Combating the Epidemic of Obesity and Cardiovascular Disease: Perspectives from School-aged Children


{kind=link}
{kind=link}
{kind=link}
Abstract
:Introduction
Methods
- (1)
- “What do you think is keeping you or other students from eating more nutritious, healthier foods?”
- (2)
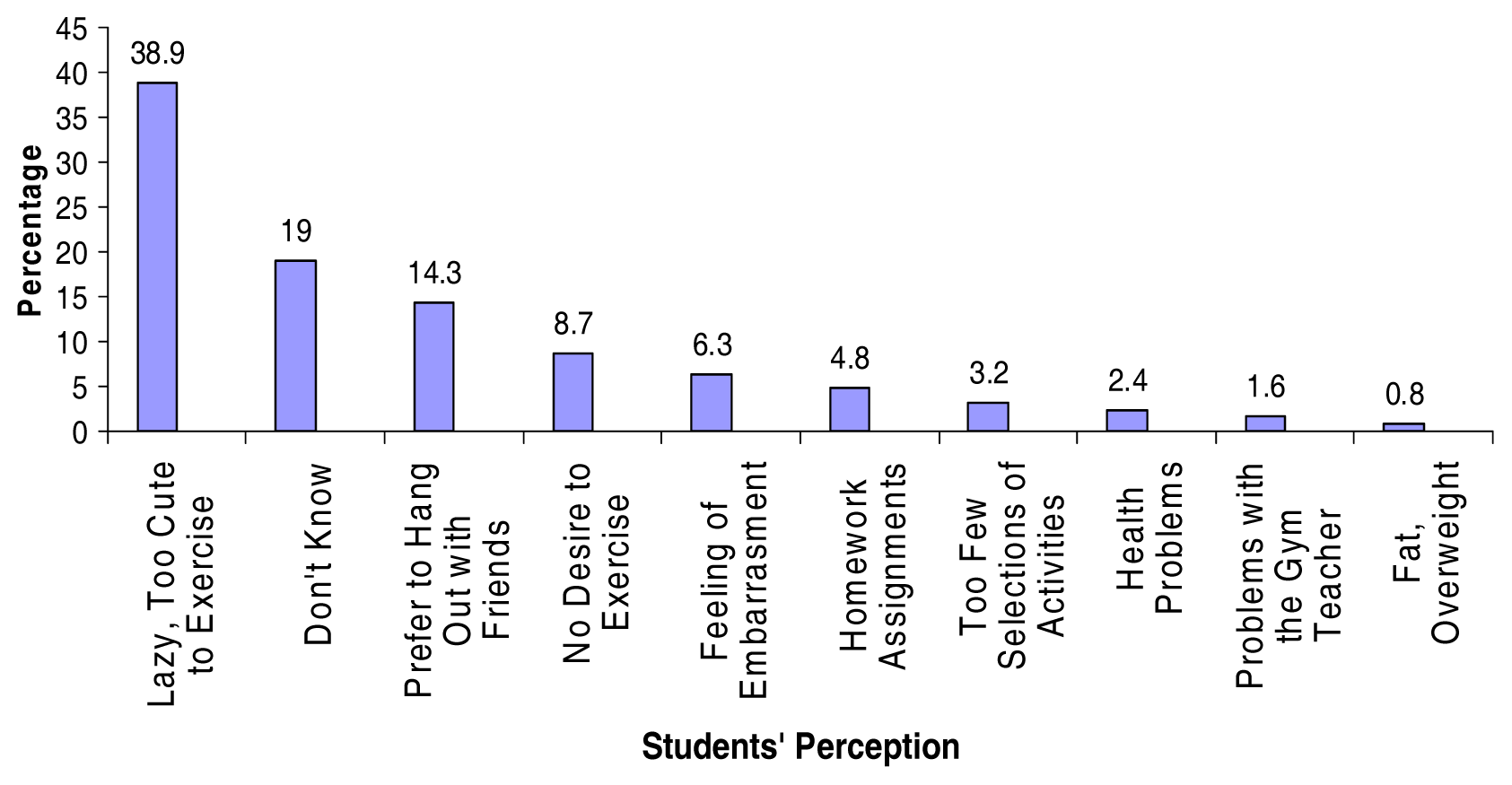
- “What do you think is preventing you or other students from taking part in daily physical activity?”
