Preferences in Information Processing, Marginalized Identity, and Non-Monogamy: Understanding Factors in Suicide-Related Behavior among Members of the Alternative Sexuality Community

 , ,
, ,
Abstract
:1. Introduction
1.1. Background
1.2. Suicide-Related Behavior among the Alternative Sexuality Community
1.3. Relationship Orientation, Marginalized Identity, and Preferences in Information Processing Applied to Suicide
1.4. The Present Study
2. Materials and Methods
2.1. Study Design and Procedure
2.2. Participants
2.3. Measures
2.3.1. Demographics
2.3.2. Suicide-Related Behavior
2.3.3. Preferences in Information Processing
2.3.4. Mental Health
2.4. Data Analysis
3. Results
3.1. Bivariate Analyses
3.2. Multi-Nomial Regression Model Testing Covariate and PIP Effects on Lifetime SRB Group Status
Multinomial Model Summary
4. Discussion
Implications for Research, Health Education, and Suicide Prevention
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- History of NCSF. Available online: https://ncsfreedom.org/who-we-are/the-history-of-the-ncsf/ (accessed on 31 March 2020).
- Hughes, S.D.; Hammack, P.L. Affirmation, compartmentalization, and isolation: Narratives of identity sentiment among kinky people. Psychol. Sex. 2019, 10, 149–168. [Google Scholar] [CrossRef]
- Wright, S. Discrimination of SM-identified individuals. J. Homosex. 2006, 50, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Wright, S. Depathologizing consensual sexual sadism, sexual masochism, transvestic fetishism, and fetishism. Arch. Sex. 2010, 39, 1229–1230. [Google Scholar] [CrossRef] [PubMed]
- Hatzenbuehler, M.L.; Phelan, J.C.; Link, B.G. Stigma as a fundamental cause of population health inequalities. Am. J. Public Health 2013, 103, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Herek, G.M. A nuanced view of stigma for understanding and addressing sexual and gender minority health disparities. Lgbt. Health 2016, 3, 397–399. [Google Scholar] [CrossRef] [PubMed]
- Rivera, L.M. Ethnic-racial stigma and health disparities: From psychological theory and evidence to public policy solutions. J. Soc. Issues 2014, 70, 198–205. [Google Scholar] [CrossRef] [Green Version]
- Fredriksen-Goldsen, K.I.; Simoni, J.M.; Kim, H.J.; Lehavot, K.; Walters, K.L.; Yang, J.; Hoy-Ellis, C.P.; Muraco, A. The health equity promotion model: Reconceptualization of lesbian, gay, bisexual, and transgender (LGBT) health disparities. Am. J. Orthopsychiat. 2014, 84, 653–663. [Google Scholar] [CrossRef] [Green Version]
- Psychological Functioning and Violence Victimization and Perpetration in BDSM Practitioners from the National Coalition for Sexual Freedom. Available online: https://pdfs.semanticscholar.org/0cd8/abb591fda8685091c1f208bc757d616f0903.pdf (accessed on 31 March 2020).
- Glossary. Available online: https://secureservercdn.net/198.71.233.68/9xj.1d5.myftpupload.com/wp-content/uploads/2019/12/BDSM-Glossary.pdf (accessed on 28 April 2020).
- Glossary of terms. Available online: https://pflag.org/glossary (accessed on 28 April 2020).
