
Traffic-Related Air Pollution and Childhood Asthma: Recent Advances and Remaining Gaps in the Exposure Assessment Methods


Abstract
:1. Introduction
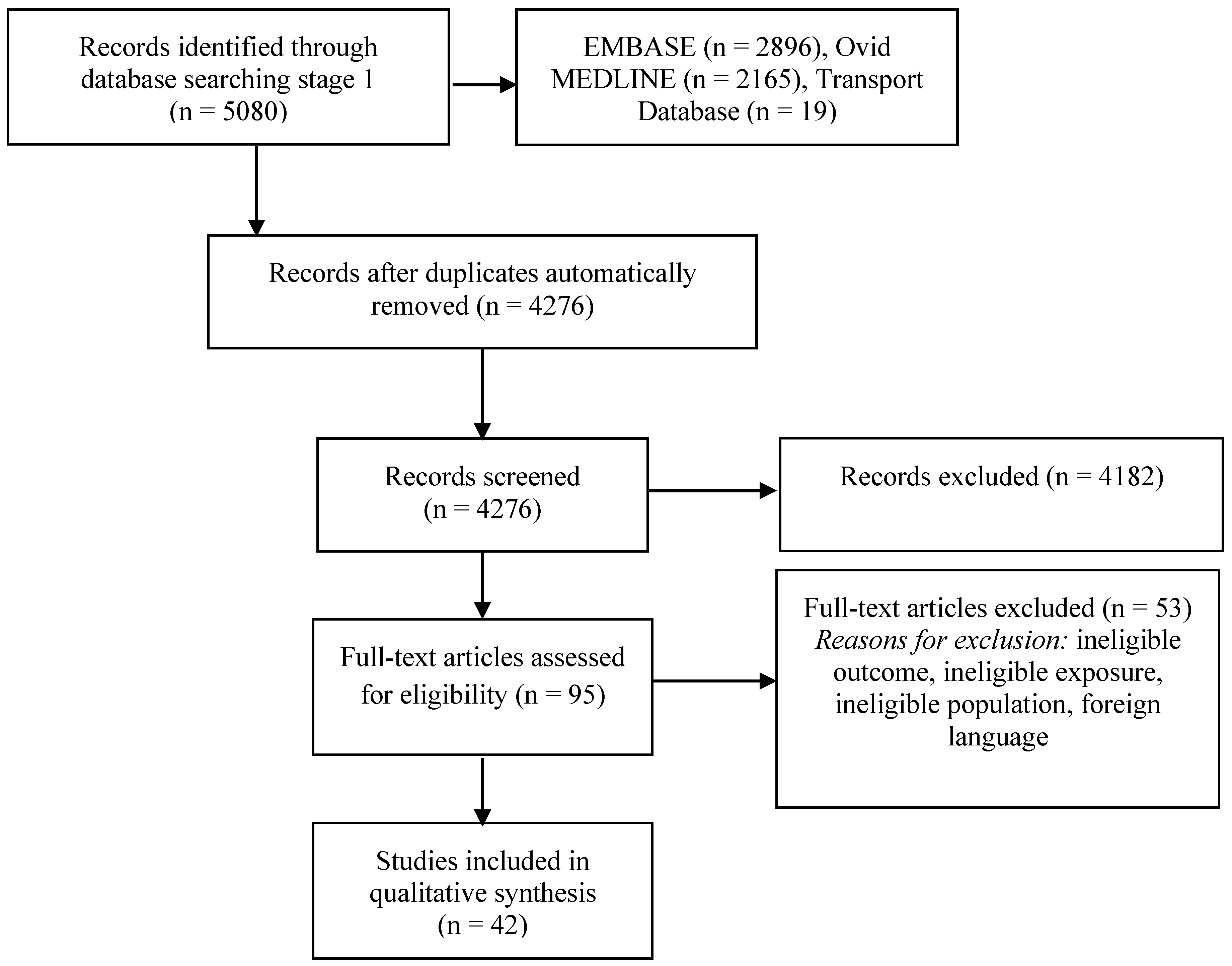
2. Methods
- “Child*” AND “air pollution” AND “asthma”;
- “Child*” AND “air quality” AND “asthma”;
- “Child*” AND “vehicle emissions” AND “asthma”; and
- “Child*” AND “ultra-fine particles” AND “asthma”.
- Were published epidemiological/observational studies;
- Explicitly specified the term “asthma” as an outcome for investigation;
- Examined the childhood exposure from birth until 18 years old [35] to any designated TRAP metric or established traffic-related air pollutant including proximity to roads or traffic, carbon monoxide (CO), elemental carbon (EC), nitrogen oxides (NOx), nitric oxide (NO), NO2, hydrocarbons, particles of different aerodynamic diameters (PM2.5, PM10, PMcoarse, UFPs) or PM2.5 absorbance as a marker for black carbon (BC) concentrations [10,36]; and
- Examined and reported associations between preceding exposure to TRAP and subsequent risk of asthma reported as incidence or lifetime prevalence from birth until 18 years old.
- Study reference and setting;
- Study design;
- Age group;
- Number of participants;
- Exposure assessment method(s);
- Pollutant(s) studied;
- Exposure assessment place;
- Exposure assessment time; and
- Air pollution estimates validation, if any.
3. Results
3.1. Overview
3.2. Exposure Assessment Methods
3.3. Pollutants Studied
3.4. Exposure Assessment Place and Time (Windows)
3.5. Exposure Assessment Validation
3.6. Risk Estimates by Exposure Assessment Model
4. Discussion
4.1. Putative Agents
4.2. Exposure Assessment Methods
4.3. Exposure Assessment Places and Time Windows
4.4. Outlook and Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Perez, L.; Declercq, C.; Iñiguez, C.; Aguilera, I.; Badaloni, C.; Ballester, F.; Bouland, C.; Chanel, O.; Cirarda, F.; Forastiere, F.; et al. Chronic burden of near-roadway traffic pollution in 10 european cities (APHEKOM network). Eur. Respir. J. 2013, 42, 594–605. [Google Scholar] [CrossRef] [PubMed]
- Milligan, K.L.; Matsui, E.; Sharma, H. Asthma in urban children: Epidemiology, environmental risk factors, and the public health domain. Curr. Allergy Asthma Rep. 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Khreis, H.; Kelly, C.; Tate, J.; Parslow, R.; Lucas, K.; Nieuwenhuijsen, M. Exposure to traffic-related air pollution and risk of development of childhood asthma: A systematic review and meta-analysis. Environ. Int. 2017, 100, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Committee on the Medical Effects of Air Pollutants (COMEAP). Asthma and Air Pollution; COMEAP: London, UK, 2014.
