeux, M. Internet addiction or excessive internet use. Am. J. Drug. Alcohol Abus. 2010, 36, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.S.; Zhang, Z.H.; Zhao, F.; Wang, W.J.; Li, Y.F.; Bi, L.; Qian, Z.Z.; Lu, S.S.; Feng, F.; Hu, C.Y.; et al. Prevalence of Internet addiction and its association with social support and other related factors among adolescents in China. J. Adolesc. 2016, 52, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; McKenzie, K. Socioeconomic and Geographic Inequalities of Internet Addiction in Korean Adolescents. Psychiatry Investig. 2015, 12, 559–562. [Google Scholar] [CrossRef] [PubMed]
- Seyrek, S.; Cop, E.; Sinir, H.; Ugurlu, M.; Şenel, S. Factors associated with Internet addiction: Cross-sectional study of Turkish adolescents. Pediatr. Int. Off. J. Jpn. Pediatr. Soc. 2017, 59, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Yeun, Y.R.; Han, S.J. Effects of Psychosocial Interventions for School-aged Children’s Internet Addiction, Self-control and Self-esteem: Meta-Analysis. Healthc. Inform. Res. 2016, 22, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Winkler, A.; Dörsing, B.; Rief, W.; Shen, Y.; Glombiewski, J.A. Treatment of internet addiction meta-analysis. Clin. Psychol. Rev. 2013, 33, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Park, S.M. A meta-analysis on the effects of adolescent internet addiction group counseling program in Korea. Korean J. Couns. Psychother. 2009, 21, 607–623. [Google Scholar]
- Oh, I.S.; Kim, C. Meta-analysis on the effects of the prevention and intervention programs for internet addiction. J. Korean Assoc. Inf. Educ. 2009, 13, 529–537. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses, the PRISMA statement. BMJ 2009, 3, e123–e130. [Google Scholar]
- West, C.P.; Dyrbye, L.N.; Erwin, P.J.; Shanafelt, T.D. Interventions to prevent and reduce physician burnout systematic review and meta-analysis. Lancet 2016, 388, 2272–2281. [Google Scholar] [CrossRef]
- Lee, J.; Lee, Y.; Gong, S.; Bae, J.; Choi, M. A meta-analysis of the effects of non-traditional teaching methods on the critical thinking abilities of nursing students. BMC Med. Educ. 2016, 16, 240. [Google Scholar] [CrossRef] [PubMed]
- Wetterslev, J.; Thorlund, K.; Brok, J.; Gluud, C. Trial sequential analysis may establish when firm evidence is reached in cumulative meta-analysis. J. Clin. Epidemiol. 2008, 61, 64–75. [Google Scholar] [CrossRef] [PubMed]
- Koyuncu, T.; Unsal, A.; Arslantas, D. Assessment of internet addiction and loneliness in secondary and high school students. J. Pak. Med. Assoc. 2014, 64, 998–1002. [Google Scholar] [PubMed]
