Sharply Reduced but Still Heavy Self-Harm Burdens in Hubei Province, China, 1990–2015


Abstract
:1. Introduction
2. Materials and Methods
3. Results
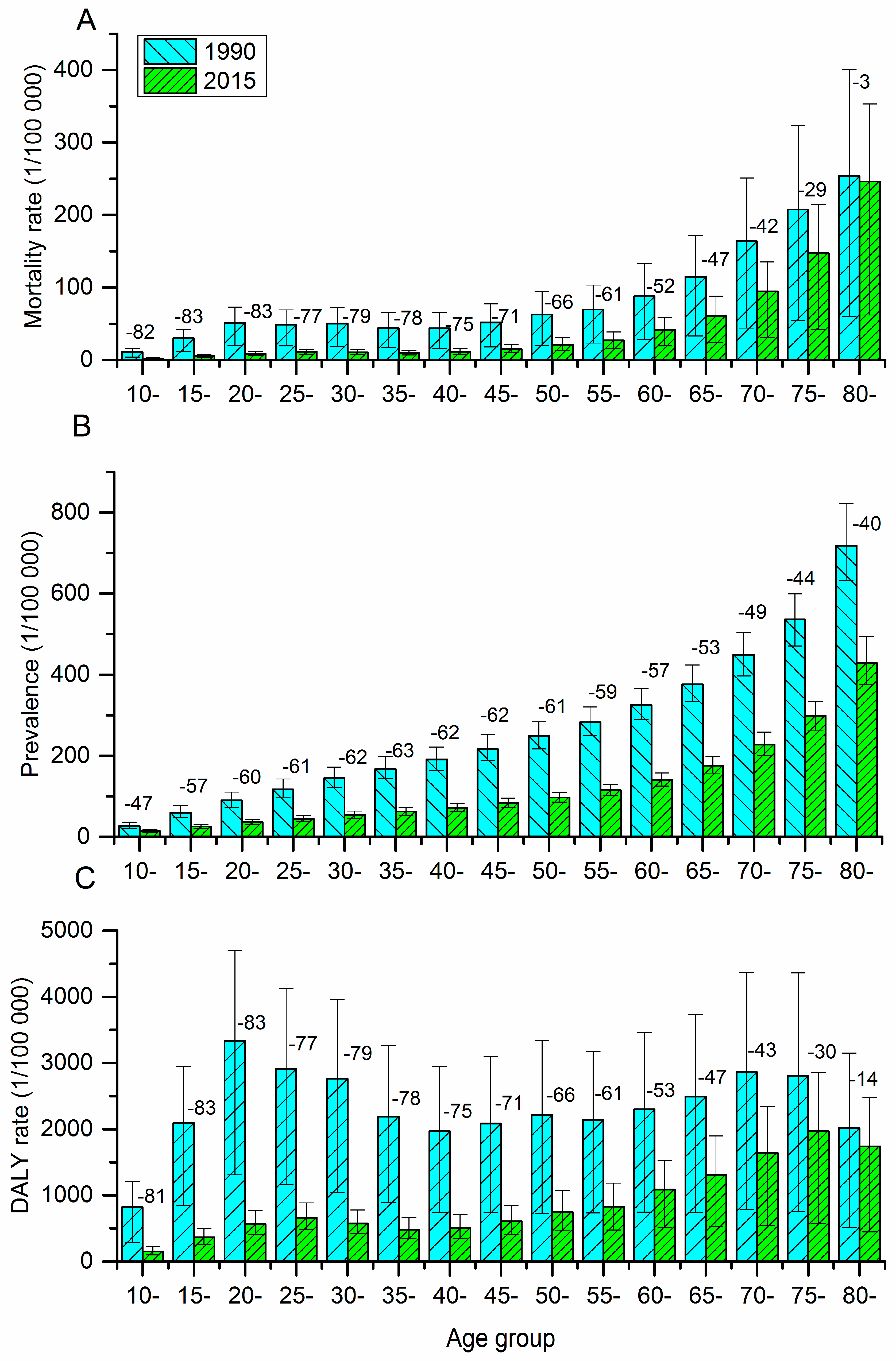
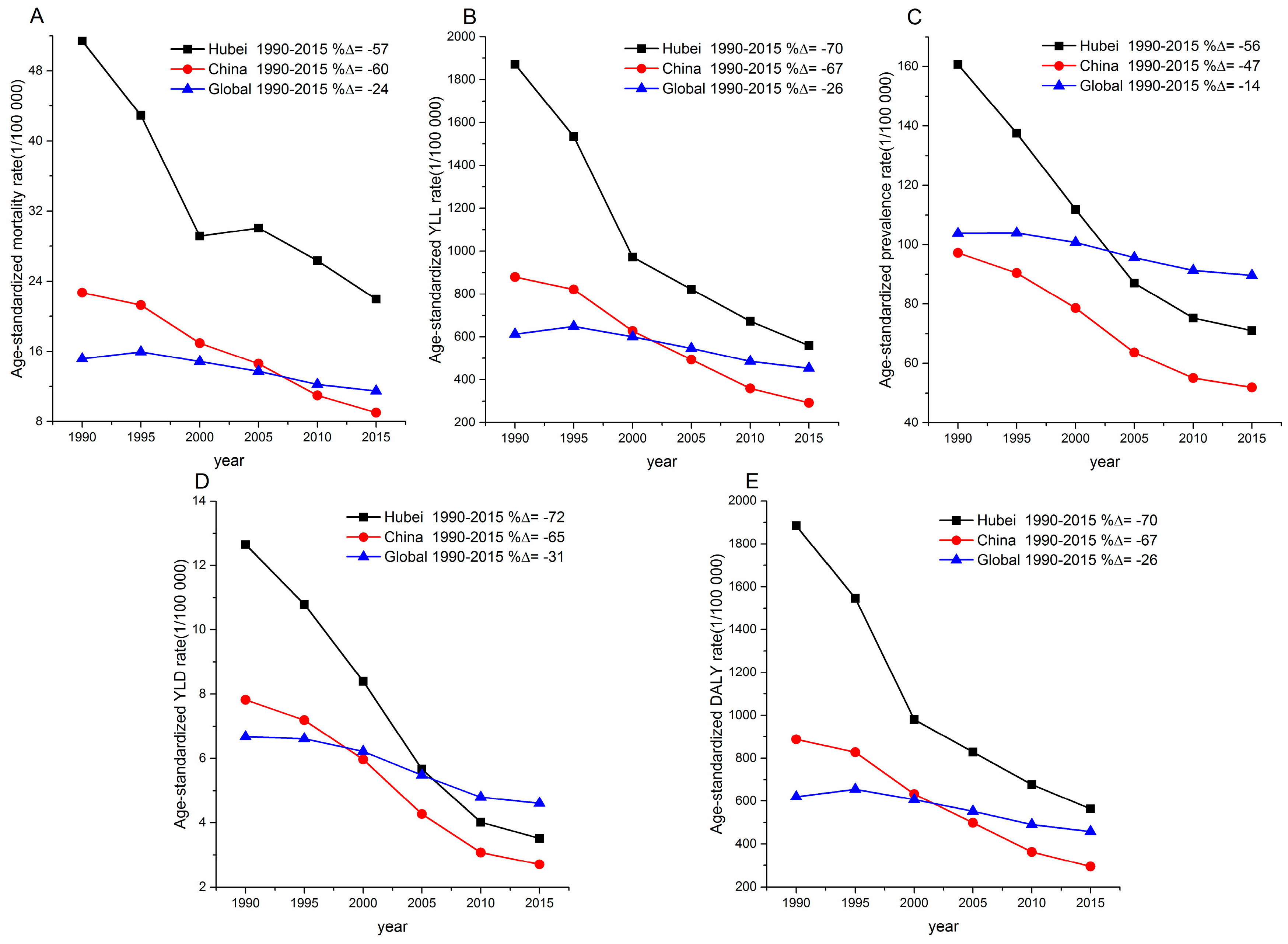
3.1. Fatal Outcomes Attributable to Self-Harm
3.2. Non-Fatal Outcomes Attributable to Self-Harm
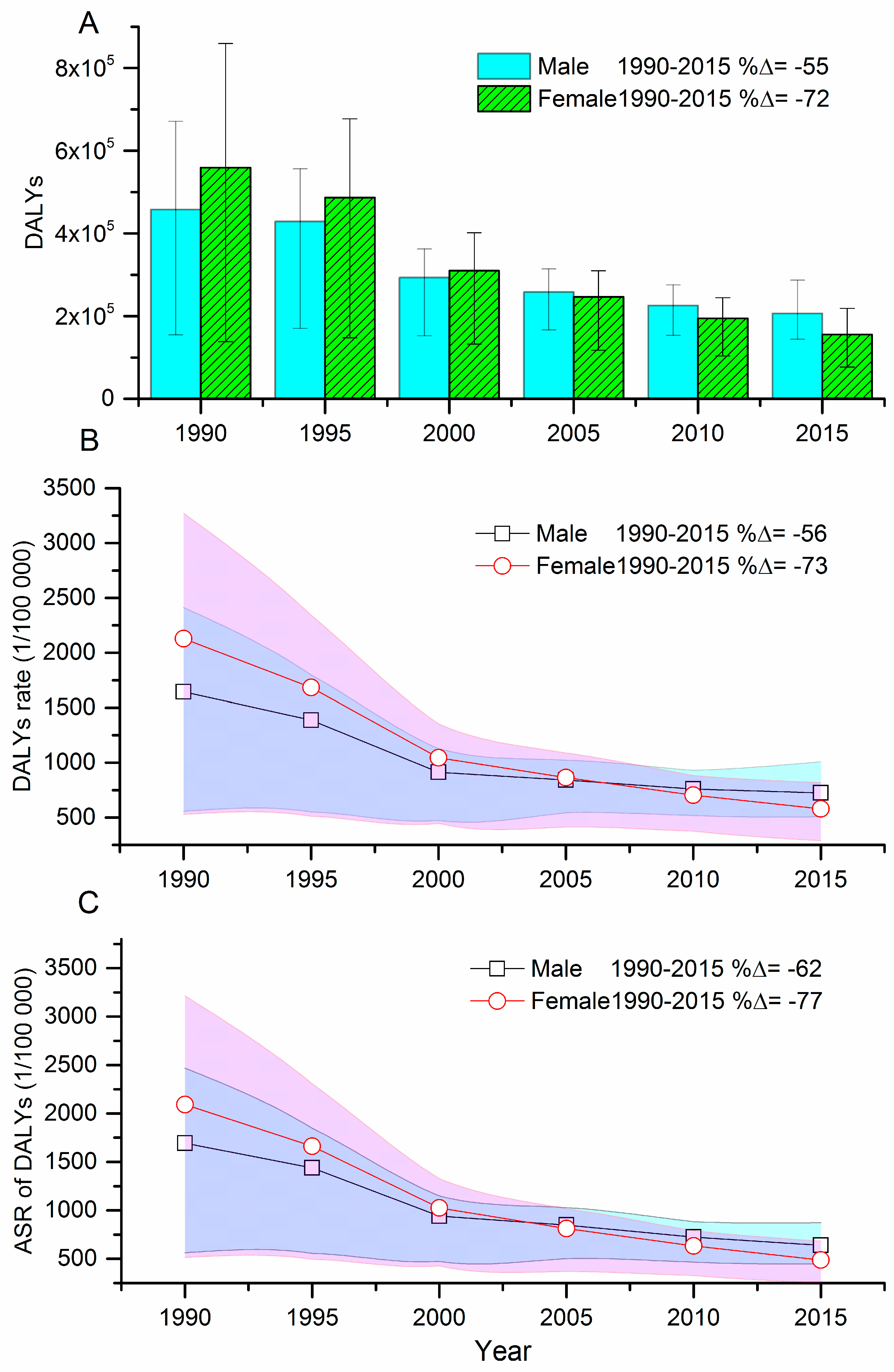
3.3. DALYs Attributable to Self-Harm
3.4. Risk Factors Attributable to Self-Harm
3.5. Variation in Suicide Methods
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hawton, K.; Harriss, L.; Hall, S.; Simkin, S.; Bale, E.; Bond, A. Deliberate self-harm in Oxford, 1990–2000: A time of change in patient characteristics. Psychol. Med. 2003, 33, 987–995. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Mental Health (UK). Self-Harm: Longer-Term Management; The British Psychological Society and The Royal College of Psychiatrists: Leicester, UK, 2012. [Google Scholar]
- Haagsma, J.A.; Graetz, N.; Bolliger, I.; Naghavi, M.; Higashi, H.; Mullany, E.C.; Abera, S.F.; Abraham, J.P.; Adofo, K.; Alsharif, U.; et al. The global burden of injury: Incidence, mortality, disability-adjusted life years and time trends from the Global Burden of Disease study 2013. Inj. Prev. 2016, 22, 3–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Burden of Disease Study 2015 (GBD 2015). Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar]
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar]
- Global Burden of Disease Study 2015 (GBD 2015). Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar]
- Liu, S.; Page, A.; Yin, P.; Astell-Burt, T.; Feng, X.; Liu, Y.; Liu, J.; Wang, L.; Zhou, M. Spatiotemporal variation and social determinants of suicide in China, 2006–2012: Findings from a nationally representative mortality surveillance system. Psychol. Med. 2015, 45, 3259–3268. [Google Scholar] [CrossRef] [PubMed]
- Statistical Bulletin of National Economy and Social Development of Hubei Province in 2015. Available online: http://www.stats-hbgovcn/tjgb/ndtjgb/hbs/112361htm (accessed on 26 February 2016).