- London, S.J. Gene–air pollution interactions in asthma. Proc. Am. Thorac. Soc. 2007, 4, 217. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Sioutas, C.; Cho, A.; Schmitz, D.; Misra, C.; Sempf, J.; Wang, M.; Oberley, T.; Froines, J.; Nel, A. Ultrafine particulate pollutants induce oxidative stress and mitochondrial damage. Environ. Health Perspect. 2003, 111, 455. [Google Scholar] [CrossRef] [PubMed]
- Kelly, F.J. Oxidative stress: Its role in air pollution and adverse health effects. Occup. Environ. Med. 2003, 60, 612–616. [Google Scholar] [CrossRef] [PubMed]
- Sundvor, I.; Castell Balaguer, N.; Viana, M.; Querol, X.; Reche, C.; Amato, F.; Mellios, G.; Guerreiro, C. Road Traffic’s Contribution to Air Quality in European Cities, ETC/ACM Technical Paper 2012/14. Available online: http://acm.eionet.europa.eu/reports/docs/ETCACM_TP_2012_14_traffic_contribution_city_aq.pdf (accessed on 17 April 2016).
- Victoria Transport Policy Institute. Transportation Cost and Benefit Analysis II—Air Pollution Costs; Victoria Transport Policy Institute: Victoria, BC, Canada, 2013. [Google Scholar]
- Vardoulakis, S.; Fisher, B.E.; Pericleous, K.; Gonzalez-Flesca, N. Modelling air quality in street canyons: A review. Atmos. Environ. 2003, 37, 155–182. [Google Scholar] [CrossRef]
- Jerrett, M.; Arain, A.; Kanaroglou, P.; Beckerman, B.; Potoglou, D.; Sahsuvaroglu, T.; Morrison, J.; Giovis, C. A review and evaluation of intraurban air pollution exposure models. J. Expo. Sci. Environ. Epidemiol. 2005, 15, 185–204. [Google Scholar] [CrossRef] [PubMed]
- Beelen, R.; Voogt, M.; Duyzer, J.; Zandveld, P.; Hoek, G. Comparison of the performances of land use regression modelling and dispersion modelling in estimating small-scale variations in long-term air pollution concentrations in a Dutch urban area. Atmos. Environ. 2010, 44, 4614–4621. [Google Scholar] [CrossRef]
- Sellier, Y.; Galineau, J.; Hulin, A.; Caini, F.; Marquis, N.; Navel, V.; Bottagisi, S.; Giorgis-Allemand, L.; Jacquier, C.; Slama, R.; et al. Health effects of ambient air pollution: Do different methods for estimating exposure lead to different results? Environ. Int. 2014, 66, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Gulliver, J.; de Hoogh, K.; Fecht, D.; Vienneau, D.; Briggs, D. Comparative assessment of gis-based methods and metrics for estimating long-term exposures to air pollution. Atmos. Environ. 2011, 45, 7072–7080. [Google Scholar] [CrossRef]
- Anderson, H.R.; Favarato, G.; Atkinson, R.W. Long-term exposure to air pollution and the incidence of asthma: Meta-analysis of cohort studies. Air Qual. Atmos. Health 2013, 6, 47–56. [Google Scholar] [CrossRef]
- Khreis, H.; De Hoogh, K.; Mueller, N.; Rojas-Rueda, D.; Tate, J.; Lucas, K.; Parslow, R.; Nieuwenhuijsen, M.J. Traffic-related air pollution and the local chronic burden of childhood asthma in Bradford, UK. 2017; in preparation. [Google Scholar]
- Health Effects Institute. Traffic-Related Air Pollution: A Critical Review of the Literature on Emissions, Exposure, and Health Effects; Special Report 17 of the HEI Panel on the Health Effects of Traffic-Related Air Pollution; Health Effects Institute: Boston, MA, USA, 2010. [Google Scholar]
- Akers, J.; Aguiar-Ibáñez, R.; Baba-Akbari Sari, A. CRD’S Guidance for Undertaking Reviews in Health Care; University of York Centre for Reviews and Dissemination (CRD): York, UK, 2009. [Google Scholar]
- Khreis, H.; Kelly, C.; Tate, J.; Parslow, R. Exposure to Traffic-Related Air Pollution and the Development of Childhood Asthma. Prospero 2014: Crd42014015448. Available online: http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42014015448 (accessed on 12 September 2016).
- Vitnerova, N.; Horstman, D.; Hnizdova, E. Prevalence priznaku chorob dychaciho traktu u deti skolniho veku Zijicich v oblastech s rozdilnym znecistenim Ovzdusi. Hygiena 1999, 44, 30–39. [Google Scholar]
- Salameh, P.; Karaki, C.; Awada, S.; Rachidi, S.; Al Hajje, A.; Bawab, W.; Saleh, N.; Waked, M. Asthme, pollutions intérieure et extérieure: Tude pilote chez des adolescents libanais scolarisés. Rev. Mal. Respir. 2015, 32, 692–704. [Google Scholar] [CrossRef] [PubMed]
- Veremchuk, L.; Cherpack, N.; Gvozdenko, T.; Volkova, M. Methodology for the assessment of the impact of the atmospheric air pollution on the formation of the levels of overall morbidity rate of bronchial asthma. Gig. Sanit. 2014, 94, 119–122. [Google Scholar]
- Braback, L.; Forsberg, B. Does traffic exhaust contribute to the development of asthma and allergic sensitization in children: Findings from recent cohort studies. Environ. Health 2009, 8, 17. [Google Scholar] [CrossRef] [PubMed]
- Gasana, J.; Dillikar, D.; Mendy, A.; Forno, E.; Ramos Vieira, E. Motor vehicle air pollution and asthma in children: A meta-analysis. Environ. Res. 2012, 117, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Gowers, A.M.; Cullinan, P.; Ayres, J.G.; Anderson, H.; Strachan, D.P.; Holgate, S.T.; Mills, I.C.; Maynard, R.L. Does outdoor air pollution induce new cases of asthma? Biological plausibility and evidence: A review. Respirology 2012, 17, 887–898. [Google Scholar] [CrossRef] [PubMed]
- Salam, M.T.; Islam, T.; Gilliland, F.D. Recent evidence for adverse effects of residential proximity to traffic sources on asthma. Curr. Opin. Pulm. Med. 2008, 14, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Sarnat, J.A.; Holguin, F. Asthma and air quality. Curr. Opin. Pulm. Med. 2007, 13, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.W.K.; Leung, T.F. The effects of air pollution on asthma in children. Clin. Pulm. Med. 2005, 12, 1–6. [Google Scholar] [CrossRef]
- Bowatte, G.; Lodge, C.; Lowe, A.J.; Erbas, B.; Perret, J.; Abramson, M.J.; Matheson, M.; Dharmage, S. The influence of childhood traffic-Elated air pollution exposure on asthma, allergy and sensitization: A systematic review and a meta-Analysis of birth cohort studies. Allergy 2015, 70, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Favarato, G.; Anderson, H.R.; Atkinson, R.; Fuller, G.; Mills, I.; Walton, H. Traffic-related pollution and asthma prevalence in children. Quantification of associations with nitrogen dioxide. Air Qual. Atmos. Health 2014, 7, 459–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, A.; Janssen, N.A.; Brunekreef, B.; Cassee, F.R.; Hoek, G.; Gehring, U. Children’s respiratory health and oxidative potential of PM2.5: The piama birth cohort study. Occup. Environ. Med. 2016, 73, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Han, Y.; Seo, S.C.; Lee, J.Y.; Choi, J.; Kim, K.H.; Woo, S.-Y.; Kim, E.-H.; Kwon, H.-J.; Cheong, H.K.; et al. Association of carbon monoxide levels with allergic diseases in children. Allergy Asthma Proc. 2016, 37, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Hasunuma, H.; Sato, T.; Iwata, T.; Kohno, Y.; Nitta, H.; Odajima, H.; Ohara, T.; Omori, T.; Ono, M.; Yamazaki, S.; et al. Association between traffic-related air pollution and asthma in preschool children in a national japanese nested case–control study. BMJ Open 2016, 6, e010410. [Google Scholar] [CrossRef] [PubMed]
- Rancière, F.; Bougas, N.; Viola, M.; Momas, I. Early exposure to traffic-related air pollution, respiratory symptoms at 4 years of age, and potential effect modification by parental allergy, stressful family events, and gender: A prospective follow-up study of the paris birth cohort. Environ. Health Perspect. 2016. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Maternal, Newborn, Child and Adolescent Health: Adolescent Development. Available online: http://www.who.int/maternal_child_adolescent/topics/adolescence/dev/en/ (accessed on 29 March 2016).
