Stroke Mortality Attributable to Ambient Particulate Matter Pollution from 1990 to 2015 in China: An Age-Period-Cohort and Spatial Autocorrelation Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Methods
3. Results
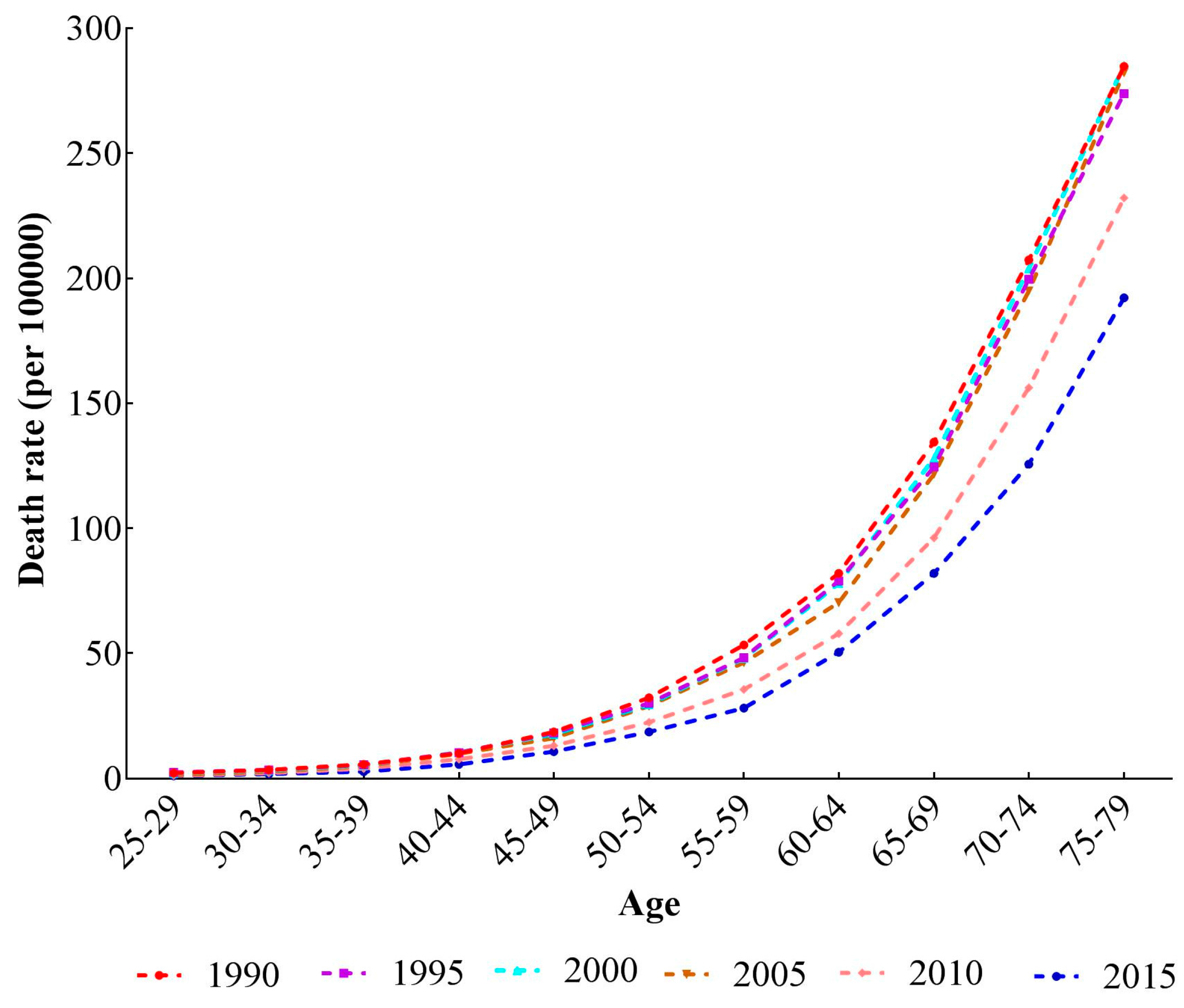
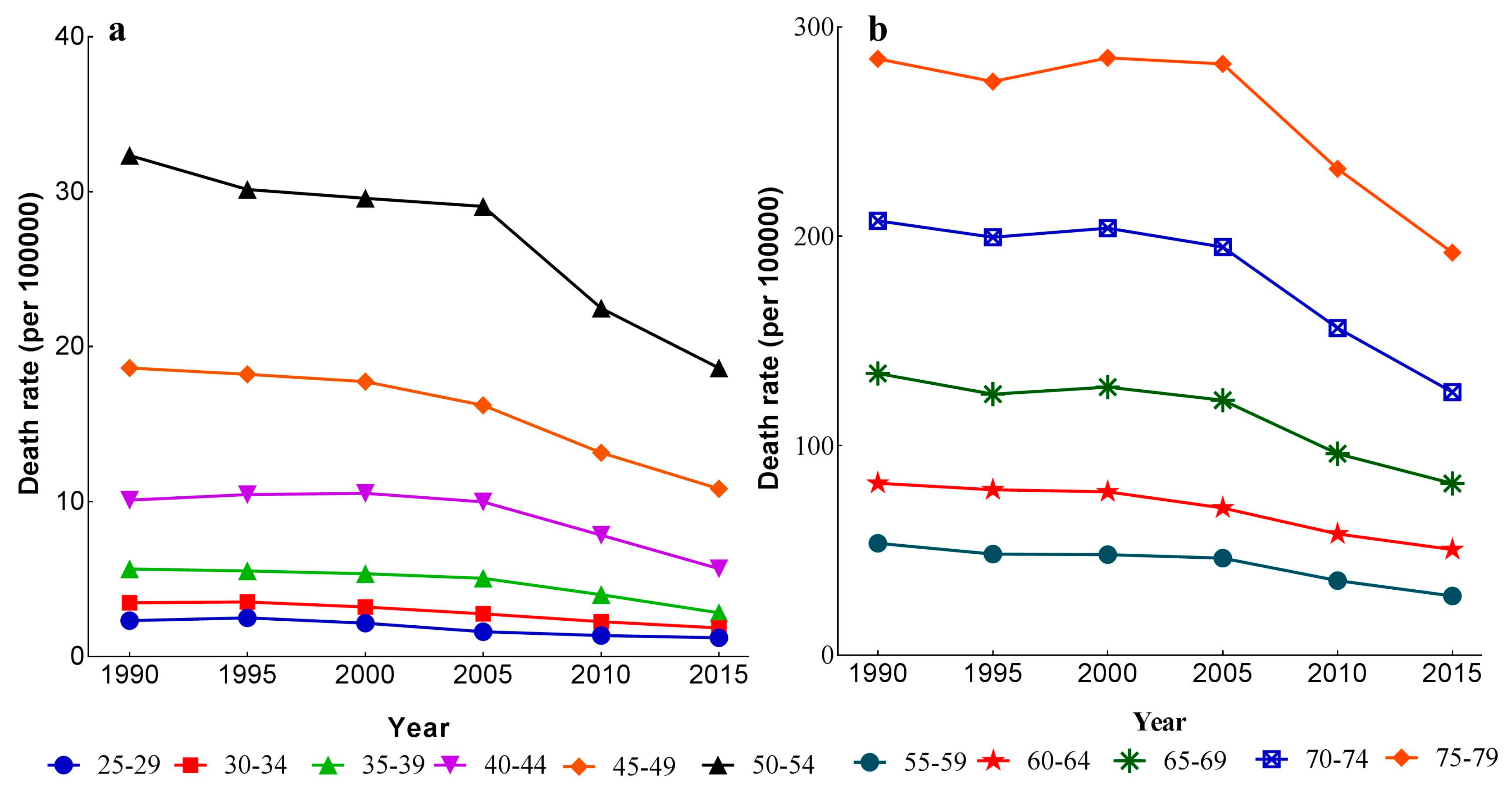
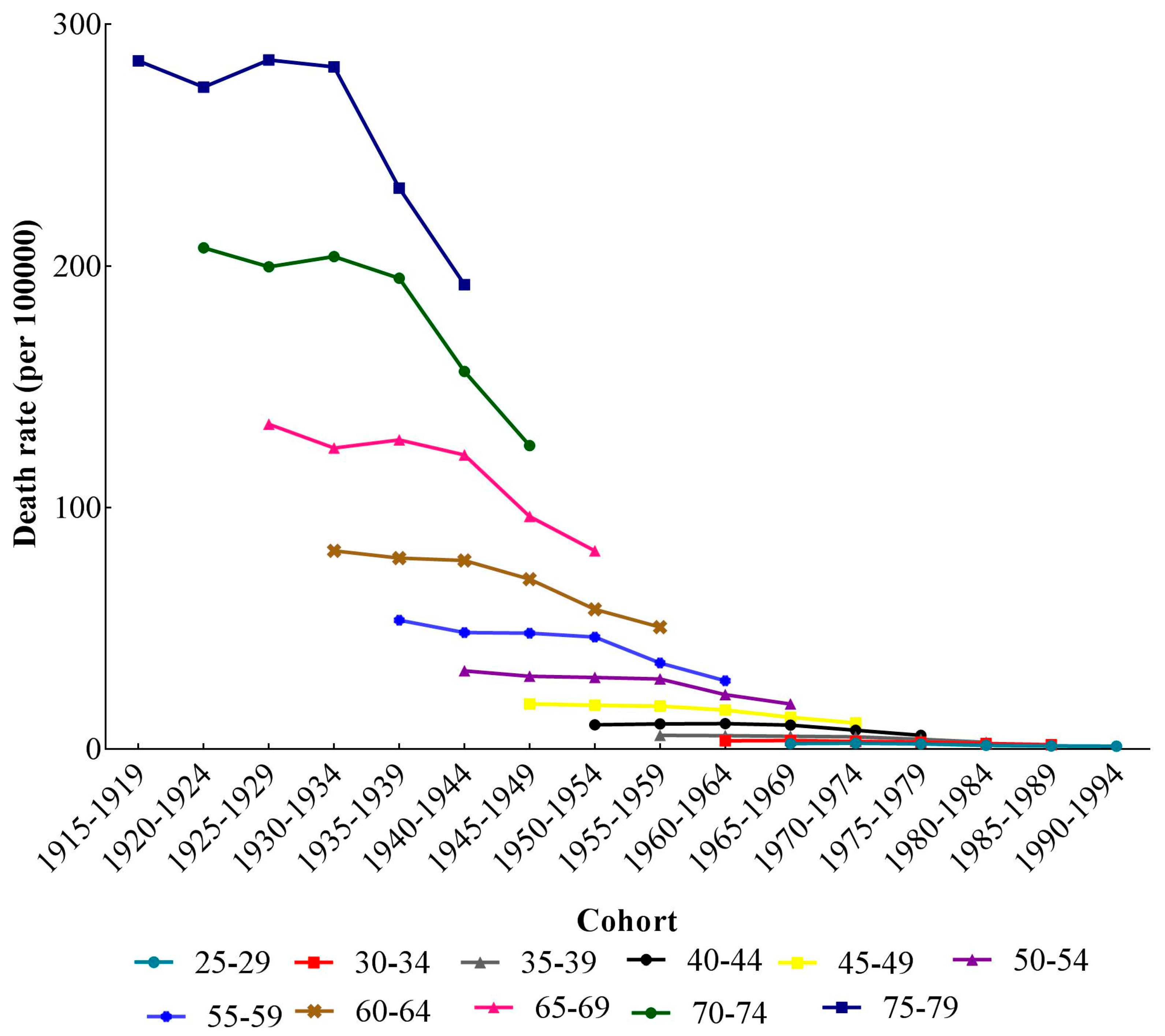
3.1. The Variation of Age, Period, and Cohort on Stroke Mortality-PM2.5
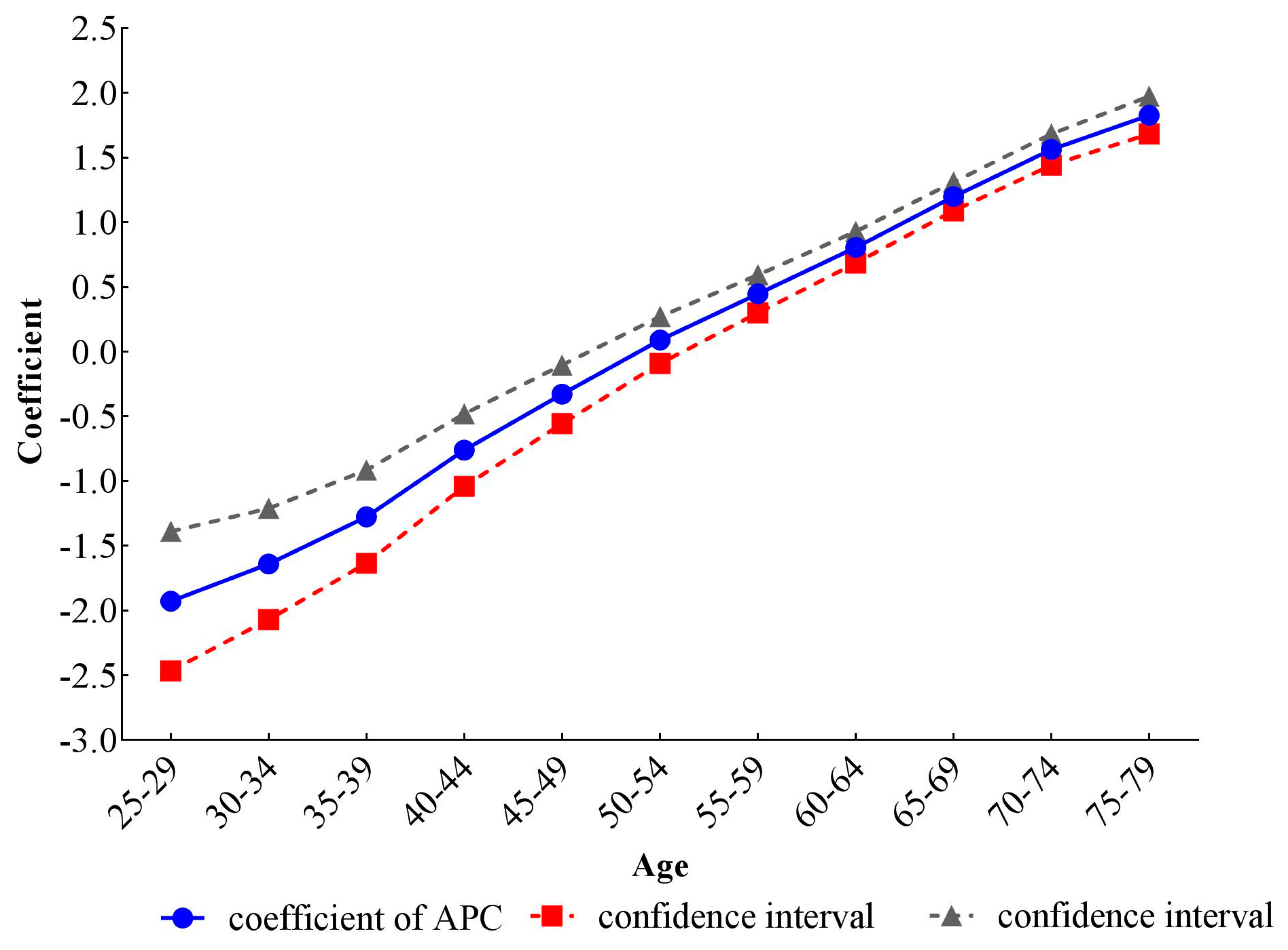
3.2. The Results of Stroke Mortality-PM2.5 from the IE Method of APC Model Analysis
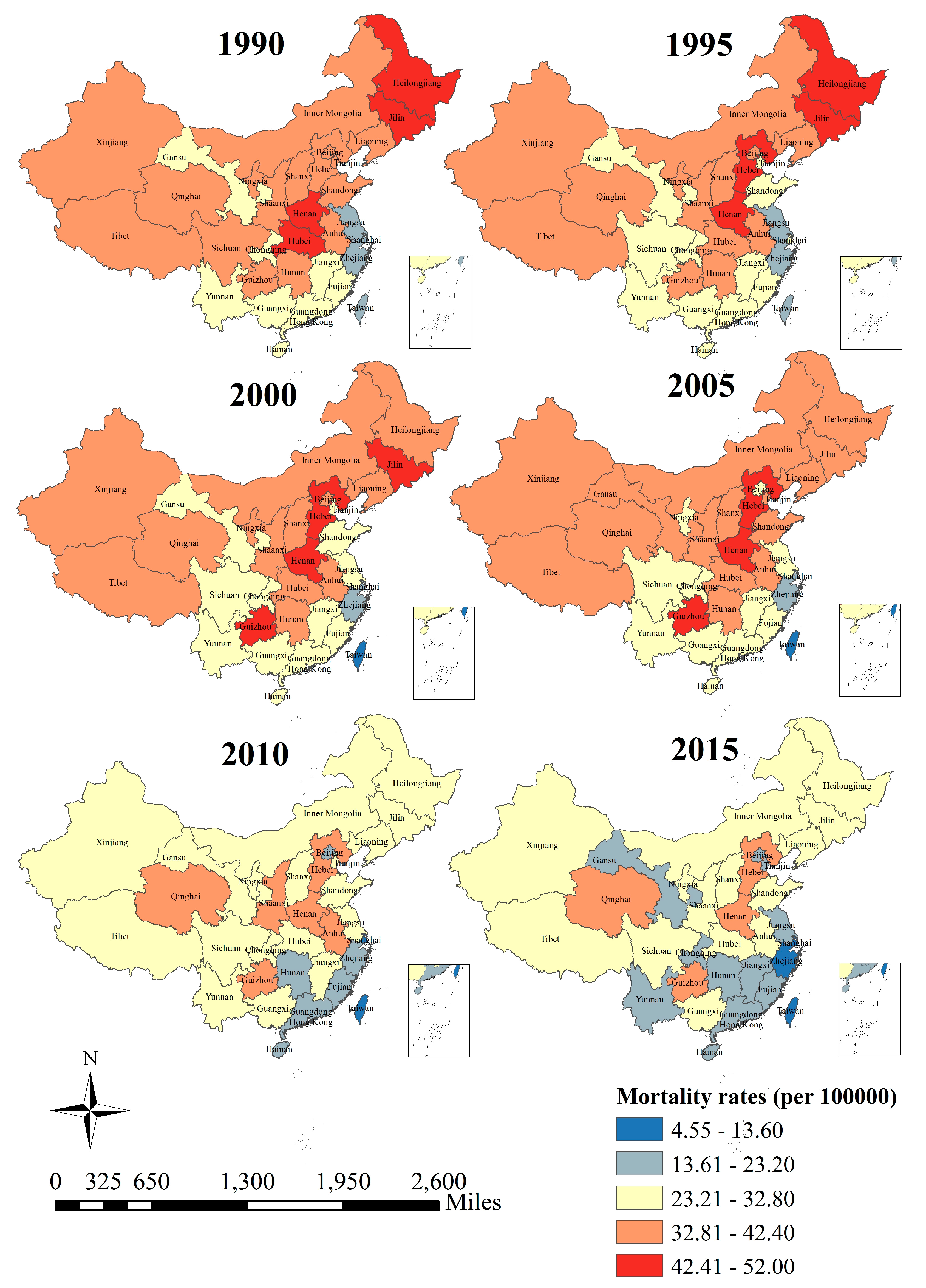
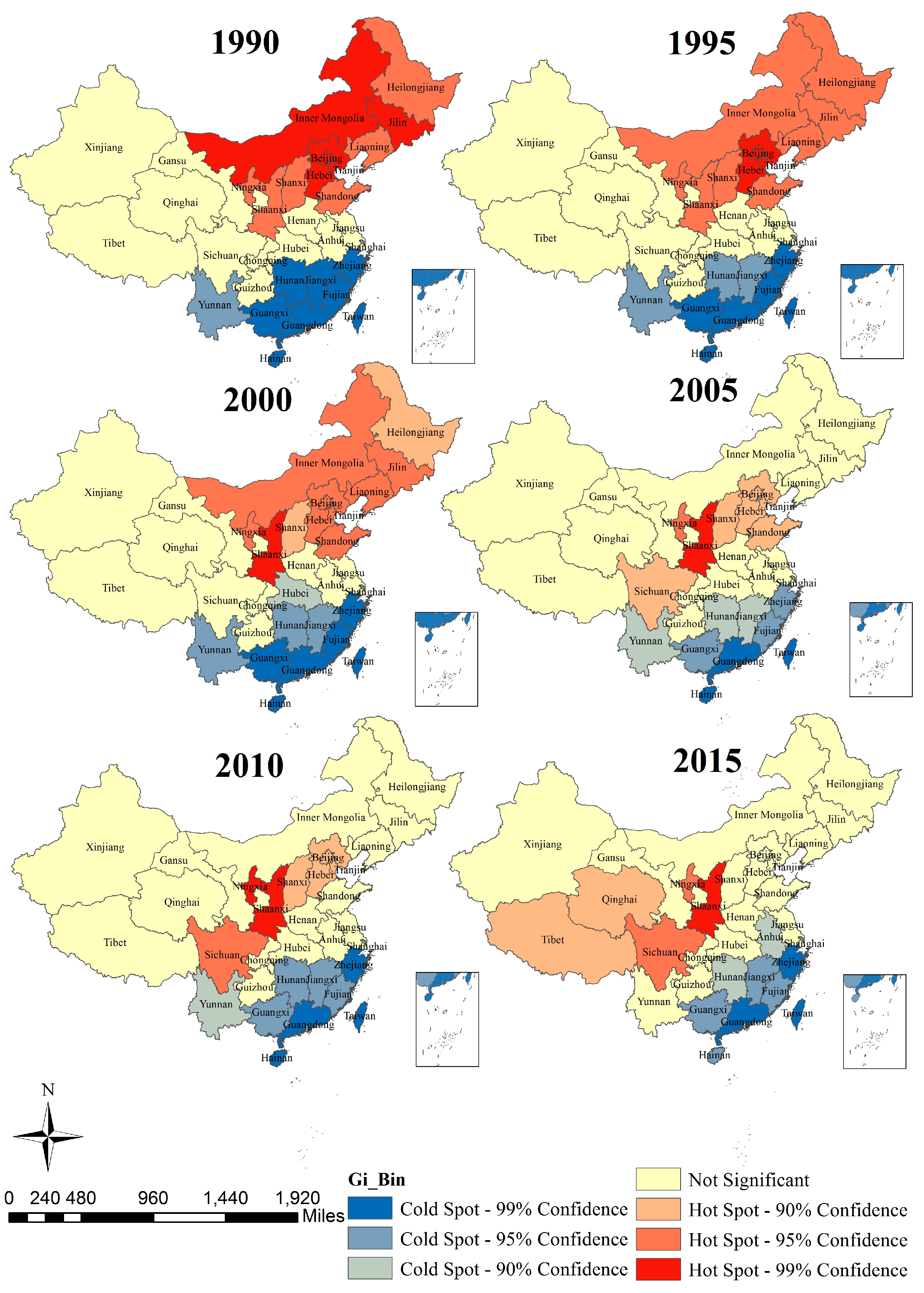
3.3. The Results of Spatial Autocorrelation
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mendis, S.; Davis, S.; Norrving, B. Organizational update: The World Health Organization Global Status Report on Noncommunicable Diseases 2014; one more landmark step in the combat against stroke and vascular disease. Stroke 2015, 46, e121–e122. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, J.; Carter, A.; Casey, D.C.; Charlson, F.J.; Coates, M.M.; Coggeshall, M.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1603–1658. [Google Scholar] [CrossRef]
- Global Burden of Diseases Study 2015. In Global Burden of Diseases Study 2015 (GBD 2015) by Location, Cause, and Risk Factors; Institute for Health Metrics and Evaluation (IHME): Seattle, WA, USA, 2017.
- Feigin, V.L.; Roth, G.A.; Naghavi, M.; Parmar, P.; Krishnamurthi, R.; Chugh, S.; Mensah, G.A.; Norrving, B.; Shiue, I.; Ng, M.; et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol. 2016, 15, 913–924. [Google Scholar] [CrossRef]
