
Understanding the Needs of Young Women Regarding Breast Cancer Risk Assessment and Genetic Testing: Convergence and Divergence among Patient-Counselor Perceptions and the Promise of Peer Support

Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Interview
2.3. Data Analysis
3. Results
3.1. Care Planning and Management
“I guess what happens after the test results … getting information about this, how this could affect your life or not, or this is what (the information) could mean”.-Patient, Age 26, tested positive
“I’m a person who likes all of the information … and I don’t want it to be dumbed-down. It was really frustrating going to physicians who wouldn’t explain things to me, then also very troubling to get bits and pieces of information over time”.-Patient, Age 24, untested
When my mom said, “Oh, you need mammograms, …” and the gynecologist said “I didn’t need them—I would get stressed out”.-Patient, Age 24, untested
“I end up posing a lot more hypothetical questions ... making sure that this is something that they’ve thought through and it’s something that they’re doing for themselves and not due to familial influences”.-Genetic Counselor
“So it’s really about being action-oriented … it moves from opening up the emotional can of worms, addressing it, reining it back in, and then being very action-focused is how I tend to handle those consultations”.-Genetic Counselor
3.2. Decision Making about BCRA/GT
“If (the genetic test) comes back positive, making decisions about how I want to protect myself would be difficult. I think one difficult thing is the timing—when is the best time to make a decision about prophylactic measures”.-Patient, Age 22, tested (results not in at time of interview)
“I already know that I’m at high risk for (cancer) so I don’t really see any difference between knowing I’m higher risk and knowing I’m positive”.-Patient, Age 19, untested
“… what we decide at 18, may be very different from what we would decide at 22 or 23. If this is not something that you’re going to act on now, you may feel like you want to know now but if we revisit this in a year or two, you’re going say, ‘Oh gosh, I’m glad I don’t know’. So it’s thinking about how people’s minds can change as their life experiences change”.-Genetic Counselor
“I think that people have a lot of growth emotionally, and someone might be in a very different head space when they’re in their 20s … so I think that could be a potential like downside. So it’s like the benefit is for them to know earlier and cope with that result and when they’re ready to get screened, they can start. But are you doing harm giving them information that they can’t do anything with for a few years?”-Genetic Counselor
“There definitely are women who are doing it for their family but they really have no idea where they’re going in life and this idea of finding out four years before it’s even going to matter—that doesn’t really sit well for some people”.-Genetic Counselor
“I feel like I have more experiences with younger women coming in and then deciding that they don’t want to do testing. Whereas older women that are coming in, they come in with more of a set idea …. But younger women may not be like that because of just life experience but also that may not be where they are in life”.-Genetic Counselor
“I think that the risks are really where they are in their life decision making. And their capacity to actually manage information like this and what we would hope would be normal decision making about finding a partner and whether or not you want to have children and how that can change as a result of being tested. So I think there are risks, but it isn’t for us to decide that they can’t be tested—some people are so concerned that they want to be tested”.-Genetic Counselor
3.3. Medical Management
