A Community-Directed Integrated Strongyloides Control Program in Queensland, Australia

 , , ,
, , ,  and
and
Abstract
:1. Background and Introduction
1.1. Background
1.2. Introduction
1.3. Context
2. Approach
2.1. Community Participation
2.2. Involvement of Primary School Children
2.3. Treat-and-Test
2.4. Environmental Risk Factors
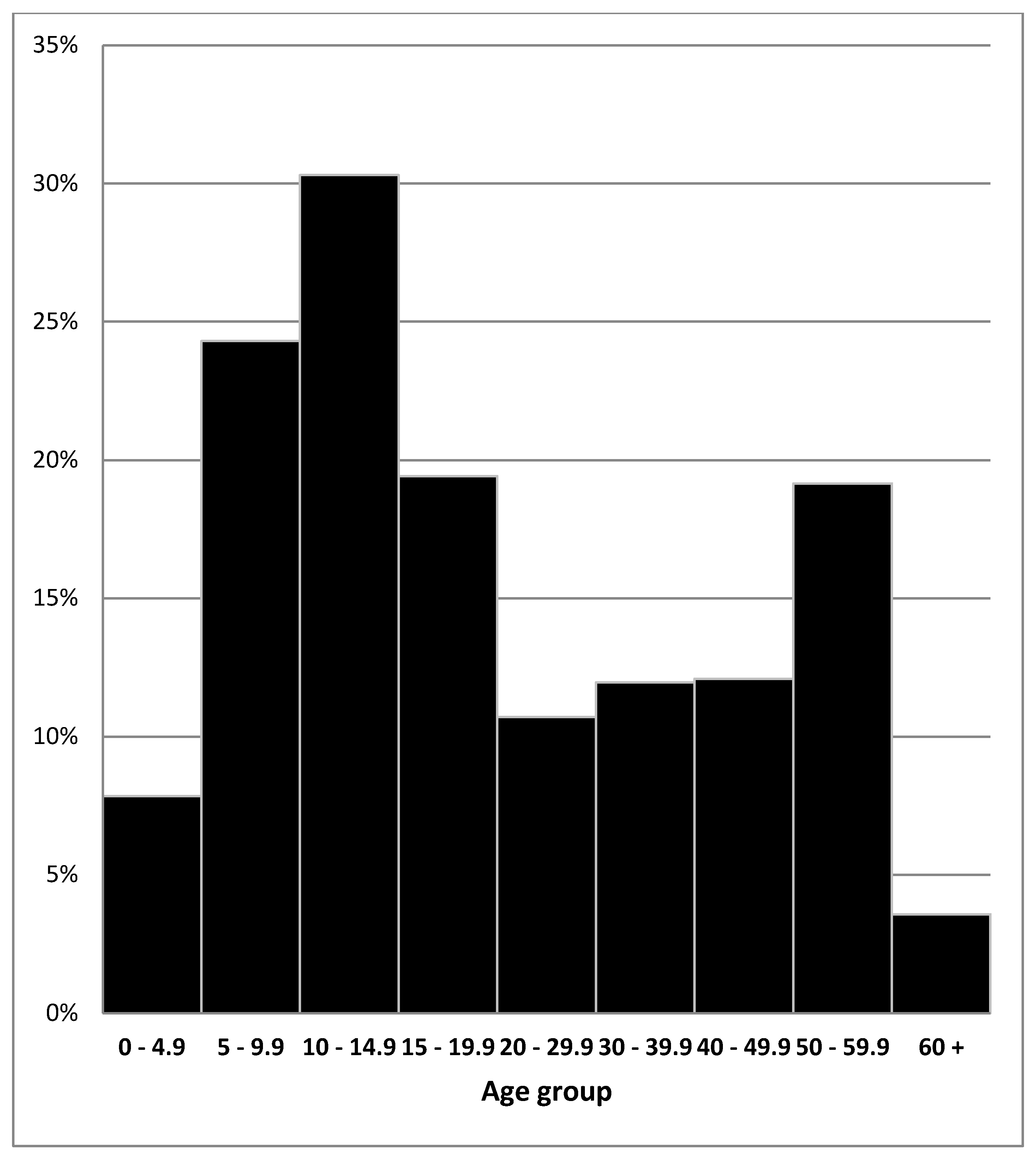
2.5. Serological Results
3. Discussion
3.1. Impact of the Program
3.2. Local Leadership and Knowledge
3.3. Big Effort, But Worth It
3.4. Knowledge and Understanding of the Parasite
3.5. Development of an Inclusive Governance Model and Skills Development
3.6. Aspects to Be Improved
4. Conclusions
Author Contributions
Funding
Acknowledgments
Ethics and Permissions
Conflicts of Interest
References
- Tervalon, M.; Murray-Garcia, J. Cultural humility versus cultural competence: A critical distinction in defining physical training outcomes in multicultural education. J. Health Care Poor Underser. 1998, 9, 117. [Google Scholar] [CrossRef]
- Olsen, A.; van Lieshout, L.; Marti, H.; Polderman, T.; Polman, K.; Steinmann, P.; Stothard, R.; Thybo, S.; Verweij, J.J.; Magnussen, P. Strongyloidiasis—The most neglected of the neglected tropical diseases? Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Puthiyakunnon, S.; Boddu, S.; Li, Y.; Zhou, X.; Wang, C.; Li, J.; Chen, X. Strongyloidiasis—An insight into its global prevalence and management. PLoS Negl. Trop. Dis. 2014, 8, e3018. [Google Scholar] [CrossRef] [PubMed]
- Shield, J.M.; Page, W. Effective diagnostic tests and anthelmintic treatment for Strongyloides stercoralis make community control feasible. PNG Med. J. 2008, 51, 105–119. [Google Scholar]
- Page, W.; Shield, J.; O’Donahoo, F.; Miller, A.; Judd, J.; Speare, R. Strongyloidiasis in Oceania. In Neglected Tropical Diseases—Oceania; Loukas, A., Ed.; Springer: Berlin, Germany, 2016; Chapter 3; pp. 69–99. [Google Scholar]
- Miller, A.; Smith, M.L.; Judd, J.A.; Speare, R. Strongyloides stercoralis: Systematic review of barriers to controlling strongyloidiasis for Australian Indigenous communities. PLoS Negl. Trop. Dis. 2014, 8, e3141. [Google Scholar] [CrossRef] [PubMed]