- Li, W.; Zhang, W.; Xiao, L.; Nie, J. The association of Internet addiction symptoms with impulsiveness, loneliness, novelty seeking and behavioral inhibition system among adults with attention-deficit/hyperactivity disorder (ADHD). Psychiatry Res. 2016, 243, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Bozoglan, B.; Demirer, V.; Sahin, I. Loneliness, self-esteem, and life satisfaction as predictors of Internet addiction cross-sectional study among Turkish university students. Scand. J. Psychol. 2013, 54, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.L.; Gau, S.S. Sleep problems and internet addiction among children and adolescents longitudinal study. J. Sleep Res. 2016, 25, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.U. The effect of a R/T group counseling program on the Internet addiction level and self-esteem of Internet addiction university students. Forum Soc. Econ. 2015, 6, 41–49. [Google Scholar]
- Park, S.Y.; Kim, S.M.; Roh, S.; Soh, M.A.; Lee, S.H.; Kim, H.; Lee, Y.S.; Han, D.H. The effects of a virtual reality treatment program for online gaming addiction. Comput. Methods Programs Biomed. 2016, 129, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Ong, S.H.; Tan, Y.R. Internet addiction in young people. Ann. Acad. Med. Singap. 2014, 43, 378–382. [Google Scholar] [PubMed]
- Du, Y.S.; Jiang, W.; Vance, A. Longer term effect of randomized, controlled group cognitive behavioural therapy for Internet addiction in adolescent students in Shanghai. Aust. N. Z. J. Psychiatry 2010, 44, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Santos, V.; Nardi, A.E.; King, A.L. Treatment of internet addiction in patient with panic disorder and obsessive compulsive disorder case report. CNS Neurol. Disord. Drug Targets 2015, 14, 341–344. [Google Scholar] [CrossRef] [PubMed]
- Rupp, T.; Jubeau, M.; Millet, G.Y.; Wuyam, B.; Levy, P.; Verges, S.; Perrey, S. Muscle, prefrontal, and motor cortex oxygenation profiles during prolonged fatiguing exercise. Adv. Exp. Med. Biol. 2013, 789, 149–155. [Google Scholar] [PubMed]
- Morris, J.P.; Pelphrey, K.A.; McCarthy, G. Regional brain activation evoked when approaching a virtual human on a virtual walk. J. Cogn. Neurosci. 2005, 17, 1744–1752. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country | Total N | tNt0/tNt1 | cNt0/cNt1 | Hours of Intervention Applied | Participants | Follow up | Type of Treatment (Group/Individual) | Diagnostic Tools of Internet Addiction | Outcome Variables (Assessment Tools) |
|---|---|---|---|---|---|---|---|---|---|---|
| Li et al., 2014 [Table S1:1] | China | 30 | 15/15 | 15/15 | 12 | College student | NR | Group counseling program (group) | CIAS-R | IA and its subscales (CIAS-R); psychopathological symptoms (SCL-90) |
| Li et al., 2015 [Table S1:2] | China | 60 | 30/30 | 30/30 | 116 | College student | 2 months | Group counseling program (group) | CIAS | IA and its subscales (CIAS) |
| Duan et al., 2012 [Table S1:3] | China | 22 | 11/11 | 11/11 | 52–65 | College student | 3 months | Group counseling program (group) | YIAS | IA and its subscales(YIAS) |
| Ren et al., 2014 [Table S1:4] | China | 8 | 4/4 | 4/4 | 54–72 | College student | NR | Sports (group) | YIAS | IA (YIAS); psychopathological symptoms (SCL-90) |