“I think that I have lived my life basically with an assumption that I would have to get breast removal surgery like my mom did. It was actually interesting to me when one of the physicians was more like, ‘You don’t have anything to worry about now, don’t get tested”. Just the concept of not doing that, was (confusing), I don’t get what you’re saying… And why wouldn’t I have to do that?”-Patient, Age 24, untested
“I think that knowing that you do have it (a positive test result)—it would give me more clout in negotiating with my physicians when I want to be more aggressive. Just because they say, ‘oh, don’t worry about it, you don’t have to do that yet … ‘and I can say, ‘But wait, I am positive for these mutations, we all know that my risk goes up’.”.-Patient, Age 24, untested
“I think that even when I’m thinking about life plans now, I don’t take the risk or the genetic testing much into account. I think it would definitely help in making decisions about being realistic about what might happen but right now it doesn’t have much effect on what I’m deciding to do”.-Patient, Age 20, untested
“Having the information definitely would not change any of my career goals. That’s something that even if I knew I would die tomorrow, I would still plan because there’s only a chance that it (getting cancer) will happen anyways”.-Patient, Age 19, untested
“I definitely do a lot more screening because of it. I would say as far as day to day life, I haven’t really changed anything. I think with each year, getting a little bit older, I’m a little more cautious about eating healthier and exercising more”.-Patient, Age 28, tested positive
“I try to be very transparent about what national recommendations are. Until they’re 25, these screening recommendations don’t need to go into effect—of course, with the caveat of depending on family history”.-Genetic Counselor
“In our practice we don’t want people to fall through the cracks. So we set them up either with someone is our practice to be followed once or twice a year or with a breast surgeon if that is who we are talking about. Just let them know that there are options available”.-Genetic Counselor
“It’s not a single encounter. It is a process, it’s a team initiative working with the physicians and where social work is indicated, behavioral health is indicated”.-Genetic Counselor
3.4. Psychosocial Distress
“I was really nervous … it was a very stressful day. It was a little hard to isolate how I was feeling about that in particular [the test results] but it was a little like, ‘I’m starting my life here, finally out of school’. It was like one of those moments when you’re not invincible anymore”.-Patient, Age 26, tested positive
“I think that if the results were negative, I think there would be an emotional sort of burden lifted. I feel that burden getting heavier the older I get, the closer I get when my aunts were diagnosed”.-Patient, Age 24, untested
“I think that being honest is good because … me and my mom’s relationship … it’s very easy to talk to her about that (genetic counseling) and I think that that’s good because it provides more of a security blanket for me that I’m not going into this blind”.-Patient, Age 20, untested
“… it was always my choice and my decision. My family always gave me the power of whether or not I should be tested”.-Patient, Age 28, tested positive
“I feel like they already have experienced it, ... they’ve gone through the process so sometimes I think there’s an expectation for these (young) women of what they’re supposed to do. There’s sometimes the element of pressure to meet the expectations of what others have done”.-Genetic Counselor
“I think in the end, it was good that she was there to support her sister, that she didn’t go through it alone and now she gets to watch her sister and see because they both ended up testing positive”.-Genetic Counselor
“… the family is really in more of a support role, an extra set of ears … they are often taking notes”.-Genetic Counselor
“... from a behavioral perspective there is much more emotional counseling in that young group, having to make complex decisions that are harder than someone who may be much older”.-Genetic Counselor