- Hubei Yearbook 2015. Available online: http://www.hubei.gov.cn/2015change/2015sq/sa/gk/201609/t20160930_902878shtml (accessed on 30 September 2016).
- Zhou, M.; Wang, H.; Zhu, J.; Chen, W.; Wang, L.; Liu, S.; Li, Y.; Liu, Y.; Yin, P.; Liu, J.; et al. Cause-Specific mortality for 240 causes in China during 1990–2013: A systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet 2016, 387, 251–272. [Google Scholar] [CrossRef]
- Liu, Q.; Zhang, L.; Li, J.; Zuo, D.; Kong, D.; Shen, X.; Guo, Y.; Zhang, Q. The gap in injury mortality rates between urban and rural residents of Hubei Province, China. BMC Public Health 2012, 12, 180. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Yi, G.; Zhang, Q.; Qian, Z.; Xuan, G.; Li, W. A Survey on suicides among Hubei province population. Med. J. Wuhan Univ. 2013, 34, 923–925. [Google Scholar]
- Global Burden of Disease Study 2015 (GBD 2015). Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1603–1658. [Google Scholar]
- Collaborators GBDRF. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar]
- Liu, S.; Wu, X.; Lopez, A.D.; Wang, L.; Cai, Y.; Page, A.; Yin, P.; Liu, Y.; Li, Y.; Liu, J.; et al. An integrated national mortality surveillance system for death registration and mortality surveillance, China. Bull. World Health Organ. 2016, 94, 46–57. [Google Scholar] [CrossRef] [PubMed]
- National Vital Statistics Reports. Available online: https://www.cdc.gov/nchs/data/nvsr/nvsr66/nvsr66_06_tables.pdf (accessed on 27 November 2017).
- Qi, X.; Hu, W.; Page, A.; Tong, S. Dynamic pattern of suicide in Australia, 1986–2005: A descriptive-analytic study. BMJ Open 2014, 4, e005311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Preventing Suicide: A Global Imperative; World Health Organization: Luxembourg, 2014. [Google Scholar]
- Lin, H. Family integration and young rural women’s suicide based on the research of ming village of Hubei province. China Agric. Univ. J. Soc. Sci. Ed. 2013, 2, 015. [Google Scholar]
- Yang, H.; Fan, F.-X. The normalization of suicide and the issue of elderly suicide in Jingshan rural areas. Open Times 2009, 5, 104–125. [Google Scholar]
- Chen, B. Change of inter-generational relations and the elderly suicide: An empirical study in Jingshan county, Hubei province. Sociol. Stud. 2009, 4, 007. [Google Scholar]
- Zhou, L.-J.; Liu, X.-X.; Gao, J. Epidemiological study on suicide among rural women in Macheng city, 2000–2002. Clin. J. Dis. Control Prev. 2004, 8, 231–233. [Google Scholar]
- Wang, C.W.; Chan, C.L.; Yip, P.S. Suicide rates in China from 2002 to 2011: An update. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 929–941. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, J.; Bao, J.; Gao, X.; Yu, C.; Xiang, H. Temporal trends of suicide mortality in Mainland China: Results from the age-period-cohort framework. Int. J. Environ. Res. Public Health 2016, 13, 784. [Google Scholar] [CrossRef] [PubMed]
- Jing, J.; Wu, X.; Zhang, J. Research on the migration of rural women and the decline of Chinese suicide rate. China Agric. Univ. J. Social Sci. Ed. 2010, 27, 004. [Google Scholar]