- (3)
- “What suggestions do you have that would help students to start eating better and exercising more?”
Statistical Analysis
Results
Limitations
Conclusion



Acknowledgements
References
- Lyznicki, J. M.; Young, D. C.; Riggs, J. A.; Davis, R. M. Obesity: assessment and management in primary care. Am Fam Physician 2001, 63, 2185–2196. [Google Scholar]
- Flegal, K. M.; Carroll, M. D.; Kuczmarski, R. J.; Johnson, C. L. Overweight and obesity in the United States: prevalence and trends, 1960–1994. Int J Obes Relat Metab Disord 1998, 22, 38–47. [Google Scholar]
- Mokdad, A. H.; Ford, E. S.; Bowman, B. A. Prevalence of obesity, diabetes, and obesity-related health risk factors. JAMA 2003, 289, 76–79. [Google Scholar]
- Ogden, C. L.; Flegal, K. M.; Carroll, M.; Johnson, C. L. Prevalence and trends in overweight among US children and adolescents, 1999–2000. JAMA 2002, 288, 1728–1732. [Google Scholar]
- Flegal, K. M.; Carroll, M. D.; Ogden, C. L.; Johnson, C. L. Prevalence and trends in obesity among US adults, 1999–2000. JAMA 2005, 288, 1723–1727. [Google Scholar]
- Serdula, M. K.; Dietz, W. H.; Bowman, B. A.; Marks, J. S.; Koplan, J. P. The spread of obesity epidemic in the United States, 1991–1998. JAMA 1999, 282, 1519–1522. [Google Scholar]
- Ogden, C. L.; Troiano, B. P.; Briefel, R. R.; Kuczmarski, R. J.; Flegal, M.; Johnson, C. L. Prevalence of overweight among preschool children in the United States. Pediatrics 1997, 99, 1e. [Google Scholar]
- Zhang, R.; Reisin, E. Obesity-hypertension: the effects on cardiovascular and renal systems. Am J Hypertens 2000, 13, 1308–1314. [Google Scholar]
- Melanson, K. J.; McInnis, K. J.; Rippe, J. M.; Blackburn, G.; Wilson, P. F. Obesity and cardiovascular disease risk: research update. Cardiol Rev 9 2001, 208–209. [Google Scholar]
- Sturm, R.; Wells, K. B. Does obesity contribute as much to morbidity as poverty or smoking? Public Health 2001, 115, 229–235. [Google Scholar]
- Calle, E.E.; Rodriquez, C.; Walker-Thurmond, K.; Thun, M.J. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med 2003, 348, 1625–1638. [Google Scholar]
- Brochu, P.; Poehlman, E. T.; Ades, P. A. Obesity, body fat distribution, and coronary artery disease. J Cardiopulm Rehabil 2005, 20, 96–108. [Google Scholar]
- Patrick, D.; Ushnell, D. M.; Rothman, K. Performance of two self-report measures for evaluating obesity and research. Obesity Research 2004, 12, 48–57. [Google Scholar]
- Must, A.; Strauss, R. S. Risks and consequences of childhood and adolescent obesity. Int J Obes Relat Metab Disord 1999, 23 Supplement 2, S2–S11. [Google Scholar]
- Erickson, S.; Robinson, T.; Haydel, F.; Killen, E. Are overweight children unhappy? Arch Pediatr Adolesc Med 2000, 154, 931–935. [Google Scholar]
- Wallace, W. J.; Sheslow, D.; Hessink, S. Obesity in children: a risk for depression. Williams, Kimm, C.L, SYS, Eds.; In Annals of the New York Academy of Science, 699: Prevention and Treatment of Childhood Obesity; The New York Academy of Sciences: New York, 1993; pp. 301–302. [Google Scholar]
- French, S. A.; Story, M.; Perry, C. L. Self-esteem and obesity in children and adolescents: a literature review. Obes Res 1995, 3, 479–490. [Google Scholar]