3.5. Intervention Development
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A. COREQ Checklist
| No. | Item | Guide Questions/Description | Response |
| Domain 1: Research Team and Reflexivity | |||
| Personal Characteristics | |||
| 1. | Interviewer/facilitator | Which author (s) conducted the interview or focus group? | Dr. Suzanne O’Neill conducted the interviews with genetic counselors and Chalanda Evans conducted the interviews with the young women. |
| 2. | Credentials | What were the researcher’s credentials? e.g., PhD, MD |
|
| 3. | Occupation | What was their occupation at the time of the study? | |
| 4. | Gender | Was the researcher male or female? | All researchers but Kenneth Tercyak were female. |
| 5. | Experience and training | What experience or training did the researcher have? |
|
| Relationship with participants | |||
| 6. | Relationship established | Was a relationship established prior to study commencement? | None of the young women was acquainted with the researchers prior to the study start. Some of the genetic counselors were professional colleagues of Dr. O’Neill through professional organizations. |
| 7. | Participant knowledge of the interviewer | What did the participants know about the researcher? e.g., personal goals, reasons for doing the research | The participants knew the purpose of the interview was to hear more about their opinions and thoughts regarding issues of genetic testing, cancer prevention, and family health for young women, aged 18–30 at risk for carrying a BRCA1/2 mutation. Participants were made aware the researchers were affiliated with Lombardi Comprehensive Cancer Center and the interview was part of a larger NCI funded study. |
| 8. | Interviewer characteristics | What characteristics were reported about the interviewer/facilitator? e.g., bias, assumptions, reasons and interests in the research topic | |
| Domain 2: Study Design | |||
| Theoretical framework | |||
| 9. | Methodological orientation and theory | What methodological orientation was stated to underpin the study? e.g., grounded theory, discourse analysis, ethnography, phenomenology, content analysis | Grounded theory |
| Participant selection | |||
| 10. | Sampling | How were participants selected? e.g., purposive, convenience, consecutive, snowball |
|
| 11. | Method of approach | How were participants approached? e.g., face-to-face, telephone, mail, email | Participants were approached by telephone to participate after completing an initial qualitative survey. |
| 12. | Sample size | How many participants were in the study? | 24 total (12 genetic counselors and 12 young women). |
| 13. | Non-participation | How many people refused to participate or dropped out? Reasons? | One counselor who was approached refused participation due to competing commitments. No individuals agreed but then dropped out before the interview. |
| Setting | |||
| 14. | Setting of data collection | Where was the data collected? e.g., home, clinic, workplace | Interviews were conducted by telephone at Georgetown University, Lombardi Comprehensive Cancer Center. |
| 15. | Presence of non-participants | Was anyone else present beside the participants and researchers? | No one else was present while researchers conducted the interview and to our knowledge all participants completed the interviews in a private setting with no else present. |
| 16. | Description of sample | What are the important characteristics of the sample? e.g., demographic data, date | Age, gender, level of education, BRCA testing status |
| Data collection | |||
| 17. | Interview guide | Were questions, prompts, guides provided by the authors? Was it pilot tested? | A semi-structured interview guide was developed. The guides were modified as needed to fit the participant being interviewed. The guides were not tested in a pilot study. |