- Zhou, M.; Wang, H.; Zhu, J.; Chen, W.; Wang, L.; Liu, S.; Li, Y.; Wang, L.; Liu, Y.; Yin, P.; et al. Cause-specific mortality for 240 causes in China during 1990–2013: A systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet 2016, 387, 251–272. [Google Scholar] [CrossRef]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Brauer, M.; Freedman, G.; Frostad, J.; van Donkelaar, A.; Martin, R.V.; Dentener, F.; van Dingenen, R.; Estep, K.; Amini, H.; Apte, J.S.; et al. Ambient Air Pollution Exposure Estimation for the Global Burden of Disease 2013. Environ. Sci. Technol. 2016, 50, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.S.; Allen, K.; Bhutta, Z.A.; Dandona, L.; Forouzanfar, M.H.; Fullman, N.; Gething, P.W.; Goldberg, E.M.; Hay, S.I.; Holmberg, M.; et al. Measuring the health-related Sustainable Development Goals in 188 countries: A baseline analysis from the Global Burden of Disease Study 2015. Lancet 2016, 388, 1813–1850. [Google Scholar] [CrossRef]
- Song, C.; He, J.; Wu, L. Health burden attributable to ambient PM2.5 in China. Environ. Pollut. 2017, 223, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Luo, Y.; Guo, Y. Particulate Matter and Hospital Admissions for Stroke in Beijing, China: Modification Effects by Ambient Temperature. J. Am. Heart Assoc. 2016, 5, e003437. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Huang, Y.; Ma, Z.; Jin, Z.; Liu, X.; Wang, H.; Liu, Y.; Wang, J.; Jantunen, M.; Bi, J.; et al. Spatial and temporal trends in the mortality burden of air pollution in China: 2004–2012. Environ. Int. 2017, 98, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Han, Y.; Tang, X.; Zhu, J.; Zhu, T. Estimating adult mortality attributable to PM2.5 exposure in China with assimilated PM2.5 concentrations based on a ground monitoring network. Sci. Total Environ. 