| Cheng et al.,2015 [Table S1:5] | China | 23 | 12/12 | 11/11 | 24 | College student | NR | CBT (individual) | YIAS | IA (YIAS) |
| Zhao et al., 2015 [Table S1:6] | China | 77 | 36/32 | 45/45 | NR | College student | 1 month | Group counseling program (group) | YDQ | IA and its subscales (CIAS,YDQ); psychopathological symptoms (SCL-90); SE (SES) |
| Ma et al., 2011 [Table S1:7] | China | 8 | 4/4 | 4/4 | NR | College student | NR | Group counseling program (group) | YIAS | IA (YIAS) |
| Qu et al., 2006 [Table S1:8] | China | 12 | 6/6 | 6/6 | NR | College student | NR | Group counseling program (group) | YIAS | IA (YIAS) |
| Ma et al., 2011 [Table S1:9] | China | 98 | 49/49 | 49/49 | NR | College student | NR | CBT (individual) | YIAS | IA (YIAS) |
| Duan et al., 2013 [Table S1:10] | China | 22 | 11/11 | 11/11 | 65 | College student | NR | Group counseling program (group) | YIAS | IA and its subscales (YIAS) |
| Wen et al., 2008 [Table S1:11] | China | 140 | 60/60 | 80/80 | 40 | College student | 3 months | Group counseling program (group) | YIAS | IA (YIAS) |
| Zheng et al., 2010 [Table S1:12] | China | 61 | 30/30 | 31/31 | 6.6 | College student | NR | Group counseling program (group) | YDQ | IA (YDQ); psychopathological symptoms (SCL-90) |
| Zhao et al., 2015 [Table S1:13] | China | 48 | 24/24 | 24/24 | 16 | College student | NR | Group counseling program (group) | CIAS-R | IA (CIAS-R) |
| Chi et al., 2012 [Table S1:14] | China | 20 | 10/10 | 10/10 | 60 | College student | NR | Sports (group) | YIAS | IA (YIAS); psychopathological symptoms (SCL-90) |
| Guan et al., 2012 [Table S1:15] | China | 50 | 25/25 | 25/25 | 26 | College student | 3 months | Group counseling program (group) | CIAS | IA (CIAS) |
| Ming et al., 2014 [Table S1:16] | China | 120 | 60/60 | 60/60 | 120–160 | College student | NR | CBT (individual) | CIAS, YDQ | IA (YIAS); psychopathological symptoms (SCL-90) |
| Xu et al., 2012 [Table S1:17] | China | 26 | 13/13 | 13/13 | 24 | Secondary school student | 1 week | Group counseling program (group) | IAS | IA (IAS-R); psychopathological symptoms (SDS, SAS) |
| Chen et al., 2011 [Table S1:18] | China | 37 | 14/14 | 23/23 | NR | College student | NR | Group counseling program (group) | YIAS, CIAS-R | IA and its subscales (CIAS-R); psychopathological symptoms (SCL-90) |
| Zhang et al., 2013 [Table S1:19] | China | 60 | 30/30 | 30/30 | 64 | College student | NR | Sports (group) | YIAS | IA(YIAS) |
| Zhang et al., 2011 [Table S1:20] | China | 26 | 13/13 | 13/13 | 10.7 | Secondary school student | NR | Group counseling program (group) | APIUS | IA and its subscales (APIUS); psychopathological symptoms (MHSMS) |
| Li et al., 2009 [Table S1:21] | China | 92 | 48/44 | 48/48 | NR | Adolescents | Post-treatment; 8 weeks | CBT (individual) | YDQ | IA (CIAS, YDQ); psychopathological symptoms (SCL-90) |
| Guo et al., 2007 [Table S1:22] | China | 18 | 9/9 | 9/9 | 16 | Adolescents | NR | Sports (group) | YIAS, IAS | Psychopathological symptoms (SCL-90) |
