Comparison of Locoregional Recurrence with Mastectomy vs. Breast Conserving Surgery in Pregnancy Associated Breast Cancer (PABC)

Abstract
:1. Introduction
2. Materials and Methods
3. Results

{kind=link}
| Mastectomy N = 33 Mean (SD) /N(%) | BCT N = 27 Mean (SD) /N(%) | P Value | |
|---|---|---|---|
| Age, years | |||
| Mean (SD) | 35.61 | 33.15 | 0.04 |
| Range | 24–42 | 24–44 | |
| Race | |||
| Caucasian | 31 (93.9) | 26 (96.3) | 0.65 |
| Afro American | 1 (3.1) | 1 (3.7) | |
| Other | 1 (3.1) | 0 (0.0) | |
| Pregnancy Timing | |||
| Antepartum | 15 (45.5) | 16 (59.3) | 0.312 |
| Post partum | 18 (54.5) | 11 (40.7) | |
| Family History | |||
| Positive | 15 (45.5) | 15 (55.6) | 0.031 |
| Negative | 11 (33.3) | 12 (44.4) | |
| Unknown | 7 (21.2) | 0 (0.0) |
| Mastectomy N = 33 N (%) | BCT N = 27 N (%) | P Value | |
|---|---|---|---|
| BRCA1/2 Mutation | |||
| Positive | 3 (37.5) | 4 (50.0) | 0.7 |
| Negative | 5 (62.5) | 4 (50.0) | |
| ER | |||
| Negative | 16 (48.5) | 10 (37.0) | 0.395 |
| Positive | 7 (21.2) | 10 (37.0) | |
| Unknown | 10 (30.3) | 7 (25.9) | |
| Nottingham Grade | |||
| 1 | 0 (0.0) | 1 (3.7) | 0.05 |
| 2 | 1 (3.0) | 7 (25.9) | |
| 3 | 23 (69.7) | 12 (44.4) | |
| Unknown | 7 (21.2) | 7 (25.9) | |
| LVSI | |||
| Absent | 13 (39.4) | 13 (48.1) | 0.720 |
| Present | 16 (48.5) | 10 (37.0) | |
| Unknown | 4 (12.1) | 4 (14.8) |
| Mastectomy N = 33 Mean (SD) /N(%) | BCT N = 27 Mean (SD) /N(%) | P Value | |
|---|---|---|---|
| Chemotherapy | |||
| No | 7 (21.2) | 2 (7.4) | 0.166 |
| Yes | 26 (78.8) | 25 (92.6) | |
| Neo-Adjuvant Chemotherapy | |||
| Yes | 13 (0.50) | 18 (0.72) | 0.08 |
| No | 13 (0.50) | 7 (0.28) | |
| Type of LN Surgery | |||
| ALND | 23 (69.7) | 19 (70.4) | 0.967 |
| SLND | 8 (24.2) | 6 (22.2) | |
| SLND plus ALND | 2 (6.1) | 2 (2.4) |
| Mastectomy N = 33 | BCT N = 27 | P Value | |
|---|---|---|---|
| Pathological LN Status | |||
| Positive | 15 (51.7) | 14 (51.9) | 0.622 |
| Negative | 14 (48.3) | 13 (48.1) | |
| No. Nodes Dissected | |||
| Mean | 12.0 (6.5) | 15.3 (8.4) | 0.099 |
| Median | 13 | 15 | |
| Range | 1–30 | 2–31 | |
| No. Nodes Positive | |||
| Mean | 3.6 (5.5) | 0 (1.8) | 0.015 |
| Median | 1 | 0 | |
| Range | 0–17 | 0–9 | |
| T Stage | |||
| Tis | 2 (6.1) | 0 (0.0) | 0.006 |
| T1 | 6 (18.2) | 13 (48.1) | |
| T2 | 11 (33.3) | 14 (51.9) | |
| T3 | 8 (24.2) | 0 (0.0) | |
| T4 | 3 (9.1) | 0 (0.0) | |
| Tx | 3 (9.1) | 0 (0.0) | |
| AJCC Stage | |||
| 0 | 2 (6.1) | 0 (0.0) | 0.077 |
| I | 3 (9.1) | 3 (11.1) | |