- Sha, F.; Yip, P.S.; Law, Y.W. Decomposing change in China’s suicide rate, 1990–2010: Ageing and urbanisation. Inj. Prev. 2017, 23, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Phillips, M.; Huang, Z.; Zhang, Y.; Zhao, Y.; Yang, G. Evaluation on the accuracy of reported suicides in the Chinese population. Chin. J. Epidemiol. 2003, 24, 889–892. [Google Scholar]
- Hubei Provincial Center for Disease Control and Prevention. Report on Chronic Disease Risk Factor Surveillance in Hubei (2013); Hubei Science and Technology Press: Wuhan, China, 2013. [Google Scholar]
- Li, Y.; Jiang, Y.; Zhang, M.; Yin, P.; Wu, F.; Zhao, W. Drinking behaviour among men and women in China: The 2007 China Chronic Disease and Risk Factor Surveillance. Addiction 2011, 106, 1946–1956. [Google Scholar] [CrossRef] [PubMed]
- Ness, J.; Hawton, K.; Bergen, H.; Cooper, J.; Steeg, S.; Kapur, N.; Clarke, M.; Waters, K. Alcohol use and misuse, self-harm and subsequent mortality: An epidemiological and longitudinal study from the multicentre study of self-harm in England. Emerg. Med. J. 2015, 32, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Stewart, D.E.; Vigod, S.; Riazantseva, E. New developments in intimate partner violence and management of its mental health sequelae. Curr. Psychiatry Rep. 2016, 18, 4. [Google Scholar] [CrossRef] [PubMed]
- Kong, Y.; Zhang, J. Access to farming pesticides and risk for suicide in Chinese rural young people. Psychiatry Res. 2010, 179, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Fulu, E.; Jewkes, R.; Roselli, T.; Garcia-Moreno, C. Men UNM-cC-sSo, violence research: Prevalence of and factors associated with male perpetration of intimate partner violence: Findings from the UN Multi-country cross-sectional study on men and violence in Asia and the Pacific. Lancet Glob. Health 2013, 1, e187–e207. [Google Scholar] [CrossRef]
- Ellsberg, M.; Jansen, H.A.; Heise, L.; Watts, C.H.; Garcia-Moreno, C. Health WHOM-cSoWs, domestic violence against women study t: Intimate partner violence and women’s physical and mental health in the WHO multi-country study on women’s health and domestic violence: An observational study. Lancet 2008, 371, 1165–1172. [Google Scholar] [CrossRef]
- Pearson, V.; Phillips, M.R.; He, F.; Ji, H. Attempted suicide among young rural women in the People’s Republic of China: Possibilities for prevention. Suicide Life Threat. Behav. 2002, 32, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.P.; Wang, C.; Meng, M.; Phillips, M.R. Understanding self-harm in victims of intimate partner violence: A qualitative analysis of calls made by victims to a crisis hotline in China. Violence Women 2011, 17, 532–544. [Google Scholar]
- Stewart, D.E.; Vigod, S.N. Mental health aspects of intimate partner violence. Psychiatr. Clin. N. Am. 2017, 40, 321–334. [Google Scholar] [CrossRef] [PubMed]