- Brown, S.L.; Roush, J.F.; Mitchell, S.M.; Cukrowicz, K.C. Suicide risk among BDSM practitioners: The role of acquired capability for suicide. J. Clin. Psychol. 2017, 73, 1642–1654. [Google Scholar] [CrossRef]
- Roush, J.F.; Brown, S.L.; Mitchell, S.M.; Cukrowicz, K.C. Shame, guilt, and suicide ideation among Bondage and Discipline, Dominance and Submission, and Sadomasochism practitioners: Examining the role of the Interpersonal Theory of Suicide. Suicide Life-Threat Behav. 2017, 47, 129–141. [Google Scholar] [CrossRef]
- Silverman, M.M.; Berman, A.L.; Sandaal, N.D.; O’Carroll, P.W.; Joiner, T.E. Rebuilding the tower of Babel: A revised nomenclature for the study of suicide and suicidal behaviors. Part 2: Suicide-related ideations, communications, and behaviors. Suicide Life-Threat Behav. 2007, 37, 264–277. [Google Scholar] [CrossRef]
- Davaasambuu, S.; Philip, H.; Ravindran, A.; Szatmari, P. A scoping review of evidence-based interventions for adolescents with depression and suicide related behaviors in low and middle income countries. Community Ment Health J. 2019, 55, 954–972. [Google Scholar] [CrossRef] [PubMed]
- Finlayson-Short, L.; Hetrick, S.; Krysinska, M.; Salom, C.; Bailey, E.; Robinson, J. A survey of people with lived experience of suicide-related behavior in Queensland, Australia: Their experiences with available resources. Crisis 2020, 41, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, S.; Cramer, R.J.; McFadden, C.; Haile, C.R.; Sime, V.L.; Wilsey, C.N. Sexual orientation and the integrated motivational–volitional model of suicidal behavior: Results from a cross-sectional study of young adults in the United Kingdom. Arch. Suicide Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Osman, A.; Bagge, C.L.; Gutierrez, P.M.; Konick, L.C.; Kopper, B.A.; Barrios, F.X. The Suicidal Behaviors Questionnaire-Revised (SBQ-R): Validation with clinical and nonclinical samples. Assessment 2001, 8, 443–454. [Google Scholar] [CrossRef]
- Joiner, T.E. Why People Die by Suicide; Harvard University Press: Cambridge, MA, USA, 2005. [Google Scholar]
- Cramer, R.J.; Mandracchia, J.; Gemberling, T.M.; Holley, S.R.; Wright, S.; Moody, K.; Nobles, M.R. Can need for affect and sexuality differentiate suicide risk in three community samples? J. Soc. Clin. Psychol. 2017, 36, 704–722. [Google Scholar] [CrossRef]
- Cramer, R.J.; Wright, S.; Long, M.M.; Kapusta, N.D.; Nobles, M.R.; Gemberling, T.M.; Wechsler, H.J. On hate crime victimization: Rates, types, and links with suicide risk among sexual orientation minority special interest group members. J. Trauma Dissociation 2018, 19, 476–489. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Kirtley, O.J. The integrated motivational-volitional model of suicidal behaviour. Philos T. R. Soc. B 2018, 373, 20170268. [Google Scholar] [CrossRef] [Green Version]
- Fairweather, A.K.; Anstey, K.J.; Rodgers, B.; Butterworth, P. Factors distinguishing suicide attempters from suicide ideators in a community sample: Social issues and physical health problems. Psychol. Med. 2006, 36, 1235–1245. [Google Scholar] [CrossRef]
- Langhinrichsen-Rohling, J.; Snarr, J.D.; Slep, A.M.S.; Heyman, R.E. Risk for suicide attempts among United States air force active duty members with suicide ideation: An ecological perspective. J. Consult. Clin. Psychol. 2019, 87, 1124–1136. [Google Scholar] [CrossRef]
- May, A.M.; Klonsky, E.D. What distinguishes suicide attempters from suicide ideators? A meta-analysis of potential factors. Clin. Psychol. Sci. Pr. 2016, 23, 5–20. [Google Scholar] [CrossRef]
