Current Insights Regarding Metal-on-Metal Bearings for Hip Arthroplasty †


Musculoskeletal Sciences and Technology, Imperial College London, London SW7 2AZ, UK
†
Metal-on-Metal bearings for hip arthroplasty: Cobalt-chromium-molybdenum alloy articulating against itself.
Lubricants 2017, 5(3), 37; https://doi.org/10.3390/lubricants5030037
Submission received: 5 August 2017
/
Revised: 30 August 2017
/
Accepted: 9 September 2017
/
Published: 11 September 2017
(This article belongs to the Special Issue Tribological Performance of Artificial Joints 2017)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Modern small diameter metal-on-metal (MoM) bearings for total hip arthroplasty (THA) have been developed in the nineteen-eighties to address the problem of polyethylene wear related osteolysis. Subsequently large diameter MoM hip resurfacings (HRA) were designed for young and active patients to preserve bone and avoid dislocation. Large diameter MoM THA were originally meant as an easy femoral component-only revision solution for femoral neck fractures in HRA, but were then advocated for primary THA as well. In the last decade however, increasing numbers of revisions for adverse local tissues reactions (ALTR) to metal debris have been reported. These ALTR are due to excessive wear of the MoM bearings, usually related to malpositioning of the components leading to edge loading, or in rare cases to metal sensitivity. Besides the immunological reactions, metal particles and ions have a potential local and systemic toxicity. Wear and tribocorrosion at the taper-trunnion connections of MoM THA but also THA with polyethylene and ceramic bearings have also been recognized as a cause of ALTR with extensive tissue destruction. Despite the fact that the long-term survivorship and functional results of certain MoM HRA are excellent and better than THA in the young and active patients group, MoM bearings have become very unpopular and are likely to be replaced by bearing couples of other materials.
Metal-on-Metal (MoM) bearings for hip arthroplasty consisting of cobalt-chromium-molybdenum (CoCrMo) alloys were first introduced in the sixties by McKee and Farrar [1] and by Ring [2]. As early as 1968, Papps et al. published their findings on the toxicity of CoCrMo particles on tissue cultures [3], endorsed by the research of Trevor Rae, who, in 1979, concluded: ‘after the implantation of orthopaedic prostheses, metals can dissolve from the alloys used, some of the metals are toxic. […] From the biological standpoint, in view of the very much higher levels of soluble metal produced, metal against metal bearings should be avoided.’ [4] By that time, however, MoM hip arthroplasties had been abandoned for the low friction metal-on-polyethylene (MoP) hip replacements developed by Sir John Charnley [5]. When an increasing number of these MoP total hip arthroplasties (THA) had to be revised because of progressive loosening and extensive osteolysis caused by a macrophage response to polyethylene (PE) wear particles [6] whilst hip simulator studies were demonstrating substantially less volumetric wear from MoM bearing surfaces [7,8], MoM hip articulations were reintroduced to solve the problem of polyethylene (PE) particle-induced osteolysis. The imperfections regarding geometry, tolerance and metallurgy (low-carbon content associated with higher wear) of the first generation MoM articulations were resolved in the second generation high carbon content Metasul® MoM bearings (Sulzer/Centerpulse, Winterthur, Switzerland, 1988), which exhibited very promising short- and medium term results [9]. Furthermore, in the nineties, modern MoM hip resurfacing arthroplasty (HRA) (Figure 1) was proposed to address the inferior clinical results of THA in young and active patients, including the high dislocation rates of the 22 and 28 mm diameter femoral heads of the low friction MoP THA [10].
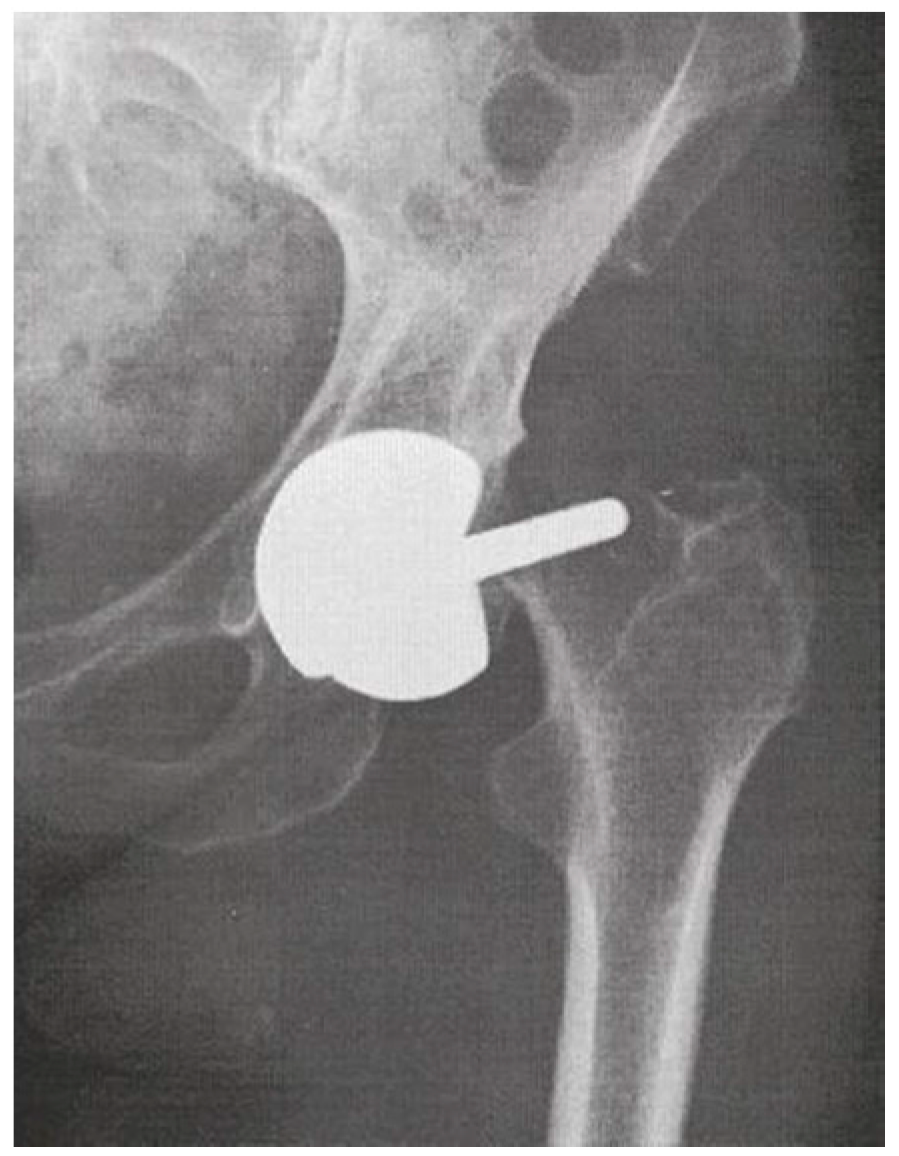
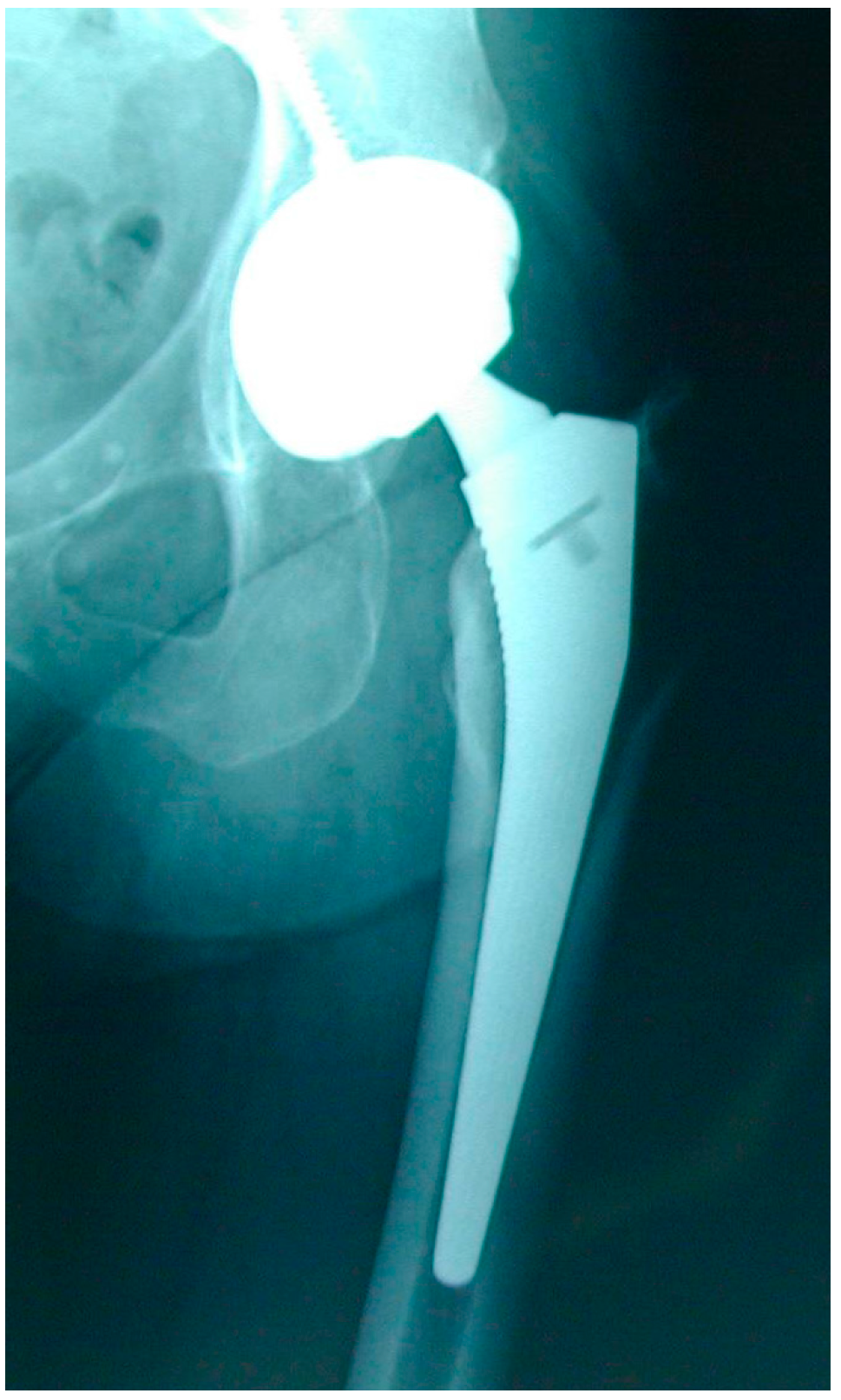
Early HRA failure modes mainly consisted of femoral neck fractures [11] (Figure 2), treated by revising only the femoral component and preserving the acetabular component and the MoM bearing. Large diameter MoM femoral heads modularly fitting on a prosthetic femoral stem had been specifically designed for these femoral component-only revisions of HRA (Figure 3). Following the good initial results of the Metasul® MoM hips and the reduced risk of dislocation with large diameter femoral heads, these HRA revision big femoral head (BFH) components were also used for primary THA, despite the smaller coverage angle of the acetabular design, the introduction of an additional MoM articulation at the taper–trunnion head–neck junction and despite the fact that these components had not been thoroughly tested for this indication [12,13].
In the meantime, Trevor Rae’s warnings remained buried under a load of papers on PE wear and PE particle disease, and were forgotten.
