Self-Medication Practices with Antibiotics among Tertiary Level Students in Accra, Ghana: A Cross-Sectional Study


Abstract
:1. Introduction
2. Methods
- prevalence of self medication with antibiotics
- association of self medication with gender and institution
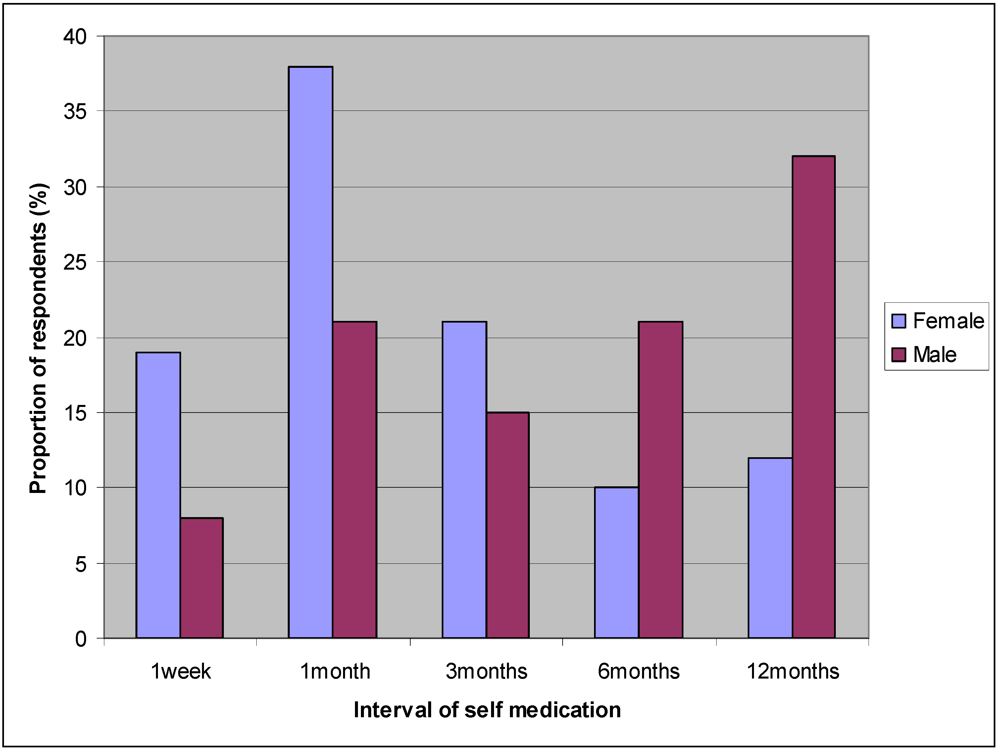
- frequency/rate of self medication
- major antibiotics used in self medication
- causal factors associated with self medication
- prevalence of treatment failures in self medication
- the extent of risk associated with self medication
3. Results

{kind=link}
| Institution | Type | Major courses offered * | Students sampled |
|---|---|---|---|
| Accra Polytechnic | State owned | Engineering, Sciences, Business | 100 |
| Central University | Private owned | Theology, Business, Arts | 200 |
| Methodist University | Private owned | Social studies, Arts, Business | 200 |
| Korle-Bu Medical Campus | State owned | Medicine, Nursing, Allied Health | 100 |
| Source | n | N | % | 95% CI |
|---|---|---|---|---|
| Gender (p = 0.08) | ||||
| Male students | 202 | 300 | 67 | 61.7–72.3 |
| Female students | 220 | 300 | 73 | 68.0–78.0 |
| Total | 422 | 600 | 70 | 66.3–73.7 |
| Institution (p < 0.001) | ||||
| Accra Polytechnic | 62 | 100 | 62 | 52.5–71.5 |
| Central University | 164 | 200 | 82 | 76.7–87.3 |
| Methodist University | 154 | 200 | 77 | 71.2–82.8 |
| Korle-Bu Medical Campus | 42 | 100 | 43 | 33.3–52.7 |
| Total | 422 | 600 | 70 | 66.3–73.7 |

| Parameter | n | % | 95% CI |
|---|---|---|---|
| Antibiotic type | |||
| Amoxacillin | 198 | 46.9 | 42.1–51.7 |
| Ampicillin | 191 | 45.3 | 40.6–50.1 |
| Penicillin | 124 | 29.4 | 25.1–33.8 |
| Gentamicin | 85 | 20.1 | 16.3–23.9 |
| Chloramphenicol | 63 | 14.9 | 11.5–18.3 |
| Streptomycin | 62 | 14.7 | 11.3–18.1 |
| Trimethoprim | 36 | 8.5 | 5.8–11.2 |
| Tetracycline | 36 | 8.5 | 5.8–11.2 |
| Cotrimoxazole | 13 | 3.1 | 1.5–4.8 |
| Erythromycin | 9 | 2.1 | 0.7–3.5 |
| Sulphonamide | 5 | 1.2 | 0.2–2.3 |
| Polymyxin | 4 | 0.9 | 0–1.8 |
| Vancomycin | 3 | 0.7 | 0.1–1.5 |
| Reasons for self medication | |||
| Less expensive | 171 | 40.5 | 35.8–45.2 |
| Long delays at clinics/hospitals | 171 | 40.5 | 35.8–45.3 |
| Application of previous prescription | 46 | 10.9 | 7.9–13.9 |
| Good knowledge of antibiotics | 34 | 8.1 | 5.5–10.7 |
| Antibiotics are easily obtained | 30 | 7.1 | 4.7–9.6 |
| Imitating others in drug usage | 4 | 0.9 | 0–1.8 |
| Hospital not accessible | 4 | 0.9 | 0–1.8 |
4. Discussion
5. Conclusions
Conflict of Interest
References
- Kunin, C.M. Problems of antibiotic usage: Definitions, causes and proposed solutions. Ann. Intern. Med. 1978, 89, 802–805. [Google Scholar]
- Nathwani, D.; Davey, P. Antibiotic prescribing-Are there lessons for physicians? Q. Med. J. 1992, 92, 287–292. [Google Scholar]
- Goossens, H.; Ferech, M.; Vander Stichele, R.; Elseviers, M. Outpatient antibiotic use in Europe and association with resistance: A cross-national database study. Lancet 2005, 365, 579–587. [Google Scholar]