| 18. | Repeat interviews | Were repeat interviews carried out? If yes, how many? | Yes, repeat interviews were carried out with XX of the participants to ask follow up questions. |
| 19. | Audio/visual recording | Did the research use audio or visual recording to collect the data? | Audio recording was used for all interviews and transcribed prior to analysis. |
| 20. | Field notes | Were field notes made during and/or after the interview or focus groups? | Yes, during the phone interviews. |
| 21. | Duration | What was the duration of the interviews or focus group? |
|
| 22. | Data saturation | Was data saturation discussed? | Yes. Interviews with genetic counselors and young women ended when saturation was reached. |
| 23. | Transcripts returned | Were transcripts returned to participants for comment and/or correction? | No. Transcripts were reviewed by researchers who listened to the audio recordings to verify their accuracy. |
| Domain 3: Analysis and Findings | |||
| Data analysis | |||
| 24. | Number of data coders | How many data coders coded the data? | 2 (SO and CE) |
| 25. | Description of the coding tree | Did authors provide a description of the coding tree? | Yes, a coding tree was developed based upon the individual nodes, coding sets and themes from the data. |
| 26. | Derivation of themes | Were themes identified in advance or derived from the data? | Initial coding was informed by the interview guide but codes were continually refined and created with data collection and analysis. All codes were agreed upon by the coders thru consensus. |
| 27. | Software | What software, if applicable, was used to manage the data? | QSR NVivo version 10 |
| 28. | Participant checking | Did participants provide feedback on the findings? | No |
| Reporting | |||
| 29. | Quotations presented | Were participant quotations presented to illustrate the themes/findings? Was each quotation identified? e.g., participant number | Yes, participant quotations are present but are not identified by participant number. |
| 30. | Data and findings consistent | Was there consistency between the data presented and the findings? | Yes |
| 31. | Clarity of major themes | Were major themes clearly presented in the findings? | Yes |
| 32. | Clarity of minor themes | Is there a description of diverse cases or discussion of minor themes? | Yes |
References
- Antoniou, A.; Pharoah, P.D.; Narod, S.; Risch, H.A.; Eyfjord, J.E.; Hopper, J.L.; Loman, N.; Olsson, H.; Johannsson, O.; Borg, A.; et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case series unselected for family history: A combined analysis of 22 studies. Am. J. Hum. Genet. 2003, 72, 1117–1130. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, A.C.; Cunningham, A.P.; Peto, J.; Evans, D.G.; Lalloo, F.; Narod, S.A.; Risch, H.A.; Eyfjord, J.E.; Hopper, J.L.; Southey, M.C.; et al. The BOADICEA model of genetic susceptibility to breast and ovarian cancers: Updates and extensions. Br. J. Cancer 2008, 98, 1457–1466. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, J.; Toscano, M.; Kotchko, N.; Friedman, S.; Schwartz, M.D.; Virgo, K.S.; Lynch, K.; Andrews, J.E.; Aguado Loi, C.X.; Bauer, J.E.; et al. Utilization and outcomes of BRCA genetic testing and counseling in a national commercially insured population: The ABOUT Study. JAMA Oncol. 2015, 1, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Kehl, K.L.; Shen, C.; Litton, J.K.; Arun, B.; Giordano, S.H. Rates of BRCA1/2 mutation testing among young survivors of breast cancer. Breast Cancer Res. Treat. 2016, 155, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, S.M.; Ruddy, K.J.; Tamimi, R.M.; Gelber, S.; Schapira, L.; Come, S.; Borges, V.F.; Larsen, B.; Garber, J.E.; Partridge, A.H. BRCA1 and BRCA2 mutation testing in young women with breast cancer. JAMA Oncol. 2016, 2, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, A.R.; Patrick-Miller, L.; Pawlowski, K.; Ibe, C.N.; Cummings, S.A.; Hlubocky, F.; Olopade, O.I.; Daugherty, C.K. Learning of your parent’s BRCA mutation during adolescence or early adulthood: A study of offspring experiences. Psychooncology 2009, 18, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Patenaude, A.F.; Tung, N.; Ryan, P.D.; Ellisen, L.W.; Hewitt, L.; Schneider, K.A.; Tercyak, K.P.; Aldridge, J.; Garber, J.E. Young adult daughters of BRCA1/2 positive mothers: What do they know about hereditary cancer and how much do they worry? Psychooncology 2013, 22, 2024–2031. [Google Scholar] [CrossRef] [PubMed]