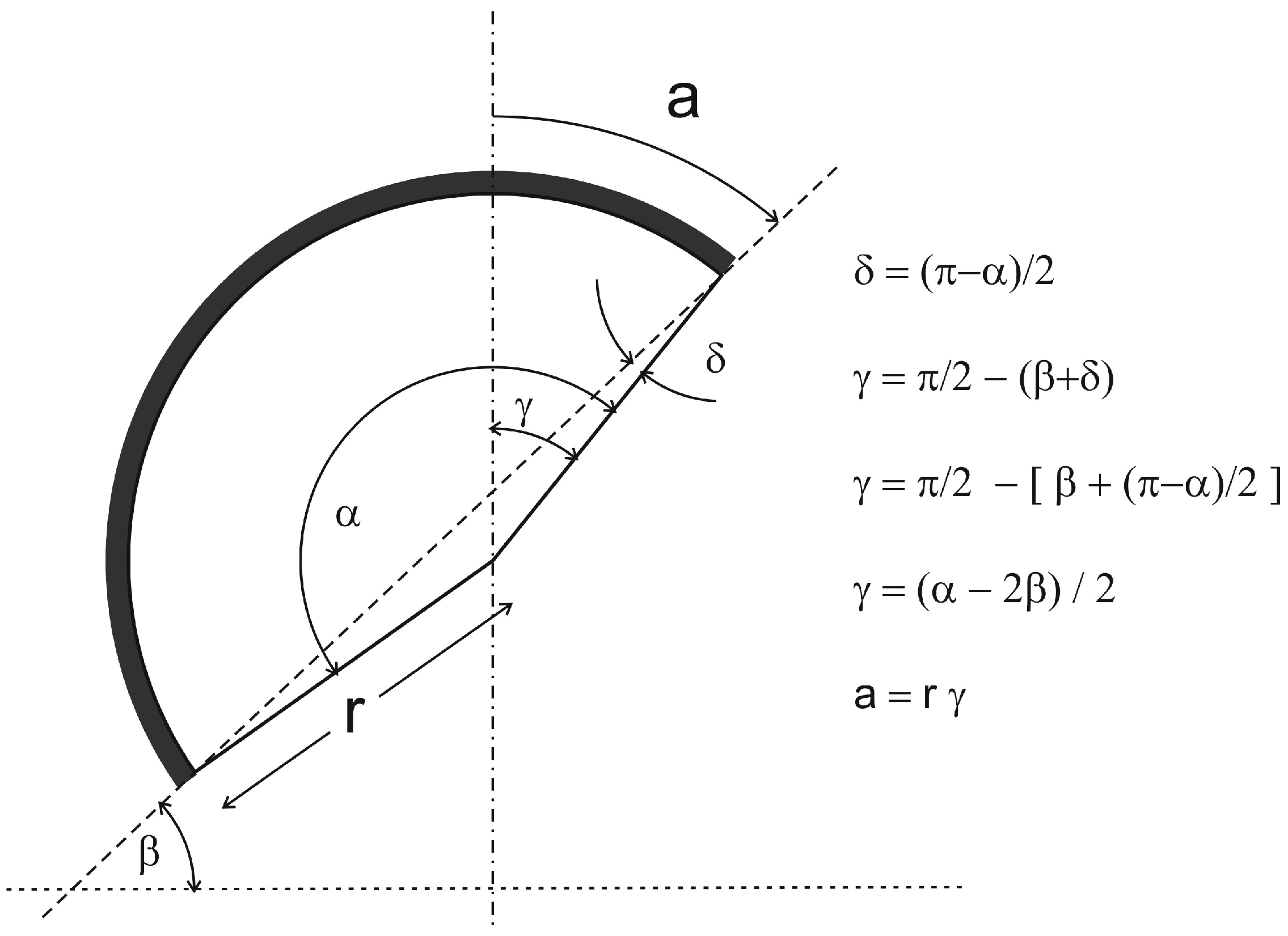
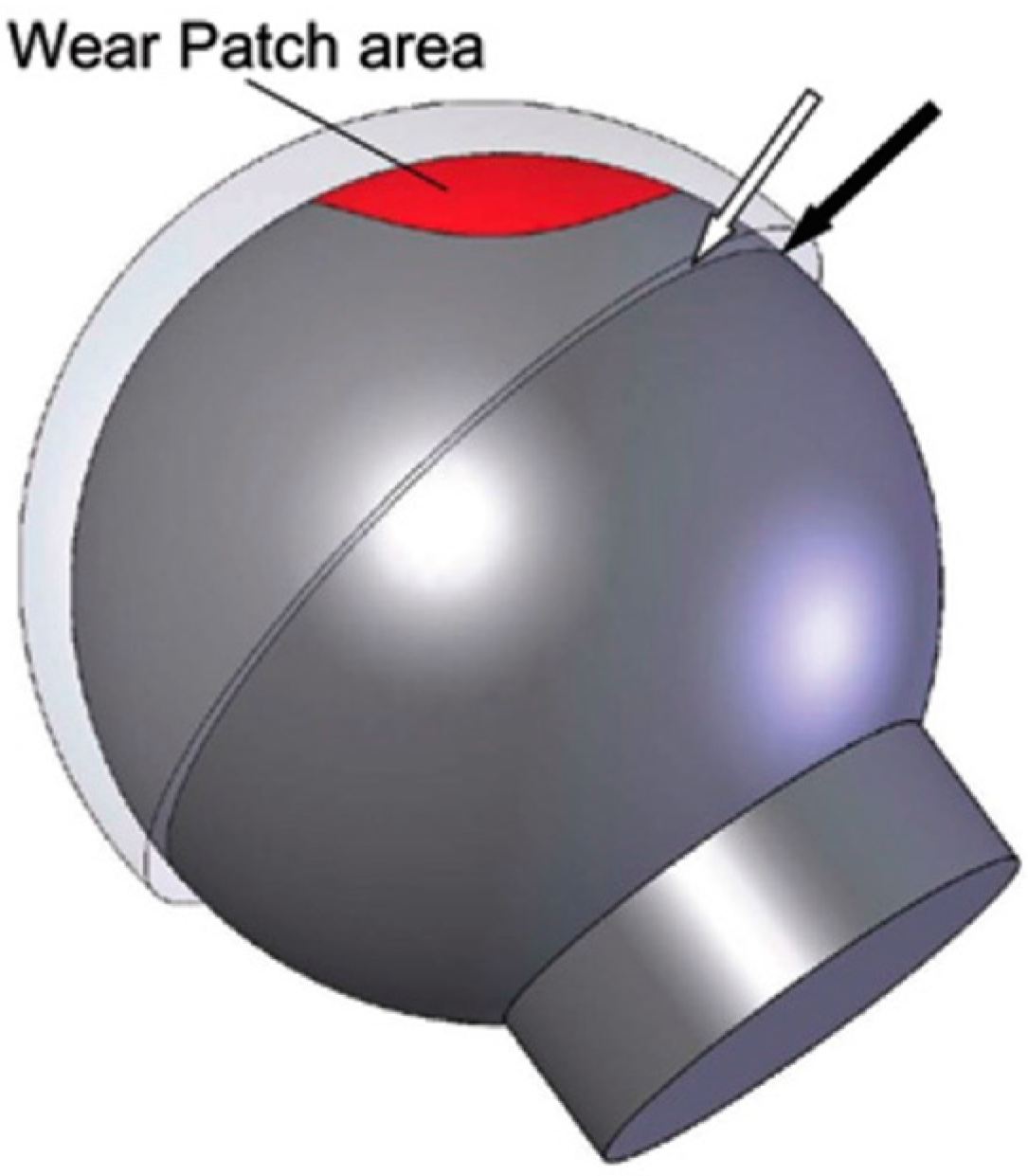
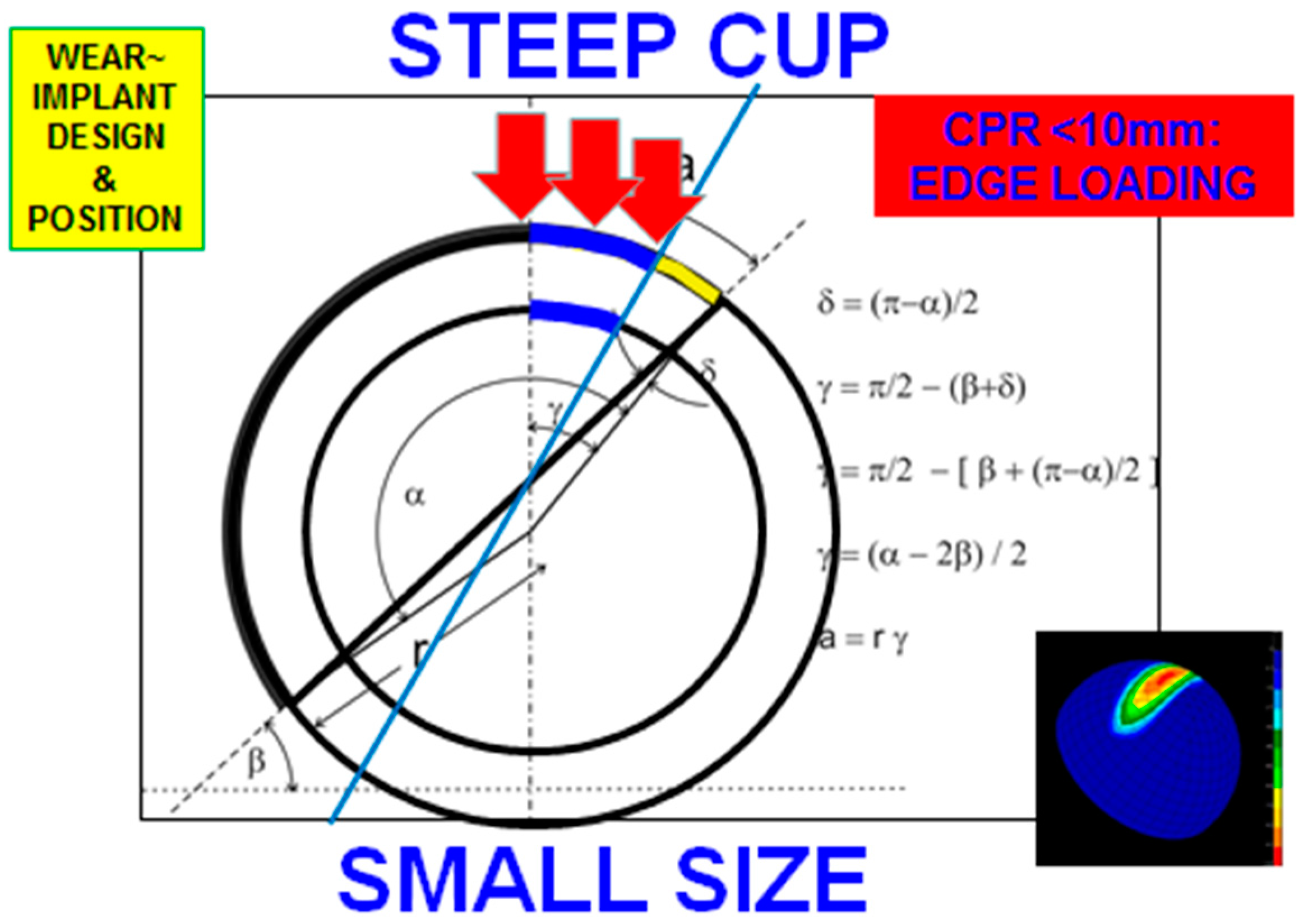
In 2005, Willert et al. published the first report on adverse tissue reactions to MoM hip arthroplasties, including 16 cases of 28 mm-diameter Metasul® bearings [14]. In 2008, the first paper on ‘Pseudotumours associated with Metal-on-Metal Hip Resurfacing’ from the Oxford group appeared [15] followed by many anecdotal reports on elevated metal ions, metallosis and soft tissue reactions from other centres [16]. In August 2010, the ASR (Articular Surface Replacement) MoM hip resurfacing and ASR-XL MoM THA (DePuy Orthopaedics, Warsaw, IN, USA) were recalled from the market for higher early revision rates due to adverse local tissue reactions (ALTR) to metal debris [17]. In the last decade, it has become apparent that design features including clearance and even more importantly the subtended articular arc (coverage angle) [18,19] (Figure 4) are crucial factors in the articular wear characteristics of MoM hip devices. In MoM hip arthroplasty, an important factor influencing the lubrication is the clearance, which is the difference in radius (radial clearance) or in diameter (diametrical clearance) between the acetabular and the femoral bearing surfaces [20]. (Figure 5). When the clearance is too large, the contact area between the femoral head and the acetabular cup during loading will be small (polar loading), which leads to high contact stresses and increased wear. When the clearance is too small, equatorial contact may occur during loading and both components will be jammed together, which also leads to increased wear (equatorial loading). In the ideal situation, a small wedge exists between the acetabular and femoral component via which a fluid film will be entrained during motion. Modern MoM hip arthroplasty designs and manufacturing have minimized the clearance problem by refining component geometry and reducing the tolerances, but with excessive wear e.g., at the edge, the altered clearance may become an additional factor accelerating implant failure [20]. The most important factor contributing to failure of modern MoM implants has been the coverage angle: a smaller subtended articular arc leads to a smaller contact patch to rim distance (CPR) (the distance between the point of intersection of the hip reaction force with the cup and the closest point on the inner side of the cup rim) [21]). A CPR < 10 mm leads to edge loading with higher wear [18,19,21] (Figure 6) and occurs more frequently with smaller femoral head sizes and when the acetabular component is placed at a higher inclination angle or at an inadequate anteversion angle [18]. This problem was most pronounced with the ASR designs exhibiting very low coverage angles but also with the smaller sizes of the BHR (Birmingham Hip Resurfacing, Smith&Nephew, London, UK) which had a smaller coverage angle and were more at risk for edge loading and increased wear, especially when not placed in the ideal position (Figure 7) [21,22]. Wear-related ALTR, as a result of innate macrophage-dominated immunological reactions to excessive wear debris (in casu metal particles) thus occurred more frequently with smaller sizes [23,24,25], in diagnoses associated with difficult surgical reconstruction because of anatomical anomalies such as developmental dysplasia of the hip (DDH) and post-traumatic osteoarthritis [23,24,25] and in the hands of less experienced surgeons with a suboptimal surgical technique leading to inadequate component positioning [23,24,26,27]. Females are more at risk for ALTR because of all the aforementioned reasons including smaller size, more frequent diagnosis of DDH, and higher anatomical hip anteversion [20,21,22]. Additionally, women seem to be more prone to metal allergy; cases of ALTR not related to excessive wear but to adaptive immunological reactions to metal particles occurring more often in females [23,24,28]. It needs to be emphasized that the generation of metal particles is not an exclusive characteristic of MoM hip arthroplasty. In wear simulator studies with total knee arthroplasties (TKA), Kretzer et al. have demonstrated that 12% (in weight) of the wear products generated in these metal-on-polyethylene articulations were metallic purely related to wear and without measuring additional soluble metal ion generation by corrosion [29].
Besides the generation of metal particles, metal ions are released by corrosion of the metal implant surfaces and also the metal wear particles. The most studied ions in relation to MoM hips are chromium (Cr) and cobalt (Co). Cr ions from MoM hip surfaces usually consist of trivalent Cr3+ ions that rapidly bind with hydroxides and anions to form Cr hydroxides, oxides and salts used for the regeneration of the passive film on the metal surfaces [30]. These ions are thus less available for bonds with biomolecules (proteins, RNA, DNA) intra- and extracellularly and potentially less toxic. Co ions, on the other hand, remain in a soluble state for a longer time and may bind to intra- and extracellular biomolecules with a potential systemic toxic effect [31].
