Identification of Serum Biomarkers for Biliary Tract Cancers by a Proteomic Approach Based on Time-of-Flight Mass Spectrometry

Abstract
:1. Introduction
2. Material and Methods
2.1. Subjects and Samples
2.2. Randomized Selection of the Test Sets
2.3. Immobilized Metal Affinity Capture (IMAC30) ProteinChip Assay and SELDI-TOF-MS Analysis
2.4. Decision tree Classification and Model Assessment
2.5. Test Set Sample Classification
2.6. Assessment of the Reproducibility of SELDI Spectra
2.7. Statistical Analysis
3. Results
3.1. Characteristics of Subjects

{kind=link}
{kind=link}
| Subjects (%) | Males(%) | Females(%) | Age range (years) | Mean age(years) | Training set (%) | Blind set (%) | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| BTCs | 50 | 15 | 35 | 42–75 | 64.6 | 30 | 20 | |||
| Tumor site | ||||||||||
| Gallbladder | 32 (64.0) | 8(53.3) | 24(68.6) | 43–72 | 63.9 | 19(63.3) | 13(65.0) | |||
| Extrahepatic bile ducts | 13 (26.0) | 4(26.7) | 9(25.7) | 42–74 | 64.8 | 8(26.7) | 5(25.0) | |||
| Ampulla of Vater | 5 (10.0) | 3(20.0) | 2(5.7) | 62–75 | 68.2 | 3(10.0) | 2(10.0) | |||
| P for χ2 test = 0.99 | ||||||||||
| Clinicopathological stage | ||||||||||
| Stage 0–I | 8 (16.0) | 4(26.7) | 4(11.4) | 53–74 | 65.2 | 7(23.3) | 1(5.0) | |||
| Stage II | 11(22.0) | 5(33.3) | 6(17.1) | 43–75 | 66.3 | 8(26.7) | 3(15.0) | |||
| Stage III | 12(24.0) | 0(0.0) | 12(34.3) | 47–70 | 62.9 | 7(23.3) | 5(25.0) | |||
| Stage IV | 18(36.0) | 6(40.0) | 12(34.3) | 42–73 | 63.9 | 7(23.3) | 11(55.0) | |||
| Unknown | 1(2.0) | 0(0.0) | 1(2.9) | -- | 74.1 | 1(3.3) | 0 (0.0) | |||
| P for χ2 test = 0.09 | ||||||||||
| Gallstone | ||||||||||
| With | 33(66.0) | 7(46.7) | 26(74.3) | 42–74 | 63.5 | 20(66.7) | 13(65.0) | |||
| Without | 17(34.0) | 8(53.3) | 9(25.7) | 43–75 | 63.5 | 10(33.3) | 7(35.0) | |||
| P for χ2 test = 0.90 | ||||||||||
| Cholestasis | ||||||||||
| With | 13(26.0) | 2(13.3) | 11(31.4) | 47–74 | 64.8 | 11(36.7) | 2(10.0) | |||
| Without | 37(74.0) | 13(86.7) | 24(68.6) | 42–75 | 63.7 | 19(63.3) | 18(90.0) | |||
| P for χ2 test = 0.04 | ||||||||||
| Controls | 60 | 21 | 39 | 35–74 | 59.9 | 40 | 20 | |||
| Cholelithiasis subjects | 30(50.0) | 10(47.6) | 20(51.3) | 43–72 | 58.3 | 20 (50.0) | 10(50.0) | |||
| Healthy subjects | 30(50.0) | 11(52.4) | 19(48.7) | 35–74 | 61.6 | 20(50.0) | 10(50.0) | |||
| P for χ2 test = 1.00 | ||||||||||
