Current Status and Future Suggestions for Improving the Pharm. D Curriculum towards Clinical Pharmacy Practice in Pakistan

 ,
,
Abstract
:1. Introduction
2. Methodology
2.1. Study Design and Study Period
2.2. Study Population and Setting
2.3. Data Collection
2.4. Data Analysis
3. Results
4. Discussion
- (1)
- (2)
- The Pharm. D degree was started without any planning [2].
- (3)
- “The Pharm. D degree is just a tool to help students qualify for job opportunities in Gulf countries, as well as to make the so-called “doctors” eligible to appear for the license examination in the United States or elsewhere” [13].
- (4)
- Whether the curriculum, without any proper clinical attachment, with just a couple of visits to hospitals, would serve the purpose is a doubtful issue [14].
- (5)
- In Pakistan, the hospital pharmacy/clinical pharmacy is at a preliminary level [12], etc.
- as the “International Pharmaceutical Federation (FIP) Global Competency Framework” suggests that pharmacy professionals must be ready in terms of their professional knowledge, skills, efficiency and availability for placements at international sites [1], we suggest that our pharmacy council should encourage the provision of a “one year paid residency program” for pharmacy students, and that the residency program should be coordinated by a residency program director (RPD), residency activities coordinators, chief resident, and/or department chair or director. In addition to the enhancement of expertise, this experience could serve to increase the students’ respect towards national, local and ethnic identities, increasing professional harmony, as well.
- Electives should be given in all disciplines of clinical pharmacy and electives should be divided into clinical and industrial categories. This will enhance their ability to integrate knowledge towards pharmacy practice.
- The pharmacy degree should be divided into a two-phase degree program, i.e., Pre-Pharmacy and Pharm. D. The Pre-Pharmacy degree should be of two or three years, and should contain all the basic subjects of formulation, and the courses needed for industry. Whereas, the Pharm. D should be more practically focused towards public health, and contain electives, an apprenticeship and internship program, and have more therapeutic subjects. As a result, depending upon the aptitude of students, the choice of degrees can be varied.
- The curriculum should place more emphasis on clinical aspects by adding therapeutics, clinical pharmacology, molecular pharmacology, clinical microbiology and pharmacogenetics as separate disciplines, rather than mere topics. In this way, students can compete internationally, having been equipped with the necessary applied knowledge following the standards.
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References and Note
- Hawboldt, J.; Nash, R.; Patrick, B.F. How Two Small Pharmacy Schools’ Competency Standards Compare with an International Competency Framework and How Well These Schools Prepare Students for International Placements. Pharmacy 2017, 5, 14. [Google Scholar] [CrossRef]
- Jamshed, S.; Babar, Z.U.D.; Masood, I. The Pharm. D Degree in Developing Countries. Am. J. Pharm. Educ. 2007, 71, 125. [Google Scholar] [CrossRef] [PubMed]
- Azhar, S.; Hassali, M.A.; Izham, M.; Ibrahim, M.; Ahmad, M.; Masood, I.; Shafie, A.A. The role of pharmacists in developing countries: The current scenario in Pakistan. Hum. Resour. Health 2009, 7, 54. [Google Scholar] [CrossRef] [PubMed]
- Hadi, M.A.; Hughes, J. Broader Perspective Needed on the Pharm. D Degree in Pakistan. Am. J. Pharm. Educ. 2009, 73, 114. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.; Futter, B. Pharm. D or Needs Based Education: Which Comes First? Am. J. Pharm. Educ. 2009, 73, 92. [Google Scholar] [CrossRef] [PubMed]
- Pharmacy Council of Pakistan. Revised Pharm. D Curriculum Final 2013. Available online: http://www.pharmacycouncil.org.pk/ (accessed on 9 September 2013).
- McLaughlin, J.E.; Dean, M.J.; Mumper, R.J.; Blouin, R.A.; Roth, M.T. A Roadmap for Educational Research in Pharmacy. Am. J. Pharm. Educ. 2013, 77, 218. [Google Scholar] [CrossRef] [PubMed]
- Alsharif, N.Z. Globalization of Pharmacy Education: What is Needed? Am. J. Pharm. Educ. 2012, 76, 77. [Google Scholar] [CrossRef] [PubMed]
- Economic Adviser’s Wing, Finance Division, Government of Pakistan, Islamabad. Highlights of Pakistan Economic Survey 2014–2015. PCPPI—2551(2015) Fin.Div-2-6-2015-500.