| Guo et al., 2008 [Table S1:23] | China | 28 | 16/14 | 16/14 | 8–8.8 | College student and secondary school student | NR | CBT (group) | CIAS, YDQ | IA (CIAS); psychopathological symptoms (SCL-90) |
| Guo et al., 2006 [Table S1:24] | China | 18 | 9/9 | 9/9 | 16 | Adolescents | NR | CBT (individual) | YIAS, IAS | Psychopathological symptoms (SCL-90) |
| Lv et al., 2012 [Table S1:25] | China | 52 | 26/26 | 26/26 | 12 | College student | 6 weeks | Group counseling program (group) | CIAS | IA (CIAS) |
| Wang et al., 2012 [Table S1:26] | China | 72 | 36/36 | 36/36 | 12 | College student | NR | CBT (individual) | IAS | IA (YDQ) |
| Ming et al., 2014 [Table S1:27] | China | 58 | 28/28 | 30/30 | 20–30 | College student | NR | CBT (individual) | CIAS-R, YDQ | Psychopathological symptoms (SCL-90) |
| Zhao et al., 2010 [Table S1:28] | China | 47 | 36/32 | 45/45 | 120–160 | College student | 1 month | CBT (individual) | YDQ | IA and its subscales (CIAS, YDQ) |
| Zheng et al.,2013 [Table S1:29] | China | 41 | 20/20 | 21/21 | 21–28 | College student | Post-treatment; 3 months | Group counseling program (group) | YIAS, CIAS | Psychopathological symptoms (SCL-90); SE (SES) |
| Deng et al., 2014 [Table S1:30] | China | 48 | 24/24 | 24/24 | 25 | College student | NR | Sports (group) | CIAS | IA (CIAS); psychopathological symptoms (SCL-90) |
| Zhang et al., 2009 [Table S1:31] | China | 32 | 16/16 | 16/16 | NR | Secondary school student | Immediate | Sports (group) | CIAS | IA and its subscales (CIAS); psychopathological symptoms (SCL-90) |
| Wu et al., 2013 [Table S1:32] | China | 16 | 8/8 | 8/8 | 28–42 | College student | Immediate | Sports (group) | YDQ | Psychopathological symptoms (SCL-90) |
| Lou et al., 2010 [Table S1:33] | China | 36 | 18/18 | 18/18 | 54–72 | Secondary school student | Immediate | Sports (group) | YDQ | IA(YDQ) |
| Fu et al., 2010 [Table S1:34] | China | 32 | 16/16 | 16/16 | >24 | Secondary school student | NR | Sports (group) | YIAS | IA (YIAS); psychopathological symptoms (SCL-90) |
| Gao et al., 2012 [Table S1:35] | China | 69 | 35/35 | 34/34 | 135 | College student | NR | Sports (group) | YIAS | IA (YIAS); psychopathological symptoms (SCL-90) |
| Liu et al., 2013 [Table S1:36] | China | 32 | 16/16 | 15/15 | 24 | College student | 1 week | Group counseling program (group) | YIAS | IA (YIAS) |
| Bai et al., 2007 [Table S1:37] | China | 48 | 24/24 | 24/24 | 16 | College student | Post-treatment; 6 weeks | Group counseling program (group) | CIAS-R | IA (CIAS-R) |
| Zhou et al., 2010 [Table S1:38] | China | 18 | 9/9 | 9/9 | 16 | College student | NR | Group counseling program (group) | CIAS | IA (CIAS) |
| Zhao et al., 2016 [Table S1:39] | China | 130 | 65/65 | 65/65 | 96 | Adolescents | NR | CBT(group) | CIAS-R | IA (CIAS) |
| Mou et al., 2013 [Table S1:40] | China | 16 | 8/8 | 8/8 | 12 | College student | NR | Group counseling program (group) | CIAS-R, YDQ | IA (CIAS-R) |
