Food Sources of Energy and Macronutrient Intakes among Infants from 6 to 12 Months of Age: The Growing Up in Singapore Towards Healthy Outcomes (GUSTO) Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Maternal and Infant Characteristics
2.3. Infant Dietary Assessment
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Energy and Macronutrient Intakes of Infants by Milk-Feed Type
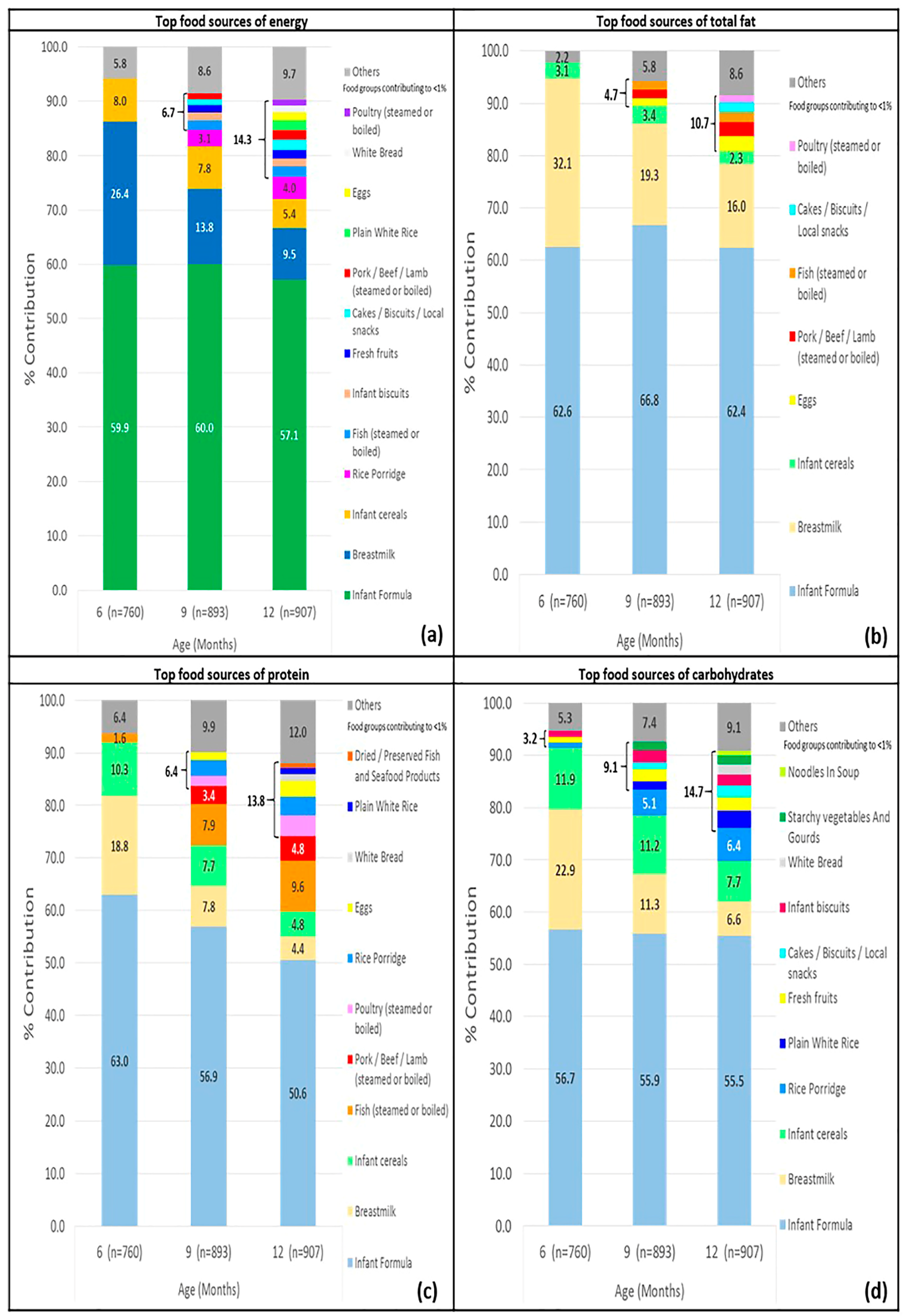
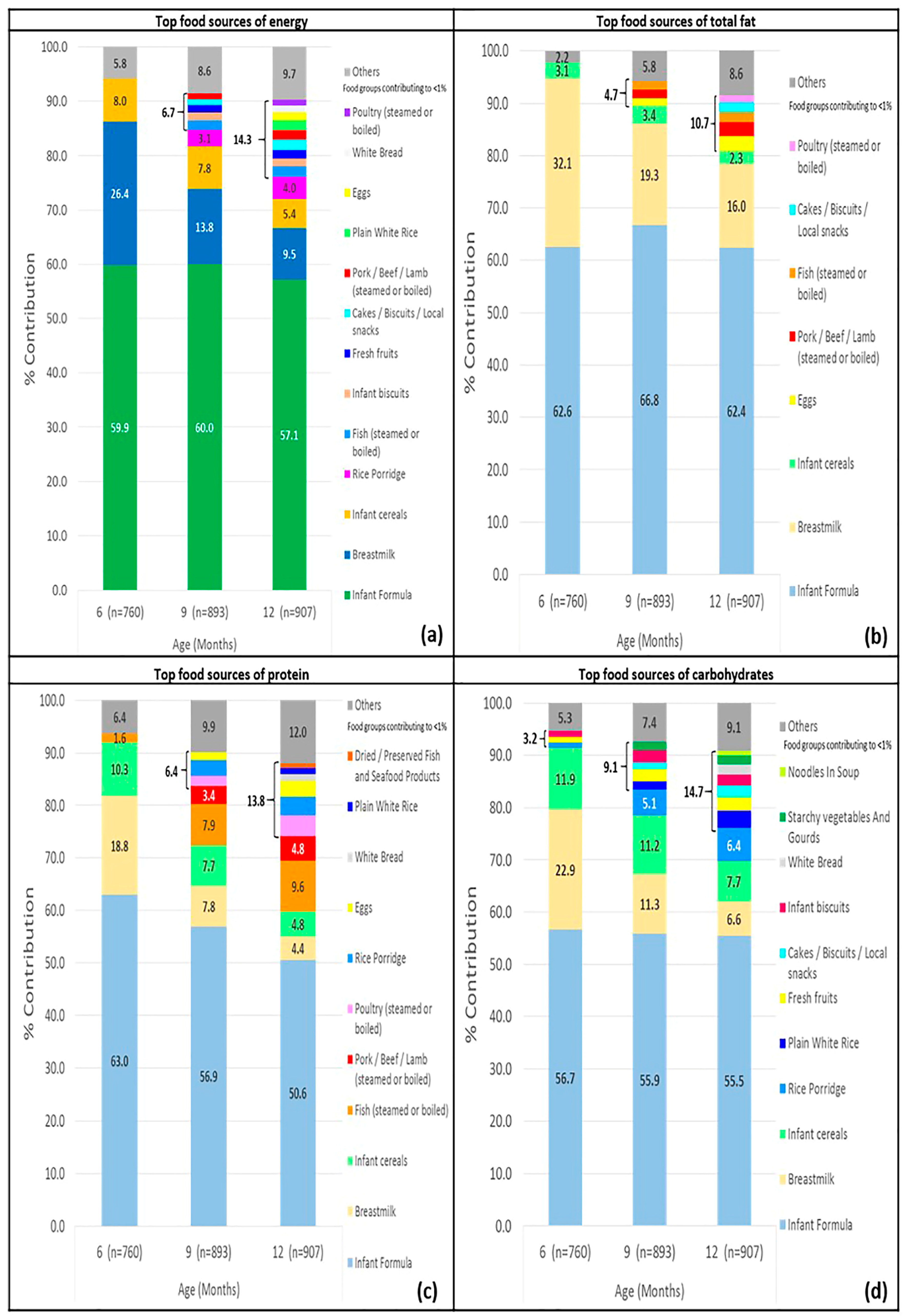
3.3. Main Food Sources of Energy and Macronutrient of Infants
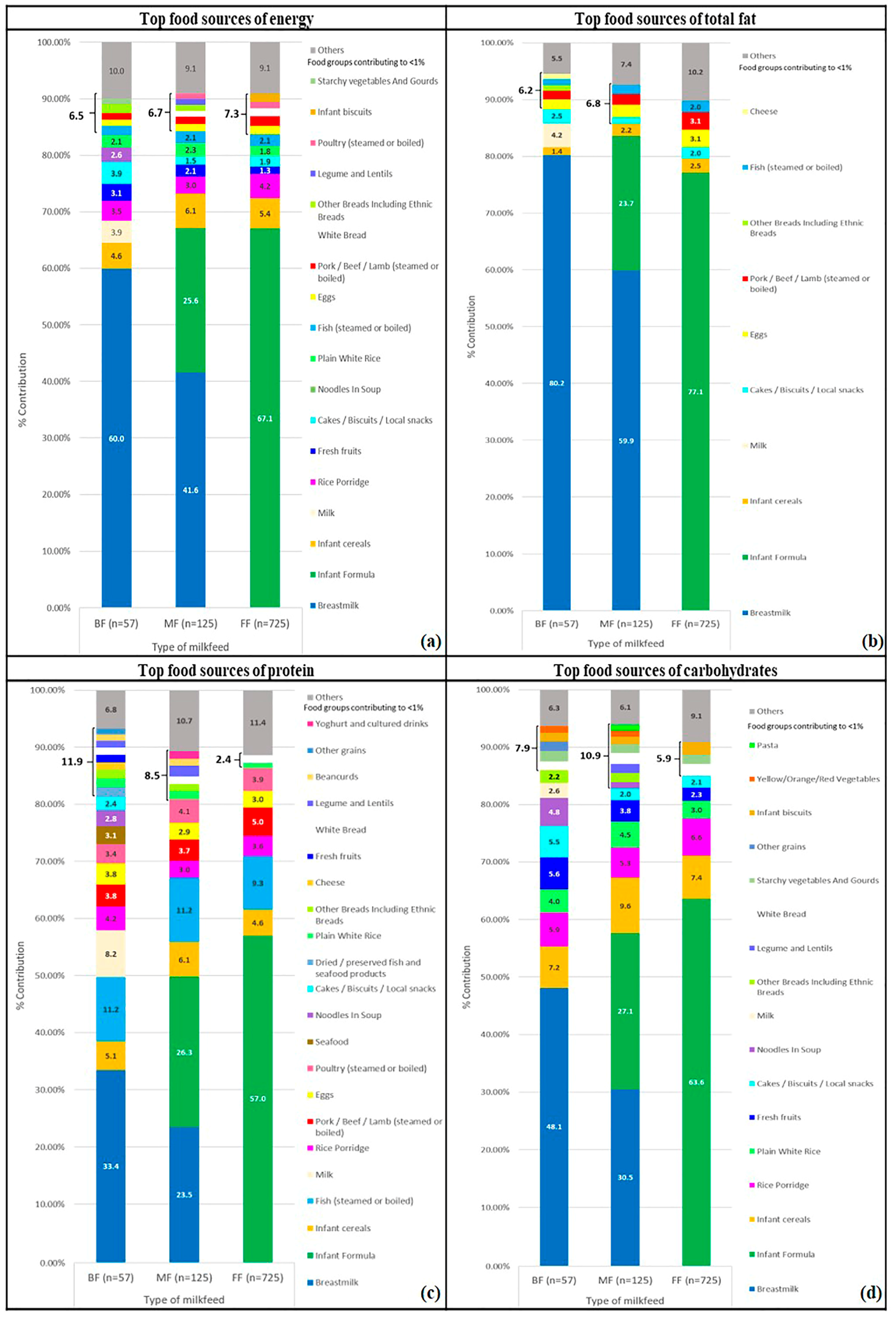
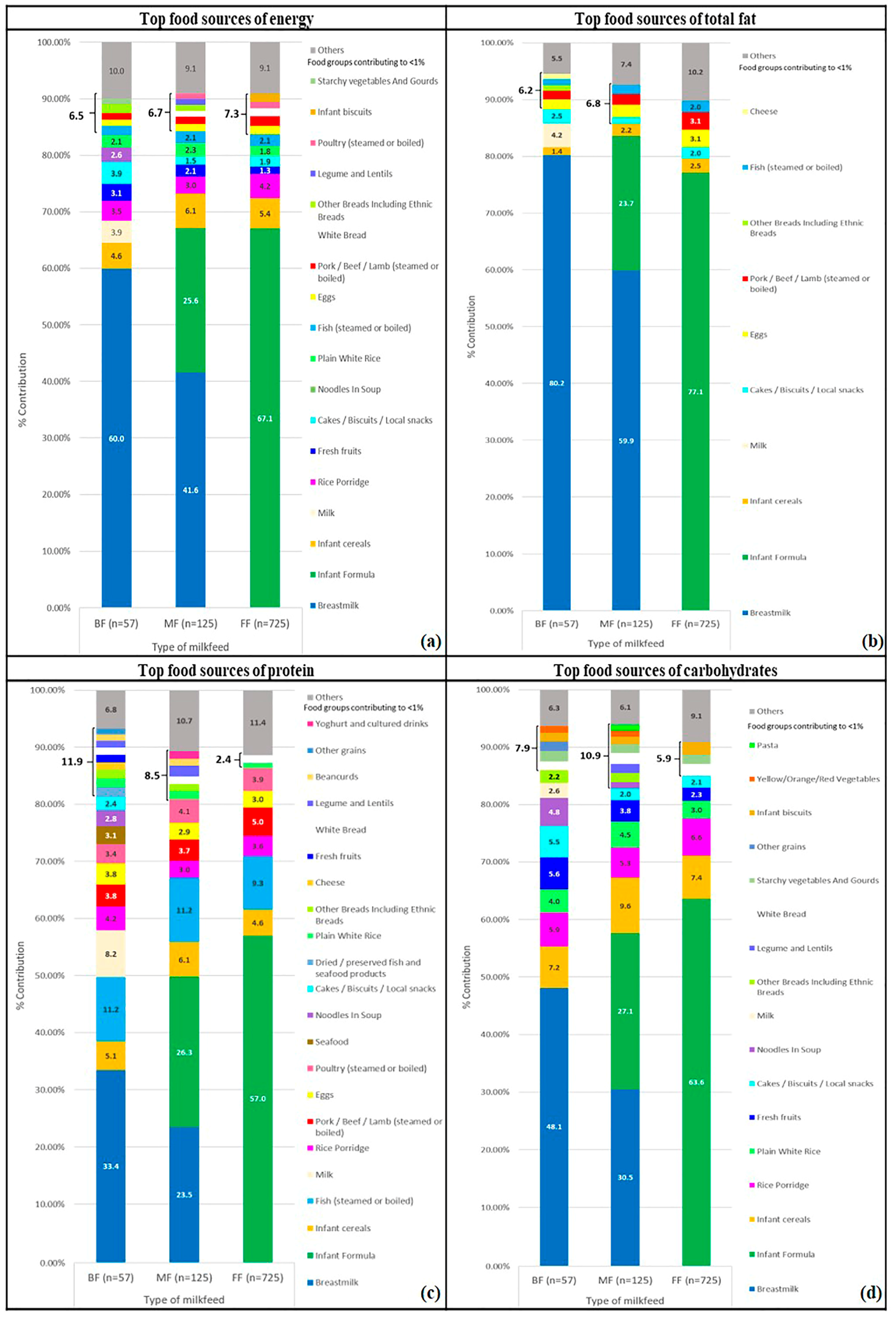
3.4. Key Food Sources of Energy and Macronutrient of Infants by Milk-Feed Type
4. Discussion
4.1. Energy and Macronutrient Intakes of All Infants and by Milk-Feed Type
4.2. Top Food Sources of Energy and Macronutrient of Infants
4.3. Strengths and Limitations
4.4. Implications for Local Recommendations and Policies
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organisation (WHO). Strengthening Action to Improve Feeding of Infants and Young Children 6–23 Months of Age in Nutrition and Child Health Programmes; World Health Organisation (WHO): Geneva, Switzerland, 2008. [Google Scholar]