- Ahmed, V.; Batool, S. India-Pakistan Trade: A Case Study of the Pharmaceutical Sector. In India-Pakistan Trade Normalisation; Springer: Berlin, Germany, 2014. [Google Scholar]
- Zaman, K. Review of Pakistan Pharmaceutical Industry: SWOT Analysis. Available online: http://www.ojs.excelingtech.co.uk/index.php/IJBIT/article/view/30 (accessed on 19 July 2017).
- Khan, T.M. Challenges to pharmacy and pharmacy practice in Pakistan. Australas. Med. J. 2011, 4, 230–235. [Google Scholar] [CrossRef]
- Jamshed, S.; Baber, Z.U.D.; Izham, M.; Ibrahim, M. Pharm. D in Pakistan: A Tag or a Degree? Am. J. Pharm. Educ. 2009, 73, 13. [Google Scholar] [PubMed]
- Pakistan Pharmaceutical Industry analysis of Pakistan. Available online: https://www.scribd.com/doc/32476064/Pharamaceutical-Industry-Analysis-of-Pakistan (accessed on 5 March 2014).

{kind=link}
| Descriptive Statistics | |||
|---|---|---|---|
| Questions | N | Mean | Std. Deviation |
| 1-year paid residency should be provided in a health care sector | 354 | 4.47 | 0.821 |
| The pharmacy curriculum should place more emphasis on clinical aspects | 354 | 4.36 | 0.831 |
| The pathology course is not enough for clinical practice | 354 | 4.24 | 0.936 |
| Electives should be divided into industrial and clinical categories | 354 | 4.24 | 0.870 |
| Electives should be provided in all disciplines of clinical sciences | 354 | 4.08 | 0.887 |
| Physical assessment, neuropsychiatric therapeutics, infectious disease therapeutics, poison management & drug abuse, and cardiopulmonary therapeutics should all be included as separate disciplines | 354 | 4.08 | 0.966 |
| Current pharmacy curriculum does not meet the international standards of pharmacy practice | 354 | 4.03 | 0.918 |
| Pharmacogenetics should be included as a separate course | 354 | 3.92 | 0.965 |
| The ongoing pharmacy curriculum has too many repetitions | 354 | 3.88 | 0.937 |