| Kong et al., 2011 [Table S1:41] | China | 71 | 36/36 | 35/35 | 40 | College student | NR | Group counseling program (group) | YIAS | IA (YIAS) |
| Wang et al., 2008 [Table S1:42] | China | 48 | 24/24 | 24/24 | 24 | College student | Post-treatment; 1 month; 3 months | Group counseling program (group) | CIAS, YDQ | IA (CIAS) |
| Zhong et al., 2009 [Table S1:43] | China | 51 | 28/28 | 24/24 | NR | Adolescents | NR | Group counseling program (group) | OCS | IA (OCS) |
| Wu et al., 2009 [Table S1:44] | China | 30 | 15/15 | 15/15 | NR | College student | NR | Group counseling program (group) | CIAS, APUIS | IA and its subscales (CIAS-R, APIUS); psychopathological symptoms (SCL-90); SE (SES) |
| Liu et al., 2010 [Table S1:45] | China | 160 | 80/80 | 80/80 | 40 | College student | 3 month | Group counseling program (group) | YIAS | IA (YIAS) |
| Chen et al., 2010 [Table S1:46] | China | 61 | 30/30 | 31/31 | 6.6 | College student | NR | CBT (group) | YDQ | IA (YDQ); psychopathological symptoms (SCL-90) |
| Ge et al., 2014 [Table S1:47] | China | 24 | 12/12 | 12/12 | 10 | Children | Post-treatment; 1 month; 3 months | Group counseling program (group) | CIAS | IA and its subscales (CIAS) |
| Wang et al., 2009 [Table S1:48] | China | 112 | 56/56 | 56/56 | 48 | Adolescents | NR | Group counseling program (group) | YDQ | Psychopathological symptoms (SCL-90, SDS, SAS) |
| Zhang et al., 2013 [Table S1:49] | China | 84 | 42/42 | 42/42 | NR | College student | NR | CBT (individual) | CIAS | IA and its subscales (CIAS) |
| Feng et al., 2011 [Table S1:50] | China | 24 | 12/12 | 12/12 | 24 | College student | NR | Group counseling program (group) | IAS | IA (IAS) and its subscales; psychopathological symptoms (SRHMS) |
| Liao et al., 2008 [Table S1:51] | China | 50 | 20/20 | 30/30 | 35 | College student | Immediate | Sports (group) | CIAS | IA (CIAS); psychopathological symptoms (SCL-90) |
| Zhang et al., 2012 [Table S1:52] | China | 42 | 22/22 | 20/20 | 30 | College student | NR | Sports (group) | CIAS | IA and its subscales (CIAS) |
| Liu et al., 2014 [Table S1:53] | China | 24 | 12/12 | 12/12 | 16 | Secondary school student | 1 week | Group counseling program (group) | IAS | IA (IAS) |
| Cao et al., 2007 [Table S1:54] | China | 57 | 29/26 | 35/31 | 8–12 | Secondary school student | NR | CBT (group) | YDQ | IA (CIAS, YDQ) |
| Li et al., 2014 [Table S1:55] | China | 51 | 27/27 | 24/24 | 30 | Secondary school student | NR | Sports (group) | YIAS | IA (YIAS) |
| Kim et al., 2008 [Table S1:56] | Korea | 25 | 13/13 | 12/12 | 12.5 | College student | NR | Group counseling program (group) | K-IAS | IA and its subscales (K-IAS); SE (SES) |
| Zhang et al., 2016 [Table S1:57] | China | 40 | 23/23 | 17/17 | 16.47 | NR | NR | CBT (group) | CIAS | IA (CIAS) |
| Zhang et al., 2016 [Table S1:58] | China | 26 | 20/20 | 16/16 | 15 | NR | NR | CBT (group) | CIAS | IA (CIAS) |
| Outcome | N | SMD | Lower | Upper | Q | I2 | p |
|---|---|---|---|---|---|---|---|