- Nock, M.K.; Millner, A.J.; Joiner, T.E.; Gutierrez, P.M.; Han, G.; Hwang, I.; King, A.; Naifeh, J.A.; Sampson, N.A.; Zaslavsky, A.M.; et al. Risk factors for the transition from suicide ideation to suicide attempt: Results from the army study to assess risk and resilience in Servicemembers (Army STARRS). J. Abnorm. 2018, 127, 139–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cramer, R.J.; Kapusta, N.D. A social-ecological framework of theory, assessment, and prevention of suicide. Front. Psychol. 2017, 8, 1756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Sex. Orientat Gend. Divers. 2013, 1, 3–26. [Google Scholar] [CrossRef] [Green Version]
- Sherman, A.D.F.; Clark, K.D.; Robinson, K.; Noorani, T.; Poteat, T. Trans* community connection, health, and wellbeing: A systematic review. Lgbt. Health 2020, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Kposowa, A.J. Marital status and suicide in the National Longitudinal Mortality Study. J. Epidemiol. Commun. H. 2000, 54, 254–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.C.; Mercy, J.A.; Cohn, J.M. Marital status and the risk of suicide. Am. J. Public Health 1988, 78, 78–80. [Google Scholar] [CrossRef] [Green Version]
- Pitagora, D. The kink-poly confluence: Relationship intersectionality in marginalized communities. Sex. Relatsh. 2016, 31, 391–405. [Google Scholar] [CrossRef]
- Balzarini, R.N.; Dharma, C.; Kohut, T.; Holmes, B.M.; Campbell, L.; Lehmiller, J.J.; Harman, J.J. Demographic comparison of American individuals in polyamorous and monogamous relationships. J. Sex. Res. 2019, 56, 681–694. [Google Scholar] [CrossRef]
- Manley, M.H.; Diamond, L.M.; Van Anders, S.M. Polyamory, monoamory, and sexual fluidity: A longitudinal study of identity and sexual trajectories. Psychol Sex. Orientat. Gend. Divers. 2015, 2, 168–180. [Google Scholar] [CrossRef]
- Ferrer, J.N. Mononormativity, Polypride, and the “Mono–Poly Wars”. Sex. Cult. 2018, 22, 817–836. [Google Scholar] [CrossRef]
- Rubel, A.N.; Bogaert, A.F. Consensual nonmonogamy: Psychological well-being and relationship quality correlates. J. Sex. Res. 2015, 52, 961–982. [Google Scholar] [CrossRef]
- Dover, D.C.; Belon, A.P. The health equity measurement framework: A comprehensive model to measure social inequities in health. Int. J. Equity Health 2019, 18, 36. [Google Scholar] [CrossRef] [Green Version]
- Damm, C.; Dentato, M.P.; Busch, N. Unravelling intersecting identities: Understanding the lives of people who practice BDSM. Psychol. Sex. 2018, 9, 21–37. [Google Scholar]
- Fraser, B.; Pierse, N.; Chisholm, E.; Cook, H. LGBTIQ+ homelessness: A review of the literature. Int. J. Environ. Res. Public Health 2019, 16, 2677. [Google Scholar] [CrossRef] [Green Version]
- Ingram, L.D.; Stafford, C.; Deming, M.E.; Anderson, J.D.; Robillard, A.; Li, X. A systematic mixed studies review of the intersections of social-ecological factors and HIV stigma in people living with HIV in the U.S. south. J. Assoc. Nurse Aids C 2019, 30, 330–343. [Google Scholar] [CrossRef]
- English, D.; Carter, J.A.; Forbes, N.; Bowleg, L.; Malebranche, D.J.; Talan, A.J.; Rendina, H.J. Intersectional discrimination, positive feelings, and health indicators among Black sexual minority men. Health Psychol. 2020, 39, 220–229. [Google Scholar] [CrossRef]
- Lefevor, G.T.; Blaber, I.P.; Huffman, C.E.; Schow, R.L.; Beckstead, A.L.; Raynes, M.; Rosik, C.H. The role of religiousness and beliefs about sexuality in well-being among sexual minority Mormons. Psychol Relig Spirit. 2019. [Google Scholar] [CrossRef]
