Pharmacists as Interprofessional Collaborators and Leaders through Clinical Pathways



1
King Abdullah International Medical Research Center, King Saud bin Abdulaziz University for Health Sciences, Pharmaceutical Care Department, King Khalid Hospital, Ministry of National Guard Health Affairs, Jeddah 21423, Saudi Arabia
2
Trillium Health Partners, Credit Valley Hospital, Mississauga, ON L5M 2N1, Canada
3
King Abdullah International Medical Research Center, King Saud bin Abdulaziz University for Health Sciences, Pharmaceutical Care Department, Prince Mohammed Bin Abdulaziz Hospital, Ministry of National Guard Health Affairs, Madinah 41511, Saudi Arabia
4
National University of Medical Sciences, The Mall, Rawalpindi 44000, Pakistan
*
Author to whom correspondence should be addressed.
Pharmacy 2018, 6(1), 24; https://doi.org/10.3390/pharmacy6010024
Submission received: 16 February 2018
/
Revised: 8 March 2018
/
Accepted: 14 March 2018
/
Published: 16 March 2018
(This article belongs to the Special Issue Interprofessional Working and Collaborative Practice)
Abstract
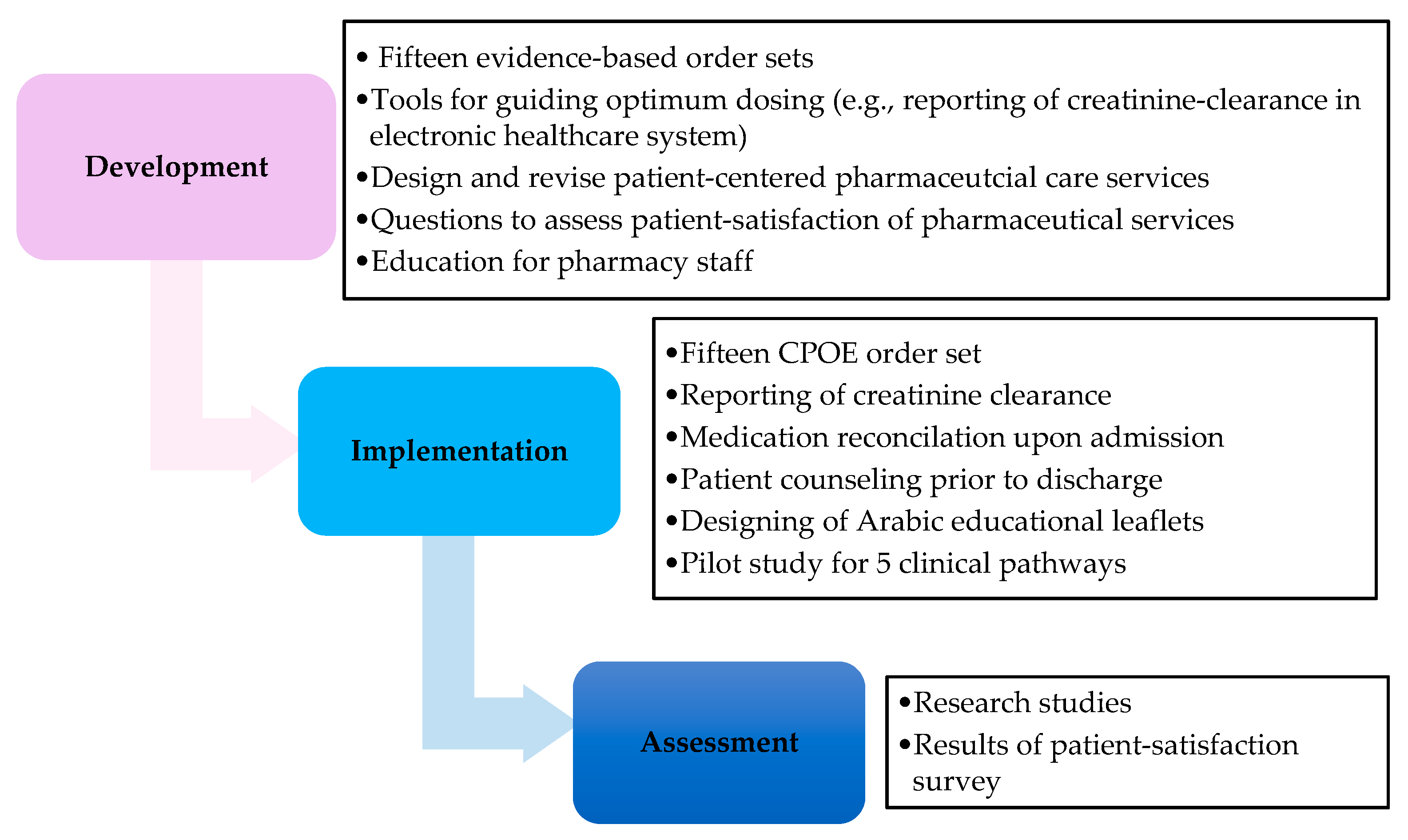
:Pharmacists possess pivotal competencies and expertise in developing clinical pathways (CPs). We present a tertiary care facility experience of pharmacists vis-a-vis interprofessional collaboration for designing and implementing CPs. We participated in the development of CPs as leading members of a collaborative team of healthcare professionals. We reviewed literature, aligning it with hospital formulary and institutional standards, and participated in weekly team meetings for six months. Several tools and services were adapted to guide prescribing and standardization of care through time-bound order sets. Fifteen CPs leading to admissions in medical wards were developed and integrated into Computerized Prescriber Order Entry (CPOE) sets. Tools and services included (1) reporting of creatinine clearance to guide optimum dosing; (2) advisory flags for dosing and infusion rates; (3) piloting of medication reconciliation and counseling services before discharge were initiated; (4) Arabic drug leaflets were designed to educate patients; and (5) five CPs were included in pragmatic randomized control trials with a clinical pharmacist as co-investigator. Clinical pharmacists conducted continuous orientation to various healthcare professionals throughout the process. CPs provide unique opportunities for establishing and evaluating patient-centered pharmaceutical services and allow clinical pharmacists to demonstrate interprofessional leadership in collaboration with multidisciplinary teams.