- Krämer, U.; Sugiri, D.; Ranft, U.; Krutmann, J.; von Berg, A.; Berdel, D.; Behrendt, H.; Kuhlbusch, T.; Hochadel, M.; Wichmann, H.-E.; et al. Eczema, respiratory allergies, and traffic-related air pollution in birth cohorts from small-town areas. J. Dermatol. Sci. 2009, 56, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Clark, N.A.; Demers, P.A.; Karr, C.J.; Koehoorn, M.; Lencar, C.; Tamburic, L.; Brauer, M. Effect of early life exposure to air pollution on development of childhood asthma. Environ. Health Perspect. 2010, 118, 284. [Google Scholar] [CrossRef] [PubMed]
- Dell, S.D.; Jerrett, M.; Beckerman, B.; Brook, J.R.; Foty, R.G.; Gilbert, N.L.; Marshall, L.; Miller, J.D.; To, T.; Walter, S.D.; et al. Presence of other allergic disease modifies the effect of early childhood traffic-related air pollution exposure on asthma prevalence. Environ. Int. 2014, 65, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Gehring, U.; Wijga, A.H.; Brauer, M.; Fischer, P.; de Jongste, J.C.; Kerkhof, M.; Oldenwening, M.; Smit, H.A.; Brunekreef, B. Traffic-related air pollution and the development of asthma and allergies during the first 8 years of life. Am. J. Respir. Crit. Care Med. 2010, 181, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Gruzieva, O.; Bergström, A.; Hulchiy, O.; Kull, I.; Lind, T.; Melén, E.; Moskalenko, V.; Pershagen, G.; Bellander, T. Exposure to air pollution from traffic and childhood asthma until 12 years of age. Epidemiology 2013, 24, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, A.; Stroh, E.; Björk, J.; Jakobsson, K. Asthma incidence in children growing up close to traffic: A registry-based birth cohort. Environ. Health 2013, 12, 91. [Google Scholar] [CrossRef] [PubMed]
- McConnell, R.; Islam, T.; Shankardass, K.; Jerrett, M.; Lurmann, F.; Gilliland, F.; Gauderman, J. Childhood incident asthma and traffic-related air pollution at home and school. Environ. Health Perspect. 2010, 118, 1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishimura, K.K.; Galanter, J.M.; Roth, L.A.; Oh, S.S.; Thakur, N.; Nguyen, E.A.; Thyne, S.; Farber, H.J.; Serebrisky, D.; Kumar, R.; et al. Early-life air pollution and asthma risk in minority children. The GALA II and SAGE II studies. Am. J. Respir. Crit. Care Med. 2013, 188, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.M.; Quinn, J.W.; Jung, K.H.; Hoepner, L.; Diaz, D.; Perzanowski, M.; Rundle, A.; Kinney, P.L.; Perera, F.P.; Miller, R.L. Traffic density and stationary sources of air pollution associated with wheeze, asthma, and immunoglobulin e from birth to age 5 years among New York city children. Environ. Res. 2011, 111, 1222–1229. [Google Scholar] [CrossRef] [PubMed]
- Ranzi, A.; Porta, D.; Badaloni, C.; Cesaroni, G.; Lauriola, P.; Davoli, M.; Forastiere, F. Exposure to air pollution and respiratory symptoms during the first 7 years of life in an italian birth cohort. Occup. Environ. Med. 2014, 71, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Brunst, K.J.; Ryan, P.H.; Brokamp, C.; Bernstein, D.; Reponen, T.; Lockey, J.; Khurana Hershey, G.K.; Levin, L.; Grinshpun, S.A.; LeMasters, G. Timing and duration of traffic-related air pollution exposure and the risk for childhood wheeze and asthma. Am. J. Respir. Crit. Care Med. 2015, 192, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Gehring, U.; Wijga, A.H.; Hoek, G.; Bellander, T.; Berdel, D.; Brüske, I.; Fuertes, E.; Gruzieva, O.; Heinrich, J.; Hoffmann, B.; et al. Exposure to air pollution and development of asthma and rhinoconjunctivitis throughout childhood and adolescence: A population-based birth cohort study. Lancet Respir. Med. 2015, 3, 933–942. [Google Scholar] [CrossRef]
- Gehring, U.; Beelen, R.; Eeftens, M.; Hoek, G.; de Hoogh, K.; de Jongste, J.C.; Keuken, M.; Koppelman, G.H.; Meliefste, K.; Oldenwening, M.; et al. Particulate matter composition and respiratory health: The piama birth cohort study. Epidemiology 2015, 26, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Ryan, P.H.; LeMasters, G.K.; Levin, L.; Burkle, J.; Biswas, P.; Hu, S.; Grinshpun, S.; Reponen, T. A land-use regression model for estimating microenvironmental diesel exposure given multiple addresses from birth through childhood. Sci. Total Environ. 2008, 404, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Mölter, A.; Agius, R.; de Vocht, F.; Lindley, S.; Gerrard, W.; Custovic, A.; Simpson, A. Effects of long-term exposure to PM10 and NO2 on asthma and wheeze in a prospective birth cohort. J. Epidemiol. Community Health 2014, 68, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Mölter, A.; Simpson, A.; Berdel, D.; Brunekreef, B.; Custovic, A.; Cyrys, J.; de Jongste, J.; de Vocht, F.; Fuertes, E.; Gehring, U.; et al. A multicentre study of air pollution exposure and childhood asthma prevalence: The escape project. Eur. Respir. J. 2015, 45, 610–624. [Google Scholar] [CrossRef] [PubMed]
- MacIntyre, E.A.; Brauer, M.; Melén, E.; Bauer, C.P.; Bauer, M.; Berdel, D.; Bergström, A.; Brunekreef, B.; Chan-Yeung, M.; Klümper, C.; et al. Gstp1 and TNF gene variants and associations between air pollution and incident childhood asthma: The traffic, asthma and genetics (TAG) study. Environ. Health Perspect. 2014, 122, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Gauderman, W.J.; Avol, E.; Lurmann, F.; Kuenzli, N.; Gilliland, F.; Peters, J.; McConnell, R. Childhood asthma and exposure to traffic and nitrogen dioxide. Epidemiology 2005, 16, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Gruzieva, O.; Bellander, T.; Eneroth, K.; Kull, I.; Melén, E.; Nordling, E.; van Hage, M.; Wickman, M.; Moskalenko, V.; Hulchiy, O.; et al. Traffic-related air pollution and development of allergic sensitization in children during the first 8 years of life. J. Allergy Clin. Immunol. 2012, 129, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Henderson, S.B.; Beckerman, B.; Jerrett, M.; Brauer, M. Application of land use regression to estimate long-term concentrations of traffic-related nitrogen oxides and fine particulate matter. Environ. Sci. Technol. 2007, 41, 2422–2428. [Google Scholar] [CrossRef] [PubMed]