- Page, A.; Liu, S.; Gunnell, D.; Astell-Burt, T.; Feng, X.; Wang, L.; Zhou, M. Suicide by pesticide poisoning remains a priority for suicide prevention in China: Analysis of national mortality trends 2006–2013. J. Affect. Disord. 2017, 208, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Mew, E.J.; Padmanathan, P.; Konradsen, F.; Eddleston, M.; Chang, S.S.; Phillips, M.R.; Gunnell, D. The global burden of fatal self-poisoning with pesticides 2006–2015: Systematic review. J. Affect. Disord. 2017, 219, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Kolves, K.; McDonough, M.; Crompton, D.; de Leo, D. Choice of a suicide method: Trends and characteristics. Psychiatry Res. 2017, 260, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Chia, B.H.; Chia, A.; Ng, W.Y.; Tai, B.C. Suicide methods in Singapore (2000–2004): Types and associations. Suicide Life Threat. Behav. 2011, 41, 574–583. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Statistics 2016: Monitoring Health for the SDGs, Sustainable Development Goals 2016.
- Van der Feltz-Cornelis, C.; Sarchiapone, M.; Postuvan, V.; Volker, D.; Roskar, S.; Grum, A.; Carli, V.; McDaid, D.; O’Connor, R.; Maxwell, M.; et al. Best practice elements of multilevel suicide prevention strategies: A review of systematic reviews. Crisis 2011, 32, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Chang, E.S.; Zeng, P.; Simon, M.A. Suicide in the global Chinese aging population: A review of risk and protective factors, consequences, and interventions. Aging Dis. 2015, 6, 121–130. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Gender/Year | All Age Deaths | Mortality Rate (1/100,000) | YLLs | YLLs Rate (1/100,000) |
|---|---|---|---|---|
| Total | ||||
| 1990 | 22,685 (8080–30,951) | 41.9 (14.9–57.2) | 1,010,770 (380,864–1,392,060) | 1869.0 (704.2–2574.0) |
| 1995 | 20,961 (7780–26,422) | 35.0 (13.0–44.2) | 909,755 (358,468–1,144,165) | 1520.9 (599.3–1912.8) |
| 2000 | 14,803 (7144–17,672) | 24.0 (11.6–28.6) | 598,279 (309,844–712,316) | 969.8 (502.2–1154.6) |
| 2005 | 15,167 (7512–17,947) | 25.6 (12.7–30.3) | 501,187 (301,344–589,108) | 847.2 (509.4–995.8) |
| 2010 | 14,244 (7367–17,073) | 24.9 (12.9–29.8) | 417,424 (274,119–493,941) | 728.5 (478.4–862.0) |
| 2015 | 13,173 (6786–16,749) | 23.9 (12.3–30.3) | 359,034 (236,934–454,291) | 650.5 (429.3–823.1) |
| Percent change between 1990 and 2015 | −41.9% | −43.1% | −64.5% | −65.2% |
| Males | ||||
| 1990 | 10,364 (3357–15,127) | 37.3 (12.1–54.4) | 454,880 (152,382–668,153) | 1635.5 (547.9–2402.2) |
| 1995 | 9910 (3752–12,795) | 32.0 (12.1–41.4) | 426,374 (166,614–553,241) | 1378.8 (538.8–1789.1) |
| 2000 | 7201 (3524–8836) | 22.5 (11.0–27.6) | 290,706 (149,907–359,895) | 906.9 (467.6–1122.7) |
| 2005 | 7715 (4136–9436) | 25.2 (13.5–30.8) | 256,382 (164,900–311,778) | 836.1 (537.8–1016.7) |
| 2010 | 7597 (4096–9384) | 25.7 (13.8–31.7) | 223,879 (151,957–274,098) | 756.0 (513.1–925.5) |
| 2015 | 7470 (4237–10,112) | 26.3 (14.9–35.6) | 204,758 (142,795–285,078) | 720.3 (502.3–1002.9) |
| Percent change between 1990 and 2015 | −27.9% | −29.5% | −54.5% | −56.0% |
| Females | ||||
| 1990 | 12,322 (2901–19,042) | 46.9 (11.0–72.5) | 555,890 (135,168–855,785) | 2116.2 (514.6–3257.9) |
| 1995 | 11,051 (3115–15,213) | 38.2 (10.8–52.7) | 483,381 (144,602–674,562) | 1673.1 (500.5–2334.8) |
| 2000 | 7603 (2918–9909) | 25.7 (9.8–33.4) | 307,573 (130,235–399,707) | 1037.8 (439.4–1348.6) |
| 2005 | 7452 (2820–9507) | 26.2 (9.9–33.4) | 244,805 (116,072–308,111) | 859.1 (407.3–1081.2) |
| 2010 | 6647 (2654–8540) | 24.0 (9.6–30.9) | 193,546 (102,402–243,165) | 699.1 (369.9–878.4) |
| 2015 | 5703 (2173–8163) | 21.3 (8.1–30.5) | 154,277 (76,143–217,569) | 576.4 (284.5–812.8) |