- Poskitt, E.; Breda, J. Complementary feeding and non communicable diseases: Current knowledge and future research needs. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 819–822. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.K.; Reidy, K.; Novak, T.; Ziegler, P. Sources of energy and nutrients in the diets of infants and toddlers. J. Am. Diet. Assoc. 2006, 106, e21–e25. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Denney, L.; Zheng, Y.; Vinyes-Pares, G.; Reidy, K.; Wang, P.; Zhang, Y. Food sources of energy and nutrients in the diets of infants and toddlers in urban areas of China, based on one 24-hour dietary recall. BMC Nutr. 2015, 1, 19. [Google Scholar] [CrossRef]
- Lioret, S.; McNaughton, S.A.; Spence, A.C.; Crawford, D.; Campbell, K.J. Tracking of dietary intakes in early childhood: The Melbourne infant program. Eur. J. Clin. Nutr. 2013, 67, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Newby, R.M.; Davies, P.S.W. A prospective study of the introduction of complementary foods in contemporary Australian infants: What, when and why? J. Paediatr. Child Health 2015, 51, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Le Nguyen, B.K.; Le Thi, H.; Nguyen Do, V.A.; Tran Thuy, N.; Nguyen Huu, C.; Thanh Do, T.; Deurenberg, P.; Khouw, I. Double burden of undernutrition and overnutrition in Vietnam in 2011: Results of the SEANUTS study in 0.5-11-year-old children. Br. J. Nutr. 2013, 110 (Suppl. S3), S45–S56. [Google Scholar] [CrossRef] [PubMed]
- Poh, B.K.; Ng, B.K.; Siti Haslinda, M.D.; Nik Shanita, S.; Wong, J.E.; Budin, S.B.; Ruzita, A.T.; Ng, L.O.; Khouw, I.; Norimah, A.K. Nutritional status and dietary intakes of children aged 6 months to 12 years: Findings of the nutrition survey of Malaysian children (SEANUTS malaysia). Br. J. Nutr. 2013, 110 (Suppl. S3), S21–S35. [Google Scholar] [CrossRef]
- Rojroongwasinkul, N.; Kijboonchoo, K.; Wimonpeerapattana, W.; Purttiponthanee, S.; Yamborisut, U.; Boonpraderm, A.; Kunapan, P.; Thasanasuwan, W.; Khouw, I. Seanuts: The nutritional status and dietary intakes of 0.5–12-year-old Thai children. Br. J. Nutr. 2013, 110 (Suppl. S3), S36–S44. [Google Scholar] [CrossRef] [PubMed]
- Sandjaja, S.; Budiman, B.; Harahap, H.; Ernawati, F.; Soekatri, M.; Widodo, Y.; Sumedi, E.; Rustan, E.; Sofia, G.; Syarief, S.N.; et al. Food consumption and nutritional and biochemical status of 0.5-12-year-old Indonesian children: The SEANUTS study. Br. J. Nutr. 2013, 110 (Suppl. S3), S11–S20. [Google Scholar]