1. Introduction
Pharmacists are pharmacotherapy experts, and possess pivotal skills which qualify them for playing active roles in the process of designing and application of clinical pathways (CPs) [1,2]. Literature has consistently reported that CPs can be differentiated from guidelines [3,4] in that CPs are time-bound patient care plans which aim to improve the quality of patient-care and optimize utilization of institutional resources [5,6].
The introduction of CPs in medical institutions was a result of the paradigm shift in the healthcare system from the quantitative aspect to focus on the quality of care and target patient-centered outcomes [7]. Additionally, the designing of CPs requires the presence of a dedicated team of multidisciplinary healthcare professionals who work collaboratively to develop evidence-based and patient-oriented pathways for high-volume, high-risk, and/or high-cost diagnoses [5,8].
A systematic review composed of twenty-seven studies that included 11,398 participants reported that CPs reduced in-hospital complications and increased the rate of documentation of the staff, but authors were not able to poll results for length of stay (LOS) [9]. Another systematic review has demonstrated that CPs had a significant decline in LOS in 12 out of 16 studies analyzed, with a weighted mean difference of −2.5 days for CPs vs. −0.8 days for the standard of care, and 4 out of 6 studies showed a decline in the costs for CPs [10]. However, the majority of CPs studied were in the surgical setting, reported high heterogeneity for LOS, and the effectiveness of CPs remained uncertain [10]. Likewise, the Department of Medicine in our Joint Commission International (JCI) accredited institution aimed to design CPs and to answer the question of the utility of CPs to improve the flow of patients and medical care across multiple medical diagnoses.
The American College of Clinical Pharmacists (ACCP) encourages pharmacists to embrace CPs as opportunities to deliver multifaceted pharmaceutical care [11]. Additionally, the American Society of Health-System Pharmacists (ASHP) provides clear guidelines on the responsibilities of pharmacists in the development, implementation, and assessment of CPs [12]. Furthermore, both the ACCP and ASHP have identified CPs as tools for pharmacists to provide cost-effective patient care plans, integrate pharmaceutical services, institutional culture, and partake leadership position in the development and implementation of the process [12,13].
To date, the literature describing a practice-based prototype of how pharmacists were engaged in the designing and the application of CPs is scarce. Therefore, we aim to describe our experience in the development, implementation, and assessment of CPs as a model of interprofessional collaboration in improving patient-centered outcomes.
2. Materials and Methods
2.1. Development of Pathway Team and Pharmacy Team
The Department of Medicine at King Abdulaziz Medical City, Jeddah, Saudi Arabia invited various healthcare professionals in 2011 to formulate a team composed of physicians, nurses, pharmacists, quality specialists, dietitians, social workers, discharge planning, primary health care physicians, and patient educators. The objective of the interprofessional collaborative team was to provide a holistic approach in designing evidence-based and patient-centered pathways. CPs were defined as time-bound plans to deliver patient care from the admission till the discharge day by all healthcare professionals for specific medical diagnoses.
In response to the invitation, Pharmaceutical Care Department designated a team of pharmacists to provide strategic planning for the participation of the pharmacy and collaboration with the pathway team. The pharmacy team included internal medicine clinical pharmacists who are Board Certified Pharmacotherapy Specialists, inpatient, IV admixture team, and clinical pharmacy supervisors. Additionally, a clinical pharmacist was assigned as a pharmacy coordinator to harmonize the perspectives of the pharmacy team in synchrony with the vision of the pathway team.
2.2. Perspectives of the Pharmacy Team
The pharmacy team set up the following goals and perspectives of pharmaceutical care services as detailed in Table 1.
2.3. The Development Phase
2.3.1. Order Sets
The pathway team targeted the fifteen most frequent admitting diagnoses in medical wards for designing CPs. The development phase was carried out over a period of 6 months. The coordinating clinical pharmacist conducted an evidence-based literature review, designed order sets for each medical diagnosis, and participated in discussions and appraisal of evidence with members of the pathway team and specialty physicians on a regular weekly basis. Furthermore, order sets for each CP were reviewed by the pharmacy team for feasibility of implementation and suggested changes were communicated back to pathway team through the coordinating clinical pharmacist. The order sets included cost-effective therapeutic plans on a daily basis during the hospital stay for each medical diagnosis, and were designed to comply with safety measures for prescribing according to the Institute of Safe Medication Practice for standard order sets [15].
2.3.2. Patient-Centered Pharmaceutical Care Services
We aimed to conduct medication reconciliation by pharmacists in collaboration with physicians based on Best Possible Medication History (BPMH) [16], to optimize patient safety upon transition of care [17]. Additionally, we redesigned our counseling team to provide patient counseling based on Indian Health Services counseling technique [18], and ASHP standards [19]. Furthermore, we designed educational leaflets in the Arabic language to enhance the education of patients during counseling before discharge. Subsequently, we trained our pharmacy staff working in the inpatient and to take-home medications using role-playing sessions to standardize their performance and provide consistent practical experience for patient-centered services. Both services of medication reconciliation and counseling were carried out during working days only, and involved designated pharmacy personnel.
2.3.3. Tools
We coordinated the integration of the reporting of creatinine clearance in the electronic healthcare system after several meetings with Nephrology team as the major stakeholders and informatics technology. We aimed to facilitate the assessment of kidney function to guide optimum drug dosing for renal patients along with order sets, which served as a clinical decision support system for healthcare providers [20,21]. In addition, we incorporated advisory flags in the order sets for maximum infusion rates and dosing for medications based on the therapeutic indications and special clinical situations for each CPs. Furthermore, we activated the documentation of the therapeutic interventions by pharmacists in the electronic medical records. Finally, detailed information based on the interview during counseling and medication reconciliation was documented to improve the communication process between pharmacists and other healthcare professionals, thus facilitating holistic patient care.