Elevated systemic (whole blood, serum or urine) levels of Co and Cr are indicative of higher wear or failure of an MoM hip articulation, after exclusion of other sources of metal ions such as occupational exposure, other metal implants or medicinal intake [17,29]. Safe upper levels have been established in unilateral (Cr < 4.6 µg/L; Co < 4.0 µg/L) and bilateral HRA (Cr < 7.4 µg/L; Co < 5 µg/L) [19,32]. These safe levels are confirmed in other studies [33]. Additionally, well performing MoM hips have been associated with decreasing ion levels [33]. Analysis of consecutive ion levels in HRA demonstrated a statistically significant overall decrease of Cr and Co levels with time [34]. In 25% of patients, ion levels were undetectable at ≥10 years postoperatively. Increasing metal ion levels correlated with greater cup inclination angles and levels >10 µg/L were associated with poorly functioning or malpositioned MoM HRA leading to metal particulate debris [34]. The in vivo decrease of metal ion levels with time is in accordance with tribocorrosion studies indicating a lower-wear bedding-in phase after the initial running-in phase of higher wear [35]. These studies also describe the formation of a passive protective film on the articulating metal surfaces after the initial wear-in, preventing further corrosion [35,36]. Ions are then mainly formed by corrosion of the metal particles provided there is no additional surface wear.
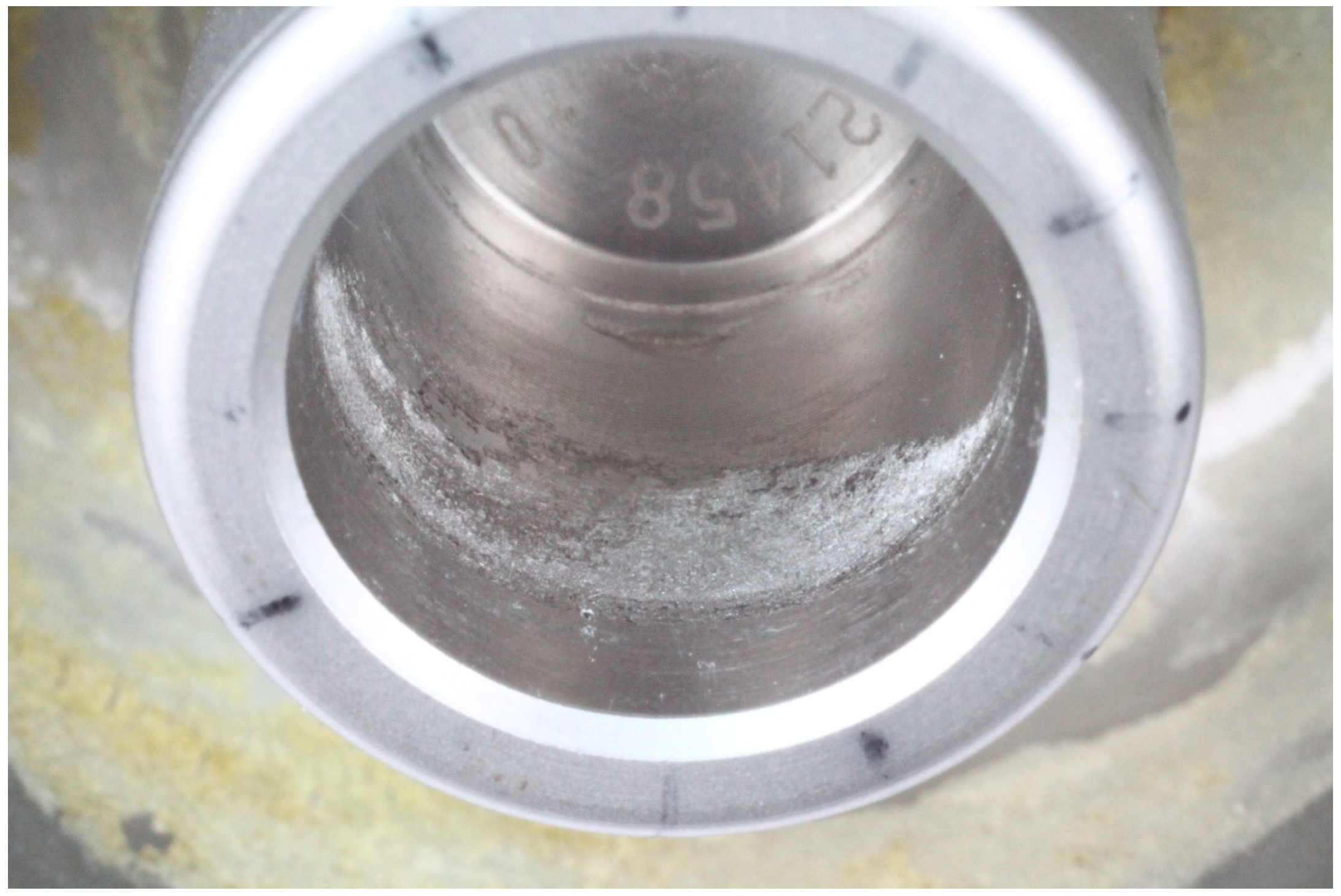
The upper acceptable levels outlined above refer to ion measurements of patients with MoM HRA and do not include MoM THA with a large diameter femoral head. Several authors have demonstrated higher levels of Co and Cr ions with MoM large diameter head THA compared to MoM HRA [37,38]. The extra burden of metal particles and ions is probably related to wear due to high tolerances leading to toggling, to the introduction of ridged surfaces on tapers/trunnions to accommodate ceramic heads as well and/or to inadequate load distributions [39,40,41]. However, crevice corrosion at the taper–trunnion connection between the modular head and the prosthetic femoral neck is probably the most important factor leading to ALTR [42]. The trunnion refers to the proximal conal extremity of the femoral stem or the ’male’ component of the modular junction. The taper refers to the ‘female’ component of the modular junction i.e., the area inside the femoral head that receives the trunnion. A taper may either be the internal cone of the femoral head or of the sleeve adaptor inserted into the metal or ceramic femoral head to accommodate the prosthetic neck. The confined spaces (crevices) between taper and trunnion allow for an alteration of the chemical environment by trapping fluid, excluding oxygen and lowering the pH [42]. In addition, toxic corrosion products including metal oxides, chlorides and organometallic compounds, but also particles and third bodies may be trapped and accumulate. The low pH and degradation products form a highly toxic environment leading to rapid cell death, necrosis and tissue destruction even with low concentration of metal ions. Crevice corrosion is recognized as one of the failure mechanisms at the taper/trunnion modular connection of MoM THA with large diameter heads (Figure 8) [42,43].
Monitoring of metal ions is advocated as a screening tool for implant performance, in order to detect increased wear at an early stage, and, if necessary, perform a hip revision before extensive tissue destruction has occurred [19]. Furthermore, metal ion measurements are useful to prevent toxic local and systemic reactions which may result from continuous exposure to high levels of ions and particles, especially Co. Animal studies have identified Co2+ as the major element mediating mainly neurotoxicity but also cardiac and thyroid toxicity [44], whilst Cr3+ ions alone had no apparent clinical or histo-pathological adverse effects. According to the Mayo Medical Laboratories (Rochester, MN, USA), Co ≥ 1 µg/L is indicative of Co exposure whilst dosages > 5 µg/L may be associated with adverse effects [45,46]. However, there is no established toxicity level in total joint arthroplasty (hips and knees). Systemic Co toxicity in relation with MoM hips has been referred to as arthroprosthetic cobaltism [47,48], including symptoms of hearing loss, visual impairment, vertigo, neurological disorders, cardiomyopathy, hypothyroidism, fatigue, cognitive disorders, behavioural and mood changes [23,47,48]. However, systemic Co toxicity is rare, is associated with high systemic Co levels >20 μg/L [19,23] to >100 μg/L [46] and is usually reversible after revision of the failing components with decrease of the Co levels [23,47,48,49,50,51]. Furthermore, there is no evidence of nephrotoxicity at 10 years [52].