2016, 568, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Krishnamurthi, R.V.; Parmar, P.; Norrving, B.; Mensah, G.A.; Bennett, D.A.; Barker-Collo, S.; Moran, A.E.; Sacco, R.L.; Truelsen, T.; et al. Update on the Global Burden of Ischemic and Hemorrhagic Stroke in 1990–2013: The GBD 2013 Study. Neuroepidemiology 2015, 45, 161–176. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Johnson, C.O.; Nguyen, G.; Naghavi, M.; Feigin, V.L.; Murray, C.J.; Forouzanfar, M.H.; Vos, T. Methods for Estimating the Global Burden of Cerebrovascular Diseases. Neuroepidemiology 2015, 45, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Wang, P.; Xu, C.; Yu, C. Age-period-cohort analysis on the cancer mortality in rural China: 1990–2010. Int. J. Equity Health 2014, 13, 1. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Bai, Z.; Wang, Z.; Yu, C. Comparison of Secular Trends in Cervical Cancer Mortality in China and the United States: An Age-Period-Cohort Analysis. Int. J. Environ. Res. Public Health 2016, 13, 1148. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.; Gandini, S.; Boyle, P. Age-period-cohort models: A comparative study of available methodologies. J. Clin. Epidemiol. 1999, 52, 569–583. [Google Scholar] [CrossRef]
- Chen, X.; Wang, P. Dynamic changes of social transformation and national health in China. Chin. J. Popul. Sci. 2014, 2, 63–73. [Google Scholar]
- Yang, Y.; Fu, W.; Land, K.C. A methodological comparison of age-period-cohort models: The intrinsic estimator and conventional generalized linear models. Sociol. Methodol. 2004, 34, 75–110. [Google Scholar] [CrossRef]
- Li, C.; Yu, C.; Wang, P. An age-period-cohort analysis of female breast cancer mortality from 1990–2009 in China. Int. J. Equity Health 2015, 14, 76. [Google Scholar] [CrossRef] [PubMed]