| The curriculum for basic medical sciences is not sufficient | 354 | 3.86 | 0.902 |
| The medical microbiology and immunological basis for therapy should be separated from pharmaceutical microbiology as a discipline | 354 | 3.86 | 1.032 |
| The discipline of pharmacognosy can be more concise, and clinical pharmacognosy can be added | 354 | 3.79 | 1.004 |
| Clinical biochemistry should be included as a separate discipline | 354 | 3.65 | 1.060 |
| I am satisfied with the changes made in the Pharm. D curriculum | 354 | 3.46 | 1.072 |
| Valid N (list wise) | 354 | ||
| Descriptive Statistics | |||
|---|---|---|---|
| Questions | N | Mean | Std. Deviation |
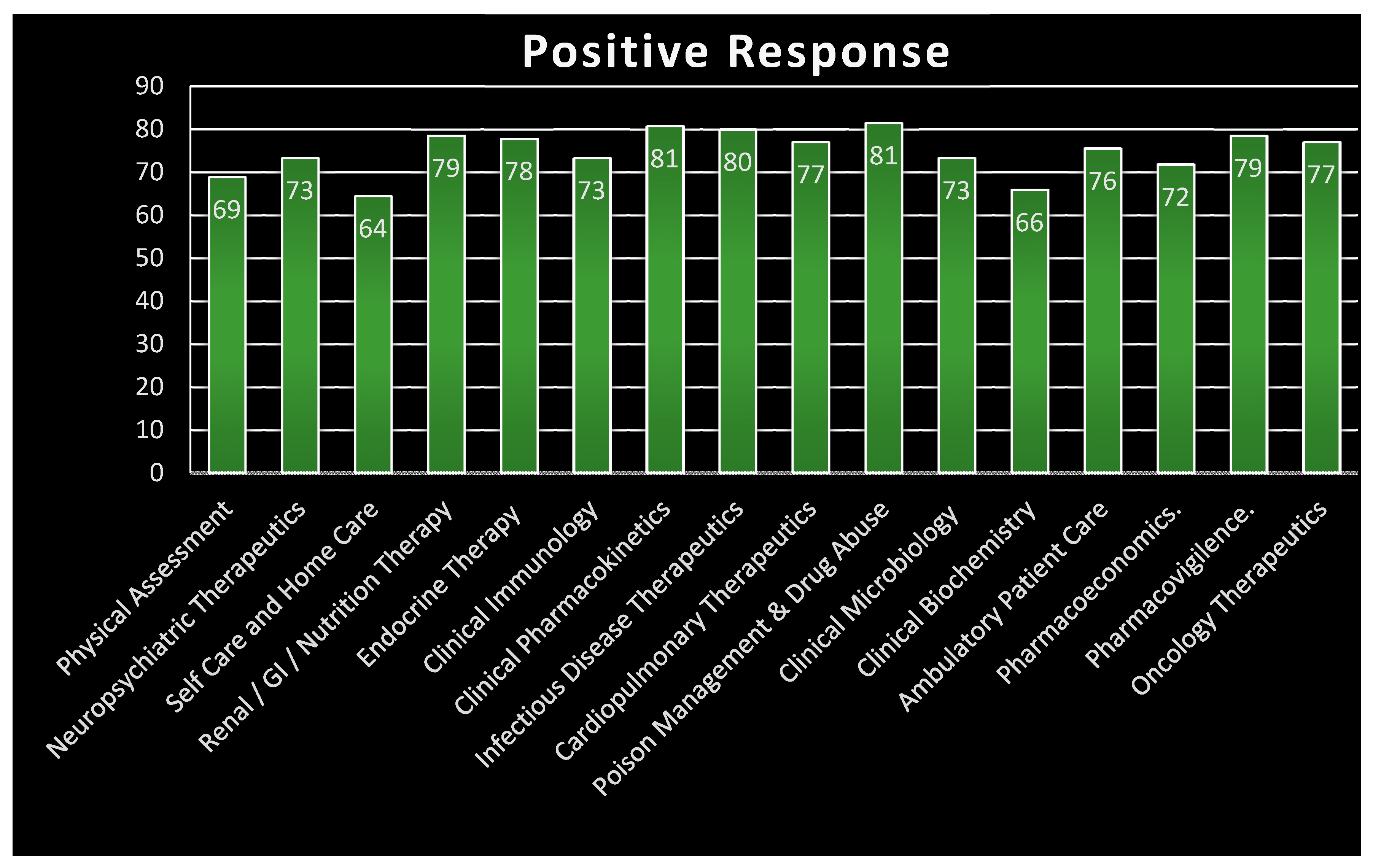
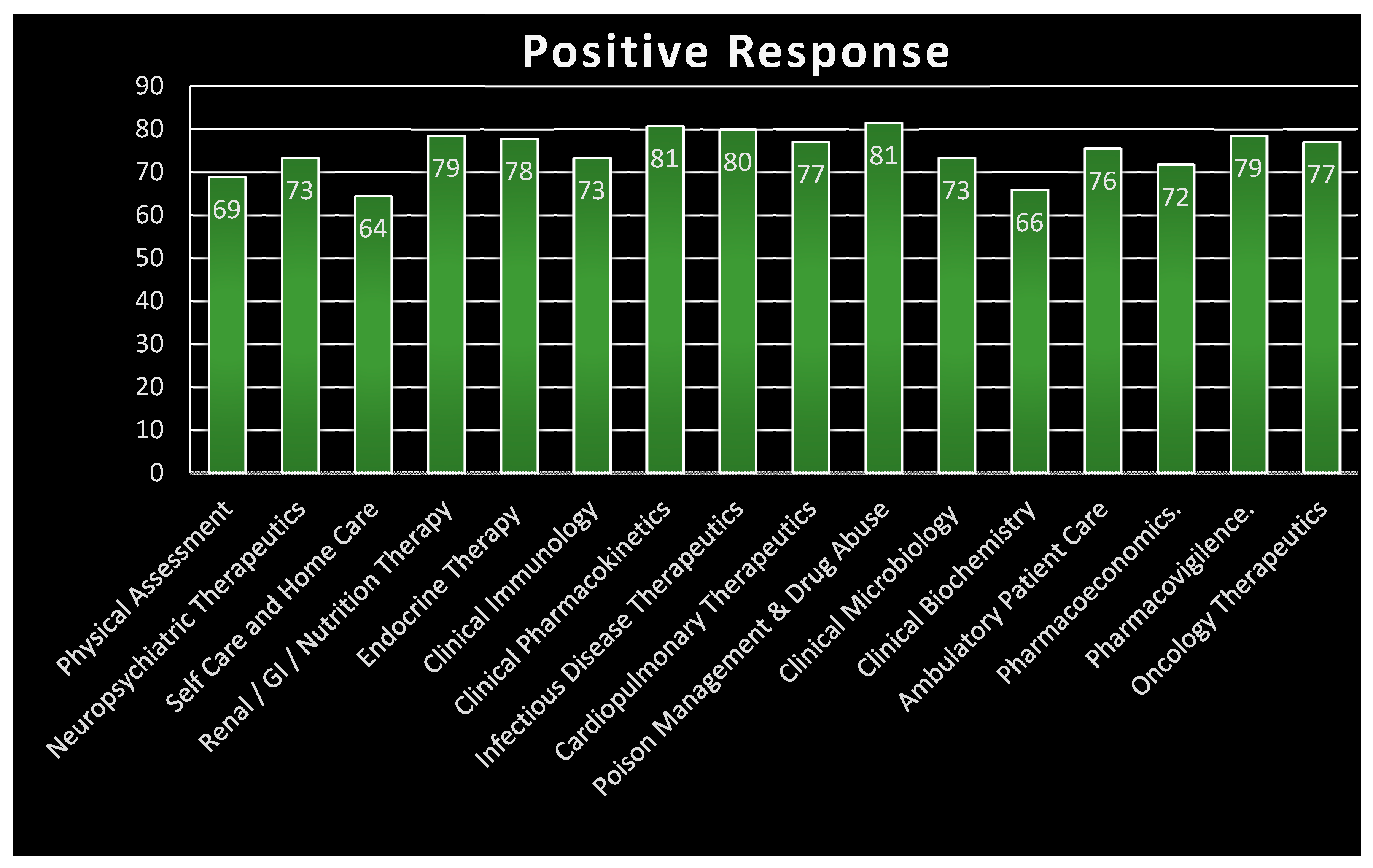
| The Pharm. D degree should include a paid residency program to facilitate hospital, clinical and compounding pharmacy | 135 | 4.37 | 0.826 |
| The Pharm. D degree should be more practical and clinically oriented | 135 | 4.33 | 0.938 |
| Pharm. D degree in Pakistan should be both clinically and industrially oriented, according to the needs of the Pakistani people | 135 | 4.32 | 0.869 |
| Elective on Poison management & drug abuse must be provided | 135 | 4.27 | 0.885 |
| The Program should be run by the residency program director (RPD), residency activities coordinator, chief resident, or department chair or director | 135 | 4.22 | 0.835 |
| Elective on clinical pharmacokinetics and laboratory data interpretation must be added | 135 | 4.16 | 0.948 |
| Elective on infectious disease therapeutics (airborne/waterborne/blood borne) must be added | 135 | 4.16 | 0.979 |
| Pharm. D should include a practical apprenticeship in last two years in different wards of tertiary health care | 135 | 4.13 | 1.018 |
| Elective on pharmacovigilance must be added | 135 | 4.06 | 0.944 |