3.2. SELDI-TOF-MS Data Analysis

| m/z | P value | Cases (N = 30) | Controls (N = 40) | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| 2,170 | 4.23E−05 | 0.78 | 1.14 | 2.87 | 2.72 | |
| 2,967 | 7.93E−07 | 1.80 | 2.37 | 4.93 | 3.01 | |
| 3,300 | 0.0016 | 1.91 | 1.38 | 3.14 | 1.81 | |
| 3,400 | 1.56E−07 | 1.61 | 2.49 | 4.09 | 2.03 | |
| 4,188 | 0.0059 | 1.55 | 1.26 | 3.81 | 4.64 | |
| 4,503 | 2.19E−06 | 4.01 | 4.50 | 9.72 | 3.57 | |
| 4,906 | 8.99E−05 | 0.07 | 0.32 | 0.59 | 0.84 | |
| 5,630 | 0.000969425 | 1.73 | 1.55 | 0.95 | 0.83 | |
| 5,681 | 0.000132676 | 10.70 | 9.24 | 4.46 | 4.75 | |
| 7,598 | 0.0009 | 23.03 | 10.82 | 32.62 | 10.45 | |
| 7,797 | 0.0035 | 3.54 | 1.47 | 4.73 | 1.53 | |
| 10,875 | 0.006116577 | 0.27 | 0.35 | 0.09 | 0.13 | |
| 11,167 | 0.004078681 | 0.60 | 0.90 | 0.13 | 0.28 | |
| 11,242 | 0.002574666 | 0.89 | 1.27 | 0.25 | 0.41 | |
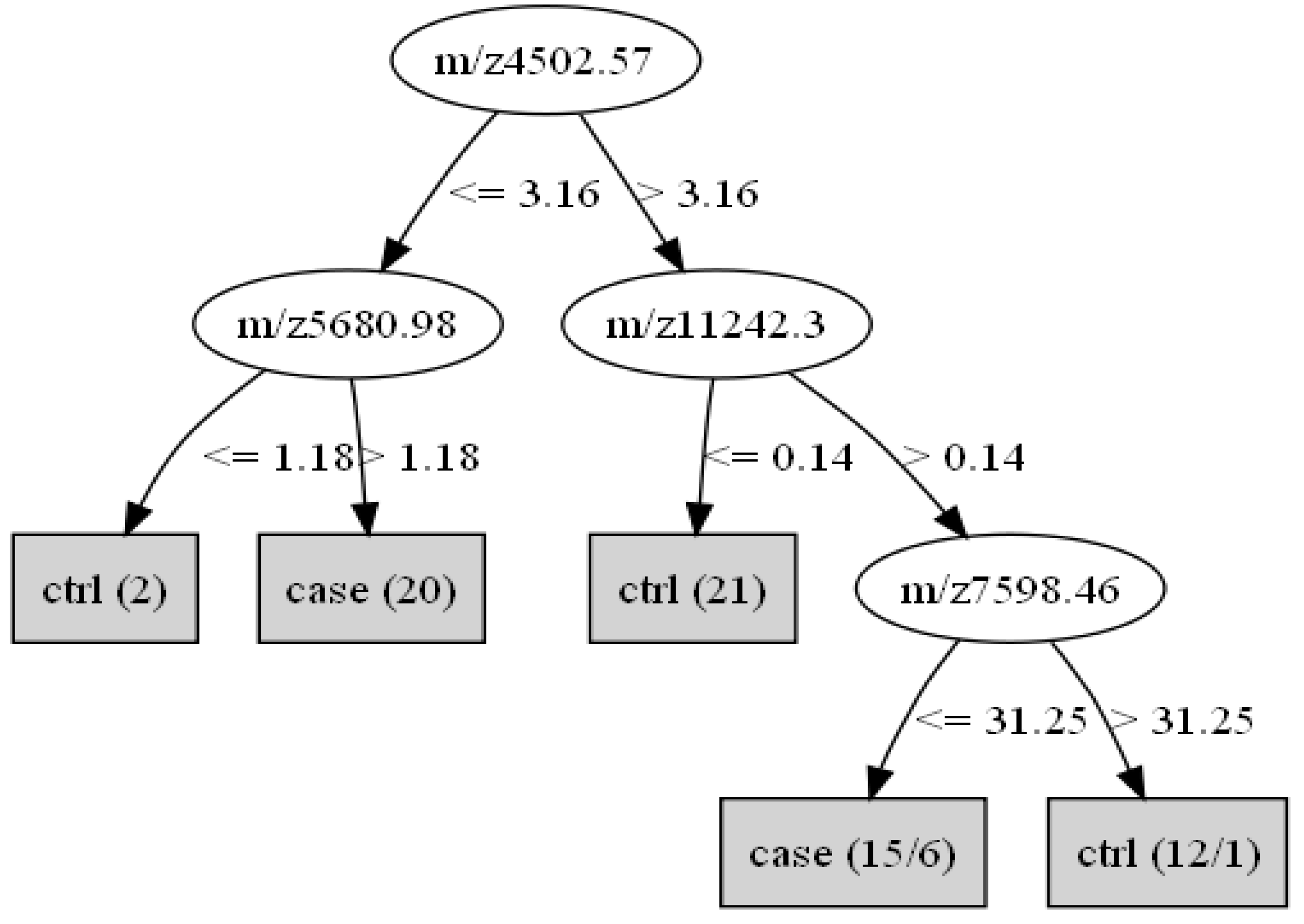
3.3. Construction of the Decision Tree Classification
| m/z | P value | Cases (N = 80) | Controls (N = 120) | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| 3,400 | 0.000000156 | 1.6057 | 2.4867 | 4.0861 | 2.0254 | |
| 4,502 | 0.00000219 | 4.0145 | 4.4959 | 9.7244 | 3.5676 | |
| 5,680 | 0.000132676 | 10.6997 | 9.2400 | 4.4620 | 4.7509 | |
| 7,598 | 0.000890586 | 23.0274 | 10.8248 | 32.6237 | 10.4506 | |
| 11,242 | 0.0025747 | 0.8937 | 1.2659 | 0.2457 | 0.4131 | |

3.4. Identification of BTC Cases and Controls
| Data set | Identified as BTCs | Identified as normal | ||||
|---|---|---|---|---|---|---|
| N | % | N | % | |||
| Training set | ||||||
| BTCs (N = 30) | 29 | 96.7 a | 1 | 3.3 | ||
| Normal (N = 40) | 6 | 15.0 | 34 | 85.0 b | ||
| Duplicate test set | ||||||
| BTCs (N = 30) | 20 | 66.7 a | 10 | 33.3 | ||
| Normal (N = 40) | 12 | 30.0 | 28 | 70.0 b | ||
| Blind test set | ||||||
| BTCs (N = 20) | 19 | 95.0 a | 1 | 5.0 | ||
| Normal (N = 20) | 5 | 25.0 | 15 | 75.0 b | ||
3.5. Reproducibility of the Assays
| Duplicate test set | Training set | Total | |
|---|---|---|---|
| BTCs | Normal | ||
| BTCs | 23 | 8 | 31 |
| Normal | 12 | 27 | 39 |
| Total | 35 | 35 | 70 |
| Protein peak(Da) | All subjects (n = 70) | BTCs (n = 30) | Controls (n = 40) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Difference in intensity (mean ± SD) | P for matchedt-test | Difference in intensity(mean ± SD) | P for matchedt-test | Difference in intensity (mean ± SD) | P forMatchedt-test | ||||