2.3.4. Research Opportunities
The Department of Medicine aimed to conduct a study to assess the effectiveness of CPs through a Collaborative Healthcare Approach in Monitoring Patient-centered outcomes through Pathways (CHAMP-Path) studies. These are pragmatic, randomized, single-blinded studies comparing five CPs vs usual care to reduce the length of stay and improve patient-centered outcomes. Clinical pharmacists with research certification were invited to participate in the study as leading co-investigators to revise and submit the proposal of the study to the Institutional Review Board (IRB) for approval. Details for the method of the CHAMP-Path study have been reported [22]. The pharmacy was responsible for allocation of the study participants. Additionally, the study included a survey to assess the level of patient satisfaction with the services provided by all healthcare professionals. We designed five questions as a part of the survey to assess the perceptions of patients towards pharmaceutical care services, which are included in Table 2.
Statistical Analyses
Survey responses were presented as proportions and 95% Confidence interval. STATA 2014 (StataCorp LLC, College Station, TX, USA) was used for statistical analysis.
Ethics
The CHAMP-Path study received IRB approval by King Abdullah International Medical Research Center ((RC 10/134/J) in October 2011. Informed consents were obtained for eligible participants.
3. Results
3.1. Implementation
3.1.1. Order Sets
Fifteen (100%) CPs were developed in collaboration with the pathway team, including acute kidney injury, venous thromboembolism, community-acquired pneumonia, asthma, adult left ventricular heart failure, chronic kidney injury, upper gastro-intestinal bleeding, ischemic stroke, hepatic encephalopathy, generalized seizures, palliative care, acute coronary syndrome, meningitis, diabetic ketoacidosis, and hyperosmolar hyperglycemia.
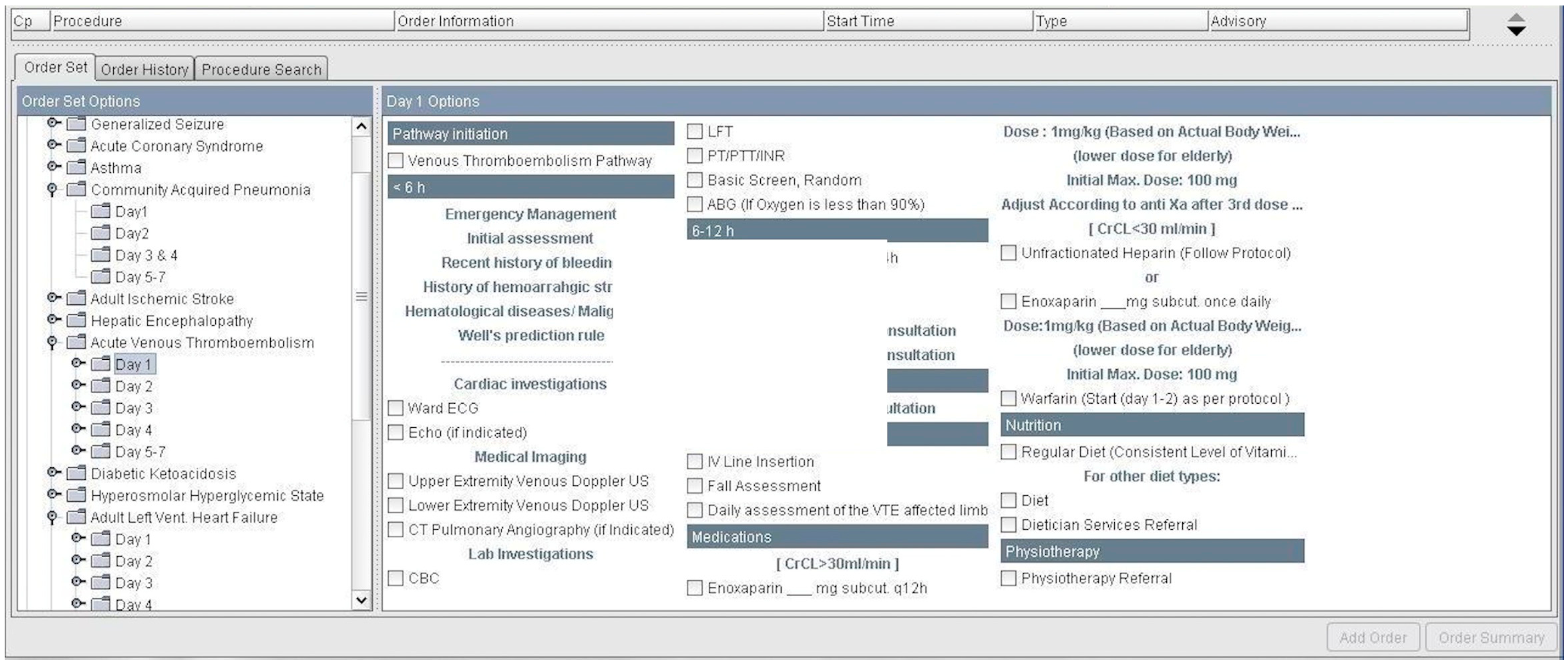
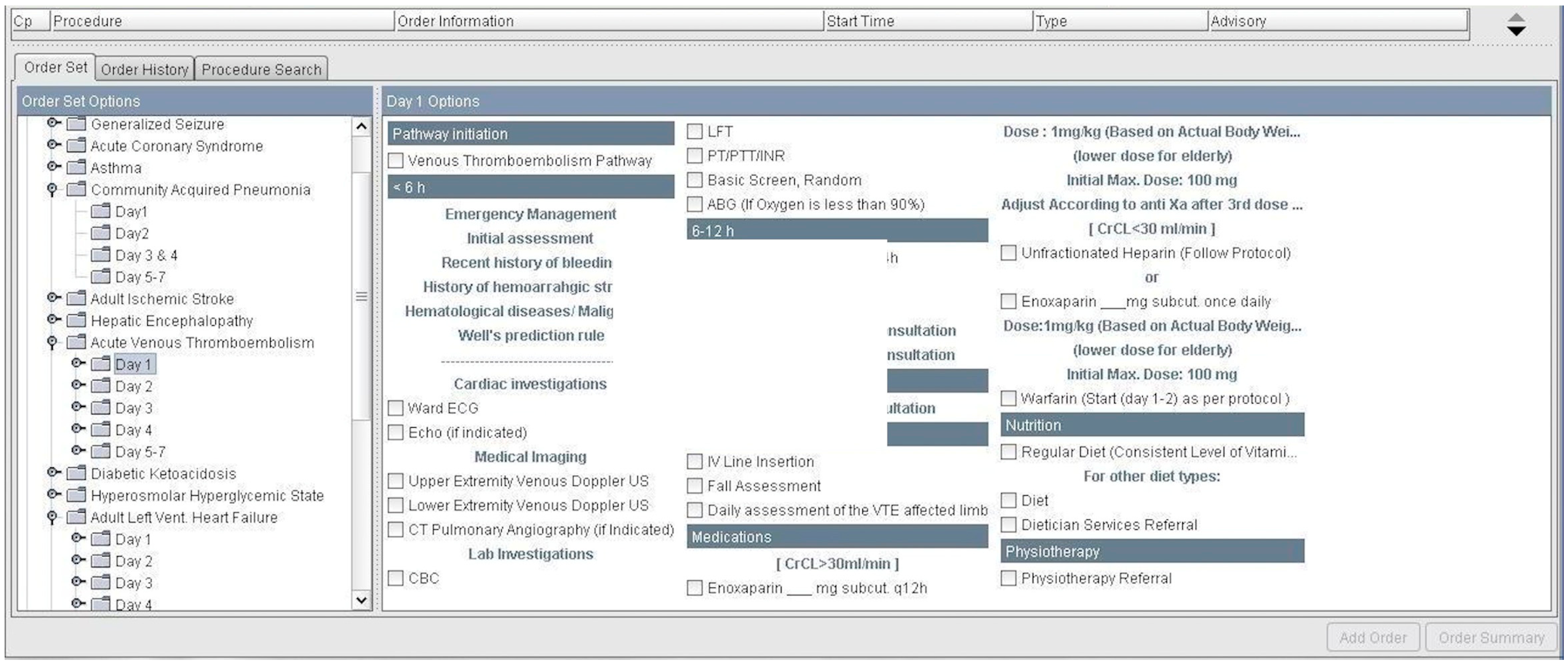
The order sets of the therapeutic regimens for all 15 CPs were integrated into CPOE over a period of three months through collaboration with pathway team and information technology department. Subsequently, CPOE order sets were reviewed by the clinical pharmacist coordinator and the chair of pathway team to ascertain the accuracy and validity for use in direct patient care. Figure 2 is a screenshot of day one for an electronic CPOE order sets for venous thromboembolism.
A pilot study of five clinical pathways started for 6 months in March 2012. We worked with physicians on updating the therapeutic components of CPs during the implementation period based on recent guidelines or new studies. Additionally, we maintained effective communication strategies with CPs team, which facilitated the integration of these therapeutic updates into CPOE order sets promptly.
3.1.2. Patient-Centered Pharmaceutical Care Services
Medication reconciliation by the pharmacist within 24 h of admission started as a pilot phase. The pharmacists provided education for patients and utilized educational leaflets to improve patient’s knowledge about their medications. Pharmacists communicated with the physicians for possible necessary changes upon order verification, and documented their therapeutic interventions during the patient interview in the electronic healthcare system.
3.1.3. Tools
Creatinine clearance estimation was reported in the electronic system as well as all cautionary and advisory flags developed in the order sets.