- Naves, L.A.; Porto, L.B.; Rosa, J.W.; Casulari, L.A.; Rosa, J.W.C. Geographical information system (GIS) as a new tool to evaluate epidemiology based on spatial analysis and clinical outcomes in acromegaly. Pituitary 2015, 18, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Ying, Y.; Wu, Q.; Zhang, H.; Ma, D.; Xiao, W. A GIS-based spatial correlation analysis for ambient air pollution and AECOPD hospitalizations in Jinan, China. Respir. Med. 2015, 109, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Bao, J.; Yang, X.; Zhao, Z.; Bao, J.; Yang, X.; Zhao, Z.; Wang, Z.; Yu, C.; Li, X. The Spatial-Temporal Characteristics of Air Pollution in China from 2001–2014. Int. J. Environ. Res. Public Health 2015, 12, 15875–15887. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Hu, S.; Sang, S.; Luo, L.; Yu, C. Age-Period-Cohort Analysis of Stroke Mortality in China: Data From the Global Burden of Disease Study 2013. Stroke 2017, 48, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Qian, Y.; Zhu, M.; Cai, B. Epidemiological evidence on association between ambient air pollution and stroke mortality. J. Epidemiol. Community Health 2013, 67, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Hansen, S.; Baptiste, K.E.; Fjeldborg, J.; Horohov, D.W. A review of the equine age-related changes in the immune system: Comparisons between human and equine aging, with focus on lung-specific immune-aging. Ageing Res. Rev. 2015, 20, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.J.; Lawrence, C.B.; Rodriguez-Grande, B.; Kovacs, K.J.; Pradillo, J.M.; Denes, A. The immune system in stroke: Clinical challenges and their translation to experimental research. J. Neuroimmune Pharmacol. 2013, 8, 867–887. [Google Scholar] [CrossRef] [PubMed]