- Health Promotion Board. A Mum’s Guide to Early Childhood Nutrition (6–12 Months); Health Promotion Board: Singapore, 2017. [Google Scholar]
- Soh, S.-E.; Tint, M.T.; Gluckman, P.D.; Godfrey, K.M.; Rifkin-Graboi, A.; Chan, Y.H.; Stünkel, W.; Holbrook, J.D.; Kwek, K.; Chong, Y.-S. Cohort profile: Growing Up in Singapore towards healthy Outcomes (GUSTO) birth cohort study. Int. J. Epidemiol. 2013, 43, 1401–1409. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.M.; Ingwersen, L.A.; Vinyard, B.T.; Moshfegh, A.J. Effectiveness of the US department of agriculture 5-step multiple-pass method in assessing food intake in obese and nonobese women. Am. J. Clin. Nutr. 2003, 77, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Lim, G.H.; Toh, J.Y.; Aris, I.M.; Chia, A.-R.; Han, W.M.; Saw, S.M.; Godfrey, K.M.; Gluckman, P.D.; Chong, Y.-S.; Yap, F. Dietary pattern trajectories from 6 to 12 months of age in a multi-ethnic Asian cohort. Nutrients 2016, 8, 365. [Google Scholar] [CrossRef] [PubMed]
- Ponza, M.; Devaney, B.; Ziegler, P.; Reidy, K.; Squatrito, C. Nutrient intakes and food choices of infants and toddlers participating in WIC. J. Am. Diet. Assoc. 2004, 104, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G.; Finley, D.A.; Lonnerdal, B. Breast milk volume and composition during late lactation (7–20 months). J. Pediatr. Gastroenterol. Nutr. 1984, 3, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Chong, M.F.-F.; Chia, A.-R.; Colega, M.; Tint, M.-T.; Aris, I.M.; Chong, Y.-S.; Gluckman, P.; Godfrey, K.M.; Kwek, K.; Saw, S.-M. Maternal protein intake during pregnancy is not associated with offspring birth weight in a multiethnic Asian population. J. Nutr. 2015, 145, 1303–1310. [Google Scholar] [PubMed]
- United States Department of Agriculture Agricultural Research Service (USDA) USDA Food Composition Databases. Available online: https://ndb.nal.usda.gov/ndb/search/list (accessed on 18 January 2018).
- Krebs-Smith, S.; Kott, P.; Guenther, P. Mean proportion and population proportion: Two answers to the same question? J. Am. Diet. Assoc. 1989, 89, 671–676. [Google Scholar] [PubMed]
- Ministry of Health, Singapore. Recommended Dietary Allowances for Normal Healthy Persons in Singapore (Children & Adolescents). Available online: https://www.healthhub.sg/live-healthy/192/recommended_dietary_allowances (accessed on 18 January 2018).