3.1.4. Research
The coordinating clinical pharmacist worked with the research team as a co-investigator. The study received IRB approval, and five out of fifteen (33%) of CPs were studied in CHAMP-Path study. The five CPs were acute kidney injury, venous thromboembolism, asthma, community acquired pneumonia, and heart failure. Emergency Pharmacy was responsible for the allocation of study participants as per the randomization scheme. The coordinating clinical pharmacist with the CHAMP-Path team participated in the presentation of the study updates on an annual basis at King Abdullah International Research forums from 2012 to 2015. Furthermore, the study method and collaboration of pharmacy with the multidisciplinary team were presented at other international research forums, such as The Principles and Practice of Clinical Research course in Sao Paulo, Brazil in 2011 offered by Harvard T H Chan School of Public Health and the Global Conference of the American College of Clinical Pharmacy, CA, United States in 2015. Finally, to date, two papers reporting CHAMP-Path studies were published with the coordinating clinical pharmacist as the leading author or co-author [22,23]. In the acute kidney injury study, the primary outcome of median length of stay (LOS) was 4.96 days (interquartile range of 6.57) for the pathway care compared to 4.8 days (interquartile range of 6.84 days) for the usual care (p = 0.8). Secondary outcomes of 30-day readmission and in-hospital mortality were also not statistically different [23]. Preliminary findings of unpublished data demonstrated that heart failure and venous thromboembolism showed a significant reduction in primary outcome of LOS and further data analysis for the findings of the studies is ongoing.
3.2. Assessment
3.2.1. Pilot Study for Validation of Patient-Satisfaction Survey
A pilot study of 20 participants was conducted to assess the validity of CHAMP-Path patient-satisfaction survey. We present the results focusing on the questions related to the pharmacy section. Forty-five percent (9/20) of respondents requested clarifications when asked if pharmacy reviewed their home medication within 24 h of admission, and 30% (6/17) of respondents did not understand the question on the medication reconciliation process. Almost one-quarter of respondents, 26.7% (4/15), asked for clarifications about receiving counseling before discharge, 20% (3/15) had some questions regarding the overall performance of pharmaceutical services, and only 13.3% (2/15) inquired about the question pertaining to their understanding of information during the counseling process.
The Cronbach’s alpha for internal consistency was 0.39 for pharmaceutical care questions, which were attributed to long questions, word phrasing, and to the fact that medication reconciliation services by pharmacists were not activated at the pilot phase. Subsequently, the survey questions and responses for pharmaceutical services were revised, and the final survey questions for pharmaceutical services are presented in Table 3.
3.2.2. Patient-Satisfaction Survey
We had 338 patients who were enrolled in the CHAMP-Path study from 2012 to 2016, of which 182 (53.85%) completed the patient-satisfaction survey. Some patients had missing responses for the questions related to pharmaceutical services. The results of the patient-satisfaction survey related to pharmaceutical services are presented in Table 4.