- Noyola, N.; Sánchez, M.; Cardemil, E.V. Minority stress and coping among sexual diverse Latinxs. J. Lat. Psychol. 2020, 8, 58–82. [Google Scholar] [CrossRef]
- Haas, A.P.; Eliason, M.; Mays, V.M.; Mathy, R.M.; Cochran, S.D.; D’Augelli, A.R.; Silverman, M.M.; Fisher, P.W.; Hughes, T.; Rosario, M.; et al. Suicide and suicide risk in lesbian, gay, bisexual, and transgender populations: Review and recommendations. J. Homosex. 2011, 58, 10–51. [Google Scholar] [CrossRef]
- Horwitz, A.G.; Berona, J.; Busby, D.R.; Eisenberg, D.; Zheng, K.; Pistorello, J.; Albucher, R.; Coryell, W.; Favorite, T.; Walloch, J.C.; et al. Variation in suicide risk among subgroups of sexual and gender minority college students. Suicide Life-Threat. Behav. 2020. Advance online publication. [Google Scholar] [CrossRef]
- Pompili, M.; Lester, D.; Forte, A.; Seretti, M.; Eruto, O.; Lamis, D.A.; Amore, M.; Girardi, P. Bisexuality and suicide: A systematic review. J. Sex. Med. 2014, 11, 1903–1913. [Google Scholar] [CrossRef] [PubMed]
- Standley, C.J. Expanding our paradigms: Intersectional and socioecological approaches to suicide prevention. Death Stud. 2020. [Google Scholar] [CrossRef] [PubMed]
- Vargas, S.M.; Huey, S.J.; Miranda, J. A critical review of current evidence on multiple types of discrimination and mental health. Am. J. Orthopsychiat 2020, 90, 374–390. [Google Scholar] [CrossRef]
- Wolford-Clevenger, C.; Frantell, K.; Smith, P.N.; Flores, L.Y.; Stuart, G.L. Correlates of suicide ideation and behaviors among transgender people: A systematic review guided by ideation-to-action theory. Clin. Psychol. Rev. 2018, 63, 93–105. [Google Scholar] [CrossRef]
- Cramer, R.J.; Bryson, C.N.; Gardner, B.O.; Webber, W.B. Can preferences in information processing aid in understanding suicide risk among emerging adults? Death Stud. 2016, 40, 383–391. [Google Scholar] [CrossRef]
- Kirkpatrick, L.A.; Epstein, S. Cognitive-experiential self-theory and subjective probability: Further evidence for two conceptual systems. J. Pers. Soc. Psychol. 1992, 63, 534–544. [Google Scholar] [CrossRef]
- Petty, R.E.; Briñol, P. Emotion and persuasion: Cognitive and meta-cognitive processes impact attitudes. Cogn. Emot. 2015, 29, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Appel, M.; Gnambs, T.; Maio, G.R. A short measure of the need for affect. J. Pers. Assess. 2012, 94, 418–426. [Google Scholar] [CrossRef]
- Maio, G.R.; Esses, V.M. The Need for Affect: Individual differences in the motivation to approach or avoid emotions. J. Pers. 2001, 69, 583–614. [Google Scholar] [CrossRef]
- Cramer, R.J.; Wevodau, A.L.; Gardner, B.O.; Bryson, C.N. A validation study of the Need for Affect Questionnaire–Short Form in legal contexts. J. Pers. Assess. 2017, 99, 67–77. [Google Scholar] [CrossRef]
- Petty, R.E.; Cacioppo, J.T. The need for cognition. J. Pers. Soc. Psychol. 1982, 42, 116–131. [Google Scholar]
- Bryson, C.N.; Cramer, R.J.; Schmidt, A.T. Need for Affect, Interpersonal Psychological Theory of Suicide, and suicide proneness. Arch. Suicide Res. 2019, 23, 634–647. [Google Scholar] [CrossRef] [PubMed]
- Cramer, R.J.; Rasmussen, S.; Webber, W.B.; Sime, V.L.; Haile, C.; McFadden, C.; McManus, M.C. Preferences in Information Processing and suicide: Results from a young adult health survey in the United Kingdom. Int. J. Soc. Psychiatry 2019, 65, 46–55. [Google Scholar] [CrossRef]
- Second National Survey of Violence & Discrimination against Sexual Minorities. Available online: https://secureservercdn.net/198.71.233.68/9xj.1d5.myftpupload.com/wpcontent/uploads/2019/12/Violence-Discrimination-Against-Sexual-Minorities-Survey.pdf (accessed on 31 March 2020).