| IA | 30 | −1.37 | −1.89 | −0.85 | 412.08 | 93.00% | p < 0.001 |
| Relapse | 4 | −0.10 | −0.40 | 0.20 | 0.2 | 0.00% | 0.98 |
| College student | 24 | −1.52 | −2.11 | −0.92 | 365.29 | 93.70% | p < 0.001 |
| Secondary school student | 2 | −1.39 | −2.00 | −0.78 | 0.27 | 0.00% | 0.61 |
| Long-term | 8 | −1.88 | −2.65 | −1.11 | 74.82 | 90.60% | p < 0.001 |
| Short-term | 15 | −1.21 | −2.09 | −0.33 | 239.94 | 94.20% | p < 0.001 |
| Time management | 10 | −0.42 | −0.76 | −0.09 | 19.36 | 53.50% | 0.02 |
| Interpersonal and health issues | 9 | −0.93 | −1.50 | −0.37 | 40.67 | 80.30% | p < 0.001 |
| Tolerance | 11 | −0.58 | −1.04 | −0.11 | 43.04 | 76.80% | p < 0.001 |
| Withdrawal symptoms | 6 | −0.53 | −1.38 | 0.32 | 41.51 | 88.00% | p < 0.001 |
| Compulsive Internet use | 10 | −0.65 | −1.15 | −0.15 | 41.15 | 78.10% | p < 0.001 |
| GSI | 6 | −0.47 | −0.98 | 0.04 | 16.11 | 69.00% | 0.01 |
| Somatization | 4 | −1.71 | −4.13 | 0.71 | 138.2 | 97.80% | p < 0.001 |
| Obsessive-compulsive | 5 | −0.97 | −1.76 | −0.17 | 30.47 | 86.90% | p < 0.001 |
| Social insecurity | 4 | −1.59 | −3.34 | 0.16 | 78.56 | 96.20% | p < 0.001 |
| Depression | 6 | −1.61 | −2.96 | −0.25 | 99.27 | 96.00% | p < 0.001 |
| Anxiousness | 6 | −1.58 | −3.11 | −0.05 | 124.68 | 96.80% | p < 0.001 |
| Aggressiveness | 5 | −2.29 | −4.39 | −0.19 | 144.61 | 97.20% | p < 0.001 |
| Phobic anxiety | 4 | −0.83 | −2.41 | 0.75 | 74.62 | 96.00% | p < 0.001 |
| Paranoid ideation | 5 | −0.98 | −2.18 | 0.21 | 64.28 | 93.80% | p < 0.001 |
| Psychoticism | 4 | −0.73 | −1.97 | 0.50 | 47.69 | 93.70% | p < 0.001 |
| SES | 4 | 0.50 | −0.62 | 1.62 | 33.44 | 91.00% | p < 0.001 |
| Outcome | N | SMD | Lower | Upper | Q | I2 | p |
|---|---|---|---|---|---|---|---|
| IA | 13 | −1.88 | −2.53 | −1.23 | 198.25 | 93.90% | p < 0.001 |
| Group | 7 | −1.53 | −1.89 | −1.16 | 185.64 | 96.80% | p < 0.001 |
| Individual | 6 | −1.88 | −2.53 | −1.23 | 10.3 | 51.40% | 0.07 |
| College student | 7 | −1.84 | −2.95 | −0.73 | 162.57 | 96.30% | p < 0.001 |
| Secondary school student | 1 | −2.08 | −3.45 | −0.70 | 0 | NA | p < 0.001 |
| Long-term | 7 | −1.80 | −2.33 | −1.26 | 40.98 | 85.40% | p < 0.001 |
| Short-term | 3 | −1.68 | −4.78 | 1.42 | 120.95 | 98.30% | p < 0.001 |
| Time management | 2 | −0.74 | −2.49 | 1.02 | 27.26 | 96.30% | p < 0.001 |
| Interpersonal and health issues | 2 | −0.94 | −3.42 | 1.54 | 48.76 | 97.90% | p < 0.001 |
| Tolerance | 2 | −0.67 | −3.09 | 1.75 | 48.72 | 97.90% | p < 0.001 |
| Withdrawal symptoms | 1 | 0.91 | 0.43 | 1.38 | 0 | NA | p < 0.001 |
| Compulsive Internet use | 2 | −1.14 | −4.25 | 1.98 | 68.36 | 98.50% | p < 0.001 |
| GSI | 4 | −2.24 | −3.60 | −0.88 | 76.40 | 96.10% | p < 0.001 |
| Somatization | 4 | −1.22 | −1.51 | −0.93 | 1.79 | 0.00% | 0.62 |
| Obsessive-compulsive | 4 | −0.57 | −1.17 | 0.04 | 11.48 | 73.90% | 0.01 |
| Social insecurity | 4 | −1.46 | −2.70 | −0.21 | 38.75 | 92.30% | p < 0.001 |
| Depression | 4 | −1.93 | −3.33 | −0.52 | 42.27 | 92.90% | p < 0.001 |