3.2.3. Continuous Education
Clinical pharmacy coordinator presented regular orientation sessions for pharmacy staff on their roles and duties during the implementation process of CPs. Furthermore, we actively participated in the pathway workshops to enhance the awareness of various healthcare professionals on the process of pathway development and strategies for integration into CPs. Additionally, the clinical pharmacy coordinator collaborated with pathway team to provide regular annual orientations to the medical residents on the use of CPOE order sets and the study-related logistics, such as screening and enrollment.
4. Discussion
Our interprofessional collaboration with the multidisciplinary team of healthcare professionals has paved the path for various opportunities to provide patient-centered pharmacist care through multifaceted interventions. As we did not have an explicit practice model, we strove to follow the standards of ACCP, ASHP, ISMP, and international guidance on the role of the pharmacist in designing CPs. The results of the patient-satisfaction survey demonstrated that counseling services were useful in improving the perception of 86.9% of respondents about their medications, which is an essential step for adherence and reducing hospital readmission. A systematic review demonstrated that patient counseling reduced morbidities, mortalities, and enhanced interprofessional collaboration [24]. Although 71.7% of respondents to the survey in our study received medication reconciliation, only 56.6% rated the service as good or very good. The low rate of satisfaction demonstrates an area for improvement in our setting. However, a study conducted at our hospital in 2012–2013 comparing medication reconciliation by pharmacist vs physician, and included >50% of medical patients, demonstrated a significant difference in the number of discrepancy medications identified by the pharmacist vs physicians [25]. These findings warrant the need to revisit the consistency and sustainability of the quality of medication reconciliation services by pharmacists in our setting, which have demonstrated their effectiveness in optimizing patient-care and medication safety [26].
Our collaborative experience had several limitations and challenges: (1) Although we worked to develop fifteen CPs, we were able to assess the outcomes of only five of these CPs, which were included in the CHAMP-Path study due to obstacles in randomizing physicians into teams for other subspecialties in a pragmatic randomized-controlled trial; (2) We were not able to monitor for the adherence to the use of CPOE order set, due to technical difficulties as well as the nature of the pragmatic design [27,28], which allows physicians to deviate from CPs to meet individual patients’ need; (3) We had periods of inconsistent pharmaceutical care services, such as medication counseling and reconciliation during weekend and holidays due to shortage of staffing, which interrupts the continuity of care and undermines the effect of these services on patient-centered outcomes. Furthermore, we did not assess therapeutic interventions by pharmacists and their effect on patient care, due to technical issues in retrieving these therapeutic interventions for auditing purposes.
We have identified several strengths in our experience in the development and implementation of CPs: first, it presents a unique model for pragmatic interprofessional collaboration with various multidisciplinary teams aiming to improve patient-centered outcomes. Interprofessional collaboration is endorsed by the Institute of Medicine for incorporation in the educational curriculum to empower the future generation of practitioners with necessary skills and competencies [29]. Second, CPs facilitated piloting, launching of many patient-centered pharmaceutical care services, and engaging pharmacists in clinical research. Additionally, it delivered key messages on areas for improvement and demonstrated the flexibility of pharmacists to changes to achieve the desired strategic goals of the institution. Third, it offered leadership opportunities for clinical pharmacists, as stakeholders of therapeutics in the organization, to provide safe and cost-effective medication regimens [7]. Future studies assessing clinical pathways should describe further practice models for interprofessional collaboration for pharmacists and pharmaceutical services targeting improved clinical outcomes.
5. Conclusions
Clinical pathways provide unique opportunities for establishing and evaluating patient-centered pharmaceutical services, and allowing pharmacists to demonstrate interprofessional leadership skills in collaboration with multidisciplinary teams.
Acknowledgments
We extend our appreciation to all members of the pharmaceutical care services, King Khalid Hospital, Jeddah, Saudi Arabia for their extended work and dedication in the development and implementation of clinical pathways. We thank all multidisciplinary team members and Department of Medicine, King Khalid Hospital, Jeddah, Saudi Arabia for the opportunity to collaborate and the continuous support to pharmaceutical care services. The team acknowledges the tremendous efforts of our research assistant Ms. Maryam Khalil during the implementation of clinical pathways, data collection, analysis and editing of the manuscript for English proofreading. A poster presentation of our experience was presented at the ACCP Global Conference on Clinical Pharmacy in 2015, SF, USA.
Author Contributions
S.I. was the clinical pharmacist coordinator, participated in the development, implementation, assessment of data, co-investigator in CHAMP-Path study, analyzed data, drafted the manuscript and finalized before submission. M.O. was the clinical pharmacist with medicine background who reviewed CPOE order sets, participated in the education of pharmacists and reviewed the manuscript before submission. R.A. was the clinical pharmacy supervisor who reviewed CPOE order sets, coordinated education of pharmacists for patient-counseling and medication reconciliation and reviewed the manuscript before submission. H.A. was the pharmacy director who organized pharmacy team, provided support to implement new services and reviewed the manuscript before submission. K.H.M.Q. was the chair of the Department of Medicine who organized the pathways team, coordinated the development, implementation, and assessment of CPs and was the principal investigator of CHAMP-Path studies, and reviewed the manuscript before submission.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Saseen, J.J.; Ripley, T.L.; Bondi, D.; Burke, J.M.; Cohen, L.J.; McBane, S.; McConnell, K.J.; Sackey, B.; Sanoski, C.; Simonyan, A.; et al. ACCP clinical pharmacist competencies. Pharmacotherapy 2017, 37, 630–636. [Google Scholar] [CrossRef] [PubMed]
- American Society of Health-System Pharmacists. ASHP guidelines on a standardized method for pharmaceutical care. Am. J. Health Syst. Pharm. 1996, 53, 1713–1716. [Google Scholar]
- Jaggers, L.D. Differentiation of critical pathways from other health care management tools. Am. J. Health Syst. Pharm. 1996, 53, 311–313. [Google Scholar] [PubMed]
- Petitta, A. Assessing the value of pharmacists’ health-systemwide services: Clinical pathways and treatment guidelines. Pharmacotherapy 2000, 20, 327s–332s. [Google Scholar] [CrossRef] [PubMed]
- Campbell, H.; Hotchkiss, R.; Bradshaw, N.; Porteous, M. Integrated care pathways. BMJ 1998, 316, 133–137. [Google Scholar] [CrossRef] [PubMed]
- European Pathway Association (EPA). Care Pathways. Available online: http://e-p-a.Org/care-pathways (accessed on 14 May 2016).