| 3400 | −0.2635 ± 3.0660 | 0.47 | −0.1313 ± 2.4212 | 0.77 | −0.3626 ± 3.4998 | 0.52 | |||
| 4502 | −0.1007 ± 4.0941 | 0.84 | −1.9796 ± 3.7785 | 0.0076 | 1.3084 ± 3.7798 | 0.03 | |||
| 5680 | 0.3937 ± 3.2844 | 0.32 | 0.2291 ± 4.0356 | 0.76 | 0.5172 ± 2.6040 | 0.22 | |||
| 7598 | 0.8956 ± 8.6985 | 0.39 | 1.6750 ± 6.7575 | 0.19 | 0.3110 ± 9.9545 | 0.84 | |||
| 11242 | −0.075 ± 0.5852 | 0.29 | −0.1597 ± 0.8023 | 0.28 | −0.0118 ± 0.3428 | 0.83 | |||
| Protein peaks (Da, mean ± SD) | CV for Intensity (%) | CV for m/z (%) |
|---|---|---|
| 3,400.04 | 68.8 | 0.00 |
| 4,502.57 | 61.0 | 0.00 |
| 5,685.76±3.08 | 32.7 | 0.05 |
| 7,600.15±3.40 | 15.8 | 0.04 |
| 11,242.30 | 39.0 | 0.00 |
4. Discussion
5. Conclusion
Acknowledgements
References
- Gao, Y.T.; Lu, W. Cancer Incidence, Mortality and Survival Rates in Urban Shanghai (1973–2000); Second Military Medical Universtiy Press: Shanghai, China, 2006. [Google Scholar]
- Jin, F.; Devesa, S.S.; Chow, W.H.; Zheng, W.; Ji, B.T.; Fraumeni, J.F., Jr.; Gao, Y.T. Cancer incidence trends in urban shanghai, 1972–1994: An updat. Int. J. Cancer 1999, 83, 435–440. [Google Scholar] [CrossRef]
- Carriaga, M.T.; Henson, D.E. Liver, gallbladder, extrahepatic bile ducts, and pancres. Cancer 1995, 75, 171–190. [Google Scholar] [CrossRef]
- Donohue, J.H.; Stewart, A.K.; Menck, H.R. The national cancer data base report on carcinoma of the gallbladder, 1989–1995. Cancer 1998, 83, 2618–2628. [Google Scholar] [CrossRef]
- Wang, B.; Qin, J.; Deng, J.; Zhang, B.; Han, T.; Shen, M.; Rashid, A.; Hsing, A.; Gao, Y. A survey on the diagnosis and treatment of biliary tract cancers in shanghai. Chin. J. Surg. 2005, 43, 455–459. [Google Scholar]
- Lowenfels, A.B.; Maisonneuve, P.; Boyle, P.; Zatonski, W.A. Epidemiology of gallbladder cancer. Hepatogastroenterology 1999, 46, 1529–1532. [Google Scholar]
- Kau, S.Y.; Shyr, Y.M.; Su, C.H.; Wu, C.W.; Lui, W.Y. Diagnostic and prognostic values of ca 19-9 and cea in periampullary cancers. J. Am. Coll. Surg. 1999, 188, 415–420. [Google Scholar] [CrossRef]
- Strom, B.L.; Maislin, G.; West, S.L.; Atkinson, B.; Herlyn, M.; Saul, S.; Rodriguez-Martinez, H.A.; Rios-Dalenz, J.; Iliopoulos, D.; Soloway, R.D. Serum cea and ca 19-9: Potential future diagnostic or screening tests for gallbladder cancer? Int. J. Cancer 1990, 45, 821–824. [Google Scholar] [CrossRef]