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; The National Academies Press: Washington, DC, USA, 2005; p. 1358. [Google Scholar]
- Butte, N.F.; Fox, M.K.; Briefel, R.R.; Siega-Riz, A.M.; Dwyer, J.T.; Deming, D.M.; Reidy, K.C. Nutrient intakes of US infants, toddlers, and preschoolers meet or exceed dietary reference intakes. J. Am. Diet. Assoc. 2010, 110, S27–S37. [Google Scholar] [CrossRef] [PubMed]
- Butte, N.F. Fat intake of children in relation to energy requirements. Am. J. Clin. Nutr. 2000, 72, 1246s–1252s. [Google Scholar] [CrossRef] [PubMed]
- Alexy, U.; Kersting, M.; Sichert-Hellert, W.; Manz, F.; Schöch, G. Macronutrient intake of 3- to 36-month-old German infants and children: Results of the DONALD study. Ann. Nutr. Metab. 1999, 43, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Gondolf, U.H.; Tetens, I.; Michaelsen, K.F.; Trolle, E. Dietary habits of partly breast-fed and completely weaned infants at 9 months of age. Public Health Nutr. 2012, 15, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Conn, J.A.; Davies, M.J.; Walker, R.B.; Moore, V.M. Food and nutrient intakes of 9-month-old infants in Adelaide, Australia. Public Health Nutr. 2009, 12, 2448–2456. [Google Scholar] [CrossRef] [PubMed]
- Grimes, C.A.; Szymlek-Gay, E.A.; Campbell, K.J.; Nicklas, T.A. Food sources of total energy and nutrients among U.S. Infants and toddlers: National health and nutrition examination survey 2005–2012. Nutrients 2015, 7, 6797–6836. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A.M.; Paul, A.A. Fat and energy needs of children in developing countries. Am. J. Clin. Nutr. 2000, 72, 1253s–1265s. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Ramirez, S.; Munoz-Espinosa, A.; Rivera, J.A.; Gonzalez-Castell, D.; Gonzalez de Cosio, T. Mexican children under 2 years of age consume food groups high in energy and low in micronutrients. J. Nutr. 2016, 146, 1916s–1923s. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, G. Deliveries in Singapore Volume and Resources; Ministry of Health Information Paper, Ministry of Health: Singapore, 2004. Available online: https://www.moh.gov.sg/content/dam/moh_web/Publications/Information%20Papers/2004/Deliveries_in_Singapore_Paper.pdf (accessed on 25 February 2018).
- Tham, E.H.; Lee, B.W.; Chan, Y.H.; Loo, E.X.L.; Toh, J.Y.; Goh, A.; Teoh, O.H.; Yap, F.; Tan, K.H.; Godfrey, K.M.; et al. Low food allergy prevalence despite delayed introduction of allergenic foods-data from the GUSTO cohort. J. Allergy Clin. Immunol. Pract. 2017. [Google Scholar] [CrossRef] [PubMed]
- James, D.C.; Lessen, R. Position of the American Dietetic Association: Promoting and supporting breastfeeding. J. Am. Diet. Assoc. 2009, 109, 1926–1942. [Google Scholar] [PubMed]
- Mennella, J.A.; Forestell, C.A.; Morgan, L.K.; Beauchamp, G.K. Early milk feeding influences taste acceptance and liking during infancy. Am. J. Clin. Nutr. 2009, 90, 780s–788s. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Singapore. Baby-friendly Hospital Initiative. 2013. Available online: https://www.moh.gov.sg/content/moh_web/home/pressRoom/Parliamentary_QA/2013/baby-friendly-hospital-initiative.html (accessed on 25 February 2018).
- U.S. Department of Health and Human Services. Centers for Disease Control and Prevention, Strategies to Prevent Obesity and Other Chronic Diseases: The CDC Guide to Strategies to Support Breastfeeding Mothers and Babies; U.S. Department of Health and Human Services: Atlanta, GA, USA, 2013. [Google Scholar]

{kind=link}
{kind=link}