- Kanasi, E.; Ayilavarapu, S.; Jones, J. The aging population: Demographics and the biology of aging. Periodontoloy 2016, 72, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Lutz, W.; Sanderson, W.; Scherbov, S. The coming acceleration of global population ageing. Nature 2008, 451, 716–719. [Google Scholar] [CrossRef] [PubMed]
- The Lancet. The best science for achieving Healthy China 2030. Lancet 2016, 388, 1851. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, J.; Bao, J.; Gao, X.; Yu, C.; Xiang, H. Temporal Trends of Suicide Mortality in Mainland China: Results from the Age-Period-Cohort Framework. Int. J. Environ. Res. Public Health 2016, 13, 15409–15418. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Song, J.; Lin, T.; Dixon, J.; Zhang, G.; Ye, H. Urbanization and health in China, thinking at the national, local and individual levels. Environ. Health 2016, 15 (Suppl. 1), S32. [Google Scholar] [CrossRef] [PubMed]
- Zeng, W.; Zhen, J.; Feng, M.; Campbell, S.M.; Finlayson, A.E.; Godman, B. Analysis of the influence of recent reforms in China: Cardiovascular and cerebrovascular medicines as a case history to provide future direction. J. Comp. Eff. Res. 2014, 3, 371–386. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Andersson, H.; Zhang, S. Air Pollution Control Policies in China: A Retrospective and Prospects. Int. J. Environ. Res. Public Health 2016, 13, 1219. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Rao, K.; Wu, S.; Liu, Q. Health care in China: Improvement, challenges, and reform. Chest J. 2013, 143, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Hou, Y.; Sun, M.; Lu, J.; Wang, Y.; Li, X.; Chang, F.; Hao, M. An evaluation of China’s new rural cooperative medical system: Achievements and inadequacies from policy goals. BMC Public Health 2015, 15, 1079. [Google Scholar] [CrossRef] [PubMed]
- Hankey, G.J. Nutrition and the risk of stroke. Lancet Neurol. 2012, 11, 66–81. [Google Scholar] [CrossRef]