- Charatcharoenwitthaya, P.; Enders, F.B.; Halling, K.C.; Lindor, K.D. Utility of serum tumor markers, imaging, and biliary cytology for detecting cholangiocarcinoma in primary sclerosing cholangitis. Hepatology 2008, 48, 1106–1117. [Google Scholar] [CrossRef]
- Cui, J.F.; Liu, Y.K.; Zhou, H.J.; Kang, X.N.; Huang, C.; He, Y.F.; Tang, Z.Y.; Uemura, T. Screening serum hepatocellular carcinoma-associated proteins by seldi-based protein spectrum analysis. World J. Gastroenterol. 2008, 14, 1257–1262. [Google Scholar] [CrossRef]
- Chen, G.; Gharib, T.G.; Huang, C.C.; Thomas, D.G.; Shedden, K.A.; Taylor, J.M.; Kardia, S.L.; Misek, D.E.; Giordano, T.J.; Iannettoni, M.D.; Orringer, M.B.; Hanash, S.M.; Beer, D.G. Proteomic analysis of lung adenocarcinoma: Identification of a highly expressed set of proteins in tumors. Clin. Cancer Res. 2002, 8, 2298–2305. [Google Scholar]
- Petricoin, E.F.; Ardekani, A.M.; Hitt, B.A.; Levine, P.J.; Fusaro, V.A.; Steinberg, S.M.; Mills, G.B.; Simone, C.; Fishman, D.A.; Kohn, E.C.; Liotta, L.A. Use of proteomic patterns in serum to identify ovarian cancer. Lancet 2002, 359, 572–577. [Google Scholar] [CrossRef]
- Koopmann, J.; Zhang, Z.; White, N.; Rosenzweig, J.; Fedarko, N.; Jagannath, S.; Canto, M.I.; Yeo, C.J.; Chan, D.W.; Goggins, M. Serum diagnosis of pancreatic adenocarcinoma using surface-enhanced laser desorption and ionization mass spectrometry. Clin. Cancer Res. 2004, 10, 860–868. [Google Scholar] [CrossRef]
- Scarlett, C.J.; Saxby, A.J.; Nielsen, A.; Bell, C.; Samra, J.S.; Hugh, T.; Baxter, R.C.; Smith, R.C. Proteomic profiling of cholangiocarcinoma: Diagnostic potential of seldi-tof ms in malignant bile duct stricture. Hepatology 2006, 44, 658–666. [Google Scholar] [CrossRef]
- Liu, L.; Wang, J.; Liu, B.; Dai, S.; Wang, X.; Chen, J.; Huang, L.; Xiao, X.; He, D. Serum levels of variants of transthyretin down-regulation in cholangiocarcinoma. J. Cell Biochem. 2008, 104, 745–755. [Google Scholar] [CrossRef]
- Andreotti, G.; Chen, J.; Gao, Y.T.; Rashid, A.; Chang, S.C.; Shen, M.C.; Wang, B.S.; Han, T.Q.; Zhang, B.H.; Danforth, K.N.; Althuis, M.D.; Hsing, A.W. Serum lipid levels and the risk of biliary tract cancers and biliary stones: A population-based study in china. Int. J. Cancer 2008, 122, 2322–2329. [Google Scholar]