- Hochadel, M.; Heinrich, J.; Gehring, U.; Morgenstern, V.; Kuhlbusch, T.; Link, E.; Wichmann, H.-E.; Krämer, U. Predicting long-term average concentrations of traffic-related air pollutants using gis-based information. Atmos. Environ. 2006, 40, 542–553. [Google Scholar] [CrossRef]
- Jerrett, M.; Arain, M.; Kanaroglou, P.; Beckerman, B.; Crouse, D.; Gilbert, N.; Brook, J.; Finkelstein, N.; Finkelstein, M. Modeling the intraurban variability of ambient traffic pollution in Toronto, Canada. J. Toxicol. Environ. Health Part A 2007, 70, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Morgenstern, V.; Zutavern, A.; Cyrys, J.; Brockow, I.; Gehring, U.; Koletzko, S.; Bauer, C.-P.; Reinhardt, D.; Wichmann, H.-E.; Heinrich, J. Respiratory health and individual estimated exposure to traffic-related air pollutants in a cohort of young children. Occup. Environ. Med. 2007, 64, 8–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oftedal, B.; Walker, S.-E.; Gram, F.; McInnes, H.; Nafstad, P. Modelling long-term averages of local ambient air pollution in Oslo, Norway: Evaluation of nitrogen dioxide, PM10 and PM2.5. Int. J. Environ. Pollut. 2008, 36, 110–126. [Google Scholar] [CrossRef]
- Stroh, E.; Rittner, R.; Oudin, A.; Ardö, J.; Jakobsson, K.; Björk, J.; Tinnerberg, H. Measured and modeled personal and environmental NO2 exposure. Popul. Health Metr. 2012. [Google Scholar] [CrossRef] [PubMed]
- Ryan, P.H.; LeMasters, G.K.; Biswas, P.; Levin, L.; Hu, S.; Lindsey, M.; Bernstein, D.I.; Lockey, J.; Villareal, M.; Hershey, G.K.K.; et al. A comparison of proximity and land use regression traffic exposure models and wheezing in infants. Environ. Health Perspect. 2007, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Beelen, R.; Hoek, G.; Vienneau, D.; Eeftens, M.; Dimakopoulou, K.; Pedeli, X.; Tsai, M.-Y.; Künzli, N.; Schikowski, T.; Marcon, A.; et al. Development of NO2 and NOx land use regression models for estimating air pollution exposure in 36 study areas in europe–the escape project. Atmos. Environ. 2013, 72, 10–23. [Google Scholar] [CrossRef]
- Eeftens, M.; Beelen, R.; de Hoogh, K.; Bellander, T.; Cesaroni, G.; Cirach, M.; Declercq, C.; Dedele, A.; Dons, E.; de Nazelle, A.; et al. Development of land use regression models for PM2.5, PM2.5 absorbance, PM10 and pmcoarse in 20 European study areas; results of the escape project. Environ. Sci. Technol. 2012, 46, 11195–11205. [Google Scholar] [CrossRef] [PubMed]
- Crouse, D.L.; Goldberg, M.S.; Ross, N.A. A prediction-based approach to modelling temporal and spatial variability of traffic-related air pollution in Montreal, Canada. Atmos. Environ. 2009, 43, 5075–5084. [Google Scholar] [CrossRef]
- Nordling, E.; Berglind, N.; Melén, E.; Emenius, G.; Hallberg, J.; Nyberg, F.; Pershagen, G.; Svartengren, M.; Wickman, M.; Bellander, T. Traffic-related air pollution and childhood respiratory symptoms, function and allergies. Epidemiology 2008, 19, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Bellander, T.; Berglind, N.; Gustavsson, P.; Jonson, T.; Nyberg, F.; Pershagen, G.; Järup, L. Using geographic information systems to assess individual historical exposure to air pollution from traffic and house heating in Stockholm. Environ. Health Perspect. 2001, 109, 633. [Google Scholar] [CrossRef] [PubMed]
- Brauer, M.; Hoek, G.; Smit, H.; De Jongste, J.; Gerritsen, J.; Postma, D.S.; Kerkhof, M.; Brunekreef, B. Air pollution and development of asthma, allergy and infections in a birth cohort. Eur. Respir. J. 2007, 29, 879–888. [Google Scholar] [CrossRef] [PubMed]
- Brauer, M.; Hoek, G.; Van Vliet, P.; Meliefste, K.; Fischer, P.H.; Wijga, A.; Koopman, L.P.; Neijens, H.J.; Gerritsen, J.; Kerkhof, M.; et al. Air pollution from traffic and the development of respiratory infections and asthmatic and allergic symptoms in children. Am. J. Respir. Crit. Care Med. 2002, 166, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Carlsten, C.; Dybuncio, A.; Becker, A.; Chan-Yeung, M.; Brauer, M. Traffic-related air pollution and incident asthma in a high-risk birth cohort. Occup. Environ. Med. 2011, 68, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.; Lu, C.; Norbäck, D.; Bornehag, C.-G.; Zhang, Y.; Liu, W.; Yuan, H.; Sundell, J. Early life exposure to ambient air pollution and childhood asthma in China. Environ. Res. 2015, 143, 83–92. [Google Scholar] [CrossRef] [PubMed]
- English, P.; Neutra, R.; Scalf, R.; Sullivan, M.; Waller, L.; Zhu, L. Examining associations between childhood asthma and traffic flow using a geographic information system. Environ. Health Perspect. 1999, 107, 761. [Google Scholar] [CrossRef] [PubMed]
- Fuertes, E.; Standl, M.; Cyrys, J.; Berdel, D.; von Berg, A.; Bauer, C.-P.; Krämer, U.; Sugiri, D.; Lehmann, I.; Koletzko, S.; et al. A longitudinal analysis of associations between traffic-related air pollution with asthma, allergies and sensitization in the GINIplus and LISAplus birth cohorts. PeerJ 2013, 1, e193. [Google Scholar] [CrossRef] [PubMed]
- Gehring, U.; Cyrys, J.; Sedlmeir, G.; Brunekreef, B.; Bellander, T.; Fischer, P.; Bauer, C.; Reinhardt, D.; Wichmann, H.; Heinrich, J. Traffic-related air pollution and respiratory health during the first 2 yrs of life. Eur. Respir. J. 2002, 19, 690–698. [Google Scholar] [CrossRef] [PubMed]