- Offit, K.; Bradbury, A.; Storm, C.; Merz, J.F.; Noonan, K.E.; Spence, R. Gene patents and personalized cancer care: Impact of the Myriad case on clinical oncology. J. Clin. Oncol. 2013, 31, 2743–2748. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, L.C.; Lindor, N.M. The role of risk-reducing surgery in hereditary breast and ovarian cancer. N. Engl. J. Med. 2016, 374, 454–468. [Google Scholar] [PubMed]
- Chen, S.; Parmigiani, G. Meta-analysis of BRCA1 and BRCA2 penetrance. J. Clin. Oncol. 2007, 25, 1329–1333. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Genetic/Familial High-Risk Assessment: Breast and Ovarian. Version 2. 2016. Available online: https://www.nccn.org/professionals/physician_gls/pdf/genetics_screening.pdf (accessed on 12 May 2016).
- Hamilton, R.; Hurley, K.E. Conditions and consequences of a BRCA mutation in young, single women of childbearing age. Oncol. Nurs. Forum 2010, 37, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Hoskins, L.M.; Werner-Lin, A. A multi-case report of the pathways to and through genetic testing and cancer risk management for BRCA mutation-positive women aged 18–25. J. Genet. Couns. 2013, 22, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Baum, A.; Friedman, A.L.; Zakowski, S.G. Stress and genetic testing for disease risk. Health Psychol. 1997, 16, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing: New York, NY, USA, 1984. [Google Scholar]
- Hamilton, R.J.; Bowers, B.J. The Theory of Genetic Vulnerability: A Roy model exemplar. Nurs. Sci. Q. 2007, 20, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, L.; McCuaig, J.; Benoit, L.; Davies, C. It’s time for the genetic counseling profession to embrace social media. J. Genet. Couns. 2016. [Google Scholar] [CrossRef] [PubMed]
- Werner-Lin, A.; Ratner, R.; Hoskins, L.M.; Lieber, C. A survey of genetic counselors about the needs of 18–25 year olds from families with hereditary breast and ovarian cancer syndrome. J. Genet. Couns. 2015, 24, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Underhill, M.L.; Crotser, C.B. Seeking balance: Decision support needs of women without cancer and a deleterious BRCA1 or BRCA2 mutation. J. Genet. Couns. 2014, 23, 350–362. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, S.C.; Rini, C.; Goldsmith, R.E.; Valdimarsdottir, H.; Cohen, L.H.; Schwartz, M.D. Distress among women receiving uninformative BRCA1/2 results: 12-month outcomes. Psychooncology 2009, 18, 1088–1096. [Google Scholar] [CrossRef] [PubMed]
- Rini, C.; O’Neill, S.C.; Valdimarsdottir, H.; Goldsmith, R.E.; Jandorf, L.; Brown, K.; DeMarco, T.A.; Peshkin, B.N.; Schwartz, M.D. Cognitive and emotional factors predicting decisional conflict among high-risk breast cancer survivors who receive uninformative BRCA1/2 results. Health Psychol. 2009, 28, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Heiniger, L.; Butow, P.N.; Price, M.A.; Charles, M. Distress in unaffected individuals who decline, delay or remain ineligible for genetic testing for hereditary diseases: A systematic review. Psychooncology 2013, 22, 1930–1945. [Google Scholar] [CrossRef] [PubMed]
- Ringwald, J.; Wochnowski, C.; Bosse, K.; Giel, K.E.; Schaffeler, N.; Zipfel, S.; Teufel, M. Psychological distress, anxiety, and depression of cancer-affected BRCA1/2 mutation carriers: A systematic review. J. Genet. Couns. 2016. [Google Scholar] [CrossRef] [PubMed]