- Hipp, R.; Abel, E.; Weber, R.J. A primer on clinical pathways. Hosp. Pharm. 2016, 51, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Kinsman, L.; Rotter, T.; James, E.; Snow, P.; Willis, J. What is a clinical pathway? Development of a definition to inform the debate. BMC Med. 2010, 8, 31. [Google Scholar] [CrossRef] [PubMed]
- Rotter, T.; Kinsman, L.; James, E.; Machotta, A.; Willis, J.; Snow, P.; Kugler, J. The effects of clinical pathways on professional practice, patient outcomes, length of stay, and hospital costs: Cochrane systematic review and meta-analysis. Eval. Health Prof. 2012, 35, 3–27. [Google Scholar] [CrossRef] [PubMed]
- Rotter, T.; Kugler, J.; Koch, R.; Gothe, H.; Twork, S.; van Oostrum, J.; Steyerberg, E. A systematic review and meta-analysis of the effects of clinical pathways on length of stay, hospital costs and patient outcomes. BMC Health Serv. Res. 2008, 8, 265. [Google Scholar] [CrossRef] [PubMed]
- Kirk, J.K.; Michael, K.A.; Markowsky, S.J.; Restino, M.R.; Zarowitz, B.J. Critical pathways: The time is here for pharmacist involvement. American college of clinical pharmacy. Pharmacotherapy 1996, 16, 723–733. [Google Scholar] [PubMed]
- American Society of Health-System Pharmacists. ASHP guidelines on the pharmacist’s role in the development, implementation, and assessment of critical pathways. Am. J. Health Syst. Pharm. 2004, 61, 939–945. [Google Scholar]
- Dobesh, P.P.; Bosso, J.; Wortman, S.; Dager, W.E.; Karpiuk, E.L.; Ma, Q.; Zarowitz, B.J. Critical pathways: The role of pharmacy today and tomorrow. Pharmacotherapy 2006, 26, 1358–1368. [Google Scholar] [CrossRef] [PubMed]
- American Society of Health-System Pharmacists. ASHP–SHM joint statement on hospitalist–pharmacist collaboration. Am. J. Health Syst. Pharm. 2008, 65, 260–263. [Google Scholar]
- Institute for Safe Medication Practices. ISMP Develops Guidelines for Standard Order Sets. Available online: http://www.Ismp.Org/newsletters/acutecare/articles/20100311.Asp (accessed on 3 February 2018).
- Best Possible Medication History Interview Guide. Available online: https://www.Ismp-canada.Org/download/medrec/shn_medcard_09_en.Pdf (accessed on 14 February 2018).
- American Society of Health-System Pharmacists. ASHP statement on the pharmacist’s role in medication reconciliation. Am. J. Health Syst. Pharm. 2013, 70, 453–456. [Google Scholar]
- Maclean, L.G. Patient consultation in the cycle of patient care. In Pharmacy Practice Manual: A Guide to the Clinical Experience, 3rd ed.; Stein, S.M., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; pp. 566–577. [Google Scholar]
- American Society of Health-System Pharmacists. ASHP guidelines on pharmacist-conducted patient education and counseling. Am. J. Health Syst. Pharm. 1997, 54, 431–434. [Google Scholar]
- Fields, W.; Tedeschi, C.; Foltz, J.; Myers, T.; Heaney, K.; Bosak, K.; Rizos, A.; Snyder, R. Reducing preventable medication safety events by recognizing renal risk. Clin. Nurse Spec. 2008, 22, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, A.L.; Henriksen, D.P.; Marinakis, C.; Hellebek, A.; Birn, H.; Nybo, M.; Sondergaard, J.; Nymark, A.; Pedersen, C. Drug dosing in patients with renal insufficiency in a hospital setting using electronic prescribing and automated reporting of estimated glomerular filtration rate. Basic Clin. Pharmacol. Toxicol. 2014, 114, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.; Khalil, M.; Hafez, J.; Yusuf, O.; Thomson, J.; Sidiqui, M.; Quadri, K.M. The Genesis of the Champ-Path: Pragmatic rcts Methodology. PPCR 2017, 3. Available online: http://ppcr.org/journal/index.php/ppcrjournal/article/view/66 (accessed on 1 February 2018).
- Almalki, A.H.; Ismail, S.E.; Qureshi, M.A.; Abunijem, Z.; Balla, M.E.; Karsou, S.; Qureshi, R.A.; Ahmad, A.; AlSulami, S.; Khalil, M.; et al. A pragmatic randomized controlled trial comparing pathway-based versus usual care in community-acquired acute kidney injury. Saudi J. Kidney Dis Transpl. 2017, 28, 1282–1292. [Google Scholar] [CrossRef] [PubMed]
- Okumura, L.M.; Rotta, I.; Correr, C.J. Assessment of pharmacist-led patient counseling in randomized controlled trials: A systematic review. Int. J. Clin. Pharm. 2014, 36, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Abdulghani, K.H.; Aseeri, M.A.; Mahmoud, A.; Abulezz, R. The impact of pharmacist-led medication reconciliation during admission at tertiary care hospital. Int. J. Clin. Pharm. 2017. [Google Scholar] [CrossRef] [PubMed]
- Mekonnen, A.B.; McLachlan, A.J.; Brien, J.A. Effectiveness of pharmacist-led medication reconciliation programmes on clinical outcomes at hospital transitions: A systematic review and meta-analysis. BMJ Open 2016, 6, e010003. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, K.E.; Zwarenstein, M.; Oxman, A.D.; Treweek, S.; Furberg, C.D.; Altman, D.G.; Tunis, S.; Bergel, E.; Harvey, I.; Magid, D.J.; et al. A pragmatic-explanatory continuum indicator summary (precis): A tool to help trial designers. CMAJ 2009, 180, E47–E57. [Google Scholar] [CrossRef] [PubMed]
- Zwarenstein, M.; Treweek, S.; Gagnier, J.J.; Altman, D.G.; Tunis, S.; Haynes, B.; Oxman, A.D.; Moher, D. Improving the reporting of pragmatic trials: An extension of the consort statement. BMJ 2008, 337, a2390. [Google Scholar] [CrossRef] [PubMed]
- Bridges, D.R.; Davidson, R.A.; Odegard, P.S.; Maki, I.V.; Tomkowiak, J. Interprofessional collaboration: Three best practice models of interprofessional education. Med. Educ. Online 2011, 16, 95–106. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Layout of the roles of pharmacists as interprofessional collaborators in CPs.