- World Health Organization, Guidelines for the Regulatory Assessment of Medicinal Products for Use in Self-Medication; WHODEDM/QSM/001; WHO: Geneva, Switzerland, 2000.
- Skliros, E.; Merkouris, P.; Papazafiropoulou, A.; Gikas, A.; Matzouranis, G.; Papafragos, C.; Tsakanikas, I.; Zarbala, I.; Vasibosis, A.; Stamataki, P.; Sotiropoulos, A. Self-medication with antibiotics in rural population in Greece: A cross-sectional multicenter study. BMC Fam. Pract. 2010, 11. [Google Scholar] [CrossRef]
- Ebert, S.C. Factors contributing to excessive antimicrobial prescribing. Pharmacotherapy 2007, 27, 126–130. [Google Scholar] [CrossRef]
- Friedman, C.R.; Whitney, C.G. It’s time for a change in practice: Reducing antibiotic use can alter antibiotic resistance. J. Infect. Dis. 2008, 197, 1082–1083. [Google Scholar] [CrossRef]
- Vila, J.; Pal, T. Update on antibacterial resistance in low-income countries: Factors favouring the emergence of resistance. Open Infect. Dis. J. 2010, 4, 38–54. [Google Scholar] [CrossRef]
- Awad, A.; Eltayeb, I.; Matowe, L.; Thalib, L. Self-medication with antibiotics and antimalarials in the community of Khartoum State, Sudan. J. Pharm. Sci. 2005, 8, 326–331. [Google Scholar]
- Sapkota, A.R.; Coker, M.E.; Goldstein, R.E.R.; Atkinson, N.L.; Sweet, S.J.; Sopeju, P.O.; Ojo, M.T.; Otivhia, E.; Ayepola, O.O.; Olajuyigbe, O.O.; Shireman, L.; Pottinger, P.S.; Ojo, K.K. Self-medication with antibiotics for the treatment of menstrual symptoms in southwest Nigeria: A cross sectional study. BMC Public Health 2010, 10. [Google Scholar] [CrossRef]
- Sarahroodi, S.; Arzi, A.; Sawalha, A.F.; Ashtarinezhad, A. Antibiotics self-medication among southern Iranian university students. Int. J. Pharmacol. 2010, 6, 48–52. [Google Scholar] [CrossRef]
- Ehigiator, O.; Azodo, C.C.; Ehikhamenor, E.E. Self-medication with antibiotics among Nigerian Dental Students. Tanzan. Dent. J. 2010, 16, 48–54. [Google Scholar]
- Syed, N.Z.; Reema, S.; Sana, W.; Akbar, Z.; Talha, V.; Mehrine, S.; Wajeeha, Y.; Saman, S.; Sarah, S. Self-medication amongst university students of Karachi: Prevalence, knowledge and attitudes. J. Pak. Med. Assoc. 2008, 58, 214–217. [Google Scholar]
- Fadare, J.O.; Tamuno, I. Antibiotic self-medication among university medical undergraduates in Northern Nigeria. J. Public Health Epidemiol. 2011, 3, 217–220. [Google Scholar]
- Olayemi, O.J.; Olayinka, B.O.; Musa, A.I. Evaluation of antibiotic self-medication pattern amongst undergraduate students of Ahmadu Bello University (Main Campus), Zaria. Res. J. Appl. Sci. Eng. Technol. 2010, 2, 35–38. [Google Scholar]
- Awad, A.I.; Eltayeb, I.B. Self-medication practices with antibiotics and antimalarials among Sudanese undergraduate university students. Ann. Pharmacother. 2007, 41, 1249–1255. [Google Scholar] [CrossRef]
- Yasmin, S.M.; Ashraf, J.; Tahira, M.; Shahla, Z.; Adnan, S. Self medication among university students of Karachi. JLUMHS 2011, 10, 102–105. [Google Scholar]
- Van den Boom, G.J.M.; Nsowah-Nuamah, N.N.N.; Overbosch, G.B. Healthcare Provision and Self-Medication in Ghana. Available online: http://web.archive.org/web/20070625163825/ http://www.saga.cornell.edu/images/vandenboom.pdf (accessed on 29 June 2012).