- Ackard, D. M.; Nuemark-Sztainer, D.; Story, M.; Perry, C. Overeating among adolescents: prevalence and association with weight-related characteristics and psychological health. Pediatrics 2003, 111, 67–74. [Google Scholar]
- Strauss, R. S. Childhood obesity and self-esteem. Pediatrics 2000, 1. [Google Scholar]
- Myers, M. D.; Raynor, H. A.; Epstein, L. H. Predictors of child psychological changes during family based treatment for obesity. Arch Pediatr Adolesc Med 1998, 152, 855–861. [Google Scholar]
- Stradmeyer, M.; Bosch, J.; Koops, W.; Seidel, J. Family functioning and psychosocial adjustment in overweight youngsters. Int J Eat Disord 2000, 27, 110–114. [Google Scholar]
- Braet, C.; Menvielde, I.; Vandercycken, W. Psychological aspects of childhood obesity: a controlled study in a clinical and non-clinical sample. J. Pediatr Psycho 1997, l 22, 59–71. [Google Scholar]
- Davison, K. K.; Birch, L. L. Weight status, parent reaction, and self-concept in five-year-old girls. Pediatrics 2001, 107, 46–53. [Google Scholar]
- Fuerst, D. R.; Rourke, B. P. Psychosocial functioning of children: relations between personality subtypes and academic achievement. J Abnorm Child Psychol 1993, 21, 597–607. [Google Scholar]
- Powell, C. L.; Arriola, K. Relationship between psychosocial factors and academic achievement among African American students. J Educ Res 2003, 96, 175–181. [Google Scholar]
- Livaditis, M.; Zaphriadis, K.; Samakouri, M.; Tellidou, C.; Tzawaras, N.; Xenitidis, K. Gender differences, family and psychological factors affecting school performance in Greek secondary school students. Educ Psychol 2003, 23, 223–231. [Google Scholar]
- Aluja, A.; Blanch, A. The Children’s Depression Inventory as predictor of social and scholastic competence. Eur J Psychol Assess 2002, 18, 259–274. [Google Scholar]
- McGee, R.; Prior, M.; Williams, S.; Smart, D.; Sanson, A. The long-term significance of teacher-rated hyperactivity and reading ability in childhood: findings from two longitudinal studies. J Child Psychol Psychiatry Allied Disciplines 2002, 43, 1004–1016. [Google Scholar]
- Falkner, N. H.; Neumark-Sztainer, D.; Story, M.; Jeffery, R. W.; Beuhring, T.; Resnick, M. D. Social, educational, and psychological correlates of weight status in adolescents. Obes Res 2001, 9, 32–42. [Google Scholar]
- McGinnis, J. M.; Foege, W. H. Actual causes of death in the United States [see comments]. JAMA 1993, 270(18), 2207–2212. [Google Scholar]
- Ng-Mak, D. S.; Dohrenwend, B. P.; Abraido-Lanza, A. F.; Turner, J. B. A further analysis of race differences in the National Longitudinal Mortality Study. Am J Public Health 1999, 89(11), 1748–1751. [Google Scholar]
- Gillum, R. F. Coronary heart disease, stroke, and hypertension in a U.S. national cohort: the NHANES I Epidemiologic Follow-up Study National Health and Nutrition Examination Survey. Ann Epidemiol 1996, 6(4), 259–262. [Google Scholar]
- National Heart Lung and BIood, Report of the working group on research in coronary heart disease in blacks; National Institutes of Health: Bethesda, Md, 1994; pp. 1–94.