- Becerk, S.P.; Holdaway, A.S.; Luebbe, A.M. Suicidal behaviors in college students: Frequency, sex differences, and mental health correlates including sluggish cognitive tempo. J. Adolesc. Health 2018, 63, 181–188. [Google Scholar]
- Winer, E.S.; Drapeau, C.W.; Veilleux, J.C.; Nadorff, M.R. The association between anhedonia, suicidal ideation, and suicide attempts in a large student sample. Arch. Suicide Res. 2016, 20, 265–272. [Google Scholar] [CrossRef]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychol. Assess. 1998, 10, 176–181. [Google Scholar] [CrossRef]
- Osman, A.; Wong, J.L.; Bagge, C.L.; Freedenthal, S.; Gutierrez, P.M.; Lozano, G. The Depression Anxiety Stress Scales-21 (DASS-21): Further examination of dimensions, scale reliability, and correlates. J. Clin. Psychol. 2012, 68, 1322–1338. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Earlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Chen, H.; Cohen, P.; Chen, S. How big is a big odds ratio? Interpreting the magnitudes of odds ratios in epidemiological studies. Commun. Stat.-Stimul. C 2010, 39, 860–864. [Google Scholar] [CrossRef]
- Balzarini, R.N.; Dharma, C.; Kohut, T.; Campbell, L.; Lehmiller, J.J.; Harman, J.J.; Holmes, B.M. Comparing relationship quality across different types of romantic partners in polyamorous and monogamous relationships. Arch. Sex. Behav. 2019, 48, 1749–1767. [Google Scholar] [CrossRef]
- Bryan, C.J.; Rudd, D.M. Advances in the assessment of suicide risk. J. Clin. Psychol. 2006, 62, 185–200. [Google Scholar] [CrossRef]
- Kleiman, E.M.; Liu, R.T. Social support as a protective factor in suicide: Findings from two nationally representative samples. J. Affect. Disord. 2013, 150, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohr, J.J.; Kendra, M.S. Revision and extension of a multidimensional measure of sexual minority identity: The Lesbian, Gay, and Bisexual Identity Scale. J. Couns. Psychol. 2011, 58, 234–245. [Google Scholar] [CrossRef] [PubMed]
- Mirowsky, J.; Ross, C.E. Education and self-rated health: Cumulative advantage and its rising importance. Res. Aging 2008, 30, 93–122. [Google Scholar] [CrossRef]
- Zajacova, A.; Hummer, R.A.; Rogers, R.G. Education and health among U.S. working-age adults: A detailed Portrait across the full educational attainment spectrum. Biodemogr. Soc. Biol. 2012, 58, 40–61. [Google Scholar] [CrossRef]
- Cerel, J.; Van De Venne, J.G.; Moore, M.M.; Maple, M.J.; Flaherty, C.; Brown, M.M. Veteran exposure to suicide: Prevalence and correlates. J. Affect. Disord. 2015, 179, 82–87. [Google Scholar] [CrossRef]