| Characteristics | Total Study Population | Completed at Least a Single-Day Dietary Record at 6, 9 and/or 12 Months | Did Not Complete Any Single-Day Dietary Record at 6, 9 and 12 Months | p-Value * |
|---|---|---|---|---|
| n (%) 1 | n (%) 1 | n (%) 1 | ||
| Infant | ||||
| Gender 2 | 0.703 | |||
| Male | 619 (52.9) | 545 (52.7) | 74 (54.8) | |
| Female | 551 (47.1) | 490 (47.3) | 61 (45.2) | |
| Gestational Age 2 | 0.006 | |||
| <37 weeks | 91 (7.8) | 72 (7.0) | 19 (14.1) | |
| ≥37 weeks | 1079 (92.2) | 963 (93.0) | 116 (85.9) | |
| Parity 2 | 0.235 | |||
| First child | 534 (46.0) | 465 (45.3) | 69 (51.1) | |
| Not the first child | 628 (54.0) | 562 (54.7) | 66 (48.9) | |
| Duration of any breastfeeding 2 | 0.005 | |||
| Never | 50 (4.7) | 48 (4.7) | 2 (4.8) | |
| <3 months | 423 (39.6) | 396 (38.6) | 27 (64.3) | |
| ≥3 months | 594 (55.7) | 581 (56.7) | 13 (31.0) | |
| Age of introduction of first foods 2 | ||||
| ≤15 weeks | 20 (2.4) | 20 (2.4) | Missing data | NA |
| 16–23 weeks | 291 (34.6) | 291 (34.6) | ||
| 24–31 weeks | 495 (58.9) | 495 (58.9) | ||
| ≥32 weeks | 34 (4.0) | 34 (4.0) | ||
| Maternal | ||||
| Maternal age | <0.001 | |||
| 18 to 29 | 527 (42.6) | 419 (40.5) | 108 (53.5) | |
| 30 to 34 | 416 (33.6) | 352 (34.0) | 64 (31.7) | |
| >34 | 294 (23.8) | 264 (25.5) | 30 (14.9) | |
| Ethnicity | 0.012 | |||
| Chinese | 691 (55.9) | 594 (57.4) | 97 (48.0) | |
| Malay | 322 (26.0) | 253 (24.4) | 69 (34.2) | |
| Indian | 224 (18.1) | 188 (18.2) | 36 (17.8) | |
| Education 2 | <0.001 | |||
| None/Primary/Secondary | 381 (31.2) | 299 (29.2) | 82 (41.6) | |
| Post-secondary | 431 (35.3) | 360 (35.2) | 71 (36.0) | |
| University and beyond | 408 (33.4) | 364 (35.6) | 44 (22.3) | |
| Employment status 2 | 0.289 | |||
| Unemployed | 358 (29.6) | 293 (28.9) | 65 (33.0) | |
| Employed | 852 (70.4) | 720 (71.1) | 132 (67.0) | |
| Monthly household income 2 | <0.001 | |||
| ≤$1999 | 181 (15.7) | 140 (14.5) | 41 (22.2) | |
| $2000–$5999 | 640 (55.6) | 532 (55.0) | 108 (58.4) | |
| ≥$6000 | 331 (28.7) | 295 (30.5) | 36 (19.5) | |
| Body mass index (BMI) at 26 weeks of gestation 2 | 0.508 | |||
| <18.5 to 24.9 | 486 (46.6) | 422 (46.2) | 64 (48.9) | |
| 25 to 29.9 | 364 (34.9) | 319 (34.9) | 45 (34.4) | |
| >30 | 194 (18.6) | 172 (18.8) | 22 (16.8) | |
| Alcohol consumption before pregnancy 2 | 0.677 | |||
| Yes | 410 (35.1) | 356 (34.8) | 54 (37.0) | |
| No | 758 (64.9) | 666 (65.2) | 92 (63.0) | |
| Alcohol consumption during pregnancy 2 | 0.986 | |||
| Yes | 20 (1.7) | 18 (1.8) | 2 (1.4) | |
| No | 1128 (98.3) | 985 (98.2) | 143 (98.6) | |
| Smoking before pregnancy 2 | 0.019 | |||
| Yes | 156 (13.3) | 127 (12.4) | 29 (19.9) | |
| No | 1014 (86.7) | 897 (87.6) | 117 (80.1) | |
| Smoking during pregnancy 2 | 0.285 | |||
| Yes | 29 (1.7) | 23 (2.2) | 6 (4.1) | |
| No | 1140 (97.5) | 1000 (97.8) | 140 (95.9) | |
| Dietary Intakes of Energy, Macronutrient and Fibre | Recommended Intakes | All | Breast-Fed (BF) | Mixed-Fed (MF) | Formula-Fed (FF) | p-Value (by Milk-Feed Type) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 760, 893, 907) ‡ | (n = 120, 94, 57) ‡ | (n = 160, 149, 125) ‡ | (n = 480, 650, 725) ‡ | ||||||||
| Mean | Standard Deviation (SD) | Mean | SD | Mean | SD | Mean | SD | ||||
| Energy (TE) (kcal) | EAR of Male/Female (HPB) † | ||||||||||
| 6 months | 600/560 | 640 | 158 | 652 | 112 | 647 | 98 | 634 | 182 | 0.450 | |
| 9 months | 670/620 | 675 | 173 | 580 a | 122 | 683 b | 137 | 687 b | 183 | <0.001 | |
| 12 months | 740/640 | 761 | 208 | 716 | 187 | 795 | 164 | 759 | 216 | 0.050 | |
| Protein (TE%) | AMDR (IOM) † | ||||||||||