- Cohen, A.K.; Syme, S.L. Education: A Missed Opportunity for Public Health Intervention. Am. J. Public Health 2013, 103, 997–1001. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y. Social Inequalities in Happiness in the United States, 1972 to 2004: An Age-Period-Cohort Analysis. Am. Sociol. Rev. 2008, 73, 204–226. [Google Scholar] [CrossRef]
- Guo, F. The Study on the Early Health Enterprise in Nanjing National Government. Master’s Thesis, Guangxi Normal University, Guilin, China, 2010. [Google Scholar]
- HO, P. Development of hygiene and health work during the first five-year plan. Chin. Med. J. 1957, 75, 953–957. [Google Scholar] [PubMed]
- Zhang, Y.; Zhang, L.; Ma, Z.; Gao, Q. Age change and phase difference of the influence of natural disaster in China in the 20th century on social economy. J. Catastrophol. 2008, 23, 55–58. [Google Scholar]
- Chen, T. An Empirical Study on China’s Reform and Opening-up Policy Effectiveness. Stat. Res. 2011, 28, 54–59. [Google Scholar]
- Lin, G.; Fu, J.; Jiang, D.; Hu, W.; Dong, D.; Huang, Y.; Zhao, M. Spatio-temporal variation of PM2.5 concentrations and their relationship with geographic and socioeconomic factors in China. Int. J. Environ. Res. Public Health 2013, 11, 173–186. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Lopez, A.D.; Murray, C.J.; Lozano, R. A comparison of maternal mortality estimates from GBD 2013 and WHO. Lancet 2014, 384, 2209–2210. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Coef | 95% CI | S.E. | RR | 95% CI |
|---|---|---|---|---|---|
| Intercept | 3.13 | (2.98, 3.28) | 0.08 | ||
| Age | |||||
| 25–29 | −1.93 *** | (−2.47, −1.39) | 0.27 | 1.00 | |
| 30–34 | −1.64 *** | (−2.07, −1.21) | 0.22 | 1.33 | (1.20, 1.49) |
| 35–39 | −1.28 *** | (−1.64, −0.92) | 0.18 | 1.92 | (1.60, 2.29) |