- Mounsey, K.; Kearns, T.; Rampton, M.; Llewellyn, S.; King, M.; Holt, D.; Currie, B.J.; Andrews, R.; Nutman, T.; McCarthy, J. Use of dried blood spots to define antibody response to the Strongyloides stercoralis recombinant antigen NIE. Acta Trop. 2014, 138, 78–82. [Google Scholar] [CrossRef] [PubMed]
- National Regional Profile: Woorabinda Local Government Area. Available online: http://www.abs.gov.au/AUSSTATS/[email protected]/Previousproducts/LGA37550Population/People12005-2009?opendocument&tabname=Summary&prodno=LGA37550&issue=2005-2009&num=&view= (accessed on 4 June 2015).
- Australian Centre for International and Tropical Health and Nutrition (ACITHN). Environmental Health in Woorabinda: Investigation of Parasite Infections in the Community; The University of Queensland and Queensland Institute of Medical Research: Brisbane, Australia, 1996. [Google Scholar]
- Raeburn, J. and Rootman, I. People Centered Health Promotion; John Wiley and Sons: Toronto, ON, Canada, 1998. [Google Scholar]
- Judd, J.; Frankish CJ and Moulton, G. Setting Standards in the evaluation of community-based health promotion programs—A unifying approach. Health Promot. Int. J. 2001, 16, 367–380. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Ottawa Charter for Health Promotion. Health Promot. 1986, 1, 3–5. [Google Scholar]
- Khieu, V.; Hattendorf, J.; Schär, F.; Marti, H.; Char, M.C.; Muth, S.; Odermatt, P. Strongyloides stercoralis infection and re-infection in a cohort of children in Cambodia. Parasitol. Int. 2014, 63, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Sampson, I.A.; and Grove, D.I. Strongyloidiasis is endemic in another Australian population group: Indochinese immigrants. Med. J. Aust. 1987, 146, 580–582. [Google Scholar] [PubMed]
- Biggs, B.A.; Caruana, S.; Mihrshahi, S.; Jolley, D.; Leydon, J.; Chea, L.; Nuon, S. Management of chronic strongyloidiasis in immigrants and refugees: Is serologic testing useful? Am. J. Trop. Med. Hyg. 2009, 80, 788–791. [Google Scholar] [PubMed]
- Page, W.; Speare, R. Recommendations from the First National Workshop on Strongyloidiasis. Brisbane, 25–26 July 2003. Available online: http://www.tropicalhealthsolutions.com/sites/default/files//uploaded/Recommendations-1NWS.pdf (accessed on 15 March 2018).