Co particles have also been shown in vitro to have a toxic effect on macrophages leading to apoptosis and necrosis [53]. In a review paper, Nine et al. tried to correlate biological findings with debris morphology and disintegration [54]. Smaller debris particles from any material (PE, metal, ceramic) are associated with higher inflammatory responses incl. cytokine release. Phagocytosis of particles by macrophages was shown to be size-dependent: nanosized particles from any material highly stimulate cells at high volumetric dosages whilst the size-dependent response rate weakens with lower doses [54]. Sansone et al. showed that CoCr particles may also have an adverse effect on bone by inhibiting osteoblastic functions whilst recruiting osteoclastic precursors, the combination of which may lead to osteolysis and aseptic component loosening [55].
Baskey et al. demonstrated that Co2+ and Cr3+ ions are capable of stimulating migration of T-lymphocytes, but not B-lymphocytes, which could explain the accumulation of T-cells in some of the ALTR [56]. These histological features were first characterised as ALVAL (Aseptic Lymphocytic Vasculitis Associated Lesions) by Willert et al. [14]. The term ALVAL is essentially a histological description and is often misused as diagnostic term. Attempts to classify the ALVAL features have led to several scores, which are mostly qualitative but unfortunately too inconsistent with each other to be compared [57,58]. Whether Baskey’s findings can also be correlated with a possible delayed type IV hypersensitivity reaction remains to be elucidated. The incidence of failures of joint arthroplasties due to metal allergy is believed to be low, but the diagnosis is difficult as skin patch tests and lymphocyte transformation tests (LTT) are usually inconclusive [59], and the differentiation from a low grade infection often tricky. In a review of the Danish allergy register and the Danish Knee Register however, Munch et al. stated that metal allergy was probably underestimated as cause of failure of total joint arthroplasty, as multiple TKA revisions were more often associated with proven Cr or Co allergies [60].
Genotoxicity of Co and Cr ions has been a concern. In vitro studies and studies of cells retrieved from synovial fluid recovered at MoM hip revisions demonstrated chromosomal changes/DNA damage associated with Cr3+/6+ and Co2+ ions [61]. These findings do not imply a greater risk for cancer, however. In young female patients with an MoM hip who became pregnant, ion transfer via the placenta amounted to about 50% of the whole blood levels [62]. However, to date, there has not been any evidence of teratogenicity or fetal toxicity. Co ions have also been found in the sperm of men with MoM hips [63], but an effect on paternal fertility comparable to the decreased fertility of stainless steel welders exposed to Cr6+ [64] has not been demonstrated.
In order to assess possible carcinogenesis of MoM hip replacements, epidemiological studies have been undertaken. Mäkelä et al. matched the Finnish Hip registry and the Finnish Cancer Registry from 2001 to 2010 to compare the overall cancer and death risk of 10,728 MoM hips and 18,235 conventional THA and concluded that the risk was not increased with MoM [65]. Similarly, Smith et al. investigated the National joint Registry of England and Wales and showed that there was no evidence that MoM was associated with an increased risk of cancer [66].
Individual series and hip registries are now publishing excellent long-term (15 to 20 years) survivorship results of MoM THA with the Metasul® bearing and of certain MoM HRA including BHR, CONSERVE PLUS (Microport Orthopaedics, Boston, MA, USA) and RECAP (Biomet Inc., Warsaw, IN, USA) [67,68,69]. A paper reporting short-term results from the Finnish registry put the BHR forward was the best hip replacement option [70]. Important factors of success were male gender and surgical volume and experience [27]. The latest reports of the Australian Registry show excellent survivorship of the BHR, ADEPT (Matortho, Leatherhead, UK) and MITCH (Stryker, Kalamazoo, MI, USA), with better results than conventional THA in patients younger than 50 at surgery [25]. Functional results including gait analysis and activity assessments are also more favourable for hip resurfacing [70,71]. Most remarkable were the papers demonstrating a significantly lower 10 year cumulative patient mortality rates for MoM hip resurfacing (2.6%) compared to non-cemented (3.2%) and especially cemented THA (7.3%) after adjustment for age, gender, comorbidity, rurality and social deprivation [72,73]. The reasons for these mortality findings have not been elucidated.
For all the aforementioned reasons, MoM bearings have become controversial. Despite the fact that an estimated 1 milllion current generation MoM hip replacements have been performed over the last 20 years with good to excellent results from experienced surgeons even on the long term, especially in the case of Metasul® THA and BHR HRA [25,67,74], the reports of revisions for unexplained pain and soft tissue reactions have alerted the orthopaedic community, the health authorities and the patients. Advisory organs such as the SCENIHR (Scientific Committees on Emerging and Newly Identified Health risks) of the European Commission [75] and Health authorities such as the Food and Drug Administration (FDA) in the USA [76] and the Medicines and Healthcare products Regulatory Agency (MHRA) in the UK [77] have issued repetitive alerts and recommendations regarding the use of MoM hip arthroplasty and the management of patients. MoM THA with BFH > 36 mm are not to be used anymore except for unusual revision cases. MoM HRA is still acceptable, but implantation in females and in patients with small head sizes is advised against. Patients with an MoM hip replacement are to be followed closely and regular metal ion measurements are advocated. In case of unexplained pain or elevated ion levels, additional cross-sectional imaging with Magnetic Resonance Imaging (MRI) or ultrasound is advised; if ALTR is diagnosed, revision of the MoM hip to a THA with an alternative bearing couple is advocated. Certain countries have banned MoM hips altogether including hip resurfacing (the Netherlands, Sweden, Denmark), and well-functioning and asymptomatic MoM hips are being revised under the pretense that they would be poisonous. In 2015, Smith&Nephew decided to withdraw the BHR smaller sizes from the market [78] and Zimmer-Biomet is ending the 30 year-long Metasul story in December 2017.
Unfortunately, due to all the negative publicity around MoM, there is a major lack of interest and funding for fundamental research to finally elucidate the pathogenesis of the ALTR and investigate individual patient susceptibility. In the meantime, the new problem of trunnionosis or taperosis and associated destructive ALTR described above has become a cause for increasing concern regarding CoCrMo and TiAlV taper–trunnion connections, and also with MoP and ceramic bearings and <40 mm head sizes [79].
Even though the long-term survivorship and functional results of MoM HRA are excellent and better than THA in the young and active patients group, the future of MoM hip replacement looks gloomy and new bearing couples for hip resurfacing are likely to take over soon.
Acknowledgments
All sources of funding of the study should be disclosed. Please clearly indicate grants that you have received in support of your research work. Clearly state if you received funds for covering the costs to publish in open access.
Conflicts of Interest
The author declares no conflict of interest.
References
- McKee, G.K.; Watson-Farrar, J. Replacement of arthritic hips by the McKee-Farrar prosthesis. J. Bone Jt. Surg. Br. 1966, 48, 245–259. [Google Scholar]
- Ring, P.A. Ring UPM total hip arthroplasty. Clin. Orthop. Relat. Res. 1983, 176, 115–123. [Google Scholar] [CrossRef]
- Papps, A.M.; Cohen, J. Toxicity of Metal Particles in Tissue Culture: Part I: A New Assay Method Using Cell Counts in The Phase of Replication. J. Bone Jt. Surg. Am. 1968, 50, 535–547. [Google Scholar] [CrossRef]
- Rae, T. Comparative laboratory studies on the production of soluble and particulate metal by total joint prostheses. Arch Orthop. Trauma. Surg. 1979, 95, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Charnley, J. Total hip replacement by low-friction arthroplasty. Clin. Orthop. Relat. Res. 1970, 72, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Jasty, M.J.; Floyd, W.E., 3rd; Schiller, A.L.; Goldring, S.R.; Harris, W.H. Localized osteolysis in stable, non-septic total hip replacement. J. Bone Jt. Surg. Am. 1986, 68, 912–919. [Google Scholar] [CrossRef]
- Weber, B.G.; Fiechter, T. Polyethylene wear and late loosening of a total prosthesis of the hip joint? New perspectives for metal/metal pairing if the capsule and head. Orthopade 1989, 18, 370–376. [Google Scholar] [PubMed]
- Anissian, H.L.; Stark, A.; Gustafson, A.; Good, V.; Clarke, I.C. Metal-on-metal bearing in hip prosthesis generates 100-fold less wear debris than metal-on-polyethylene. Acta Orthop. Scand. 1999, 70, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Sieber, H.P.; Rieker, C.B.; Köttig, P. Analysis of 118 second-generation metal-on-metal retrieved hip implants. J. Bone Jt. Surg. Br. 1999, 81, 46–50. [Google Scholar] [CrossRef]
- Hedlundh, U.; Ahnfelt, L.; Hybbinette, C.H.; Wallinder, L.; Weckström, J.; Fredin, H. Dislocations and the femoral head size in primary total hip arthroplasty. Clin. Orthop. Relat. Res. 1996, 333, 226–233. [Google Scholar] [CrossRef]
- Shimmin, A.J.; Bare, J.; Back, D.L. Complications associated with hip resurfacing arthroplasty. Orthop. Clin. N. Am. 2005, 36, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Girard, J. Femoral head diameter considerations for primary total hip arthroplasty. Orthop. Trauma. Surg. Res. 2015, 101, S25–S29. [Google Scholar] [CrossRef] [PubMed]
- Malviya, A.; Ramaskandhar, J.R.; Bowman, R.; Kometa, S.; Hashmi, M.; Lingard, E.; Holland, J.P. What advantage is there to be gained using large modular metal-on-metal bearings in routine primary total hip replacement? Bone Jt. J. Dec. 2011, 93, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- Willert, H.G.; Buchhorn, G.H.; Fayyazi, A.; Flury, R.; Windler, M.; Köster, G.; Lohmann, C.H. Metal-on-metal bearings and hypersensitivity in patients with artificial hip joints. A clinical and histomorphological study. J. Bone Jt. Surg. Am. 2005, 87, 28–36. [Google Scholar]
- Pandit, H.; Glyn-Jones, S.; McLardy-Smith, P.; Gundle, R.; Whitwell, D.; Gibbons, C.L.; Ostlere, S.; Athanasou, N.; Gill, H.S.; Murray, D.W. Pseudotumours associated with Metal-on-Metal Hip Resurfacing. J. Bone Jt. Surg. Br. 2008, 90, 847–851. [Google Scholar] [CrossRef] [PubMed]
- De Smet, K.A.; Van Der Straeten, C.; Van Orsouw, M.; Doubi, R.; Backers, K.; Grammatopoulos, G. Revisions of metal-on-metal hip resurfacing: Lessons learned and improved outcome. Orthop. Clin. N. Am. 2011, 42, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Australian Orthopaedic Association National Joint Replacement Registry. Annual Report 2010. Published October 2010. Available online: www.dmac.adelaide.edu.au/aoanjrr/publications.jsp (accessed on 4 August 2017).