- Park, S.K.; Andreotti, G.; Sakoda, L.C.; Gao, Y.T.; Rashid, A.; Chen, J.; Chen, B.E.; Rosenberg, P.S.; Shen, M.C.; Wang, B.S.; Han, T.Q.; Zhang, B.H.; Yeager, M.; Chanock, S.; Hsing, A.W. Variants in hormone-related genes and the risk of biliary tract cancers and stones: A population-based study in china. Carcinogenesis 2009, 30, 606–614. [Google Scholar] [CrossRef]
- Sakoda, L.C.; Gao, Y.T.; Chen, B.E.; Chen, J.; Rosenberg, P.S.; Rashid, A.; Deng, J.; Shen, M.C.; Wang, B.S.; Han, T.Q.; Zhang, B.H.; Cohen-Webb, H.; Yeager, M.; Welch, R.; Chanock, S.; Fraumeni, J.F., Jr.; Hsing, A.W. Prostaglandin-endoperoxide synthase 2 (ptgs2) gene polymorphisms and risk of biliary tract cancer and gallstones: A population-based study in shanghai, china. Carcinogenesis 2006, 27, 1251–1256. [Google Scholar] [CrossRef]
- Hsing, A.W.; Gao, Y.T.; McGlynn, K.A.; Niwa, S.; Zhang, M.; Han, T.Q.; Wang, B.S.; Chen, J.; Sakoda, L.C.; Shen, M.C.; Zhang, B.H.; Deng, J.; Rashid, A. Biliary tract cancer and stones in relation to chronic liver conditions: A population-based study in shanghai, china. Int. J. Cancer 2007, 120, 1981–1985. [Google Scholar] [CrossRef]
- Hsing, A.W.; Gao, Y.T.; Han, T.Q.; Rashid, A.; Sakoda, L.C.; Wang, B.S.; Shen, M.C.; Zhang, B.H.; Niwa, S.; Chen, J.; Fraumeni, J.F., Jr. Gallstones and the risk of biliary tract cancer: A population-based study in china. Br. J. Cancer 2007, 97, 1577–1582. [Google Scholar] [CrossRef]
- Hsing, A.W.; Sakoda, L.C.; Rashid, A.; Andreotti, G.; Chen, J.; Wang, B.S.; Shen, M.C.; Chen, B.E.; Rosenberg, P.S.; Zhang, M.; Niwa, S.; Chu, L.; Welch, R.; Yeager, M.; Fraumeni, J.F., Jr.; Gao, Y.T.; Chanock, S.J. Variants in inflammation genes and the risk of biliary tract cancers and stones: A population-based study in china. Cancer Res. 2008, 68, 6442–6452. [Google Scholar] [CrossRef]
- Hsing, A.W.; Sakoda, L.C.; Rashid, A.; Chen, J.; Shen, M.C.; Han, T.Q.; Wang, B.S.; Gao, Y.T. Body size and the risk of biliary tract cancer: A population-based study in china. Br. J. Cancer 2008, 99, 811–815. [Google Scholar] [CrossRef]
- Golland, P.; Liang, F.; Mukherjee, S.; Panchenko, D. Permutation Tests for Classification; Morgan Kaufmann: San Francisco, CA, USA, 2005. [Google Scholar]
- Pelzer, A.E.; Feuerstein, I.; Fuchsberger, C.; Ongarello, S.; Bektic, J.; Schwentner, C.; Klocker, H.; Bartsch, G.; Bonn, G.K. Influence of blood sampling on protein profiling and pattern analysis using matrix-assisted laser desorption/ionisation mass spectrometry. BJU Int. 2007, 99, 658–662. [Google Scholar] [CrossRef]