| Percent change between 1990 and 2015 | −53.7% | −54.6% | −72.2% | −72.8% |
| Gender/Year | Number of Patients | Prevalence Rate (1/100,000) | YLDs | YLDs Rate (1/100,000) |
|---|---|---|---|---|
| Total | ||||
| 1990 | 68,368 (60,673–78,307) | 126.4 (112.2–144.8) | 5772 (4102–7784) | 10.7 (7.6–14.4) |
| 1995 | 66,279 (59,058–75,242) | 110.8 (98.7–125.8) | 5552 (3916–7460) | 9.3 (6.5–12.5) |
| 2000 | 58,856 (52,534–66,327) | 95.4 (85.2–107.5) | 4702 (3309–6350) | 7.6 (5.4–10.3) |
| 2005 | 49,236 (44,305–54,982) | 83.2 (74.9–92.9) | 3367 (2372–4535) | 5.7 (4.0–7.7) |
| 2010 | 45,314 (41,082–50,304) | 79.1 (71.7–87.8) | 2479 (1718–3370) | 4.3 (3.0–5.9) |
| 2015 | 45,408 (41,079–50,364) | 82.3 (74.4–91.3) | 2237 (1525–3066) | 4.1 (2.8–5.6) |
| Percent change between 1990 and 2015 | −33.6% | −34.9% | −61.2% | −62.0% |
| Males | ||||
| 1990 | 34,329 (30,688–38,641) | 123.4 (110.3–138.9) | 2580 (1818–3449) | 9.3 (6.5–12.4) |
| 1995 | 34,109 (30,594–38,172) | 110.3 (98.9–123.4) | 2552 (1795–3427) | 8.3 (5.8–11.1) |
| 2000 | 31,200 (28,160–34,698) | 97.3 (87.8–108.2) | 2238 (1587–3021) | 7.0 (4.9–9.4) |
| 2005 | 26,553 (24,123–29,419) | 86.6 (78.7–95.9) | 1622 (1138–2170) | 5.3 (3.7–7.1) |
| 2010 | 24,882 (22,711–27,352) | 84.0 (76.7–92.4) | 1212 (839–1647) | 4.1 (2.8–5.6) |
| 2015 | 25,436 (23,083–28,004) | 89.5 (81.2–98.5) | 1121 (773–1522) | 3.9 (2.7–5.4) |
| Percent change between 1990 and 2015 | −25.9% | −27.5% | −56.6% | −57.5% |
| Females | ||||
| 1990 | 34,039 (29,714–39,714) | 129.6 (113.1–151.2) | 3191 (2235–4367) | 12.1 (8.5–16.6) |
| 1995 | 32,170 (28,315–37,157) | 111.3 (98.0–128.6) | 3000 (2110–4050) | 10.4 (7.3–14.0) |
| 2000 | 27,656 (24,465–31,684) | 93.3 (82.5–106.9) | 2464 (1710–3373) | 8.3 (5.8–11.4) |
| 2005 | 22,683 (20,230–25,787) | 79.6 (71.0–90.5) | 1745 (1210–2390) | 6.1 (4.2–8.4) |
| 2010 | 20,431 (18,306–23,041) | 73.8 (66.1–83.2) | 1267 (871–1730) | 4.6 (3.1–6.2) |
| 2015 | 19,973 (17,870–22,438) | 74.6 (66.8–83.8) | 1116 (749–1541) | 4.2 (2.8–5.8) |
| Percent change between 1990 and 2015 | −41.3% | −42.4% | −65.0% | −65.7% |
| Risk Factors | Alcohol and Drug Use | Sexual Abuse and Violence | ||
|---|---|---|---|---|
| Alcohol Use, % (95%, UI) | Drug Use, % (95%, UI) | Childhood Sexual Abuse, % (95%, UI) | Intimate Partner Violence, % (95%, UI) | |
| Years | ||||
| 1990 | 7.7 (5.0–12.0) | 2.8 (1.7–4.5) | 9.2 (2.1–19.6) | 9.9 (4.5–14.9) |
| 1995 | 8.7 (6.3–12.9) | 3.1 (1.9–4.9) | 8.8 (2.0–18.7) | 10.8 (5.1–15.5) |
| 2000 | 8.9 (6.7–12.1) | 3.0 (1.9–4.8) | 8.4 (1.9–17.9) | 10.5 (6.2–14.7) |
| 2005 | 9.8 (7.5–13.1) | 2.8 (1.8–4.3) | 8.0 (1.8–17.2) | 10.8 (6.6–14.9) |
| 2010 | 11.3 (9.0–14.5) | 2.9 (1.8–4.6) | 7.5 (1.7–16.1) | 10.9 (7.0–14.6) |
| 2015 | 12.8 (9.8–16.6) | 3.0 (1.9–4.7) | 7.4 (1.6–16.0) | 10.4 (6.3–14.8) |
| Age groups | ||||
| 10- | 0 | 0.1 (0.0–0.2) | 6.3 (1.3–13.7) | 0 |
| 15- | 6.8 (3.8–11.2) | 4.6 (2.2–8.7) | 7.9 (1.7–17.1) | 0.0 (0.0–0.1) |
| 20- | 8.9 (5.5–13.4) | 7.6 (4.1–13.1) | 8.9 (2.0–18.8) | 3.5 (0.6–9.4) |
| 25- | 10.0 (6.2–14.6) | 6.9 (4.0–11.4) | 9.1 (2.1–19.1) | 9.3 (1.8–22.3) |
| 30- | 11.3 (7.7–15.8) | 5.1 (3.2–8.4) | 9.1 (2.0–19.5) | 12.9 (3.2–26.8) |