| Elective on oncology therapeutics must be added | 135 | 4.05 | 0.964 |
| Electives on Endocrine therapy & special patient population groups (such as infants, paeds, geriatrics, pregnancy, immunocompromised and renal and hepatic insufficient patients) must be provided | 135 | 4.05 | 1.002 |
| Electives on Renal/GI/Nutrition therapy should be provided | 135 | 4.04 | 0.988 |
| Elective on cardiopulmonary therapeutics should be provided | 135 | 4.04 | 0.988 |
| Ambulatory patient care can be added as an elective | 135 | 4.01 | 1.018 |
| Electives should be provided in all the disciplines during final year. | 135 | 3.99 | 1.007 |
| Electives on pharmacogenetics and pharmacogenomics should be provided | 135 | 3.95 | 0.949 |
| Clinical pharmacy should not be included as a subject, rather it should be introduced as a discipline or department | 135 | 3.95 | 1.115 |
| The Pharm. D curriculum in Pakistan does not meet the international standards of practice | 135 | 3.93 | 1.009 |
| Elective on pharmacoeconomics should be provided | 135 | 3.91 | 0.934 |
| Clinical immunology/Hematology can be added as topics | 135 | 3.90 | 0.984 |
| Clinical microbiology can be added as topics | 135 | 3.90 | 0.995 |
| Electives on neuropsychiatric therapeutics must be provided | 135 | 3.89 | 0.975 |
| Physical assessment/Patient and family counseling can be added | 135 | 3.85 | 1.062 |
| Clinical biochemistry can be added as a subject | 135 | 3.79 | 1.010 |
| Self care and home care can also be added as subject | 135 | 3.77 | 1.029 |
| The Pre-Pharmacy includes all the basic subjects and industrial subjects necessary for a pharmacist to work in industry | 135 | 3.33 | 1.112 |
| The basic Pharm. D degree should be divided into Pre-Pharm. D and professional Pharm. D | 135 | 3.08 | 1.191 |
| Valid N (listwise) | 135 | ||