- Harris, M. I.; Hadden, W. C.; Knowler, W. C.; Bennett, P. H. Prevalence of diabetes and impaired glucose tolerance and plasma glucose levels in U.S. population aged 20–74 yr. Diabetes 1987, 36(4), 523–534. [Google Scholar]
- Svec, F.; Nastasi, K.; Hilton, C.; Bao, W.; Srinivasan, S. R.; Berenson, G. S. Black-white contrasts in insulin levels during pubertal development. The Bogalusa Heart Study. Diabetes 1992, 41(3), 313–317. [Google Scholar]
- Sprafka, J. M.; Folsom, A. R.; Burke, G. L.; Edlavitch, S.A. Prevalence of cardiovascular disease risk factors in blacks and whites: the Minnesota Heart Survey. Am J Public Health 1988, 78(12), 1546–1549. [Google Scholar]
- Kuczmarski, R. J.; Flegal, K. M.; Campbell, S. M.; Johnson, C. L. Increasing prevalence of overweight among US adults. The National Health and Nutrition Examination Surveys, 1960 to 1991. JAMA 1994, 272(3), 205–211. [Google Scholar]
- Powell, K. E.; Thompson, P. D.; Caspersen, C. J.; Kendrick, J. S. Physical activity and the incidence of coronary heart disease. Annu Rev Public Health 1987, 8, 253–287. [Google Scholar]
- Clark, L. T.; Bellam, S. V.; Shah, A. H.; Feldman, J. G. Analysis of prehospital delay among inner-city patients with symptoms of myocardial infarction: implications for therapeutic intervention. J Natl Med Assoc 1992, 84(11), 931–937. [Google Scholar]
- Sempos, C. T.; Bild, D. E.; Manolio, T. A. Overview of the Jackson Heart Study: a study of cardiovascular diseases in African American men and women. Am J Med Sci 1999, 317(3), 142–146. [Google Scholar]
- Troiano, R. P.; Flegal, K. M.; Kuczmarski, R. J.; Campbell, S. M.; Johnson, C. L. Overweight prevalence and trends for children and adolescents. The National Health and Nutrition Examination Surveys, 1963 to 1991. Arch Pediatr Adolesc Med 1995, 149(10), 1085–1091. [Google Scholar]
- Lauer, R.M.; Connor, W.E.; Leaverton, P.E.; Reiter, M.A.; Clarke, W.R. Coronary heart disease risk factors in school children: the Muscatine study. J Pediatr 1975, 86(5), 697–706. [Google Scholar]
- Webber, L. S.; Osganian, V.; Leupker, R. V.; Feldman, H. A.; Stone, E. J.; Elder, J. P.; et al. Cardiovascular risk factors among third grade children in four regions of the United States. The CATCH Study. Child and Adolescent Trial for Cardiovascular Health. Am J Epidemiol 1995, 141(5), 428–439. [Google Scholar]
- National Heart Lung & Blood Institute, Report of the expert panel on blood cholesterol levels in children and adolescents; U.S. Department of Health and Human Services; NIH Publication no. 91-2732; Bethesda, MD, 1991.
- Berenson, G. S.; Epstein, F. A. Conference on blood lipids in children; optimal levels for early prevention of coronary artery disease. Workshop report; Epidemiological Section. Prev. Med 1983, 12, 741–797. [Google Scholar]
- Lewis, J. Obesity and lifestyle: After-school program encourages weight loss. Endocrine Today 2005. [Google Scholar]
© 2006 MDPI. All rights reserved.
Share and Cite
Addison, C.C.; White, M.S.; Jenkins, B.W.; Young, L. Combating the Epidemic of Obesity and Cardiovascular Disease: Perspectives from School-aged Children. Int. J. Environ. Res. Public Health 2006, 3, 268-273. https://doi.org/10.3390/ijerph2006030032
Addison CC, White MS, Jenkins BW, Young L. Combating the Epidemic of Obesity and Cardiovascular Disease: Perspectives from School-aged Children. International Journal of Environmental Research and Public Health. 2006; 3(3):268-273. https://doi.org/10.3390/ijerph2006030032
Chicago/Turabian StyleAddison, Clifton C., Monique S. White, Brenda W. Jenkins, and Lavon Young. 2006. "Combating the Epidemic of Obesity and Cardiovascular Disease: Perspectives from School-aged Children" International Journal of Environmental Research and Public Health 3, no. 3: 268-273. https://doi.org/10.3390/ijerph2006030032