- De Haan, R.; Pattyn, C.; Gill, H.S.; Murray, D.W.; Campbell, P.A.; De Smet, K. Correlation between inclination of the acetabular component and metal ion levels in metal-on-metal hip resurfacing replacement. J. Bone Jt. Surg. Br. 2008, 90, 1291–1297. [Google Scholar] [CrossRef] [PubMed]
- Van Der Straeten, C.; Grammatopoulos, G.; Gill, H.S.; Calistri, A.; Campbell, P.; De Smet, K.A. The 2012 Otto Aufranc Award: The interpretation of metal ion levels in unilateral and bilateral hip resurfacing. Clin. Orthop. Relat. Res. 2013, 471, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Brockett, C.L.; Harper, P.; Williams, S.; Isaac, G.H.; Dwyer-Joyce, R.S.; Jin, Z.; Fisher, J. The influence of clearance on friction, lubrication and squeaking in large diameter metal-on-metal hip replacements. J. Mater. Sci. Mater. Med. 2008, 19, 1575–1579. [Google Scholar] [CrossRef] [PubMed]
- Langton, D.J.; Jameson, S.S.; Joyce, T.J.; Gandhi, J.N.; Sidaginamale, R.; Mereddy, P.; Lord, J.; Nargol, A.V. Accelerating failure rate of the ASR total hip replacement. J. Bone Jt. Surg. Br. 2011, 93, 1011–1016. [Google Scholar] [CrossRef] [PubMed]
- Clarke, I.C.; Donaldson, T.K.; Burgett, M.D.; Smith, E.J.; Bowsher, J.; Savisaar, C.; John, A.; Lazennec, J.Y.; McPherson, E.; Peters, C.L. Normal and adverse wear patterns created in vivo on metal-on-metal surfaces—A retrieval study representing four vendors. Metal-on-Metal Total Hip Replacement Devices STP 1560. 2013. Available online: www.astm.org (accessed on 4 August 2017).
- De Smet, K.; Campbell, P.; Van Der Straeten, C. The Hip Resurfacing Handbook. A Practical Guide to the Use and Management of Modern Hip Resurfacings. Introduction; Woodhead Publishing Limited: Oxford, UK; Cambridge, UK; Philadelphia, PA, USA; New Delhi, India, 2013. [Google Scholar]
- Van Der Straeten, C.; De Smet, K.A. Current expert views on metal-on-metal hip resurfacing arthroplasty. Consensus of the 6th Advanced hip resurfacing course, Ghent, Belgium, May 2014. Hip Int. 2016, 26, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Australian Orthopaedic Association National Joint Replacement Registry. Annual Report 2016. Published October 2016. Available online: www.dmac.adelaide.edu.au/aoanjrr/publications.jsp (accessed on 4 August 2017).
- Shimmin, A.B.; Baré, J.V. Comparison of Functional Results of Hip Resurfacing and Total Hip Replacement: A Review of the Literature. Orthop. Clin. N. Am. 2011, 42, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Seppänen, M.; Mäkelä, K.; Virolainen, P.; Remes, V.; Pulkkinen, P.; Eskelinen, A. Hip resurfacing arthroplasty: Short-term survivorship of 4401 hips from the Finnish Arthroplasty Register. Acta Orthop. 2012, 83, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Hallab, N.; Merritt, K.; Jacobs, J.J. Metal sensitivity in patients with orthopaedic implants. J. Bone Jt. Surg. Am. 2001, 83, 428–436. [Google Scholar] [CrossRef]
- Kretzer, J.P.; Reinders, J.; Sonntag, R.; Hagmann, S.; Streit, M.; Jeager, S.; Moradi, B. Wear in total knee arthroplasty—Just a question of polyethylene?: Metal ion release in total knee arthroplasty. Int. Orthop. 2014, 38, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Neville, A.; Dowson, D. Understanding the role of corrosion in the degradation of metal-on-metal implants. Proc. Inst. Mech. Eng. Part H 2006, 220, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Hanawa, T. Metal ion release from metal implants. Mater. Sci. Eng. C 2004, 24, 745–752. [Google Scholar] [CrossRef]
- Estey, M.P.; Van Der Straeten, C.; Tower, S.S.; Hart, A.J.; Moyer, T.P.; Diamandis, E.P. Cobalt and Chromium Measurement in Patients with Metal Hip Prostheses. Clin. Chem. 2013, 59, 6. [Google Scholar] [CrossRef] [PubMed]
- Sidaginamale, R.P.; Joyce, T.J.; Lord, J.K.; Jefferson, R.; Blain, P.G.; Nargol, A.V.; Langton, D.J. Blood metal ion testing is an effectivescreening tool to identify poorly performing metal-on-metal bearingsurfaces. Bone Jt. Res. 2013, 16, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Van Der Straeten, C.; Van Quickenborne, D.; De Roest, B.; Calistri, A.; Victor, J.; De Smet, K. Metal ion levels from well-functioning Birmingham Hip Resurfacings decline significantly at ten years. Bone Jt. J. 2013, 95, 1332–1338. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Dowson, D.; Neville, A. In-situ electrochemical study of interaction of tribology and corrosion in artificial hip prosthesis simulators. J. Mech. Behav. Biomed. Mater. 2012, 18, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Mathew, M.T.; Jacobs, J.J.; Wimmer, M.A. Wear-corrosion synergism in a CoCrMo hip bearing alloy is influenced by proteins. Clin. Orthop. Relat. Res. 2012, 470, 3109–3117. [Google Scholar] [CrossRef] [PubMed]
- Venditolli, P.-A.; Amzica, T.; Roy, A.; Lusignan, D.; Girard, J.; Lavigne, M. Metal ion release with large-diameter metal-on-metal hip arthroplasty. J. Arthroplast. 2011, 26, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Garbuz, D.S.; Tanzer, M.; Greidanus, N.V.; Masri, B.A.; Duncan, C.P. The John Charnley Award: Metal-on-metal hip resurfacing versus large-diameter head metal-on-metal total hip arthroplasty: A randomized clinical trial. Clin. Orthop. Relat. Res. 2010, 468, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Osman, K.; Panagiotidou, A.P.; Khan, M.; Blunn, G.; Haddad, F.S. Corrosion at the head-neck interface of current designs of modular femoral components: Essential questions and answers relating to corrosion in modular head-neck junctions. Bone Jt. J. 2016, 98, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Panagiotidou, A.; Meswania, J.; Hua, J.; Muirhead-Allwood, S.; Hart, A.; Blunn, G. Enhanced wear and corrosion in modular tapers in total hip replacement is associated with contact area and surface topography. J. Orthop. Res. 2013, 31, 2032–2039. [Google Scholar] [CrossRef] [PubMed]
- Hothi, H.S.; Eskelinen, A.P.; Berber, R.; Lainiala, O.S.; Moilanen, T.P.S.; Skinner, J.A.; Hart, A.J. Factors associated with Trunnionosis in the Metal-on-Metal Pinnacle Hip. J. Arthroplast. 2017, 32, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Cooper, H.J.; Della Valle, C.J.; Berger, R.A.; Tetreault, M.; Paprosky, W.G.; Sporer, S.M.; Jacobs, J.J. Corrosion at the head–neck taper as a cause for adverse local tissue reactions after total hip arthroplasty. J. Bone Jt. Surg. Am. 2012, 94, 1655–1661. [Google Scholar] [CrossRef]
- Cook, R.B.; Bolland, B.J.; Wharton, J.A.; Tilley, S.; Latham, J.M.; Wood, R.J. Pseudotumour formation due to tribocorrosion at the taper interface of large diameter metal on polymer modular total hip replacements. J. Arthroplast. 2013, 28, 1430–1436. [Google Scholar] [CrossRef] [PubMed]
- Hallab, N.J.; Jacobs, J.J. Biologic effects of implant debris. Bull. NYU Hosp. Jt. Dis. 2009, 67, 182–188. [Google Scholar] [PubMed]
- Leavelle, D.E. Interpretive Handbook: Interpretive Data for Diagnostic Laboratory Tests; Mayo Medical Laboratories: Rochester, MN, USA, 2001. [Google Scholar]
- Leyssens, L.; Vinck, B.; Van Der Straeten, C.; Wuyts, F.; Maes, L. Cobalt toxicity in humans—A review of the potential sources and systemic health effects. Toxicology 2017, 387, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Tower, S.S. Arthroprosthetic cobaltism: Neurological and cardiac manifestations in two patients with metal-on-metal arthroplasty: A case report. J. Bone Jt. Surg. Am. 2010, 92, 2847–2851. [Google Scholar] [CrossRef] [PubMed]
- Tower, S. Arthroprosthetic cobaltism: Identification of the at-risk patient. Alaska Med. 2010, 52, 28–32. [Google Scholar] [PubMed]