- Adu-Sarkodie, Y.A. Antimicrobial self medication in patients attending a sexually transmitted diseases clinic. Int. J. STD AIDS 1997, 8, 456–458. [Google Scholar] [CrossRef]
- Donkor, E.S.; Nartey, E. Nasal colonisation of drug resistant bacteria in Ghanaian children less than five years. Internet J. Microbiol. 2008, 5. [Google Scholar] [CrossRef]
- Edoh, D.; Alomatu, B. Comparison of antibiotic resistance patterns between laboratories in Accra east Ghana. Niger. Ann. Nat. Sci. 2008, 8, 10–18. [Google Scholar]
- Newman, M.J.; Frimpong, E.; Donkor, E.S.; Opintan, J.A.; Asamoah-Adu, A. Resistance to antimicrobial drugs in Ghana. Infect. Drug Resist. 2011, 4, 215–220. [Google Scholar]
- Ghana Statistical Service. 2010 Population and Housing Census. Provisional Results. 2010. Available online: http://www.ghana.gov.gh/census/phc2010.pdf (accessed on 29 June 2012).
- Owusu-Daak, F.T.; Marfo, A.F.A.; Boateng, E.A. The contribution of Ghanaian pharmacists to mental health care: Current practice and barriers. Int. J. Ment. Health Syst. 2010, 4. [Google Scholar] [CrossRef]
- Daniel, W.W. Biostatistics: A Foundation for Analysis in the Health Sciences; John Wiley & Sons, Inc.: New York, NY, USA, 1998. [Google Scholar]
- Naing, L.; Winn, T.; Rusli, B.N. Practical issues in calculating the sample size for prevalence studies. Arch. Orofac. Sci. 2006, 1, 9–14. [Google Scholar]
- Pannucci, C.J.; Wilkins, E.G. Identifying and avoiding bias in research. Plast Reconstr. Surg. 2010, 126, 619–625. [Google Scholar] [CrossRef]
- Buke, C.; Hosgor-Limoncu, M.; Ermertcan, S.; Ciceklioglu, M.; Tuncel, M.; Kose, T.; Eren, S. Irrational use of antibiotics among university students. J. Infect. 2005, 51, 135–139. [Google Scholar] [CrossRef]
- Al-Bakri, A.G.; Bustanji, Y.; Yousef, A.M. Community consumption of antibacterial drugs within the Jordanian population: Sources, patterns and appropriateness. Int. J. Antimicrob. Agents 2005, 26, 389–395. [Google Scholar] [CrossRef]
- Muscat, M.; Monnet, D.L.; Klemmensen, T.; Grigoryan, L.; Jensen, M.H.; Andersen, M.; Haaijer-Ruskamp, F.M. Patterns of antibiotic use in the community in Denmark. Scand. J. Infect. Dis. 2006, 38, 597–603. [Google Scholar] [CrossRef]
- Väänänen, M.H.; Pietilä, K.; Airaksinen, M. Self-medication with antibiotics-Does it really happen in Europe? Health Policy 2006, 77, 166–171. [Google Scholar] [CrossRef]
- Borg, M.A.; Scicluna, E.A. Over-the-counter acquisition of antimicrobial drugs in the Maltese general population. Int. J. Antimicrob. Agents 2002, 20, 253–257. [Google Scholar] [CrossRef]
- Berzanskyte, A.; Valinteliene, R.; Haaijer-Ruskamp, F.M.; Gurevicius, R.; Grigoryan, L. Self-medication with antibiotics in Lithuania. Int. J. Occup. Med. Environ. Health 2006, 19, 246–253. [Google Scholar] [CrossRef]
- López, J.J.; Dennis, R.; Moscoso, S.M. A study of self-medication in a neighborhood in Bogotá. Rev. Salud. Publica (Bogota) 2009, 11, 432–442. [Google Scholar]