| IIA | 10 (30.3) | 15 (55.6) | |
| IIB | 4 (12.1) | 5 (18.5) | |
| IIIA | 8 (24.2) | 4 (14.8) | |
| IIIC | 6 (18.2) | 0 (0.0) | |
| Stage Grouping | |||
| 0 | 2 (6.1) | 0 (0.0) | 0.044 |
| 1 | 3 (9.1) | 3 (11.1) | |
| 2 | 17 (42.4) | 22 (74.1) | |
| 3 | 17 (42.4) | 2 (14.8) | |
| Follow up | |||
| Mean (Months) | 51.3 | 61 | 0.401 |
| Range | 2–194 | 9.7–164 |
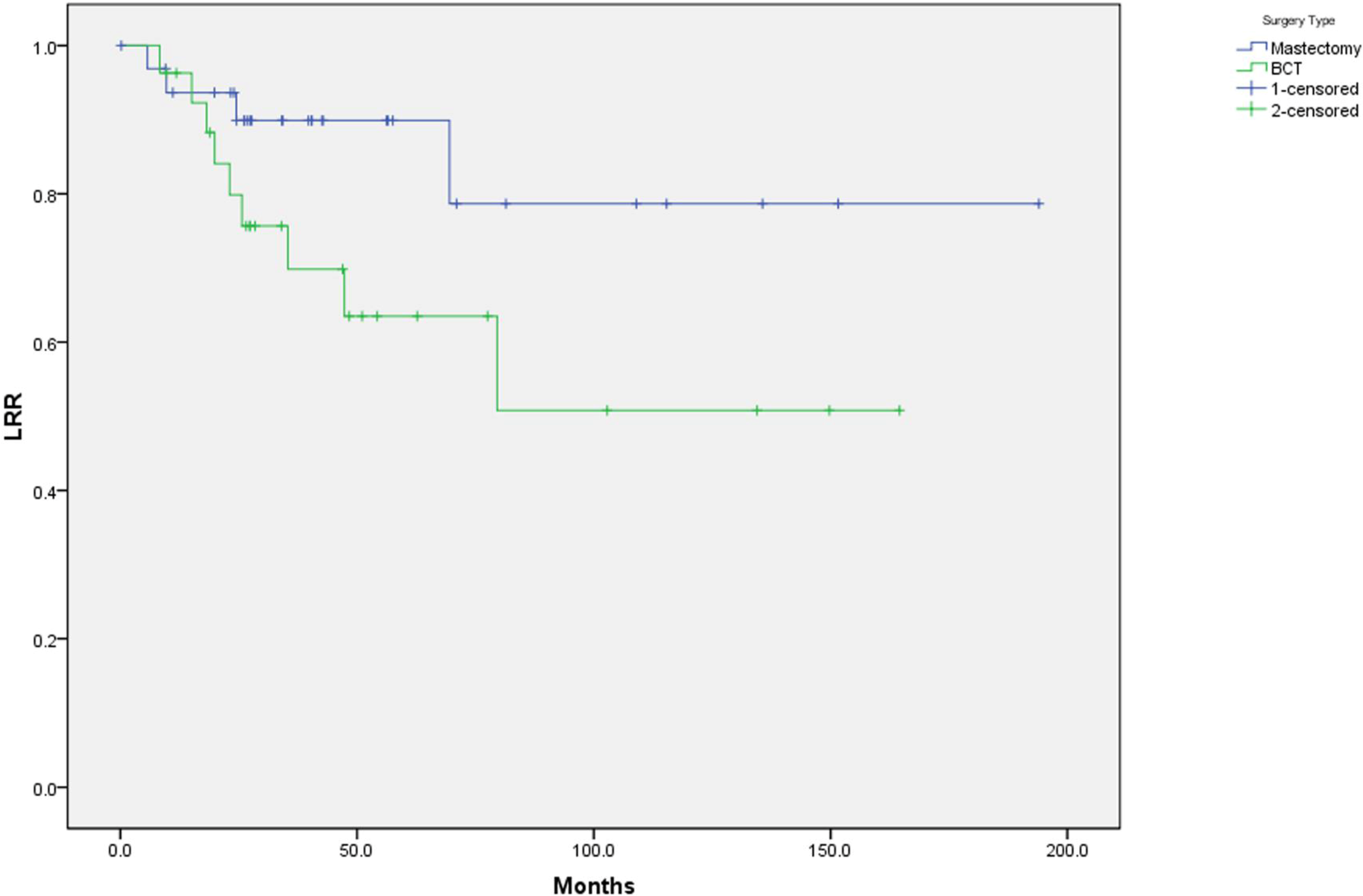
| 5 yrs (actuarial) | Group 1 % N = 33 (%) | Group 2 % N = 27 (%) | P value |
|---|---|---|---|
| Locoregional Recurrence | 10 | 37 | 0.04 |
| Distant Mets Free | 73 | 81 | 0.68 |
| Disease Free Survival | 60 | 71 | 0.52 |
| Overall Survival | 57 | 59 | 0.85 |

4. Conclusions
References
- Ives, A.D.; Saunders, C.M.; Semmens, J.B. The Western Australian gestational breast cancer project: A population-based study of the incidence, management and outcomes. Breast J. 2005, 14, 276–282. [Google Scholar] [CrossRef]
- Parente, J.T.; Amsel, M.; Lerner, R.; Chinea, F. Breast cancer associated with pregnancy. Obstet. Gynecol. 1988, 71, 861–864. [Google Scholar]
- Bernik, S.F.; Bernik, T.R.; Whooley, B.P.; Wallack, M.K. Carcinoma of the breast during pregnancy: a review and update on treatment options. Surg. Oncol. 1999, 7, 45–49. [Google Scholar]
- Haagensen, C.; Stout, A. Carcinoma of the breast. Ann. Surg. 1943, 118, 859–870. [Google Scholar]
- Loibl, S.; von Minckwitz, G.; Gwyn, K.; Ellis, P.; Blohmer, J.U.; Schlegelberger, B.; Keller, M.; Harder, S.; Theriault, R.L.; Crivellari, D.; Klingebiel, T.; Louwen, F.; Kaufmann, M. Breast carcinoma during pregnancy. International recommendations from an expert meeting. Cancer 2006, 106, 237–246. [Google Scholar] [CrossRef]
- Zemlickis, D.; Lishner, M.; Degendorfer, P.; Panzarella, T; Burke, B.; Sutcliffe, S.B.; Koren, G. Maternal and fetal outcome after breast cancer in pregnancy. Am. J. Obstet. Gynecol. 1992, 166, 781–787. [Google Scholar] [CrossRef]
- Ezzat, A.; Raja, M.A.; Berry, J.; Zwaan, F.E.; Jamshed, A.; Rhydderch, D.; Rostom, A.; Bazarbashi, S. Impact of pregnancy of nonmetastatic breast cancer: a case control study. Clin. Oncol. 1996, 8, 367–370. [Google Scholar] [CrossRef]
- Beadle, B.M.; Woodward, W.A.; Middleton, L.P.; Tereffe, W.; Strom, E.A.; Litton, J.K.; Meric-Bernstam, F.; Theriault, R.L.; Buchholz, T.A.; Perkins, G.H. The impact of pregnancy on breast cancer outcomes in women </ = 35 years. Cancer 2009, 115, 1174–1184. [Google Scholar] [CrossRef]