- Rizzetti, M.C.; Liberini, P.; Zarattini, G.; Catalani, S.; Pazzaglia, U.; Apostoli, P.; Padovani, A. Loss of sight and sound. Could it be the hip? Lancet 2009, 373, 1052. [Google Scholar] [CrossRef]
- Van Lingen, C.P.; Ettema, H.B.; Van Der Straeten, C.; Kollen, B.J.; Verheyen, C.C. Self-reported neurological clinical manifestations of metal toxicity in metal-on-metal hip arthroplasty. Hip Int. 2014, 24, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, T.; Takahashi, K.; Kabata, T.; Sakagoshi, D.; Tomita, K.; Yamada, M. Polyneuropathy caused by cobalt-chromium metallosis after total hip replacement. Muscle Nerve 2010, 42, 140–143. [Google Scholar] [CrossRef] [PubMed]
- Corradi, M.; Daniel, J.; Ziaee, H.; Alinovi, R.; Mutti, A.; McMinn, D. Early Markers of Nephrotoxicity in Patients With Metal-on-metal Hip Arthroplasty. Clin. Orthop. Relat. Res. 2011, 469, 1651–1659. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.M.; Xia, Z.; Glyn-Jones, S.; Beard, D.; Gill, H.S.; Murray, D.W. Dose-dependent cytotoxicity of clinically relevant cobalt nanoparticles and ions on macrophages in vitro. Biomed. Mater. 2009, 4, 025018. [Google Scholar] [CrossRef] [PubMed]
- Nine, M.J.; Choudhury, D.; Hee, A.C.; Mootanah, R.; Osman, N.A.A. Wear Debris Characterization and Corresponding Biological Response: Artificial Hip and Knee Joints. Materials 2014, 7, 980–1016. [Google Scholar] [CrossRef] [PubMed]
- Sansone, V.; Pagani, D.; Melato, M. The effects on bone cells of metal ions released from orthopaedic implants. A review. Clin. Cases Miner. Bone Metab. 2013, 10, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Baskey, S.J.; Lehoux, E.A.; Catelas, I. Effects of cobalt and chromium ions on lymphocyte migration. J. Orthop. Res. 2017, 35, 916–924. [Google Scholar] [CrossRef] [PubMed]
- Campbell, P.; Ebramzadeh, E.; Nelson, S.; Takamura, K.; De Smet, K.; Amstutz, H.C. Histological features of pseudotumor-like tissues from metal-on-metal hips. Clin. Orthop. Relat. Res. 2010, 468, 2321–2327. [Google Scholar] [CrossRef] [PubMed]
- Smeekes, C.; Cleven, A.H.G.; van der Wal, B.C.H.; Dubois, S.V.; Rouse, R.W.; Ongkiehong, B.F.; Wolterbeek, R.; Nelissen, R.G.H.H. Current Pathologic Scoring Systems for Metal-on-metal THA Revisions are not Reproducible. Clin. Orthop. Relat. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Frigerio, E.; Pigatto, P.D.; Guzzi, G.; Altomare, G. Metal sensitivity in patients with orthopaedic implants: A prospective study. Contact Dermat. 2011, 64, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Münch, H.J.; Jacobsen, S.S.; Olesen, J.T.; Menné, T.; Søballe, K.; Johansen, J.D.; Thyssen, J.P. The association between metal allergy, total knee arthroplasty, and revision: Study based on the Danish Knee Arthroplasty Register. Acta Orthop. 2015, 86, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Ladon, D.; Doherty, A.; Newson, R.; Turner, J.; Bhamra, M.; Case, C.P. Changes in metal levels and chromosome aberrations in the peripheral blood of patients after metal-on-metal hip arthroplasty. J. Arthroplast. 2004, 19 (Suppl. 3), 78–83. [Google Scholar] [CrossRef]
- Ziaee, H.; Daniel, J.; Datta, A.K.; Blunt, S.; McMinn, D.J. Transplacental transfer of cobalt and chromium in patients with metal-on-metal hip arthroplasty: A controlled study. J. Bone Jt. Surg. Br. 2007, 89, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Nikolaou, V.; Petit, A.; Huk, O.; Zukor, D.; Bergeron, S.; Antoniou, J. Semen metal ion levels and sperm quality in patients with metal on metal total hip replacement. J. Bone Jt. Surg. Br. 2011, 93, 130. [Google Scholar]
- Jelnes, J.E.; Knudsen, L.E. Stainless steel welding and semen quality. Reprod. Toxicol. 1988, 2, 213–215. [Google Scholar] [CrossRef]
- Mäkelä, K.T.; Visuri, T.; Pulkkinen, P.; Eskelinen, A.; Remes, V.; Virolainen, P.; Junnila, M.; Pukkala, E. Cancer incidence and cause-specific mortality in patients with metal-on-metal hip replacements in Finland. Acta Orthop. 2014, 85, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.J.; Dieppe, P.; Porter, M.; Blom, A.W. National Joint Registry of England and Wales. Risk of cancer in first seven years after metal-on-metal hip replacement compared with other bearings and general population: Linkage study between the National Joint Registry of England and Wales and hospital episode statistics. BMJ 2012, 344, e2383. [Google Scholar] [PubMed]
- Daniel, J.; Pradhan, C.; Ziaee, H.; Pynsent, P.B.; McMinn, D.J. Results of Birmingham hip resurfacing at 12 to 15 years: A single-surgeon series. Bone Jt. J. 2014, 96-B, 1298–1306. [Google Scholar] [CrossRef] [PubMed]
- Amstutz, H.C.; Le Duff, M.J. Hip resurfacing: History, current status, and future. Hip Int. 2015, 25, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, M.D.; Gross, T.P. Metal-on-metal hip resurfacing in patients younger than 50 years: A retrospective analysis: 1285 cases, 12-year survivorship. J. Orthop. Surg. Res. 2017, 12, 79. [Google Scholar] [CrossRef] [PubMed]
- Aqil, A.; Drabu, R.; Bergmann, J.H.; Masjedi, M.; Manning, V.; Andrews, B.; Muirhead-Allwood, S.; Cobb, J. The gait of patients with one resurfacing and one replacement hip: A single blinded controlled study. Int. Orthop. 2013, 37, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Vendittoli, P.A.; Rivière, C.; Roy, A.G.; Barry, J.; Lusignan, D.; Lavigne, M. Metal-on-metal hip resurfacing compared with 28-mm diameter metal-on-metal total hip replacement: A randomised study with six to nine years’ follow-up. Bone Jt. J. 2013, 95-B, 1464–1473. [Google Scholar] [CrossRef] [PubMed]
- McMinn, D.J.; Snell, K.I.; Daniel, J.; Treacy, R.B.; Pynsent, P.B.; Riley, R.D. Mortality and implant revision rates of hip arthroplasty in patients with osteoarthritis: Registry based cohort study. BMJ 2012, 344, e3319. [Google Scholar] [CrossRef] [PubMed]
- Kendal, A.R.; Arden, N.K.; Carr, A.; Judge, A. Mortality rates at 10 years after metal-on-metal hip resurfacing compared with total hip replacement in England: Retrospective cohort analysis of hospital episode statistics. BMJ 2013, 347, f6549. [Google Scholar] [CrossRef] [PubMed]
- Delaunay, C.P.; Putman, S.; Puliéro, B.; Bégin, M.; Migaud, H.; Bonnomet, F. Cementless Total Hip Arthroplasty With Metasul Bearings Provides Good Results in Active Young Patients: A Concise Followup. Clin. Orthop. Relat. Res. 2016, 474, 2126–2133. [Google Scholar] [CrossRef] [PubMed]
- Scientific Committee on Emerging and Newly Identified Health Risks of the European COmmission DG health and COnsumers. Opinion on the safety of Metal-on-Metal joint replacements with a particular focus on hip implants. In Proceedings of the Opinion Adopted at 7th Plenary of SCENIHR, Luxembourg, 24–25 September 2014. [Google Scholar]
- Food and Drug Administration. FDA 522 Guidance Document. Available online: www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/ucm072564.pdf (accessed on 16 August 2011).
- MHRA Updated Advice Provided in MDA/2012/036, to Assist the Early Detection of Soft Tissue Reactions in Patients Implanted with Metal-on-Metal (MoM) Hip Replacements (MDA/2017/018). Available online: www.gov.uk since (accessed on 29 June 2017).
- Smith&Nephew Statement Regarding BHR System 4th June 2015. Available online: Smith-Nephew.com (accessed on 4 June 2015).
- Hussey, D.K.; McGrory, B.J. Ten-Year Cross-Sectional Study of Mechanically Assisted Crevice Corrosion in 1352 Consecutive Patients With Metal-on-Polyethylene Total Hip Arthroplasty. J. Arthroplast. 2017, 32, 2546–2551. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Radiograph of a Metal-on-Metal (MoM) Hip Resurfacing Arthroplasty (HRA).
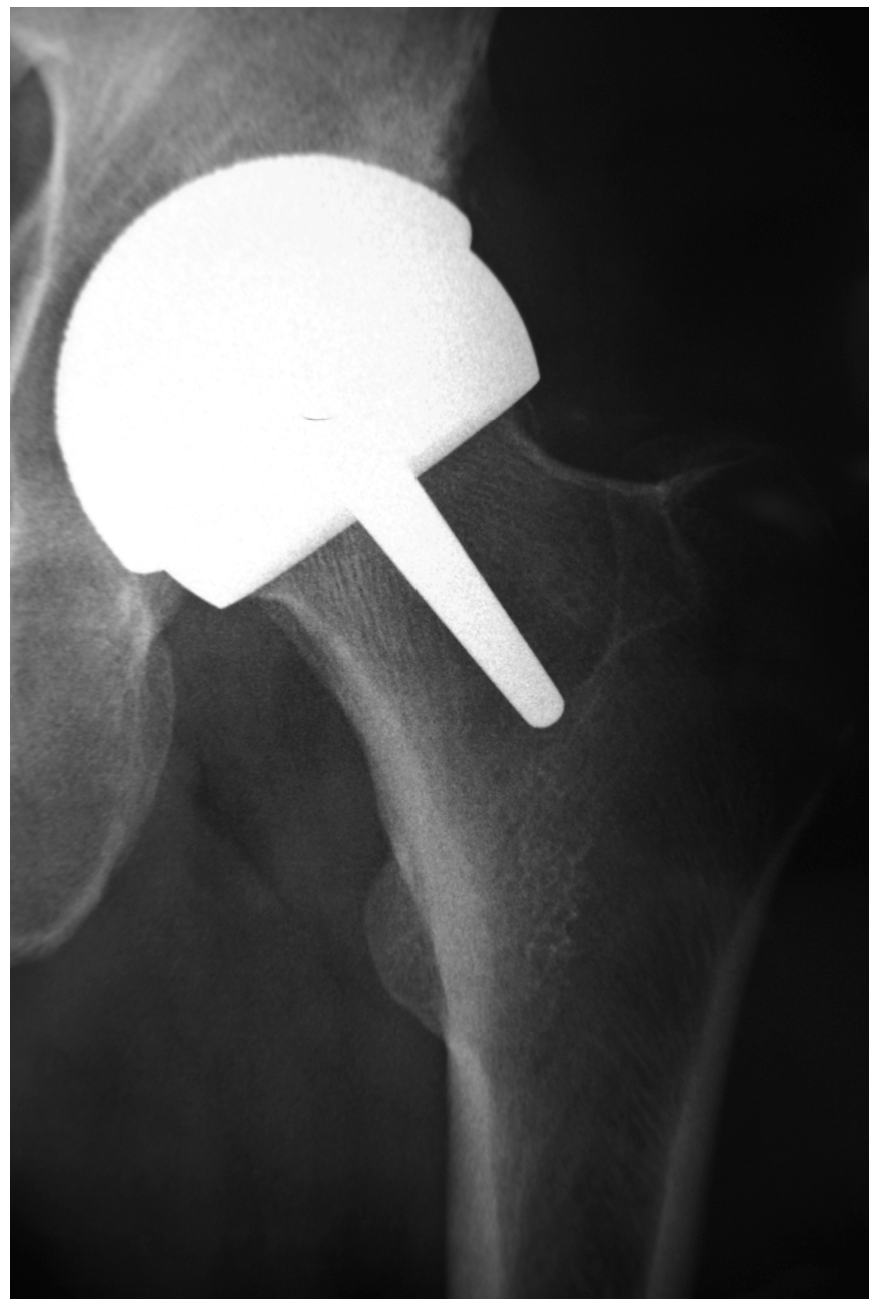
Figure 2.
Early failure of an MoM HRA due to femoral neck fracture.
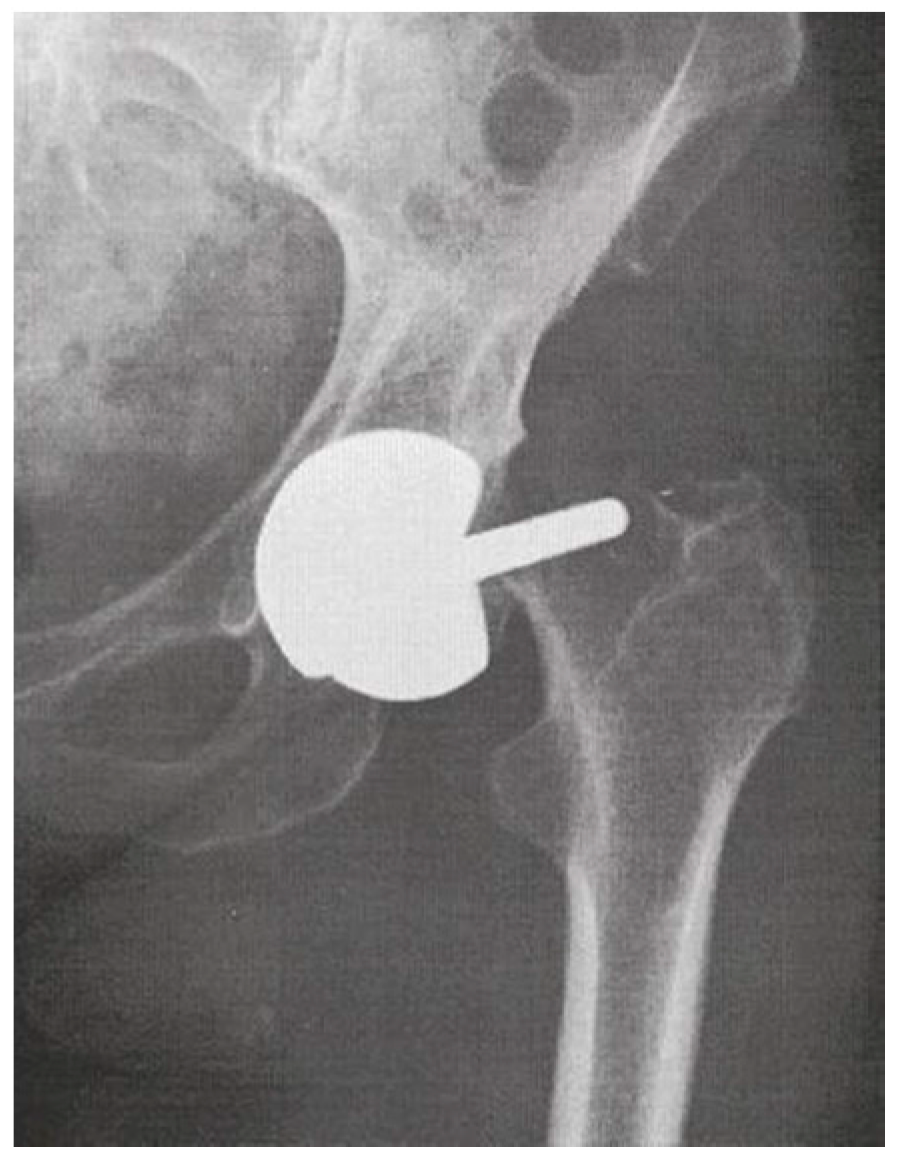
Figure 3.