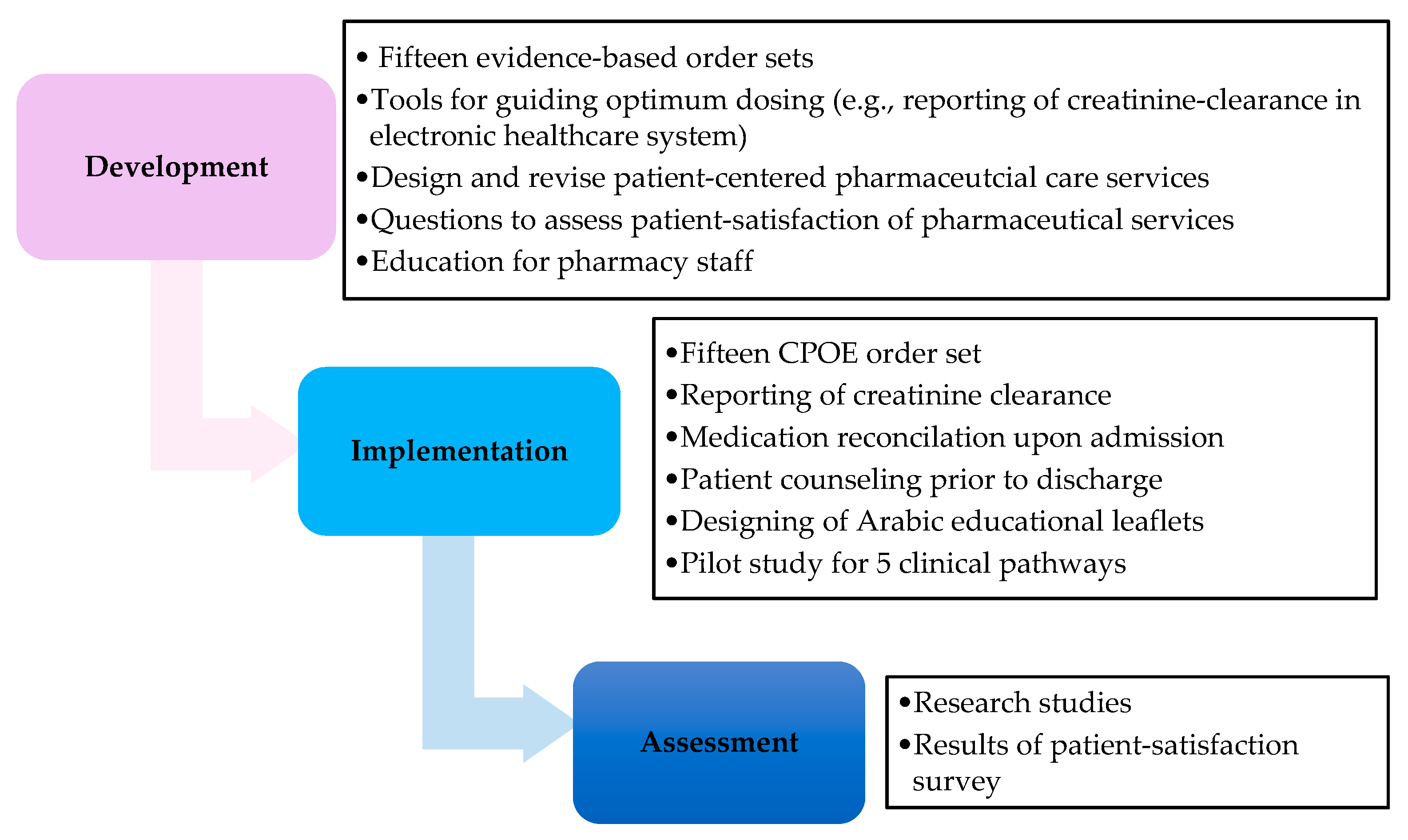
Figure 2.
An example of Computerized Order Prescriber Entry of day one for venous thromboembolism pathway.
Figure 2.
An example of Computerized Order Prescriber Entry of day one for venous thromboembolism pathway.

{kind=link}
{kind=link}
Table 1.
Goals and Perspectives of the Pharmacy team.
|
Table 2.
Questions related to pharmaceutical care services in the pilot phase of CHAMP-Path patient-satisfaction survey.
Table 2.
Questions related to pharmaceutical care services in the pilot phase of CHAMP-Path patient-satisfaction survey.
| Pharmaceutical Care (الرعاية الصيدلانية) | Responses | ||||
|---|---|---|---|---|---|
| 1 Did the Pharmacist review your home medication within 24 h of admission? هل راجع الصيدلي أدويتك الخاصة بك التى تتناولها بالمنزل خلال 24 ساعة من تنويمك؟ | Yes ( نعم ) □ | No ( لا ) □ | |||
| 2 Did you receive counseling by the Pharmacist on your medications before discharge? هل حصلت على معلومات خاصة بادويتك من الصيدلي قبل خروجك من المستشفى؟ | Yes ( نعم ) □ | No ( لا ) □ | |||
 |  |  |  |  | |
| Excellent | Very Good | Good | Poor | Unsatisfactory | |
| ممتا ز | جيد جدا | جيد | ضعيف | غير مقبول | |
| 3 How would you describe the process of reviewing your home medication with the Pharmacist upon admission? كيف تصف طريقة مراجعة أدويتك الخاصة مع الصيدلي عند التنويم؟ | □ | □ | □ | □ | □ |
| 4 How would you best describe your level of understanding about your medications based on the educational information you received from your pharmacist before discharge? كيف تصف مستوى فهمك للأدوية الخاصة بك حسب التعليمات التي تلقيتها من الصيدلي قبل خروجك من المستشفى؟ | □ | □ | □ | □ | □ |
| 5 How would you best describe the overall performance of the pharmaceutical services provided during your stay in hospital? كيف تصف الأداء العام للخدمات الصيدلانية المقدمة خلال إقامتك في المستشفى؟ | □ | □ | □ | □ | □ |
Table 3.