- Kuerer, H.M.; Gwyn, K.; Ames, F.C.; Theriault, R.L. Conservative surgery and chemotherapy for breast carcinoma during pregnancy. Surgery 2008, 131, 108–110. [Google Scholar]
- Kuerer, H.M.; Cunningham, J.D.; Bleiweiss, I.J.; Doucette, J.T.; Divino, C.M.; Brower, S.T.; Tartter, P.I. Conservative surgery for breast carcinoma associated with pregnancy. Breast J. 1998, 4, 171–176. [Google Scholar]
- Kurtz, J.M.; Spitalier, J.M.; Amalric, R.; Brandone, H.; Ayme, Y.; Bressac, C.; Hans, D. Mammary recurrences in women younger than forty. Int. J. Radiat. Oncol. Biol. Phys. 1988, 15, 271–276. [Google Scholar] [CrossRef]
- Recht, A.; Connolly, J.L.; Schnitt, S.J.; Silver, B.; Rose, M.A.; Love, S.; Harris, J.R. The effect of young age on tumor recurrence in the treated breast after conservative surgery and radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 1988, 14, 3–10. [Google Scholar] [CrossRef]
- Kurtz, J.M.; Jacquemier, J.; Amalric, R.; Brandone, H.; Ayme, Y.; Hans, D.; Bressac, C.; Spitalier, J.M. Why are local recurrences after breast-conserving therapy more frequent in younger patients? J. Clin. Oncol. 1990, 8, 591–598. [Google Scholar]
- de la Rochefordiere, A.; Asselain, B.; Campana, F.; Scholl, S.M.; Fenton, J.; Vilcoq, J.R.; Durand, J.C.; Pouillart, P.; Magdelenat, H.; Fourquet, A. Age as prognostic factor in premenopausal breast carcinoma. Lancet 1993, 341, 1039–1043. [Google Scholar] [CrossRef]
- Kim, S.H.; Simkovich-Heerdt, A.; Tran, K.N.; Maclean, B.; Borgen, P.I. Women 35 years of age or younger have higher locoregional relapse rates after undergoing breast conservation therapy. J. Am. Coll. Surg. 1998, 187, 1–8. [Google Scholar] [CrossRef]
- Coulombe, G.; Tyldesley, S.; Speers, C.; Paltiel, C.; Aquino-Parsons, C.; Bernstein, V.; Truong, P.T.; Keyes, M.; Olivotto, I.A. Is mastectomy superior to breast-conserving treatment for young women? Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 1282–1290. [Google Scholar] [CrossRef]
- Albain, K.S.; Allred, D.C.; Clark, G.M. Breast cancer outcome and predictors of outcome: Are there age differentials? J. Natl. Cancer. Inst. Monogr. 1994, 16, 35–42. [Google Scholar]
- Elkhuizen, P.H.; van de Vijver, M.J.; Hermans, J.; Zonderland, H.M.; van de Velde, C.J.; Leer, J.W. Local recurrence after breast-conserving therapy for invasive breast cancer: High incidence in young patients and association with poor survival. Int. J. Radiat. Oncol. Biol. Phys. 1998, 40, 859–867. [Google Scholar] [CrossRef]