- Crotser, C.B.; Dickerson, S.S. Women receiving news of a family BRCA1/2 mutation: Messages of fear and empowerment. J. Nurs. Scholarsh. 2010, 42, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Mahon, S.M. Impact of the genetic screening revolution: Understanding and meeting the needs of previvors with a known family mutation in BRCA/BRCA2. Evid. Based Nurs. 2011, 14, 126–127. [Google Scholar] [CrossRef] [PubMed]
- Moreau, A.; Carol, L.; Dedianne, M.C.; Dupraz, C.; Perdrix, C.; Laine, X.; Souweine, G. What perceptions do patients have of decision making (DM)? Toward an integrative patient-centered care model. A qualitative study using focus-group interviews. Patient Educ. Couns. 2012, 87, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Graves, K.D.; Wenzel, L.; Schwartz, M.D.; Luta, G.; Wileyto, P.; Narod, S.; Peshkin, B.N.; Marcus, A.; Cella, D.; Emsbo, S.P.; et al. Randomized controlled trial of a psychosocial telephone counseling intervention in BRCA1 and BRCA2 mutation carriers. Cancer Epidemiol. Biomark. Prev. 2010, 19, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Hooker, G.W.; Leventhal, K.G.; DeMarco, T.; Peshkin, B.N.; Finch, C.; Wahl, E.; Joines, J.R.; Brown, K.; Valdimarsdottir, H.; Schwartz, M.D. Longitudinal changes in patient distress following interactive decision aid use among BRCA1/2 carriers: A randomized trial. Med. Decis. Mak. 2011, 31, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, K.A.; Poll, A.; O’Connor, A.; Gershman, S.; Armel, S.; Finch, A.; Demsky, R.; Rosen, B.; Narod, S.A. Development and testing of a decision aid for breast cancer prevention for women with a BRCA1 or BRCA2 mutation. Clin. Genet. 2007, 72, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.D.; Valdimarsdottir, H.B.; DeMarco, T.A.; Peshkin, B.N.; Lawrence, W.; Rispoli, J.; Brown, K.; Isaacs, C.; O’Neill, S.; Shelby, R.; et al. Randomized trial of a decision aid for BRCA1/BRCA2 mutation carriers: Impact on measures of decision making and satisfaction. Health Psychol. 2009, 28, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Van Roosmalen, M.S.; Stalmeier, P.F.; Verhoef, L.C.; Hoekstra-Weebers, J.E.; Oosterwijk, J.C.; Hoogerbrugge, N.; Moog, U.; van Daal, W.A. Randomized trial of a shared decision-making intervention consisting of trade-offs and individualized treatment information for BRCA1/2 mutation carriers. J. Clin. Oncol. 2004, 22, 3293–3301. [Google Scholar] [CrossRef] [PubMed]
- White, V.M.; Young, M.A.; Farrelly, A.; Meiser, B.; Jefford, M.; Williamson, E.; Ieropoli, S.; Duffy, J.; Winship, I. Randomized controlled trial of a telephone-based peer-support program for women carrying a BRCA1 or BRCA2 mutation: Impact on psychological distress. J. Clin. Oncol. 2014, 32, 4073–4080. [Google Scholar] [CrossRef] [PubMed]
- Bradbury, A.R.; Patrick-Miller, L.; Egleston, B.L.; Schwartz, L.A.; Sands, C.B.; Shorter, R.; Moore, C.W.; Tuchman, L.; Rauch, P.; Malhotra, S.; et al. Knowledge and perceptions of familial and genetic risks for breast cancer risk in adolescent girls. Breast Cancer Res. Treat. 2012, 136, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Tercyak, K.P.; Mays, D.; DeMarco, T.A.; Peshkin, B.N.; Valdimarsdottir, H.B.; Schneider, K.A.; Garber, J.E.; Patenaude, A.F. Decisional outcomes of maternal disclosure of BRCA1/2 genetic test results to children. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1260–1266. [Google Scholar] [CrossRef] [PubMed]
- Ashing-Giwa, K.; Tapp, C.; Rosales, M.; McDowell, K.; Martin, V.; Santifer, R.H.; Clark, P.; Steward, J.; Lewis, L.; Mitchell, E. Peer-based models of supportive care: The impact of peer support groups in African American breast cancer survivors. Oncol. Nurs. Forum 2012, 39, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Farrelly, A.; White, V.; Young, M.A.; Jefford, M.; Ieropoli, S.; Duffy, J.; Winship, I.; Meiser, B. Implementing a telephone based peer support intervention for women with a BRCA1/2 mutation. Fam. Cancer 2015, 14, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Hartzler, A.; Pratt, W. Managing the personal side of health: How patient expertise differs from the expertise of clinicians. J. Med. Internet Res. 2011. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Interview Content | ||