- Jerrett, M.; Shankardass, K.; Berhane, K.; Gauderman, W.J.; Künzli, N.; Avol, E.; Gilliland, F.; Lurmann, F.; Molitor, J.N.; Molitor, J.T.; et al. Traffic-related air pollution and asthma onset in children: A prospective cohort study with individual exposure measurement. Environ. Health Perspect. 2008, 116, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Kerkhof, M.; Postma, D.; Brunekreef, B.; Reijmerink, N.; Wijga, A.; De Jongste, J.; Gehring, U.; Koppelman, G. Toll-like Receptor 2 and 4 genes influence susceptibility to adverse effects of traffic-related air pollution on childhood asthma. Thorax 2010, 65, 690–697. [Google Scholar] [CrossRef] [PubMed]
- LeMasters, G.; Levin, L.; Bernstein, D.I.; Lockey, S.D.; Lockey, J.E.; Burkle, J.; Khurana Hershey, G.K.; Brunst, K.; Ryan, P.H. Secondhand smoke and traffic exhaust confer opposing risks for asthma in normal and overweight children. Obesity 2015, 23, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Morgenstern, V.; Zutavern, A.; Cyrys, J.; Brockow, I.; Koletzko, S.; Kramer, U.; Behrendt, H.; Herbarth, O.; von Berg, A.; Bauer, C.P.; et al. Atopic diseases, allergic sensitization, and exposure to traffic-related air pollution in children. Am. J. Respir. Crit. Care Med. 2008, 177, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Oftedal, B.; Nystad, W.; Brunekreef, B.; Nafstad, P. Long-term traffic-related exposures and asthma onset in schoolchildren in Oslo, Norway. Environ. Health Perspect. 2009, 117, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Shima, M.; Adachi, M. Effect of outdoor and indoor nitrogen dioxide on respiratory symptoms in schoolchildren. Int. J. Epidemiol. 2000, 29, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Shima, M.; Nitta, Y.; Adachi, M. Traffic-related air pollution and respiratory symptoms in children living along trunk roads in Chiba prefecture, Japan. J. Epidemiol. 2003, 13, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Shima, M.; Nitta, Y.; Ando, M.; Adachi, M. Effects of air pollution on the prevalence and incidence of asthma in children. Arch. Environ. Health 2002, 57, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Wang, I.-J.; Tung, T.-H.; Tang, C.-S.; Zhao, Z.-H. Allergens, air pollutants, and childhood allergic diseases. Int. J. Hyg. Environ. Health 2016, 219, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, S.; Shima, M.; Nakadate, T.; Ohara, T.; Omori, T.; Ono, M.; Sato, T.; Nitta, H. Association between traffic-related air pollution and development of asthma in school children: Cohort study in Japan. J. Expo. Sci. Environ. Epidemiol. 2014, 24, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Zmirou, D.; Gauvin, S.; Pin, I.; Momas, I.; Sahraoui, F.; Just, J.; Le Moullec, Y.; Bremont, F.; Cassadou, S.; Reungoat, P.; et al. Traffic related air pollution and incidence of childhood asthma: Results of the Vesta case-control study. J. Epidemiol. Community Health 2004, 58, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Tétreault, L.-F.; Doucet, M.; Gamache, P.; Fournier, M.; Brand, A.; Kosatsky, T.; Smargiassi, A. Childhood exposure to ambient air pollutants and the onset of asthma: An administrative cohort study in Québec. Environ. Health Perspect. 2016, 124, 1276–1282. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.; Lu, C.; Ou, C.; Chen, L.; Yuan, H. Preconceptional, prenatal and postnatal exposure to outdoor and indoor environmental factors on allergic diseases/symptoms in preschool children. Chemosphere 2016, 152, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Huang, C.; Hu, Y.; Fu, Q.; Zou, Z.; Sun, C.; Shen, L.; Wang, X.; Cai, J.; Pan, J. Associations of gestational and early life exposures to ambient air pollution with childhood respiratory diseases in shanghai, china: A retrospective cohort study. Environ. Int. 2016, 92, 284–293. [Google Scholar] [CrossRef] [PubMed]
- Héroux, M.-E.; Anderson, H.R.; Atkinson, R.; Brunekreef, B.; Cohen, A.; Forastiere, F.; Hurley, F.; Katsouyanni, K.; Krewski, D.; Krzyzanowski, M.; et al. Quantifying the health impacts of ambient air pollutants: Recommendations of a who/europe project. Int. J. Public Health 2015, 60, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Vineis, P.; Chadeau-Hyam, M.; Gmuender, H.; Gulliver, J.; Herceg, Z.; Kleinjans, J.; Kogevinas, M.; Kyrtopoulos, S.; Nieuwenhuijsen, M.; Phillips, D.; et al. The exposome in practice: Design of the exposomics project. Int. J. Hyg. Environ. Health 2016. [Google Scholar] [CrossRef] [PubMed]
- Timmers, V.R.; Achten, P.A. Non-exhaust pm emissions from electric vehicles. Atmos. Environ. 2016, 134, 10–17. [Google Scholar] [CrossRef]
- Gulliver, J.; de Hoogh, K.; Hansell, A.; Vienneau, D. Development and back-extrapolation of NO2 land use regression models for historic exposure assessment in Great Britain. Environ. Sci. Technol. 2013, 47, 7804–7811. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Henderson, S.B.; Sbihi, H.; Allen, R.W.; Brauer, M. Temporal stability of land use regression models for traffic-related air pollution. Atmos. Environ. 2013, 64, 312–319. [Google Scholar] [CrossRef]
- Cesaroni, G.; Porta, D.; Badaloni, C.; Stafoggia, M.; Eeftens, M.; Meliefste, K.; Forastiere, F. Nitrogen dioxide levels estimated from land use regression models several years apart and association with mortality in a large Cohort study. Environ. Health 2012, 11, 48. [Google Scholar] [CrossRef] [PubMed]
- Carslaw, D.; Beevers, S.; Westmoreland, E.; Williams, M.; Tate, J.; Murrells, T.; Stedman, J.; Li, Y.; Grice, S.; Kent, A.; et al. Trends in NOx and NO2 Emissions and Ambient Measurements in the UK; DEFRA: London, UK, 2011.