Questions related to pharmaceutical care services in the CHAMP-Path patient satisfaction survey.
Table 3.
Questions related to pharmaceutical care services in the CHAMP-Path patient satisfaction survey.
| Pharmaceutical Care | الرعاية الصيدلانية | |||||||
|---|---|---|---|---|---|---|---|---|
| 1 | Did the Pharmacist review your home medications? | Yes | □ | نعم | هل راجع الصيدلي أدويتك التى تتناولها بالمنزل؟ | ١ـ | ||
| No | □ | لا | ||||||
| | | | | | ||||
| جيد جدا | جيدا | محايد | ضعيف | ضعيف جدا | ||||
| Very Good | Good | Neutral | Poor | Very Poor | ||||
| 2 | How would you rate the process of reviewing your home medication with the Pharmacist upon admission? | □ | □ | □ | □ | □ | ما هو تقييمك لطريقة مراجعة أدويتك مع الصيدلي عند دخولك في المستشفى؟ | ٢ـ |
| Did not Review | □ | لم يراجع أدويتي | ||||||
| 3 | Has the pharmacist counseled you on the medications, which you will be taking home with you? | Yes | □ | نعم | هل نصحك الصيدلي عن الأدوية التي ستأخذ معك إلى المنزل؟ | ٣ـ | ||
| No | □ | لا | ||||||
| Not Applicable | □ | لا ينطبق | ||||||
| (Discharged after-hours) | ||||||||
| | | | | | ٤ـ | |||
| فهمت تماما | فهمت كثيرا | فهمت نوعا ما | فهمت قليلا | لم أفهم | ||||
| Completely understood | Understood a lot | Understood somewhat | Understood a little | Did not understand | ||||
| 4 | How would you rate your level of understanding about your medications based on the educational information you received from your pharmacist before discharge? | □ | □ | □ | □ | □ | ما هو تقييمك لمستوى فهمك للأدوية الخاصة بك حسب التعليمات التي تلقيتها من الصيدلي قبل خروجك من المستشفى؟ | -٥ |
| No Information | □ | لم أتلق أي معلومات | ||||||
| | | | | | ||||
| جيد جيد جدا | جيد ا | محايد | ضعيف | ضعيف جدا | ||||
| Very Good | Good | Neutral | Poor | Very Poor | ||||
| 5 | How would you rate the overall performance of the pharmaceutical services provided during your stay in hospital? | □ | □ | □ | □ | □ | ما هو تقييمك عموما للخدمات الصيدلية المقدمة خلال إقامتك في المستشفى؟ | ٦ـ |
Table 4.
Results of CHAMP-Path patient-satisfaction survey related to pharmaceutical care services.
| Questions | Responses | Proportions n/N (%) | 95% Confidence Intervals | |
|---|---|---|---|---|
| Medication Reconciliation upon admission | ||||
| 1 | Received medication reconciliation by pharmacist | Yes | 119/166 (71.7) | 64.8–78.6 |
| 2 | Evaluation of Medication reconciliation by pharmacist | Did not review | 49/159 (30.8) | 23.6–38.0 |
| Poor a | 20/159 (12.6) | 7.4–17.8 | ||
| Good b | 90/159 (56.6) | 48.9–64.3 | ||
| Patient counseling before discharge | ||||
| 3 | Received counseling by pharmacist | Yes | 102/147 (69.4) | 62.0–76.8 |
| Not applicable c | 28/147 (19.0) | 12.7–25.3 | ||
| 4 | Level of understanding about medications based on counseling by pharmacist | No information provided | 14/145 (9.7) | 4.9–14.5 |
| Poor understanding d | 5/145 (3.4) | 0.5–6.3 | ||
| Good understanding e | 126/145 (86.9) | 81.4–92.4 | ||
| Overall performance of Pharmaceutical Services | ||||
| 5 | Evaluation of overall performance of the pharmaceutical services provided | Poor a | 38/144 (26.4) | 19.2–33.6 |
| Good b | 106/144 (73.6) | 66.4–80.8 | ||
a Poor: Poor is a collapsed category of very poor, poor and neutral; b Good: good is a collapsed category of good and very good; c Not applicable was due to discharge during the weekend or patient discharge after working hours for counseling pharmacist; d Poor understanding: is a collapsed category of did not understand and understood a little; e Good understanding: is a collapsed category of somewhat understand, understood a lot and understood completely.
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ismail, S.; Osman, M.; Abulezz, R.; Alhamdan, H.; Quadri, K.H.M. Pharmacists as Interprofessional Collaborators and Leaders through Clinical Pathways. Pharmacy 2018, 6, 24. https://doi.org/10.3390/pharmacy6010024
AMA Style
Ismail S, Osman M, Abulezz R, Alhamdan H, Quadri KHM. Pharmacists as Interprofessional Collaborators and Leaders through Clinical Pathways. Pharmacy. 2018; 6(1):24. https://doi.org/10.3390/pharmacy6010024
Chicago/Turabian StyleIsmail, Sherine, Mohamed Osman, Rayf Abulezz, Hani Alhamdan, and K. H. Mujtaba Quadri. 2018. "Pharmacists as Interprofessional Collaborators and Leaders through Clinical Pathways" Pharmacy 6, no. 1: 24. https://doi.org/10.3390/pharmacy6010024
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.