|---|---|---|
| Interview Themes | Genetic Counselors | Young Women |
| Role of the Family and Social Support in Testing | What role does the family play in counseling? Partner, friends, outside resources? | Who started the conversation and when? What did you think the genetic test results meant for your family member’s health? Was your family member available to discuss genetic testing if you had any questions? Have they brought up the topic of you undergoing testing/counseling? How did your family, friends, providers play a role? |
| Counseling and Testing Process | Do women vary in whether they are ready for testing at this age? How is counseling different for young women that have a familial cancer risk? What are the risks/advantages of testing young women? What concerns do you have about testing in this age group? | Do you plan to get testing in the future? When? What prompted you to move ahead with testing? Did you seek out additional resources? |
| Implications of Testing | What techniques do you use when talking to women about testing? How do you present and resolve the issue of fewer risk management options for younger women? | How do you think this information has changed or will change your personal life plans? Having children? Long-term relationships? Do you think knowing the information will be helpful to you? |
| Participant Variables | Young Women (N = 12) | Genetic Counselors (N = 12) |
|---|---|---|
| M (SD) N (%) | M (SD) N (%) | |
| Gender | ||
| Female | 12 (100) | 11 (91.7) |
| Male | 1 (8.3) | |
| Race/Ethnicity | ||
| White | 12 (100) | 11 (91.7) |
| African American | 1 (8.3) | |
| Age | 22.6 (2.84) | 35.4 (7.94) |
| Work Setting | ||
| Academic medical center | 5 (41.6) | |
| Private group practice | 4 (33.3) | |
| Government | 3 (25.1) | |
| Years in Practice | 8.3 (6.41) |
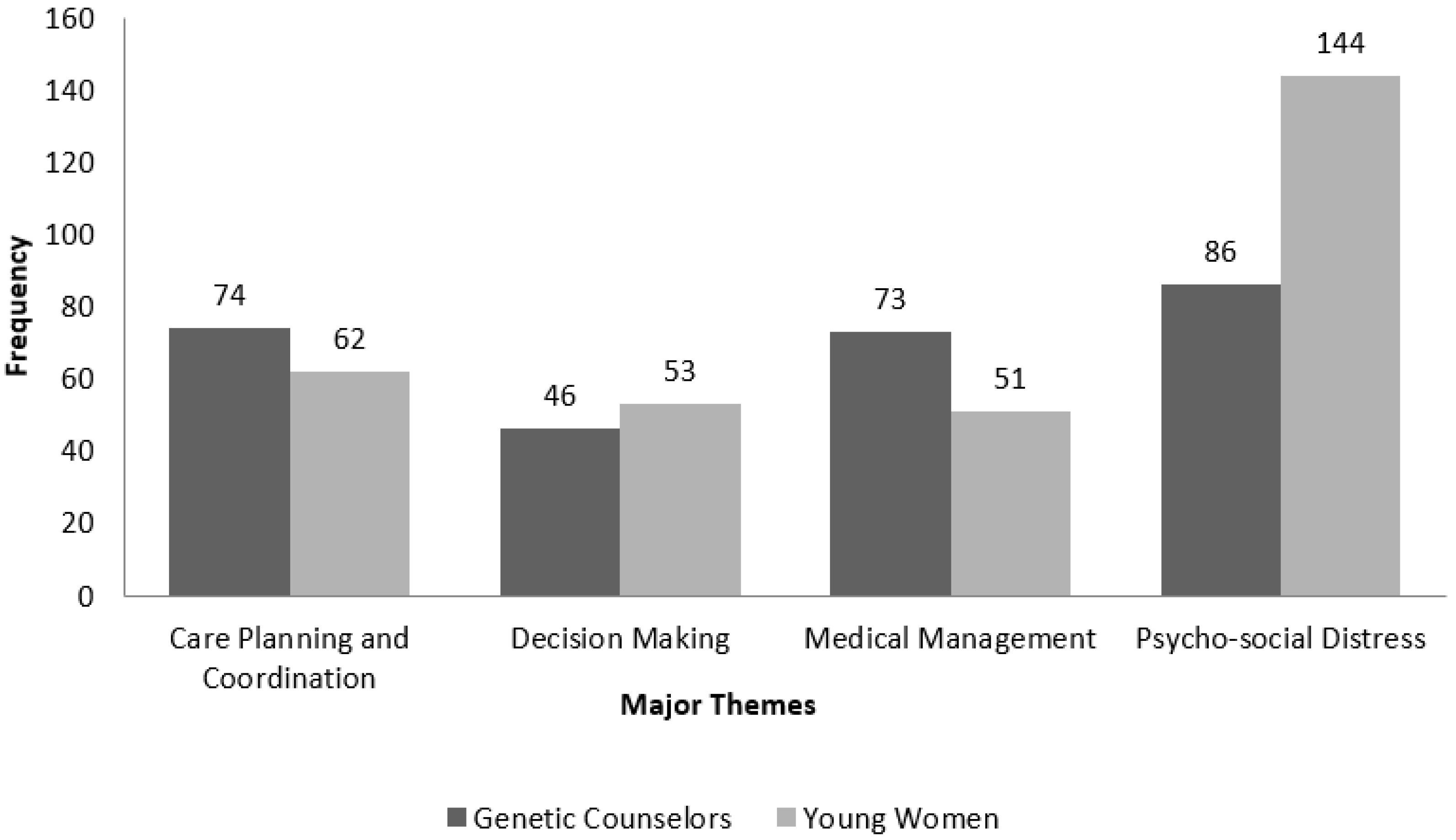
| Themes | Coding Sets | Individual Nodes | Genetic Counselors | Young Women |
|---|---|---|---|---|
| Care planning and coordination | 74 | 62 | ||
| Intervention | 70 | 32 | ||
| Technique | 39 | 11 | ||
| In print resources | 0 | 4 | ||
| Decision support | 4 | 12 | ||
| Long Term Cancer Risk | 7 | 3 | ||
| Short Term Cancer Risk | 11 | 1 | ||
| Affective forecasting | 9 | 1 | ||
| Clinical communication | 4 | 30 | ||
| Young women-talking to providers | 0 | 24 | ||
| Results communication-how delivered | 0 | 3 | ||
| Negative Result-initial reaction | 0 | 3 | ||
| Rapport with young patients | 4 | 0 | ||
| Decisions related to pros and cons | 46 | 53 | ||
| Harms of testing | 27 | 24 | ||
| Life insurance | 3 | 11 | ||
| Harms of testing | 4 | 4 | ||
| GINA | 2 | 2 | ||
| Genetic discrimination | 2 | 0 | ||
| Confusion about what to do with results | 0 | 1 | ||
| Age of testing-potentially too young | 16 | 6 | ||
| Benefits of testing | 19 | 29 | ||
| Young women-testing effects romantic relationships | 2 | 3 | ||
| Work planning | 4 | 5 | ||
| Benefits of testing | 13 | 21 | ||
| Medical management | 73 | 51 | ||
| Fertility | 23 | 11 | ||
| Surgical menopause | 1 | 0 | ||
| Fertility and family planning | 22 | 11 | ||
| Risk Management | 50 | 40 | ||
| Young women-future plans for management | 0 | 25 | ||
| Surgery | 11 | 7 | ||
| Screening | 22 | 2 | ||
| Deciding Not to be tested | 10 | 1 | ||
| Healthcare navigation | 7 | 5 | ||
| Psycho-social Distress | 86 | 144 | ||
| Familial Influences | 45 | 115 | ||
| Young women-sibling discussion | 0 | 10 | ||
| Young women-finding out about family risk | 0 | 28 | ||
| Testing influences | 16 | 16 | ||
| Family Support | 4 | 3 | ||
| Presence of parent changes counseling | 8 | 0 | ||
| Family distress | 12 | 5 | ||
| Negative family communication | 2 | 0 | ||
| Young women sharing results | 0 | 11 | ||