| Anxiousness | 4 | −1.48 | −2.75 | −0.21 | 40.11 | 92.50% | p < 0.001 |
| Aggressiveness | 4 | −1.01 | −1.63 | −0.38 | 11.38 | 73.60% | 0.01 |
| Phobic anxiety | 4 | −1.27 | −2.01 | −0.54 | 14.66 | 79.50% | p < 0.001 |
| Paranoid ideation | 4 | −1.04 | −1.64 | −0.43 | 10.57 | 71.60% | 0.01 |
| Psychoticism | 4 | −1.69 | −2.82 | −0.56 | 30.12 | 90.00% | p < 0.001 |
| Outcome | N | SMD | Lower | Upper | Q | I2 | p |
|---|---|---|---|---|---|---|---|
| IA | 8 | −1.70 | −2.14 | −1.26 | 28.48 | 67.50% | p < 0.001 |
| Mild IA | 3 | −2.6 | −3.44 | −1.75 | 2.91 | 31.40% | 0.23 |
| Moderate IA | 3 | −2.35 | −3.00 | −1.69 | 0.08 | 0.00% | 0.96 |
| Serious IA | 2 | −0.76 | −1.47 | −0.05 | 0.01 | 0.00% | 0.91 |
| College student | 6 | −1.89 | −2.30 | −1.48 | 10.64 | 34.20% | 0.16 |
| Secondary school student | 2 | −1.70 | −2.73 | −0.66 | 4.04 | 75.20% | 0.04 |
| Long-term | 4 | −1.92 | −2.37 | −1.47 | 6.79 | 26.30% | 0.24 |
| Short-term | 3 | −1.98 | −2.70 | −1.27 | 4.50 | 55.50% | 0.11 |
| Time management | 3 | −0.93 | −1.32 | −0.53 | 0.43 | 0.00% | 0.81 |
| Interpersonal and health issues | 3 | −0.34 | −1.30 | 0.63 | 11.88 | 83.20% | p < 0.001 |
| Tolerance | 3 | −0.95 | −1.52 | −0.37 | 4.06 | 50.80% | 0.13 |
| Withdrawal symptoms | 3 | −1.07 | −1.48 | −0.67 | 1.57 | 0.00% | 0.46 |
| Compulsive Internet use | 3 | −2.58 | −4.54 | −0.61 | 28.21 | 92.90% | p < 0.001 |
| GSI | 3 | −1.01 | −1.55 | −0.47 | 0.52 | 0.00% | 0.77 |
| Somatization | 5 | −0.79 | −1.15 | −0.44 | 1.6 | 0.00% | 0.81 |
| Obsessive-compulsive | 5 | −0.51 | −1.05 | 0.03 | 8.69 | 53.90% | 0.07 |
| Social insecurity | 5 | −0.64 | −1.07 | −0.21 | 5.67 | 29.50% | 0.23 |
| Depression | 5 | −0.85 | −1.20 | −0.49 | 1.19 | 0.00% | 0.88 |
| Anxiousness | 5 | −0.90 | −1.26 | −0.55 | 2.82 | 0.00% | 0.59 |
| Aggressiveness | 5 | −0.62 | −0.97 | −0.27 | 3.45 | 0.00% | 0.49 |
| Phobic anxiety | 5 | −0.52 | −0.97 | −0.08 | 6.23 | 35.80% | 0.18 |
| Paranoid ideation | 5 | −0.60 | −0.95 | −0.26 | 2.38 | 0.00% | 0.67 |
| Psychoticism | 5 | −0.53 | −0.97 | −0.08 | 6.15 | 34.90% | 0.19 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, J.; Nie, J.; Wang, Y. Effects of Group Counseling Programs, Cognitive Behavioral Therapy, and Sports Intervention on Internet Addiction in East Asia: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2017, 14, 1470. https://doi.org/10.3390/ijerph14121470
Liu J, Nie J, Wang Y. Effects of Group Counseling Programs, Cognitive Behavioral Therapy, and Sports Intervention on Internet Addiction in East Asia: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2017; 14(12):1470. https://doi.org/10.3390/ijerph14121470
Chicago/Turabian StyleLiu, Jun, Jing Nie, and Yafeng Wang. 2017. "Effects of Group Counseling Programs, Cognitive Behavioral Therapy, and Sports Intervention on Internet Addiction in East Asia: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 14, no. 12: 1470. https://doi.org/10.3390/ijerph14121470