- Harbarth, S.; Samore, M.H. Antimicrobial resistance determinants and future control. Emerg. Infect. Dis. 2005, 11, 794–801. [Google Scholar] [CrossRef]
- Bavestrello, L.; Cabello, A.; Casanova, D. Impact of regulatory measures in the trends of community consumption of antibiotics in Chile. Rev. Med. Chil. 2002, 130, 1265–1272. [Google Scholar]
- Macfarlane, J.; Holmes, W.; Macfarlane, R.; Britten, N. Influence of patients’ expectations on antibiotic management of acute lower respiratory tract illness in general practice: Questionnaire study. BMJ 1997, 315, 1211–1214. [Google Scholar]
- Reeves, D. The 2005 Garrod lecture: The changing access of patients to antibiotics-For better or worse? J. Antimicrob. Chemother. 2007, 59, 333–341. [Google Scholar] [CrossRef]
- Lee, P.R.; Lurie, P.; Silverman, M.M.; Lydecker, M. Drug labelling and promotion in the developing countries: An update. J. Clin. Epidemiol. 1991, 44, 49–55. [Google Scholar]
- Donkor, E.S.; Newman, M.J.; Yeboah-Manu, D. Epidemiological aspects of non-human antibiotic usage and resistance: Implications for the control of antibiotic resistance in Ghana. Trop. Med. Int. Health 2012, in press. [Google Scholar]
- Bonsu, W.K.; Ofori-Adjei, D. An audit of prescribing practice in health care facilities of the Wassa west district of Ghana. West Afr. J. Med. 2000, 19, 298–303. [Google Scholar]
- Donkor, E.S.; Nortey, T.; Opintan, J.A.; Dayie, N.; Akyeh, M.L. Antimicrobial susceptibility of Salmonella typhi and Staphylococcus aureus and the effect of some media on susceptibility testing results. Internet J. Microbiol. 2008, 4, 1–5. [Google Scholar]
- Donkor, E.S.; Newman, M.J.; Oliver-Commey, J.; Bannerman, E.; Dayie, N.T.K.D.; Badoe, E.V. Invasive disease and paediatric carriage of Streptococcus pneumoniae in Ghana. Scand. J. Infect. Dis. 2010, 42, 254–259. [Google Scholar] [CrossRef]
- Opintan, J.A.; Newman, M.J. Distribution of serogroups and serotypes of multiple drug resistant Shigella isolates. Ghana Med. J. 2007, 41, 50–54. [Google Scholar]
- Enweronu-Laryea, C.C.; Newman, M.J. Changing pattern of bacterial isolates and antimicrobial susceptibility in neonatal infections in Korle Bu Teaching Hospital, Ghana. East Afr. Med. J. 2007, 84, 136–140. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Donkor, E.S.; Tetteh-Quarcoo, P.B.; Nartey, P.; Agyeman, I.O. Self-Medication Practices with Antibiotics among Tertiary Level Students in Accra, Ghana: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2012, 9, 3519-3529. https://doi.org/10.3390/ijerph9103519
Donkor ES, Tetteh-Quarcoo PB, Nartey P, Agyeman IO. Self-Medication Practices with Antibiotics among Tertiary Level Students in Accra, Ghana: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2012; 9(10):3519-3529. https://doi.org/10.3390/ijerph9103519
Chicago/Turabian StyleDonkor, Eric S., Patience B. Tetteh-Quarcoo, Patrick Nartey, and Isaac O. Agyeman. 2012. "Self-Medication Practices with Antibiotics among Tertiary Level Students in Accra, Ghana: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 9, no. 10: 3519-3529. https://doi.org/10.3390/ijerph9103519