| 40–44 | −0.76 *** | (−1.04, −0.48) | 0.14 | 3.22 | (2.48, 4.18) |
| 45–49 | −0.33 *** | (−0.56, −0.10) | 0.12 | 4.96 | (3.63, 6.75) |
| 50–54 | 0.09 | (−0.09, 0.27) | 0.09 | 7.54 | (5.26, 10.80) |
| 55–59 | 0.45 *** | (0.30, 0.59) | 0.07 | 10.75 | (7.24, 15.96) |
| 60–64 | 0.81 *** | (0.69, 0.93) | 0.06 | 15.43 | (10.18, 23.57) |
| 65–69 | 1.20 *** | (1.09, 1.31) | 0.06 | 22.87 | (14.88, 35.16) |
| 70–74 | 1.56 *** | (1.44, 1.68) | 0.06 | 32.87 | (21.54, 49.90) |
| 75–79 | 1.83 *** | (1.68, 1.97) | 0.07 | 42.85 | (28.79, 63.43) |
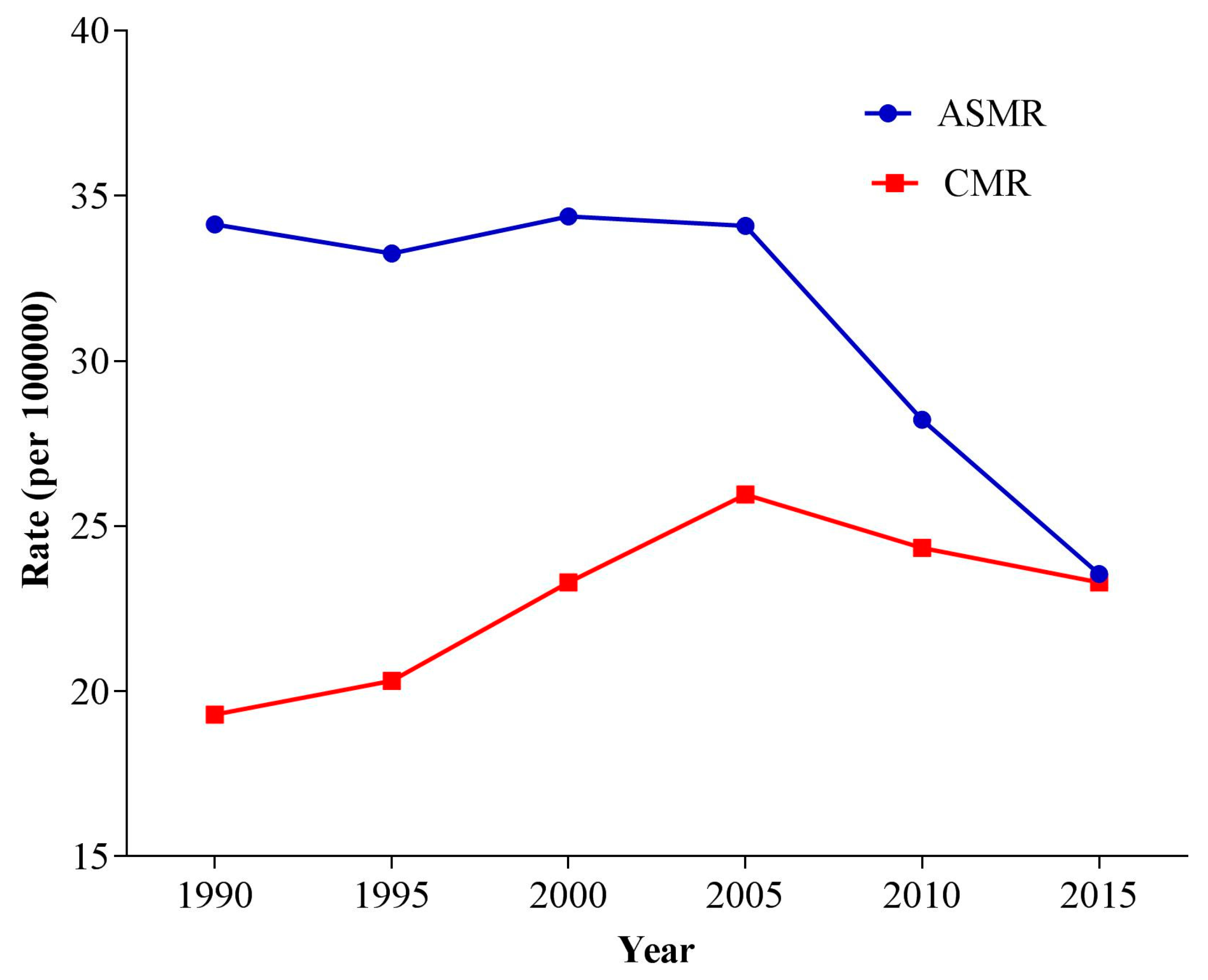
| Period | |||||
| 1990 | −0.08 | (−0.20, 0.05) | 0.06 | 1.00 | |
| 1995 | −0.05 | (−0.14, 0.04) | 0.05 | 1.03 | (0.99, 1.06) |
| 2000 | 0.06 | (−0.01, 0.13) | 0.04 | 1.15 | (1.08, 1.21) |
| 2005 | 0.12 ** | (0.04, 0.19) | 0.04 | 1.22 | (1.15, 1.27) |
| 2010 | 0.01 | (−0.08, 0.11) | 0.05 | 1.10 | (1.06, 1.13) |
| 2015 | −0.06 | (−0.18, 0.06) | 0.06 | 1.02 | (1.01, 1.02) |
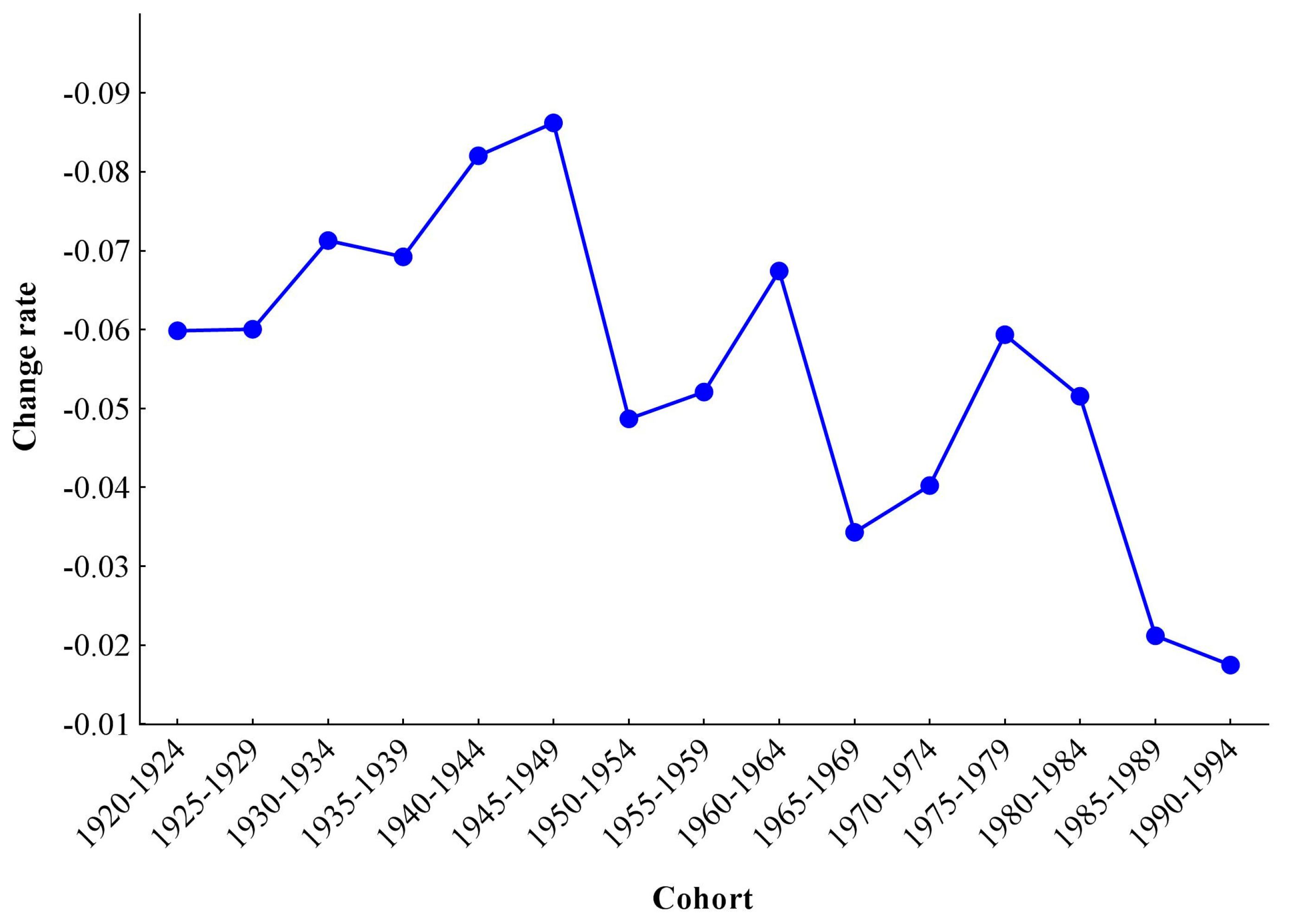
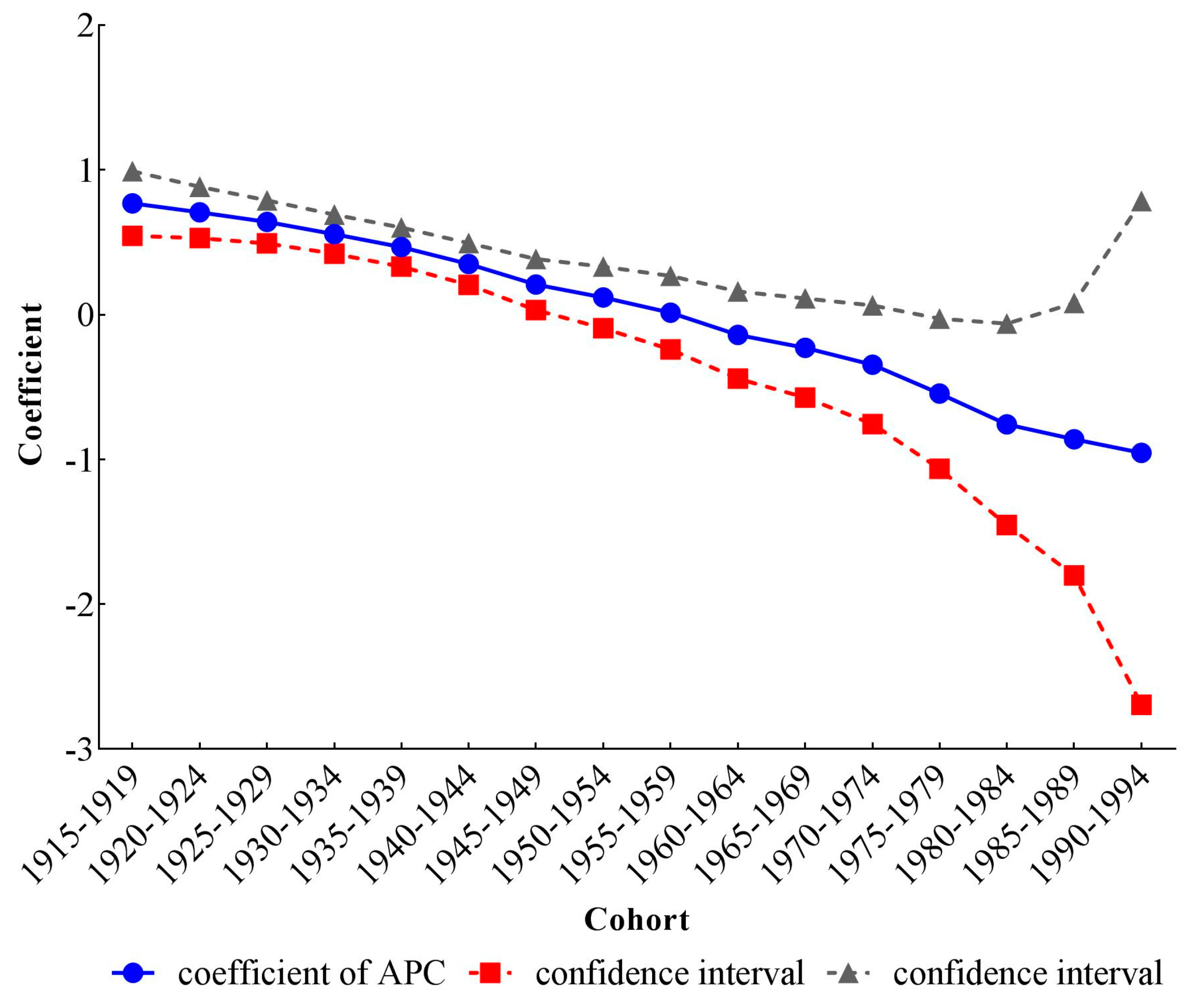
| Cohort | |||||
| 1915–1919 | 0.77 *** | (0.55, 0.99) | 0.11 | 1.00 | |
| 1920–1924 | 0.71 *** | (0.53, 0.88) | 0.09 | 0.94 | (0.90, 0.98) |
| 1925–1929 | 0.64 *** | (0.49, 0.79) | 0.08 | 0.88 | (0.82, 0.94) |
| 1930–1934 | 0.56 *** | (0.42, 0.69) | 0.07 | 0.81 | (0.74, 0.88) |
| 1935–1939 | 0.47 *** | (0.33, 0.6) | 0.07 | 0.74 | (0.68, 0.80) |
| 1940–1944 | 0.35 *** | (0.21, 0.49) | 0.07 | 0.66 | (0.61, 0.71) |
| 1945–1949 | 0.21 | (0.03, 0.38) | 0.09 | 0.57 | (0.54, 0.59) |
| 1950–1954 | 0.12 | (−0.09, 0.33) | 0.11 | 0.52 | (0.52, 0.53) |
| 1955–1959 | 0.01 | (−0.24, 0.27) | 0.13 | 0.47 | (0.45, 0.49) |
| 1960–1964 | −0.14 | (−0.44, 0.16) | 0.15 | 0.40 | (0.37, 0.44) |
| 1965–1969 | −0.23 | (−0.57, 0.11) | 0.17 | 0.37 | (0.33, 0.41) |