| The basic degree of Pharm. D should be divided into Pre-Pharm. D and Professional Pharm. D | Valid Response | Frequency | Percent | Valid Percent |
| Negative Response | 49 | 36.3 | 36.2963 | |
| Neutral | 34 | 25.2 | 25.18519 | |
| Positive Response | 52 | 38.5 | 38.51852 | |
| Total | 135 | 100 | 100 | |
| The Pre-Pharmacy Includes all the basic subjects and industrial subjects necessary for a pharmacist to work in industry | Valid Response | Frequency | Percent | Valid Percent |
| Negative Response | 37 | 27 | 27.40741 | |
| Neutral | 33 | 24 | 24.44444 | |
| Positive Response | 65 | 48 | 48.14815 | |
| Total | 135 | 100 | 100 | |
| Clinical Pharmacy should not be included as a subject rather it is introduced as a discipline or department | Valid Response | Frequency | Percent | Valid Percent |
| Negative Response | 22 | 16.2963 | 16.2963 | |
| Neutral | 18 | 13.33333 | 13.33333 | |
| Positive Response | 95 | 70.37037 | 70.37037 | |
| Total | 135 | 100 | 100 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malhi, S.M.; Raza, H.; Ajmal, K.; Shamim, S.; Ata, S.; Farooq, S.; Sharib, S.M.; Muntaha, S.-u. Current Status and Future Suggestions for Improving the Pharm. D Curriculum towards Clinical Pharmacy Practice in Pakistan. Pharmacy 2017, 5, 46. https://doi.org/10.3390/pharmacy5030046
Malhi SM, Raza H, Ajmal K, Shamim S, Ata S, Farooq S, Sharib SM, Muntaha S-u. Current Status and Future Suggestions for Improving the Pharm. D Curriculum towards Clinical Pharmacy Practice in Pakistan. Pharmacy. 2017; 5(3):46. https://doi.org/10.3390/pharmacy5030046
Chicago/Turabian StyleMalhi, Saima Mahmood, Hassan Raza, Kiran Ajmal, Sumbul Shamim, Saniya Ata, Salman Farooq, Syed Muhammad Sharib, and Sidrat-ul Muntaha. 2017. "Current Status and Future Suggestions for Improving the Pharm. D Curriculum towards Clinical Pharmacy Practice in Pakistan" Pharmacy 5, no. 3: 46. https://doi.org/10.3390/pharmacy5030046