| 35- | 13.6 (8.9–19.5) | 3.4 (2.2–5.4) | 8.9 (1.9–18.7) | 15.2 (3.5–31.9) |
| 40- | 14.9 (10.0–20.4) | 2.4 (1.5–3.7) | 8.6 (1.8–18.0) | 15.2 (3.6–30.9) |
| 45- | 15.3 (10.2–21.0) | 1.8 (1.1–2.8) | 8.0 (1.7–17.1) | 14.9 (3.6–29.9) |
| 50- | 15.2 (10.3–20.6) | 1.6 (1.0–2.4) | 7.5 (1.6–16.1) | 13.9 (3.5–28.8) |
| 55- | 16.0 (10.7–22.1) | 1.7 (1.1–2.6) | 7.1 (1.5–15.5) | 11.2 (2.6–24.2) |
| 60- | 14.0 (9.4–19.0) | 1.9 (1.3–2.8) | 6.7 (1.4–14.7) | 9.5 (2.0–20.8) |
| 65- | 13.6 (9.4–18.9) | 2.1 (1.3–3.1) | 6.4 (1.4–13.9) | 9.2 (2.0–20.7) |
| 70- | 13.2 (9.1–18.8) | 2.1 (1.3–3.2) | 6.0 (1.3–13.3) | 8.3 (1.9–18.9) |
| 75- | 12.2 (8.2–17.7) | 1.6 (1.0–2.5) | 5.6 (1.2–12.5) | 8.2 (1.5–19.5) |
| 80- | 7.6 (4.3–12.5) | 0.4 (0.2–0.7) | 4.1 (0.9–9.2) | 9.4 (1.6–20.9) |
| Gender | ||||
| Male | 20.9 (17.9–24.7) | 3.7 (2.4–5.8) | 8.8 (1.9–18.4) | 0 |
| Female | 1.9 (1.5–2.3) | 2.0 (1.3–3.1) | 5.7 (1.2–12.6) | 24.4 (17.8–31.2) |
| Both | 12.8 (9.8–16.6) | 3.0 (1.9–4.7) | 7.4 (1.6–16.0) | 10.4 (6.3–14.8) |
| External Causes | Male | Female | Both Sexes | |||
|---|---|---|---|---|---|---|
| Percent (%) | Mortality Rate (1/100,000) | Percent (%) | Mortality Rate (1/100,000) | Percent (%) | Mortality Rate (1/100,000) | |
| Totals | ||||||
| Poisoning | 59.1 | 13.5 | 67.5 | 14.7 | 63.1 | 14.1 |
| Hanging | 27.4 | 6.2 * | 22.9 | 5.0 | 25.2 | 5.6 |
| Drowning | 5.1 | 1.2 | 5.4 | 1.2 | 5.2 | 1.2 |
| Cutting | 1.4 | 0.3 * | 0.4 | 0.1 | 0.9 | 0.2 |
| Jumping | 6.2 | 1.4 * | 3.6 | 0.8 | 4.9 | 1.1 |
| Other methods | 0.9 | 0.2 | 0.3 | 0.1 | 0.6 | 0.1 |
| Totals | 100.0 | 22.8 | 100.0 | 21.8 | 100.0 | 22.3 |
| Urban | ||||||
| Poisoning | 54.9 | 11.3 | 66.1 | 12.7 | 60.2 | 12.0 |
| Hanging | 29.1 | 6.0 * | 24.7 | 4.7 | 27.0 | 5.4 |
| Drowning | 5.4 | 1.1 | 4.3 | 0.8 | 4.8 | 1.0 |
| Cutting | 1.7 | 0.3 * | 0.3 | 0.1 | 1.0 | 0.2 |
| Jumping | 8.5 | 1.7 * | 4.4 | 0.8 | 6.5 | 1.3 |
| Other methods | 0.6 | 0.1 | 0.2 | 0.0 | 0.4 | 0.1 |
| Totals | 100.0 | 20.6 | 100.0 | 19.2 | 100.0 | 19.9 |
| Rural | ||||||
| Poisoning | 63.7 | 16.5 # | 68.9 | 17.5 # | 66.2 | 17.0 # |
| Hanging | 25.5 | 6.6 | 20.9 | 5.3 | 23.3 | 6.0 |
| Drowning | 4.8 | 1.2 | 6.5 | 1.7 # | 5.6 | 1.4 # |
| Cutting | 1.1 | 0.3 | 0.5 | 0.1 | 0.8 | 0.2 |
| Jumping | 3.7 | 1.0 # | 2.7 | 0.7 | 3.2 | 0.8 # |
| Other methods | 1.2 | 0.3 | 0.5 | 0.1 | 0.9 | 0.2 |
| Totals | 100.0 | 25.9 # | 100.0 | 25.4 # | 100.0 | 25.6 # |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, J.; Zhang, L.; Tang, Y.; Li, Q.; Yu, C.; He, T. Sharply Reduced but Still Heavy Self-Harm Burdens in Hubei Province, China, 1990–2015. Int. J. Environ. Res. Public Health 2018, 15, 391. https://doi.org/10.3390/ijerph15020391
Pan J, Zhang L, Tang Y, Li Q, Yu C, He T. Sharply Reduced but Still Heavy Self-Harm Burdens in Hubei Province, China, 1990–2015. International Journal of Environmental Research and Public Health. 2018; 15(2):391. https://doi.org/10.3390/ijerph15020391
Chicago/Turabian StylePan, Jingju, Lan Zhang, Yumeng Tang, Qian Li, Chuanhua Yu, and Tianjing He. 2018. "Sharply Reduced but Still Heavy Self-Harm Burdens in Hubei Province, China, 1990–2015" International Journal of Environmental Research and Public Health 15, no. 2: 391. https://doi.org/10.3390/ijerph15020391