| 6 months | - | 9.9 | 2.5 | 7.1 a | 0.7 | 9.2 b | 1.8 | 10.8 c | 2.4 | <0.001 | |
| 9 months | - | 13.1 | 3.1 | 10.5 a | 3.0 | 11.6 b | 2.8 | 13.8 c | 2.8 | <0.001 | |
| 12 months | 5–20 | 14.5 | 3.4 | 10.9 a | 3.4 | 12.5 b | 2.7 | 15.1 c | 3.2 | <0.001 | |
| Total Fat (TE%) | AMDR (IOM) † | ||||||||||
| 6 months | - | 42.0 | 6.3 | 49.7 a | 3.1 | 44.4 b | 4.3 | 39.2 c | 5.5 | <0.001 | |
| 9 months | - | 36.9 | 5.7 | 38.5 a | 5.1 | 41.7 b | 5.6 | 35.6 c | 5.1 | <0.001 | |
| 12 months | 30–40 | 34.6 | 7.5 | 42.1 a | 9.0 | 41.5 a | 7.0 | 32.8 b | 6.3 | <0.001 | |
| Carbohydrate (TE%) | AMDR (IOM) † | ||||||||||
| 6 months | - | 48.1 | 5.3 | 43.1 a | 2.8 | 46.4 b | 3.7 | 50.0 c | 5.2 | <0.001 | |
| 9 months | - | 50.0 | 5.7 | 51.0 a | 5.3 | 46.7 b | 5.3 | 50.6 a | 5.5 | <0.001 | |
| 12 months | 45–65 | 50.9 | 7.6 | 47.0 a | 8.1 | 46.0 a | 6.5 | 52.1 b | 7.4 | <0.001 | |
| Dietary Fibre (g per 1000 kcal of TE) § | |||||||||||
| 6 months | - | 2.5 | 2.7 | 1.1 a | 1.6 | 1.9 a | 2.2 | 3.0 b | 2.9 | <0.001 | |
| 9 months | - | 4.0 | 3.1 | 3.9 | 3.5 | 4.0 | 2.9 | 4.0 | 3.1 | 0.981 | |
| 12 months | - | 4.4 | 3.3 | 4.7 | 2.7 | 4.3 | 3.8 | 4.4 | 3.2 | 0.743 | |
| Dietary Intake of Energy (kcal) | Recommended Intakes | All | Breast-Fed | Mixed-Fed | Formula-Fed | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| (n = 760, 893, 907) * | (n = 120, 94, 57) * | (n = 160, 149, 125) * | (n = 480, 650, 725) * | |||||||
| EAR (HPB) † | Mean (Standard Deviation) | |||||||||
| Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | |
| 6 months | 600 | 560 | 655 (164) | 623 (151) | 662 (129) | 642 (94) | 649 (103) | 644 (94) | 655 (186) | 611 (178) |
| 9 months | 670 | 620 | 692 (171) | 658 (175) | 592 (111) | 567 (134) | 682 (127) | 685 (148) | 709 (182) | 665 (182) |
| 12 months | 740 | 640 | 781 (219) | 741 (195) | 720 (129) | 711 (245) | 829 (187) | 757 (127) | 778 (229) | 741 (201) |
| Dietary Intake of Energy (kcal) | EAR (HPB) † | Percentage of Infants Meeting the EAR (HPB) (%) # | ||||||||
| Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | |
| 6 months | 600 | 560 | 62.6 | 69.5 | 70.2 | 90.5 | 72.1 | 90.3 | 57.8 | 56.1 |
| 9 months | 670 | 620 | 50.2 | 56.2 | 18.4 | 33.3 | 44.9 | 67.2 | 56.2 | 57.1 |
| 12 months | 740 | 640 | 54.3 | 67.3 | 46.9 | 52.0 | 71.2 | 84.2 | 51.9 | 65.6 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, S.-X.; Toh, J.-Y.; Van Lee, L.; Han, W.-M.; Shek, L.P.-C.; Tan, K.-H.; Yap, F.; Godfrey, K.M.; Chong, Y.-S.; Chong, M.F.-F. Food Sources of Energy and Macronutrient Intakes among Infants from 6 to 12 Months of Age: The Growing Up in Singapore Towards Healthy Outcomes (GUSTO) Study. Int. J. Environ. Res. Public Health 2018, 15, 488. https://doi.org/10.3390/ijerph15030488
Lim S-X, Toh J-Y, Van Lee L, Han W-M, Shek LP-C, Tan K-H, Yap F, Godfrey KM, Chong Y-S, Chong MF-F. Food Sources of Energy and Macronutrient Intakes among Infants from 6 to 12 Months of Age: The Growing Up in Singapore Towards Healthy Outcomes (GUSTO) Study. International Journal of Environmental Research and Public Health. 2018; 15(3):488. https://doi.org/10.3390/ijerph15030488
Chicago/Turabian StyleLim, Shan-Xuan, Jia-Ying Toh, Linde Van Lee, Wee-Meng Han, Lynette Pei-Chi Shek, Kok-Hian Tan, Fabian Yap, Keith M. Godfrey, Yap-Seng Chong, and Mary Foong-Fong Chong. 2018. "Food Sources of Energy and Macronutrient Intakes among Infants from 6 to 12 Months of Age: The Growing Up in Singapore Towards Healthy Outcomes (GUSTO) Study" International Journal of Environmental Research and Public Health 15, no. 3: 488. https://doi.org/10.3390/ijerph15030488