- De Hoogh, K.; Korek, M.; Vienneau, D.; Keuken, M.; Kukkonen, J.; Nieuwenhuijsen, M.J.; Badaloni, C.; Beelen, R.; Bolignano, A.; Cesaroni, G. Comparing land use regression and dispersion modelling to assess residential exposure to ambient air pollution for epidemiological studies. Environ. Int. 2014, 73, 382–392. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Gehring, U.; Hoek, G.; Keuken, M.; Jonkers, S.; Beelen, R.; Eeftens, M.; Postma, D.S.; Brunekreef, B. Air pollution and lung function in dutch children: A comparison of exposure estimates and associations based on land use regression and dispersion exposure modeling approaches. Environ. Health Perspect. 2015, 123, 847. [Google Scholar] [CrossRef] [PubMed]
- Korek, M.; Johansson, C.; Svensson, N.; Lind, T.; Beelen, R.; Hoek, G.; Pershagen, G.; Bellander, T. Can dispersion modeling of air pollution be improved by land-use regression? An example from Stockholm, Sweden. J. Expo. Sci. Environ. Epidemiol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuijsen, M.J.; Donaire-Gonzalez, D.; Rivas, I.; De Castro, M.; Cirach, M.; Hoek, G.; Seto, E.; Jerrett, M.; Sunyer, J. Variability in and agreement between modeled and personal continuously measured black carbon levels using novel smartphone and sensor technologies. Environ. Sci. Technol. 2015, 49, 2977–2982. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Pu, Z.; Li, M.; Sundell, J. Characterizing the indoor-outdoor relationship of fine particulate matter in non-heating season for urban residences in Beijing. PLoS ONE 2015, 10, e0138559. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Morawska, L.; He, C.; Zhang, Y.L.; Ayoko, G.; Cao, M. Characterization of particle number concentrations and PM2.5 in a school: Influence of outdoor air pollution on indoor air. Environ. Sci. Pollut. Res. 2010, 17, 1268–1278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cyrys, J.; Pitz, M.; Bischof, W.; Wichmann, H.-E.; Heinrich, J. Relationship between indoor and outdoor levels of fine particle mass, particle number concentrations and black smoke under different ventilation conditions. J. Expo. Sci. Environ. Epidemiol. 2004, 14, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Vrijheid, M.; Slama, R.; Robinson, O.; Chatzi, L.; Coen, M.; van den Hazel, P.; Thomsen, C.; Wright, J.; Athersuch, T.J.; Avellana, N.; et al. The human early-life exposome (HELIX): Project rationale and design. Environ. Health Perspect. 2014, 122, 535–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Study Reference | Setting | Study Design | Age Group (Years) | Participants Included in the Analysis | Exposure Assessment | Pollutant(s) |
|---|---|---|---|---|---|---|
| Brauer, Hoek, Van Vliet, Meliefste, Fischer, Wijga, Koopman, Neijens, Gerritsen and Kerkhof [68] | The Netherlands, north, west and center communities | Birth cohort (PIAMA) | Birth–2 | 2989 | LUR modelling | BC, NO2, PM2.5 |
| Brauer, Hoek, Smit, De Jongste, Gerritsen, Postma, Kerkhof and Brunekreef [67] | The Netherlands, north, west and center communities | Follow-up on Brauer et al. (2002) | Birth–4 | 2826 | LUR modelling | BC, NO2, PM2.5 |
| Brunst, Ryan, Brokamp, Bernstein, Reponen, Lockey, Khurana Hershey, Levin, Grinshpun and LeMasters [46] | USA, Cincinnati | Birth cohort (CCAAPS) | Birth–7 | 589 | LUR modelling | EC |
| Carlsten, Dybuncio, Becker, Chan-Yeung and Brauer [69] | Canada, Vancouver | Birth cohort (CAPPS) | Birth–7 | 184 | LUR modelling | BC, NO, NO2, PM2.5 |
| Clark, Demers, Karr, Koehoorn, Lencar, Tamburic and Brauer [37] | Canada, Southwestern British Columbia | Case-control nested in British Columbia birth cohort | Birth–4 | 37,401 | LUR modelling, monitoring data at closest three monitors weighted by inverse distance to child’s residence, proximity to highways/major roads | BC, CO, NO, NO2, PM10, PM2.5 |
| Fuertes, Standl, Cyrys, Berdel, von Berg, Bauer, Krämer, Sugiri, Lehmann and Koletzko [72] | Germany | 2 birth cohorts (GINIplus and LISAplus) | 3–10 | 4585 | LUR modelling | BC, NO2, PM2.5 |
| Gehring, Cyrys, Sedlmeir, Brunekreef, Bellander, Fischer, Bauer, Reinhardt, Wichmann and Heinrich [73] | Germany, Munich | 2 birth cohorts (GINI and LISA) | Birth–2 | 1756 | LUR modelling | BC, NO2, PM2.5 |
| Gehring, Wijga, Brauer, Fischer, de Jongste, Kerkhof, Oldenwening, Smit and Brunekreef [39] | The Netherlands, north, west and center communities | Follow-up on Brauer et al. (2007) | Birth–8 | 3143 | LUR modelling | BC, NO2, PM2.5 |
| Gehring, Beelen, Eeftens, Hoek, de Hoogh, de Jongste, Keuken, Koppelman, Meliefste and Oldenwening [48] | The Netherlands, north, west and center communities | Follow-up on Gehring et al. (2010) | Birth–12 | 3702 | LUR modelling | BC, NO2, PM2.5, PM10, PMcoarse and PM composition elements: copper (Cu), iron (Fe), zinc (Zn), nickel (Ni), sulfur (S), vanadium (V) |
| Gehring, Wijga, Hoek, Bellander, Berdel, Brüske, Fuertes, Gruzieva, Heinrich and Hoffmann [47] | Sweden, Germany, The Netherlands | Pooled data from four birth cohorts: BAMSE; GINIplus; LISAplus and PIAMA | Birth–16 | 14,126 | LUR modelling | BC, NO2, PM2.5, PM10, PMcoarse |
| Gruzieva, Bergström, Hulchiy, Kull, Lind, Melén, Moskalenko, Pershagen and Bellander [40] | Sweden, Stockholm | Birth cohort (BAMSE) | Birth–12 | 3633 | Dispersion modelling (Airviro, street canyon contribution for 160 houses) | NOx, PM10 |
| Jerrett, Shankardass, Berhane, Gauderman, Künzli, Avol, Gilliland, Lurmann, Molitor and Molitor [74] | USA, 11 southern Californian communities | Cohort (CHS) | 10–18 | 209 | NO2 Palmes tubes monitoring for 2 weeks in 2 seasons at the child’s residence | NO2 |
| Kerkhof, Postma, Brunekreef, Reijmerink, Wijga, De Jongste, Gehring and Koppelman [75] | The Netherlands, north, west and center communities | Birth cohort (PIAMA) | Birth–8 | 916 | LUR modelling | BC, NO2, PM2.5 |
| Krämer, Sugiri, Ranft, Krutmann, von Berg, Berdel, Behrendt, Kuhlbusch, Hochadel and Wichmann [36] | Germany, Wesel | 2 birth cohorts (GINIplus and LISAplus) | 4–6 | 2059 | LUR modelling, distance to next major road traversed by more than 10,000 cars/day | BC, NO2 |