- de Bock, G.H.; van der Hage, J.A.; Putter, H.; Bonnema, J.; Bartelink, H.; van de Velde, C.J. Isolated loco-regional recurrence of breast cancer is more common n young patients and following breast conserving therapy: Long-term results of European Organisation for Research and Treatment of Cancer studies. Eur. J. Cancer 2006, 41, 351–356. [Google Scholar]
- Beadle, B.M.; Woodward, W.A.; Tucker, S.L.; Outlaw, E.D.; Allen, P.K.; Oh, J.L.; Strom, E.A.; Perkins, G.H.; Tereffe, W.; Yu, T.K.; Meric-Bernstam, F.; Litton, J.K.; Buchholz, T.A. Ten-year recurrence rates in young women with breast cancer by locoregional treatment approach. Int. J. Radiat. Oncol. Biol. Phys. 2009, 72, 734–744. [Google Scholar]
- Nixon, A.J.; Neuberg, D.; Hayes, D.F.; Gelman, R.; Connolly, J.L.; Schnitt, S.; Abner, A.; Recht, A.; Vicini, F.; Harris, J.R. Relationship of patient age to pathologic features of the tumor and prognosis for patients with stage I or II breast cancer. J. Clin. Oncol. 1994, 12, 888–894. [Google Scholar]
- Middleton, L.; Amin, M.; Gwyn, K.; Theriault, R.; Sahin, A. Breast carcinoma in pregnant women—Assessment of clinicopathologic and immunohistochemical features. Cancer 2003, 98, 1055–1060. [Google Scholar] [CrossRef]
- Carey, L.A.; Dees, E.C.; Sawyer, L.; Gatti, L.; Moore, D.T.; Collichio, F.; Ollila, D.W.; Sartor, C.I.; Graham, M.L.; Perou, C.M. The triple negative paradox: Primary tumor chemosensitivity of breast cancer subtypes. Clin. Cancer. Res. 2007, 13, 3239–3234. [Google Scholar]
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Beriwal, S.; Rungruang, B.; Soran, A.; Thull, D.; Kelley, J.L.; Bhargava, R.; Lin, C.J.; Sukumvanich, P. Comparison of Locoregional Recurrence with Mastectomy vs. Breast Conserving Surgery in Pregnancy Associated Breast Cancer (PABC). Cancers 2009, 1, 12-20. https://doi.org/10.3390/cancers1010012
Beriwal S, Rungruang B, Soran A, Thull D, Kelley JL, Bhargava R, Lin CJ, Sukumvanich P. Comparison of Locoregional Recurrence with Mastectomy vs. Breast Conserving Surgery in Pregnancy Associated Breast Cancer (PABC). Cancers. 2009; 1(1):12-20. https://doi.org/10.3390/cancers1010012
Chicago/Turabian StyleBeriwal, Sushil, Bunja Rungruang, Atilla Soran, Darcy Thull, Joseph L. Kelley, Rohit Bhargava, Chyongchiou J. Lin, and Paniti Sukumvanich. 2009. "Comparison of Locoregional Recurrence with Mastectomy vs. Breast Conserving Surgery in Pregnancy Associated Breast Cancer (PABC)" Cancers 1, no. 1: 12-20. https://doi.org/10.3390/cancers1010012