| Family communication | 1 | 26 | ||
| Positive family communication | 2 | 16 | ||
| Peers/Partners | 20 | 7 | ||
| Group support | 8 | 1 | ||
| Friend support | 1 | 0 | ||
| Romantic partner support | 3 | 0 | ||
| Online support | 4 | 3 | ||
| Feelings of isolation | 4 | 3 | ||
| Patient Distress | 21 | 22 | ||
| Patient distress | 21 | 22 |
| Domain | 1–3 N (%) | 4–6 N (%) | 7 + N (%) | Sample Quote |
|---|---|---|---|---|
| Theme 1: Care Planning and Management | 0 (0%) | 2 (22%) | 7 (78%) | n/a |
| Theme 2: Decision Making about BCRA/GT | 0 (0%) | 2 (22%) | 7 (78%) | n/a |
| Theme 3: Medical Management | 0 (0%) | 1 (11%) | 8 (89%) | n/a |
| Theme 4: Psychosocial Distress | 0 (0%) | 2 (22%) | 7 (78%) | n/a |
| Session 1: Information about genetic cancer risks, medical management; how to make medical choices consistent with values/preferences | 0 (0%) | 2 (22%) | 7 (78%) | “It’s something that’s hard to make yourself look for on your own. To have it put together would make it more likely that someone would (use it)”. |
| Session 2: Coping skills; learning where/how to reach out for help | 0 (0%) | 0 (0%) | 9 (100%) | “Even people [who] know how to deal in general with their own stress and anxiety … I think it is a different way of coping that we may not realize we don’t really know how to deal with”. |
| Session 3: Skill building for medical management and patient-provider communication. | 0 (0%) | 1 (11%) | 8 (89%) | “Helping you to be more of a partner in your medical decisions. I think it would be helpful … as far as what to do now that I have my results”. |
| Session 4: Review of skills gained in Session 1–3, focused on self-efficacy in implementing skills. | 0 (0%) | 1 (11%) | 8 (89%) | “It’s very reinforcing, and it’s a good review to make sure that everything is going to be good going forward”. |
| Overall Program Rating | 0 (0%) | 0 (0%) | 9 (100%) | “It sounds like it would be very helpful to young women going through this, and helping decide what they’re going to do, calming them down about it, and making sure that they know they have this communication with their doctor”. |
| Endorsement of a Peer Coach Model | 1 (11%) | 1 (11%) | 7 (78%) | “It would provide that extra layer of support and uniqueness to the program. To talk to somebody who is in similar age group, and recently went through a similar decision and situation would be really helpful”. |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evans, C.; Hamilton, R.J.; Tercyak, K.P.; Peshkin, B.N.; Rabemananjara, K.; Isaacs, C.; O’Neill, S.C. Understanding the Needs of Young Women Regarding Breast Cancer Risk Assessment and Genetic Testing: Convergence and Divergence among Patient-Counselor Perceptions and the Promise of Peer Support. Healthcare 2016, 4, 35. https://doi.org/10.3390/healthcare4030035
Evans C, Hamilton RJ, Tercyak KP, Peshkin BN, Rabemananjara K, Isaacs C, O’Neill SC. Understanding the Needs of Young Women Regarding Breast Cancer Risk Assessment and Genetic Testing: Convergence and Divergence among Patient-Counselor Perceptions and the Promise of Peer Support. Healthcare. 2016; 4(3):35. https://doi.org/10.3390/healthcare4030035
Chicago/Turabian StyleEvans, Chalanda, Rebekah J. Hamilton, Kenneth P. Tercyak, Beth N. Peshkin, Kantoniony Rabemananjara, Claudine Isaacs, and Suzanne C. O’Neill. 2016. "Understanding the Needs of Young Women Regarding Breast Cancer Risk Assessment and Genetic Testing: Convergence and Divergence among Patient-Counselor Perceptions and the Promise of Peer Support" Healthcare 4, no. 3: 35. https://doi.org/10.3390/healthcare4030035
APA StyleEvans, C., Hamilton, R. J., Tercyak, K. P., Peshkin, B. N., Rabemananjara, K., Isaacs, C., & O’Neill, S. C. (2016). Understanding the Needs of Young Women Regarding Breast Cancer Risk Assessment and Genetic Testing: Convergence and Divergence among Patient-Counselor Perceptions and the Promise of Peer Support. Healthcare, 4(3), 35. https://doi.org/10.3390/healthcare4030035