| LeMasters, Levin, Bernstein, Lockey, Lockey, Burkle, Khurana Hershey, Brunst and Ryan [76] | USA, Cincinnati | Birth cohort (CCAAPS) | Birth–7 | 575 | LUR modelling | EC |
| Lindgren, Stroh, Björk and Jakobsson [41] | Sweden, Scania | Birth cohort | Birth–6 | 6007 | Dispersion modelling (AERMOD), traffic intensity on road with heaviest traffic within 100 m around residence | NOx |
| MacIntyre, Brauer, Melén, Bauer, Bauer, Berdel, Bergström, Brunekreef, Chan-Yeung, Klümper, Fuertes, Gehring, Gref, Heinrich, Herbarth, Kerkhof, Koppelman, Kozyrskyj, Pershagen, Postma, Thiering, Tiesler, Carlsten and Group [52] | Sweden, Canada, Germany, The Netherlands | Pooled data from 6 birth cohorts: BAMSE; CAPPS; GINI; LISA; PIAMA; SAGE | Birth–8 | 5115 | LUR modelling, dispersion modelling for BAMSE only | NO2 (sensitivity analyses for BC and PM2.5) |
| McConnell, Islam, Shankardass, Jerrett, Lurmann, Gilliland and Gauderman [42] | USA, 13 southern Californian communities | Cohort (CHS) | Kindergarten/first grade–fourth grade | 2497 | Dispersion modelling for NOx (CALINE 4), monitoring data for NO2, PM2.5, PM10, distance to nearest freeway or other highways or arterial roads, traffic density within 150 m around residence and school | NOx, NO2, PM2.5, PM10 |
| Mölter, Agius, de Vocht, Lindley, Gerrard, Custovic and Simpson [50] | England, Greater Manchester | Birth cohort (MAAS) | Birth–11 | 1108 | Microenvironmental exposure model (LUR modelling for outdoor and INDAIR for indoor environments, indoor to outdoor ratios: journey to school and school) | NO2, PM10 |
| Mölter, Simpson, Berdel, Brunekreef, Custovic, Cyrys, de Jongste, de Vocht, Fuertes and Gehring [51] | ESCAPE multi-center analysis, England, Sweden, Germany, The Netherlands | Pooled data from 5 birth cohorts: MAAS, BAMSE, PIAMA, GINI, LISA (South and North) | Birth–10 | 10,377 | LUR modelling, traffic intensity on the nearest street, traffic intensity on major roads within a 100-m radius | BC, NO2, NOx, PM2.5, PM10, PMcoarse |
| Morgenstern, Zutavern, Cyrys, Brockow, Gehring, Koletzko, Bauer, Reinhardt, Wichmann and Heinrich [58] | Germany, Munich Metropolitan area | 2 birth cohorts (GINI and LISA)—extension on Gehring et al. (2002) | Birth–2 | 3577 | LUR modelling, living close to major road | BC, NO2, PM2.5 |
| Morgenstern, Zutavern, Cyrys, Brockow, Koletzko, Kramer, Behrendt, Herbarth, von Berg and Bauer [77] | Germany, Munich | 2 birth cohorts (GINI and LISA) | 4–6 | 2436 | LUR modelling, minimum distance to next motorway, federal or state road | BC, NO2, PM2.5 |
| Oftedal, Nystad, Brunekreef and Nafstad [78] | Norway, Oslo | Oslo birth cohort and sample from simultaneous cross-sectional study | Birth–10 | 2329 | Dispersion modelling (EPISODE), distance to main transport routes with any form of motor transport | NO2 |
| Patel, Quinn, Jung, Hoepner, Diaz, Perzanowski, Rundle, Kinney, Perera and Miller [44] | USA, New York | Birth cohort (CCCEH) | Birth–5 | 593 | Proximity to roadways, roadway density, truck route density, four-way street intersection density, number of bus stops, percentage of building area designated for commercial use | NA |
| Rancière [34] | Paris, France | Birth cohort (PARIS) | Birth–4 | 2015 | Dispersion modelling | NOx |
| Ranzi, Porta, Badaloni, Cesaroni, Lauriola, Davoli and Forastiere [45] | Italy, Rome | Birth cohort (GASPII) | Birth–7 | 672 | LUR modelling, proximity to high traffic roads | NO2 |
| Shima and Adachi [79] | Japan, 7 Chiba Prefecture communities | Cohort | 9/10–12/13 | 842 | Monitoring data | NO2 |
| Shima, Nitta, Ando and Adachi [81] | Japan, 8 Chiba Prefecture communities | Cohort | 6–12 | 1910 | Monitoring data | NO2, PM10 |
| Shima, Nitta and Adachi [80] | Japan, 8 Chiba Prefecture communities | Cohort | 6/9–10/13 | 1858 | Distance to trunk roads | NA |
| Tétreault, Doucet, Gamache, Fournier, Brand, Kosatsky and Smargiassi [85] | Canada, Québec | Birth cohort | Birth–12 | 1,133,938 | LUR modelling for NO2, satellite imagery for PM2.5 | NO2, PM2.5 |
| Wang, Tung, Tang and Zhao [82] | Taiwan, 11 communities in Taipei | Cohort (CEAS) | Birth–kindergarten (average age 5.5 ± 1.1) | 2661 | Monitoring data | CO, NO2, PM2.5, PM10 |
| Yamazaki, Shima, Nakadate, Ohara, Omori, Ono, Sato and Nitta [83] | Japan, 57 elementary schools | Cohort (SORA) | 6–9 | 10,069 | Dispersion modelling for outdoor and indoor concentrations, living near heavily trafficked roads | EC, NOx |
| Yang, Janssen, Brunekreef, Cassee, Hoek and Gehring [31] | The Netherlands, north, west and center communities | Birth cohort (PIAMA) | Birth-14 | 3701 | LUR modelling | Oxidative Potential, BC, NO2, PM2.5, copper (Cu), iron (Fe), zinc (Zn), nickel (Ni), sulfur (S), vanadium (V) |
| Dell, Jerrett, Beckerman, Brook, Foty, Gilbert, Marshall, Miller, To and Walter [38] | Canada, Toronto | Case-control | 5–9 | 1497 | LUR modelling, monitoring data weighted by inverse distance to child’s residence, distance to highways/major roadways | NO2 |
| English, Neutra, Scalf, Sullivan, Waller and Zhu [71] | USA, San Diego | Case-control | ≤14 | 8280 | Average daily traffic on streets within a 168-m buffer around residence | NA |
| Hasunuma, Sato, Iwata, Kohno, Nitta, Odajima, Ohara, Omori, Ono and Yamazaki [33] | Japan, 9 cities and wards | Case-control (nested in SORA) | 1.5–3 | 416 | Dispersion modelling including indoor concentration assuming an infiltration rate from outdoor concentration, distance from heavily trafficked roads | EC, NOx |
| [43] | USA, Chicago, Bronx, Houston, San Francisco, Puerto Rico | 2 case-controls (GALA II and SAGE II) | 8–21 | 3015 | Monitoring data at closest four monitors weighted by inverse distance squared to child’s residence | NO2, PM2.5, PM10 |
| Zmirou, Gauvin, Pin, Momas, Sahraoui, Just, Le Moullec, Bremont, Cassadou and Reungoat [84] | France, Paris, Nice, Toulouse, Clermont-Ferrand, Grenoble | Case-control (VESTA) | 4–14 | 390 | Traffic density within 300 m to road distance ratio | NA |