- Sprott, R.A.; Randall, A.; Davison, K.; Cannon, N.; Witherspoon, R.G. Alternative or nontraditional sexualities and therapy: A case report. J. Clin. Psychol. 2017, 73, 929–937. [Google Scholar] [CrossRef]
- Pillai-Friedman, S.; Pollitt, J.L.; Castaldo, A. Becoming kink-aware—A necessity for sexuality professionals. Sex. Relatsh. 2015, 30, 196–210. [Google Scholar] [CrossRef]
- Waldura, J.F.; Arora, I.; Randall, A.M.; Farala, J.P.; Sprott, R.A. Fifty shades of stigma: Exploring the health care experiences of kink-oriented patients. J. Sex. Med. 2016, 13, 1918–1929. [Google Scholar] [CrossRef]
- Jobes, D.A. The collaborative assessment and management of suicidality (CAMS): An evolving evidence-based clinical approach to suicidal risk. Suicide Life-Threat. Behav. 2012, 42, 640–653. [Google Scholar] [CrossRef]
- Fazel, S.; Runseon, B. Suicide. N. Engl. J. Med. 2020, 382, 266–274. [Google Scholar] [CrossRef]


{kind=link}
| Variable | n (%) |
|---|---|
| Lifetime suicide-related behavior | |
| None | 75 (22.5%) |
| Ideation only | 190 (56.9%) |
| Attempt | 69 (20.7%) |
| Race | |
| White | 285 (85.3%) |
| Black | 5 (1.5%) |
| American Indian/Alaskan Native | 1 (0.3%) |
| Asian American | 2 (0.6%) |
| Native Hawaiian/Pacific Islander | 2 (0.6%) |
| Biracial | 30 (9.0% |
| Other | 9 (2.7%) |
| Sexual Orientation | |
| Gay | 16 (4.8%) |
| Lesbian | 4 (1.2%) |
| Queer | 17 (5.1%) |
| Straight | 73 (21.9%) |
| Questioning | 1 (0.3%) |
| Experimenting | 8 (2.4%) |
| Pansexual | 45 (13.5%) |
| Demisexual | 2 (0.6%) |
| Heteroflexible | 27 (8.1%) |
| Bisexual | 63 (18.9%) |
| Other | 2 (0.6%) |
| Multiple sexual identities | 76 (22.8%) |
| Education | |
| Some high school | 4 (1.2%) |
| High school diploma/general education degree | 61 (18.3%) |
| Associate’s Degree | 56 (16.8%) |
| Bachelor’s Degree | 99 (29.6%) |
| Graduate Degree | 114 (34.1%) |
| Gender | |
| Male | 117 (35.0%) |
| Female | 172 (51.5%) |
| Male-to-female | 7 (2.1%) |
| Female-to-male | 4 (1.2%) |
| Transitioning | 1 (0.3% |
| Queer | 20 (6.0%) |
| Other | 13 (3.9%) |
| Ethnicity | |
| Non-Hispanic/Latino(a) | 320 (95.8%) |
| Hispanic/Latino(a) | 14 (4.2%) |
| Relationship Status | |
| Single | 35 (10.5%) |
| In a monogamous/long-term committed/married/civil union | 113 (33.8%) |
| Non-monogamous | 186 (55.7%) |
| Lifetime Suicide Death Exposure | |
| No | 97 (29.0%) |
| Yes | 237 (71.0%) |
| Lifetime Suicide Attempt Exposure | |
| No | 59 (17.7%) |
| Yes | 275 (82.3%) |