MoM total hip arthroplasty with large diameter femoral head.

Figure 4.
Subtended articular arc (a) (coverage angle) of a metal-on-metal articulation.
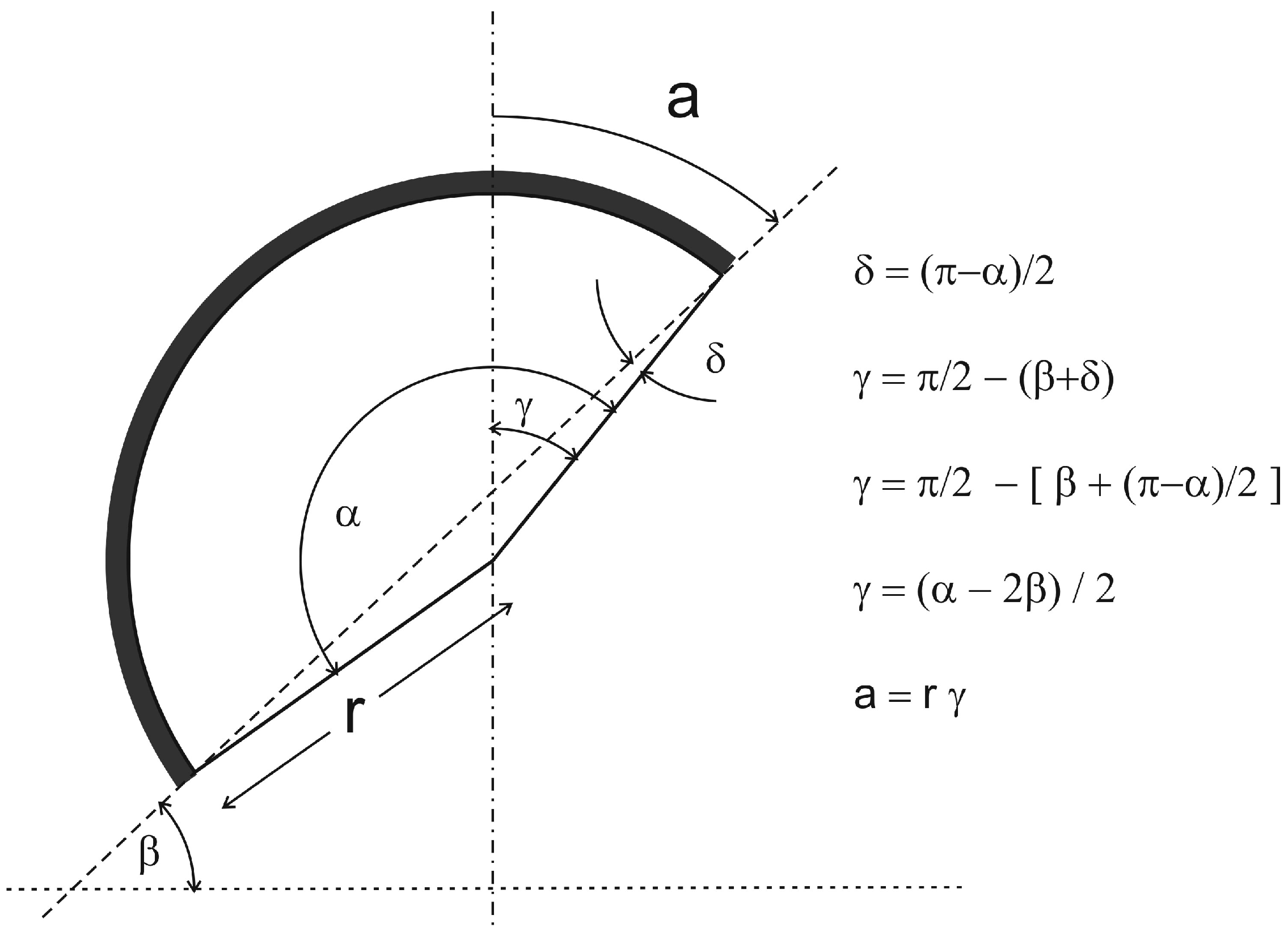
Figure 5.
The clearance is difference in radius (radial clearance) or in diameter (diametrical clearance) between the acetabular (white arrow) and the femoral (black arrow) bearing surfaces. Lubrication of the articulation is achieved by fluid being entrapped in that inter-bearing space.
Figure 5.
The clearance is difference in radius (radial clearance) or in diameter (diametrical clearance) between the acetabular (white arrow) and the femoral (black arrow) bearing surfaces. Lubrication of the articulation is achieved by fluid being entrapped in that inter-bearing space.
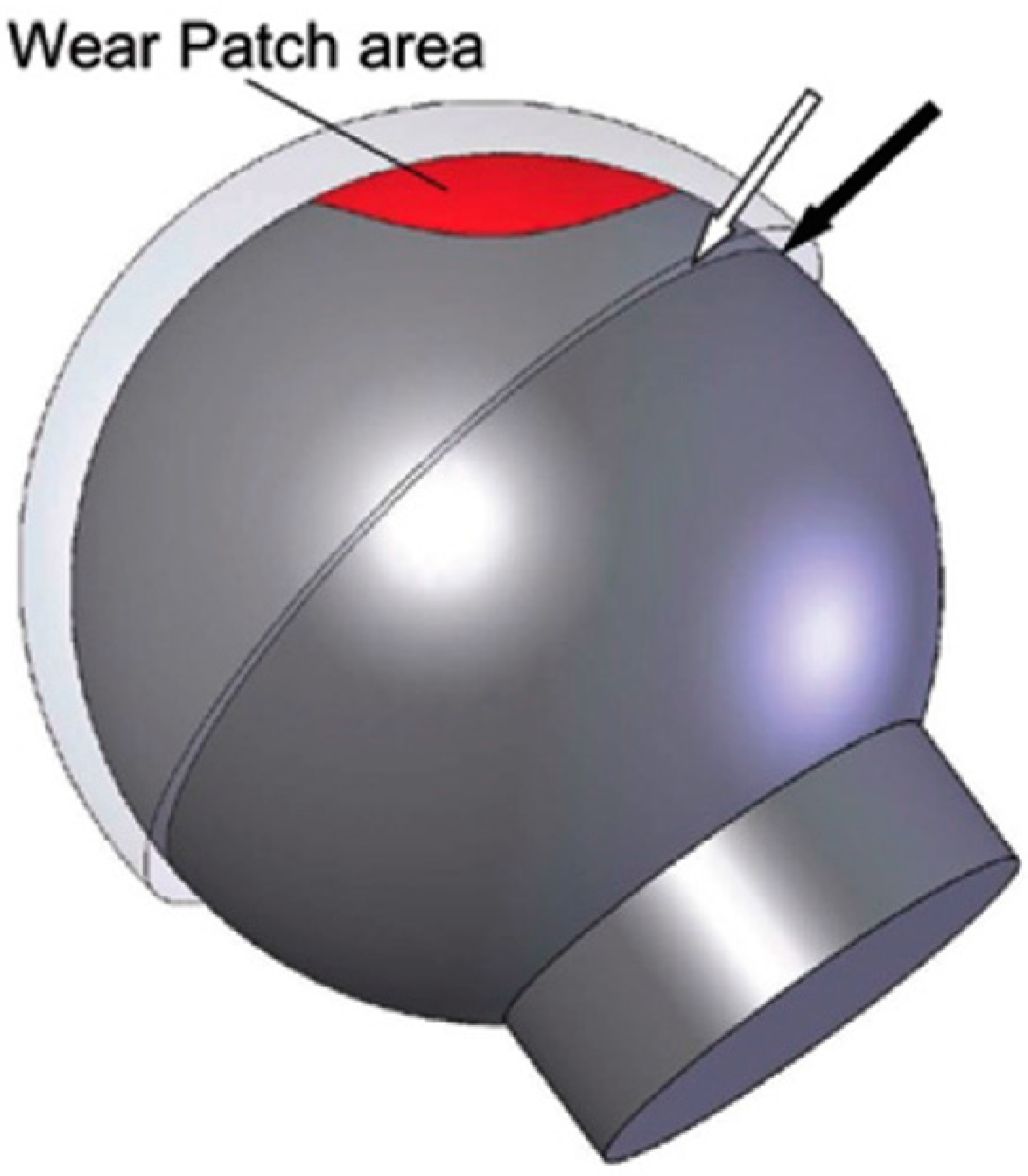
Figure 6.
Edge loading associated with small coverage angle, steep cup position and/or small size.

Figure 7.