| Deng, Lu, Norbäck, Bornehag, Zhang, Liu, Yuan and Sundell [70] | China, Changsha | Cross-sectional (CCHH) | 3–6 | 2490 | Monitoring data weighted by inverse distance to child’s kindergarten | NO2, PM10 (as a mixture surrogate) |
| Deng, Lu, Ou, Chen and Yuan [86] | China, Changsha | Cross-sectional (CCHH) | 3–6 | 2598 | Monitoring data weighted by inverse distance to child’s kindergarten | NO2, PM10 (as a mixture surrogate) |
| [32] | Korea, 45 elementary schools | Cross-sectional | 6–7 | 1828 | Monitoring data | CO, NO2, PM10 |
| Liu, Huang, Hu, Fu, Zou, Sun, Shen, Wang, Cai and Pan [87] | China, Shanghai | Cross-sectional (CCHH) | 4–6 | 3358 | Monitoring data | NO2, PM10 |
| Exposure Model | Resolution | Specificity to Traffic | Pros | Cons | |
|---|---|---|---|---|---|
| Spatial | Temporal | ||||
| TRAP surrogates main e.g., proximity to “major roads” or “freeways” | - | -- | + | Intuitive, simple and cost effective, more insightful when complemented with vehicle counts and composition, low need for updated data. | Assumes a road of a certain type or size corresponds to a certain amount of traffic, sometime uses self-reported traffic intensity (collected via questionnaires) which can be subjective, assumes all pollutants disperse similarly (limited directional dependence), cannot consider street canyon effects, generally does not consider compounded effects of proximity to multiple roads, disregards exposure variability due to mobility/individual activity. |
| Air pollutants measurements from fixed-site monitoring stations | -- | ++ | -- | High and continuous temporal resolution, actual measurements rather than predictions, cost-effective, can provide large sample sizes, medium need for updated data. | Not present at all locations, locations usually based on regulatory (not scientific) purposes, cannot consider street canyon effects (unless located in a street canyon), conceals persons’ differences because of a mismatch between data used to estimate exposure and actual subjects’ locations, potential for significant amounts of missing data in practice, quality of the data depends on quality of data ratification and verification, disregards exposure variability due to mobility/individual activity. |
| Air pollutant measurements from residential (stationary) samplers | ++ | - | - | Provides individualized data, captures spatial variability in exposure between study subjects, actual measurements rather than predictions, cost effective for select pollutants (e.g., NO2), medium need for updated data. | Only practical/feasible in small timeframes and populations, logistic and costs concerns, not available or cost prohibitive (e.g., ultra-fine particles) for all pollutants of concern, disregards exposure variability due to mobility/individual activity. |
| Remote sensing | + | - | -- | Can provide estimate for large areas, can provide estimate areas where measurements or models are not available (e.g., low income countries), relatively standardized method across regions, medium need for updated data. | Availability depends on satellite presence (i.e., time resolution is limited), crude spatial resolution (10 * 10 km), only available for select pollutants, challenging to assess errors in estimates, cannot consider street canyon effects, disregards exposure variability due to mobility/individual activity. |
| Land-use regression models | + | -- | + | Assume independence between sampled locations, good agreement between measured and predicted averages of NO2, less with PM, modelling based on measurements and information around measurement points, relatively easy to collate input data, practical, low costs, medium need for updated data. | Only reflect the predictors used in the model, subject to varying uncertainties amongst different pollutants, the true contribution of traffic to the regression is not always known or reported, difficult to take into account street canyon effects; meteorology and atmospheric chemistry, the quality of the data representing “meaningful” predictors may be an issue and will affect the overall accuracy of the model, the model’s outputs are sensitive to the locations and density of the sampling sites, generally disregards exposure variability due to mobility/individual activity. |
| Air dispersion models | ++ | ++ | ++ | Continuous exposure metric, traffic-specific i.e., based on traffic flows and flow mix, traffic emissions, meteorology and atmospheric chemistry, covers relatively large areas, can assess episodic short-term and long-term exposures, can consider street canyon effects through optional built-in street canyon model, considers compounded effects of proximity to multiple roads, medium need for updated data. | Severe data demands, resource intensive, at the mercy of the emission factors inputted in the model (subject to high uncertainty), meteorology at the exposure scale is influenced by complex physical features including traffic turbulence which is difficult to consider, overestimates pollution levels during periods of calm wind, generally disregards exposure variability due to mobility/individual activity. |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khreis, H.; Nieuwenhuijsen, M.J. Traffic-Related Air Pollution and Childhood Asthma: Recent Advances and Remaining Gaps in the Exposure Assessment Methods. Int. J. Environ. Res. Public Health 2017, 14, 312. https://doi.org/10.3390/ijerph14030312
Khreis H, Nieuwenhuijsen MJ. Traffic-Related Air Pollution and Childhood Asthma: Recent Advances and Remaining Gaps in the Exposure Assessment Methods. International Journal of Environmental Research and Public Health. 2017; 14(3):312. https://doi.org/10.3390/ijerph14030312
Chicago/Turabian StyleKhreis, Haneen, and Mark J. Nieuwenhuijsen. 2017. "Traffic-Related Air Pollution and Childhood Asthma: Recent Advances and Remaining Gaps in the Exposure Assessment Methods" International Journal of Environmental Research and Public Health 14, no. 3: 312. https://doi.org/10.3390/ijerph14030312