| Variable | Total Sample (N = 334) | None (n = 75) | Ideation Only (n = 190) | Attempt (n = 69) | Test-Statistic (df) | Effect Size |
|---|---|---|---|---|---|---|
| Gender | Χ2 (4) = 12.36, p = 0.01 | 0.19 | ||||
| Male | 117 | 38 (32.5%) | 61 (52.1%) | 18 (15.4%) | ||
| Female | 172 | 32 (18.6%) | 100 (58.1%) | 40 (23.3%) | ||
| TGNC+ | 45 | 5 (11.1%) | 29 (64.4%) | 11 (24.4%) | ||
| Education | Χ2 (6) = 18.70, p = 0.005 | 0.24 | ||||
| Some high school/GED | 65 | 11 (16.9%) | 35 (53.8%) | 19 (29.2%) | ||
| Associate’s degree | 56 | 9 (16.1%) | 32 (57.1%) | 15 (26.8%) | ||
| Bachelor’s degree | 99 | 17 (17.2%) | 59 (59.6%) | 23 (23.2%) | ||
| Graduate degree | 114 | 38 (33.3%) | 64 (64.9%) | 12 (10.5%) | ||
| Sexual Orientation | Χ2 (2) = 7.53, p = 0.02 | 0.15 | ||||
| Straight/heterosexual | 73 | 25 (34.2%) | 36 (49.3%) | 12 (16.4%) | ||
| Sexual minority | 261 | 50 (19.2%) | 154 (59.0%) | 57 (21.8%) | ||
| Relationship Orientation | Χ2 (4) = 19.45, p = 0.01 | 0.24 | ||||
| Single | 35 | 6 (17.1%) | 15 (42.9%) | 14 (40.0%) | ||
| Monogamous Rel. | 113 | 36 (31.9%) | 64 (56.6%) | 13 (11.5%) | ||
| Non-monogamous Rel. | 186 | 33 (17.7%) | 111 (59.7%) | 42 (22.6%) | ||
| Race | Χ2 (2) = 0.84, p = 0.66 | 0.05 | ||||
| White | 285 | 66 (23.2%) | 162 (56.8%) | 57 (20.0%) | ||
| Racial minority | 49 | 9 (18.4%) | 28 (57.1%) | 12 (24.5%) | ||
| Ethnicity | Χ2 (4) = 2.12 p = 0.35 | 0.08 | ||||
| Non-Hispanic/Latino(a) | 320 | 72 (22.5%) | 184 (57.5%) | 64 (20.0%) | ||
| Hispanic/Latino(a) | 14 | 4 (21.4%) | 6 (42.9%) | 5 (35.7%) | ||
| Suicide attempt exposure | 1.29 (0.96) | 0.99 (0.89) a, b | 1.27 (0.90) a | 1.68 (1.06) b | F (2, 331) = 8.75, p < 0.001 | a.31, b.70 |
| Suicide death exposure | 0.92 (0.78) | 0.87 (0.83) | 0.86 (0.72) a | 1.13 (0.87) a | F (2, 331) = 3.28, p = 0.04 | a.34 |
| Total SRB | 7.13 (3.47) | 3.51 (0.93) a, b | 7.17 (2.62) a,c | 10.97 (3.05) b,c | F (2, 331) = 165.85, p < 0.001 | a1.86, b3.31, c1.34 |
| Depression | 5.25 (5.15) | 2.19 (2.50) a,b | 5.51 (4.89) a, c | 7.87 (6.30) b,c | F (2, 331) = 25.78, p < 0.001 | a.85, b1.18, c.42 |
| Anxiety | 4.05 (4.15) | 2.05 (2.49) | 4.00 (3.86) | 6.35 (5.15) | F (2, 331) = 21.60, p < 0.001 | a.60, b1.06, c.52 |
| NFA Approach | 7.28 (5.41) | 6.68 (5.75) | 7.71 (5.05) | 7.28 (5.41) | F (2, 331) = 1.37, p = 0.25 | - |
| NFA Avoidance | −4.70 (7.62) | −7.07 (6.33) a | −4.71 (7.34) b | −2.07 (8.81) a,b | F (2, 331) = 8.04, p < 0.001 | a.65, b.32 |
| Need for Cognition | 70.45 (10.20) | 71.93 (11.28) | 69.94 (9.66) | 70.23 (10.40) | F (2, 331) = 1.04, p = 0.35 | - |