| 1970–1974 | −0.35 | (−0.76, 0.07) | 0.21 | 0.33 | (0.27, 0.40) |
| 1975–1979 | −0.54 * | (−1.06, −0.03) | 0.26 | 0.27 | (0.20, 0.36) |
| 1980–1984 | −0.76 * | (−1.45, −0.06) | 0.36 | 0.22 | (0.14, 0.35) |
| 1985–1989 | −0.86 | (−1.80, 0.08) | 0.48 | 0.20 | (0.10, 0.40) |
| 1990–1994 | −0.95 | (−2.70, 0.79) | 0.89 | 0.18 | (0.04, 0.82) |
| Deviance | 0.81 | ||||
| AIC | 5.94 | ||||
| BIC | −150.02 | ||||
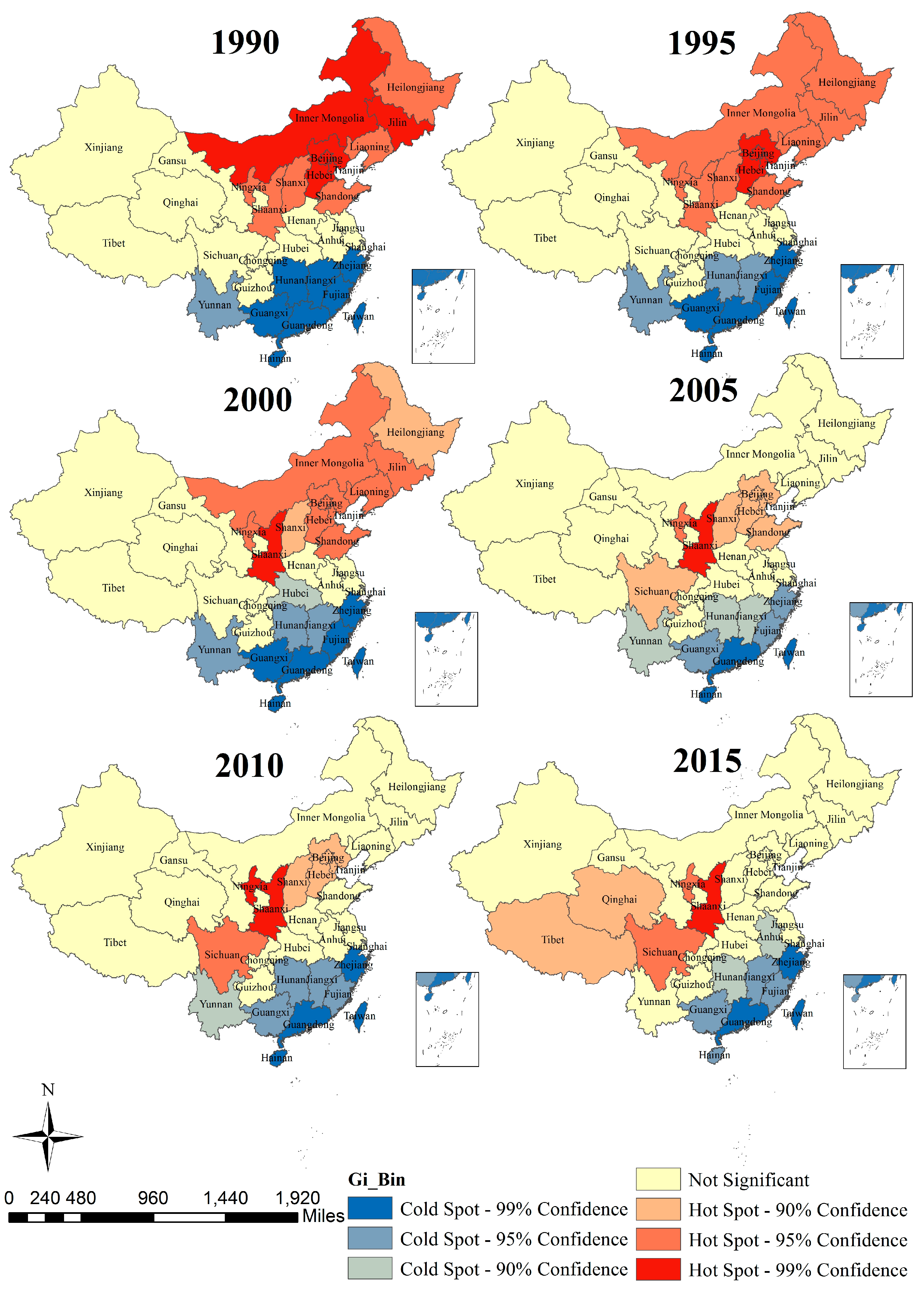
| Year | Moran’s I | Z Score | p |
|---|---|---|---|
| 1990 | 0.55 | 7.36 | <0.001 |
| 1995 | 0.53 | 7.15 | <0.001 |
| 2000 | 0.54 | 7.34 | <0.001 |
| 2005 | 0.44 | 6.12 | <0.001 |
| 2010 | 0.44 | 6.09 | <0.001 |
| 2015 | 0.39 | 5.35 | <0.001 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, L.; Jiang, J.; Zhang, G.; Wang, L.; Wang, Z.; Yang, J.; Yu, C. Stroke Mortality Attributable to Ambient Particulate Matter Pollution from 1990 to 2015 in China: An Age-Period-Cohort and Spatial Autocorrelation Analysis. Int. J. Environ. Res. Public Health 2017, 14, 772. https://doi.org/10.3390/ijerph14070772
Luo L, Jiang J, Zhang G, Wang L, Wang Z, Yang J, Yu C. Stroke Mortality Attributable to Ambient Particulate Matter Pollution from 1990 to 2015 in China: An Age-Period-Cohort and Spatial Autocorrelation Analysis. International Journal of Environmental Research and Public Health. 2017; 14(7):772. https://doi.org/10.3390/ijerph14070772
Chicago/Turabian StyleLuo, Lisha, Junfeng Jiang, Ganshen Zhang, Lu Wang, Zhenkun Wang, Jin Yang, and Chuanhua Yu. 2017. "Stroke Mortality Attributable to Ambient Particulate Matter Pollution from 1990 to 2015 in China: An Age-Period-Cohort and Spatial Autocorrelation Analysis" International Journal of Environmental Research and Public Health 14, no. 7: 772. https://doi.org/10.3390/ijerph14070772