- Gast, M.C.; Bonfrer, J.M.; van Dulken, E.J.; de Kock, L.; Rutgers, E.J.; Schellens, J.H.; Beijnen, J.H. Seldi-tof ms serum protein profiles in breast cancer: Assessment of robustness and validity. Cancer Biomark. 2006, 2, 235–248. [Google Scholar]
- Chaube, A.; Tewari, M.; Singh, U.; Shukla, H.S. Ca 125: A potential tumor marker for gallbladder cancer. J. Surg. Oncol. 2006, 93, 665–669. [Google Scholar] [CrossRef]
- Qin, X.L.; Wang, Z.R.; Shi, J.S.; Lu, M.; Wang, L.; He, Q.R. Utility of serum ca19-9 in diagnosis of cholangiocarcinoma: In comparison with cea. World J. Gastroenterol. 2004, 10, 427–432. [Google Scholar]
- Kim, H.J.; Kim, M.H.; Myung, S.J.; Lim, B.C.; Park, E.T.; Yoo, K.S.; Seo, D.W.; Lee, S.K.; Min, Y.I. A new strategy for the application of ca19-9 in the differentiation of pancreaticobiliary cancer: Analysis using a receiver operating characteristic curve. Am. J. Gastroenterol. 1999, 94, 1941–1946. [Google Scholar] [CrossRef]
© 2010 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Wang, W.-J.; Xu, W.-H.; Liu, C.-Z.; Rashid, A.; Cheng, J.-R.; Liao, P.; Hu, H.; Chu, L.W.; Gao, Y.-T.; Yu, K.; et al. Identification of Serum Biomarkers for Biliary Tract Cancers by a Proteomic Approach Based on Time-of-Flight Mass Spectrometry. Cancers 2010, 2, 1602-1616. https://doi.org/10.3390/cancers2031602
Wang W-J, Xu W-H, Liu C-Z, Rashid A, Cheng J-R, Liao P, Hu H, Chu LW, Gao Y-T, Yu K, et al. Identification of Serum Biomarkers for Biliary Tract Cancers by a Proteomic Approach Based on Time-of-Flight Mass Spectrometry. Cancers. 2010; 2(3):1602-1616. https://doi.org/10.3390/cancers2031602
Chicago/Turabian StyleWang, Wen-Jing, Wang-Hong Xu, Cha-Zhen Liu, Asif Rashid, Jia-Rong Cheng, Ping Liao, Heng Hu, Lisa W. Chu, Yu-Tang Gao, Kai Yu, and et al. 2010. "Identification of Serum Biomarkers for Biliary Tract Cancers by a Proteomic Approach Based on Time-of-Flight Mass Spectrometry" Cancers 2, no. 3: 1602-1616. https://doi.org/10.3390/cancers2031602
APA StyleWang, W.-J., Xu, W.-H., Liu, C.-Z., Rashid, A., Cheng, J.-R., Liao, P., Hu, H., Chu, L. W., Gao, Y.-T., Yu, K., & Hsing, A. W. (2010). Identification of Serum Biomarkers for Biliary Tract Cancers by a Proteomic Approach Based on Time-of-Flight Mass Spectrometry. Cancers, 2(3), 1602-1616. https://doi.org/10.3390/cancers2031602