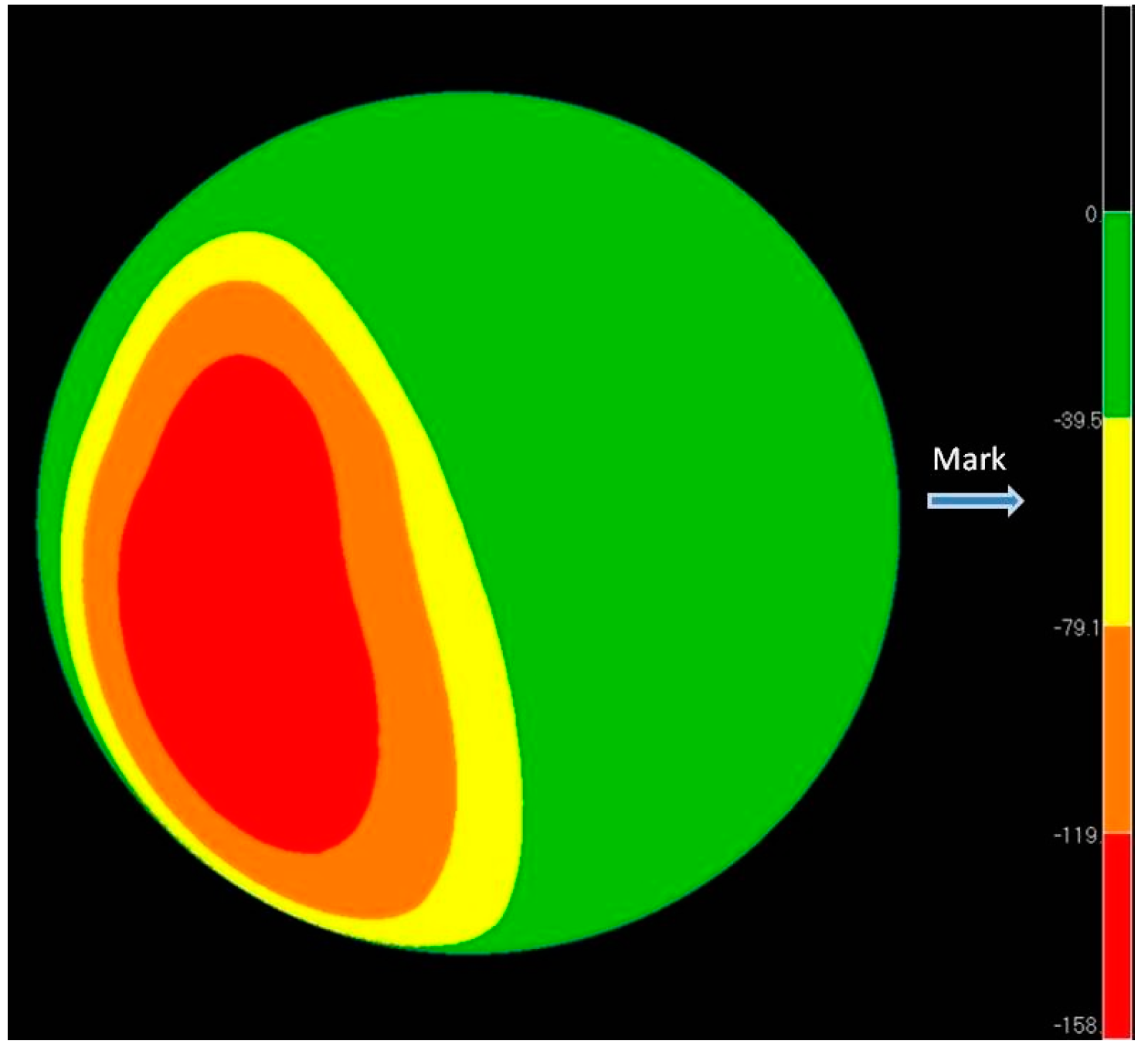
Retrieval of high wear Birmingham Hip Resurfacing (BHR) HRA, head size 52 mm, implanted in a 59-year-old male with primary osteoarthritis. This was revised after 58 months for cup malpositioning (EBRA measurement inclination 57°; anteversion 51°) associated with very high metal ions (Cr: 25.1 µg/L; Co 72.4 µg/L) and a soft tissue mass. This coordinate measuring machine derived wear depth map shows high wear due to edge loading, (maximum 158 microns).
Figure 7.
Retrieval of high wear Birmingham Hip Resurfacing (BHR) HRA, head size 52 mm, implanted in a 59-year-old male with primary osteoarthritis. This was revised after 58 months for cup malpositioning (EBRA measurement inclination 57°; anteversion 51°) associated with very high metal ions (Cr: 25.1 µg/L; Co 72.4 µg/L) and a soft tissue mass. This coordinate measuring machine derived wear depth map shows high wear due to edge loading, (maximum 158 microns).
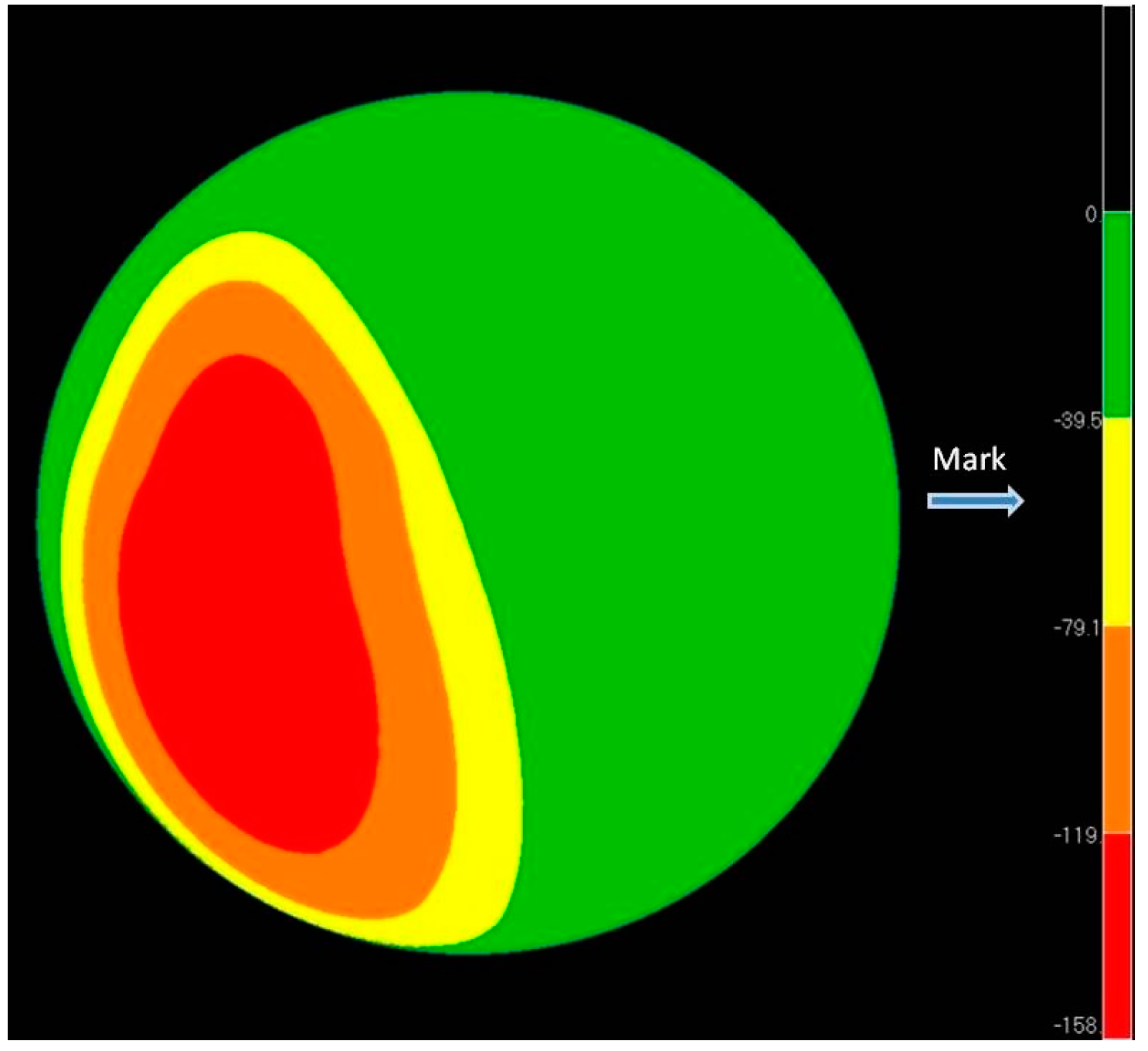
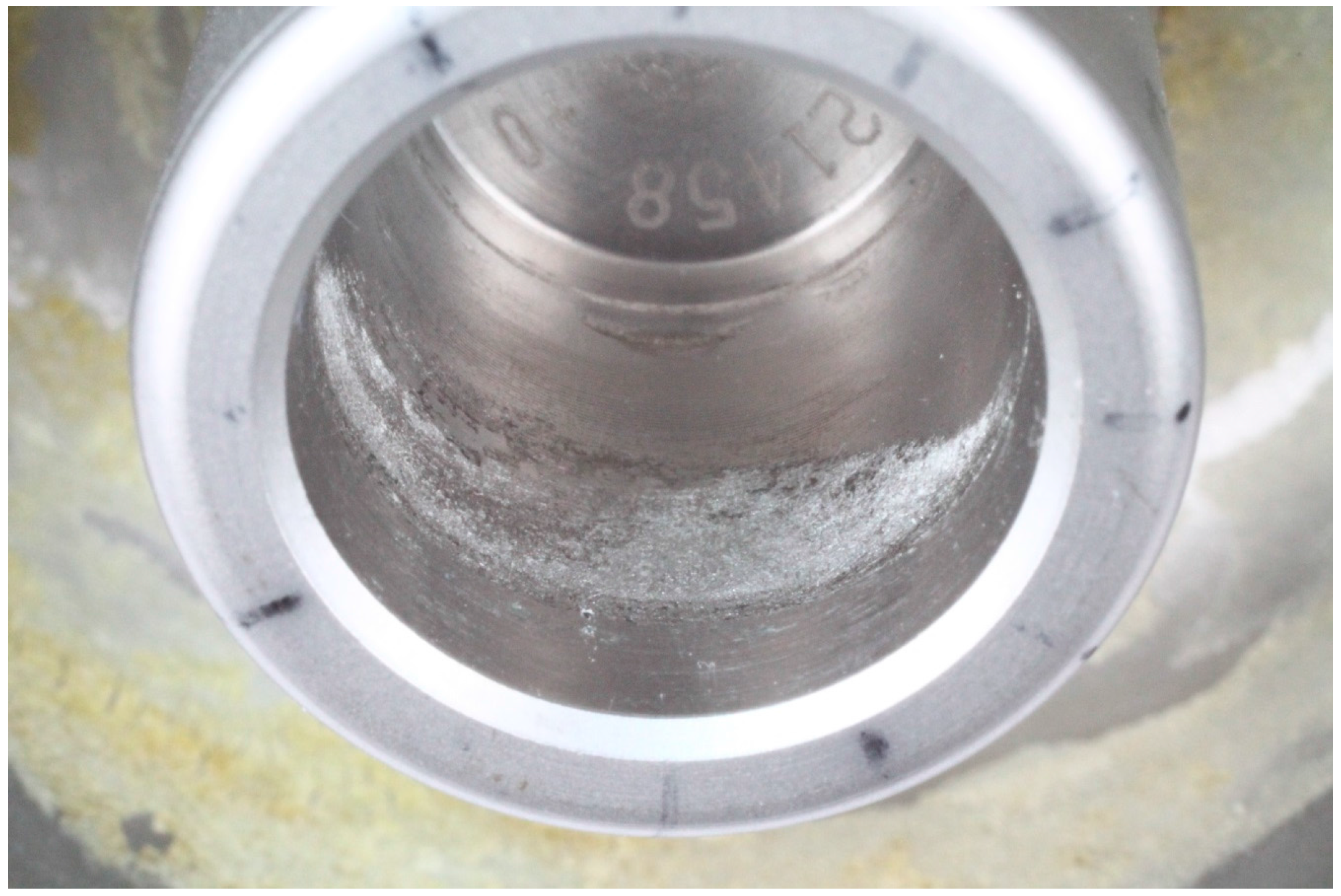
Figure 8.
Crevice corrosion inside taper of large diameter femoral head.
© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Van Der Straeten, C. Current Insights Regarding Metal-on-Metal Bearings for Hip Arthroplasty. Lubricants 2017, 5, 37. https://doi.org/10.3390/lubricants5030037
AMA Style
Van Der Straeten C. Current Insights Regarding Metal-on-Metal Bearings for Hip Arthroplasty. Lubricants. 2017; 5(3):37. https://doi.org/10.3390/lubricants5030037
Chicago/Turabian StyleVan Der Straeten, Catherine. 2017. "Current Insights Regarding Metal-on-Metal Bearings for Hip Arthroplasty" Lubricants 5, no. 3: 37. https://doi.org/10.3390/lubricants5030037
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.