| Predictor | F (df) | p-value |
|---|---|---|
| Intercept | - | - |
| Gender | 1.72 (4) | 0.79 |
| Education level | 12.95 (6) | 0.04 |
| Relationship orientation | 18.52 (4) | 0.001 |
| Sexual orientation | 2.68 (2) | 0.26 |
| Suicide attempt exposure | 5.21 (2) | 0.07 |
| Suicide death exposure | 5.21 (2) | 0.07 |
| Anxiety | 8.46 (2) | 0.01 |
| Depression | 15.71 (2) | <0.001 |
| Need for Affect Approach | 0.03(2) | 0.98 |
| Need for Affect Avoidance | 0.20(2) | 0.90 |
| Need for Cognition | 0.69(2) | 0.71 |
| Anxiety x Need for Affect Approach | 4.54 (2) | 0.10 |
| Anxiety x Need for Affect Avoidance | 0.91 (2) | 0.63 |
| Anxiety x Need for Cognition | 4.23 (2) | 0.12 |
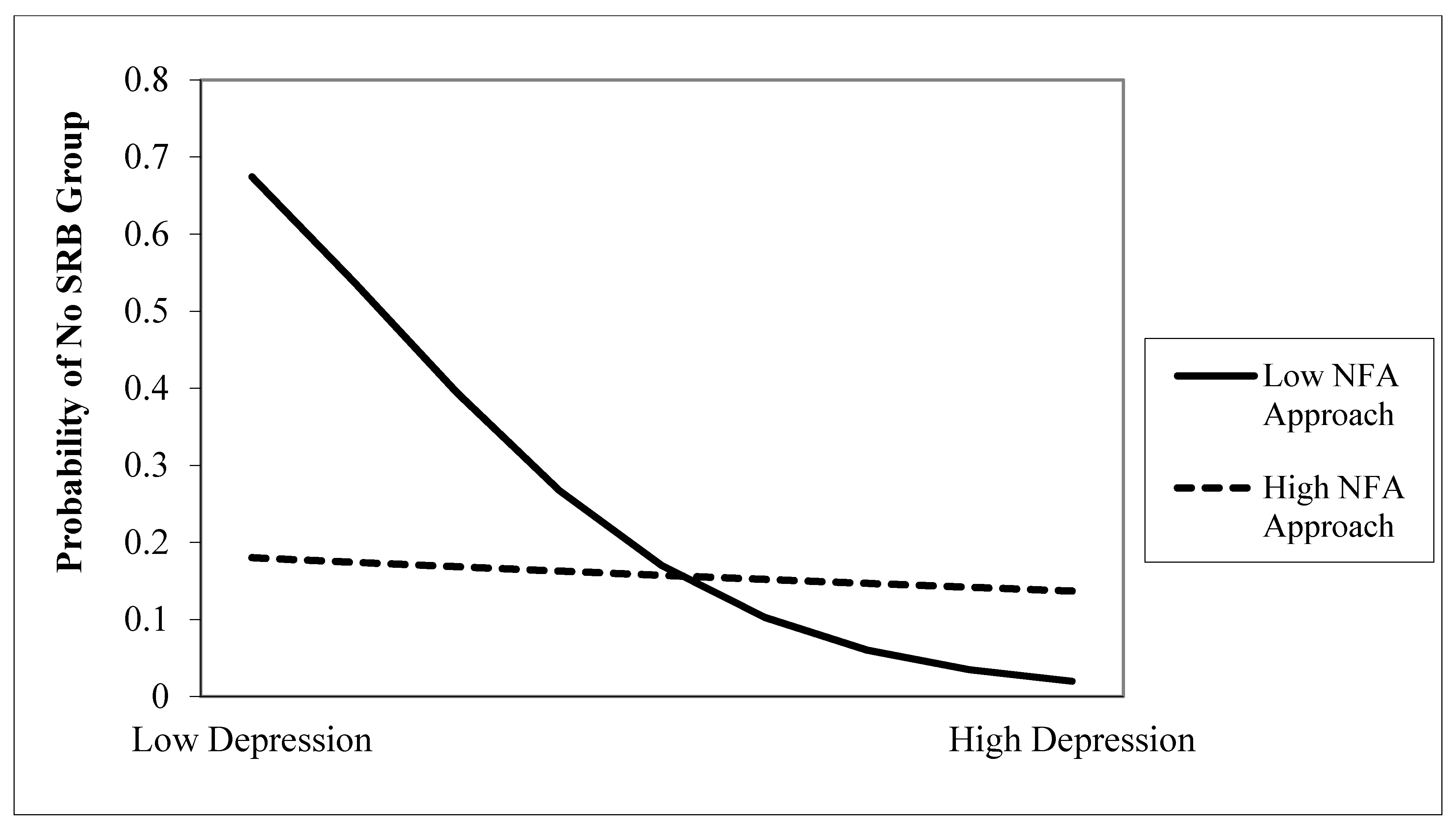
| Depression x Need for Affect Approach | 10.93 (2) | 0.004 |
| Depression x Need for Affect Avoidance | 1.06 (2) | 0.59 |
| Depression x Need for Cognition | 5.31 (2) | 0.07 |
| Need for Affect Approach x Need for Affect Avoidance | 1.16 (2) | 0.56 |
| Need for Affect Approach x Need for Cognition | 1.45 (2) | 0.48 |
| Need for Affect Avoidance x Need for Cognition | 1.30 (2) | 0.52 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cramer, R.J.; Langhinrichsen-Rohling, J.; Kaniuka, A.R.; Wilsey, C.N.; Mennicke, A.; Wright, S.; Montanaro, E.; Bowling, J.; Heron, K.E. Preferences in Information Processing, Marginalized Identity, and Non-Monogamy: Understanding Factors in Suicide-Related Behavior among Members of the Alternative Sexuality Community. Int. J. Environ. Res. Public Health 2020, 17, 3233. https://doi.org/10.3390/ijerph17093233
Cramer RJ, Langhinrichsen-Rohling J, Kaniuka AR, Wilsey CN, Mennicke A, Wright S, Montanaro E, Bowling J, Heron KE. Preferences in Information Processing, Marginalized Identity, and Non-Monogamy: Understanding Factors in Suicide-Related Behavior among Members of the Alternative Sexuality Community. International Journal of Environmental Research and Public Health. 2020; 17(9):3233. https://doi.org/10.3390/ijerph17093233
Chicago/Turabian StyleCramer, Robert J., Jennifer Langhinrichsen-Rohling, Andrea R. Kaniuka, Corrine N. Wilsey, Annelise Mennicke, Susan Wright, Erika Montanaro, Jessamyn Bowling, and Kristin E. Heron. 2020. "Preferences in Information Processing, Marginalized Identity, and Non-Monogamy: Understanding Factors in Suicide-Related Behavior among Members of the Alternative Sexuality Community" International Journal of Environmental Research and Public Health 17, no. 9: 3233. https://doi.org/10.3390/ijerph17093233