- Conway, D.J.; Lindo, J.F.; Robinson, R.D.; Bundy, D.A.P. Towards effective control of Strongyloides stercoralis. Parasitol. Today 1995, 11, 421–424. [Google Scholar] [CrossRef]
- Toma, H.; Shimabukura, I.; Kobayashi, J.; Tasaki, T.; Takara, M.; Sato, Y. Community control studies on Strongyloides infection in a model island of Okinawa, Japan. Southeast Asian J. Trop. Med. Public Health 2000, 31, 383–387. [Google Scholar] [PubMed]
- Speare, R.; Miller, A.; Page, W. Strongyloidiasis: A case for notification in Australia? Med. J. Aust. 2015, 202, 523–524. [Google Scholar] [CrossRef] [PubMed]
- Massey, P.D.; Miller, A.; Saggers, S.; Durrheim, D.N.; Speare, R.; Taylor, K.; Pearce, G.; Odo, T.; Broome, J.; Judd, J.; et al. Australian Aboriginal and Torres Strait Islander communities and the development of pandemic influenza containment strategies: Community voices and community control. Health Policy 2011, 103, 184–190. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Months After Commencement | Action | Responsibility * |
|---|---|---|
| 3–4 months | Formation of a steering committee | DON |
| Adoption of program plan | Steering committee | |
| Appointment of personnel to conduct program | DON | |
| Develop consent forms: ivermectin, albendazole, beta-HCG (test for pregnancy), release of information. | PO/RN | |
| Develop data collection tools for treatment—paper and electronic | PO/RN | |
| Develop drug recording systems | PO/RN | |
| Develop management flow chart | PO/RN | |
| Develop education and awareness-raising materials | PO/RN | |
| Collect baseline data results from previous studies conducted in Woorabinda and develop evaluation measures for comparison: (a) Environmental health and household survey; (b) Animal census. | PO | |
| Environmental health program commences | EHO, EH Coordinator/HW’s/Council | |
| Education and awareness-raising commences | HW | |
| 6 months | Pilot of initial treatment | DR/RN/HW |
| Review and modification of management flow chart | Steering Committee | |
| Environmental health program continues | EHO, EH Coordinator/HW’s/Council | |
| Initial serology/treatment of community | DR/RN/HW | |
| Follow-up of community members not presenting for treatment/re-treatment of positive cases at two weeks | RN/HW | |
| Education and awareness-raising continues | HW | |
| Environmental health program continues | EHO, EH Coordinator/HW’s/Council | |
| Analysis of results from initial treatment and report | RN | |
| 12–13 months | First follow-up serology and treatment of resistant/positive cases. | DR/RN/HW |
| Follow-up community members who have not presented for serology and treatment/resistant cases | RN/HW | |
| Analysis of results from first follow-up and report | RN | |
| Second follow-up treatment for resistant cases | DR/RN/HW | |
| Follow-up community members not presenting for serology and treatment | RN/HW | |
| Education and awareness raising continues | HW | |
| Environmental health program continues | EHO, EH Coordinator/HW’s/Council | |
| Analysis of results from second follow-up and report | RN | |
| 14 months | Third follow-up serology and treatment | DR/RN/HW |
| Follow-up community members not presenting for serology and treatment | RN/HW | |
| Education and awareness raising continues | HW | |
| Environmental health program continues | EHO, EH Coordinator/HW’s/Council | |
| Analysis of results from third follow-up and report | RN | |
| 21–24 months | Fourth follow-up serology | DR/RN/HW |
| Follow-up community members not presenting for serology and treatment | RN/HW | |
| Education and awareness raising continues | HW | |
| Environmental health program continues | EHO, EH Coordinator/HW’s/Council | |
| Analysis of results from fourth follow-up and report | RN | |
| Refer resistant cases to Dr | RN | |
| Final report and recommendations | RN | |
| Second yearly review to confirm eradication | Health Service |
| The Strongyloides Song |
|---|
| Words by June Barkworth and adapted by the Woorabinda Schoolchildren. The children and staff of the Woorabinda State School wrote the music. This song was used as a signature tune to herald radio updates on the Strongyloides project. No, no, no, ‘Mr Worm’ we don’t want you Travelling through our skin and making us sick, With boots and shoes on our feet (stamp, stamp) Blankets on the ground, We’re gon’na stop you from moving around ‘Our bodies’ Yes, yes, yes, ‘Mr Worm’ you have got to go ho, ho, ho, ho, Go, go, go ‘Mr Worm’ we’re getting tough You have no place to live in us. We’re gon’na thrash you out, we’re gon’na move you on …… then Woorabinda will say that ‘Mr Strongyloides’ worm is gone. Yes, yes, yes ‘Mr Worm’ you have got to go. Ho, ho, ho, ho, ho. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miller, A.; Young, E.L.; Tye, V.; Cody, R.; Muscat, M.; Saunders, V.; Smith, M.L.; Judd, J.A.; Speare, R. A Community-Directed Integrated Strongyloides Control Program in Queensland, Australia. Trop. Med. Infect. Dis. 2018, 3, 48. https://doi.org/10.3390/tropicalmed3020048
Miller A, Young EL, Tye V, Cody R, Muscat M, Saunders V, Smith ML, Judd JA, Speare R. A Community-Directed Integrated Strongyloides Control Program in Queensland, Australia. Tropical Medicine and Infectious Disease. 2018; 3(2):48. https://doi.org/10.3390/tropicalmed3020048
Chicago/Turabian StyleMiller, Adrian, Elizebeth L. Young, Valarie Tye, Robert Cody, Melody Muscat, Vicki Saunders, Michelle L. Smith, Jenni A. Judd, and Rick Speare. 2018. "A Community-Directed Integrated Strongyloides Control Program in Queensland, Australia" Tropical Medicine and Infectious Disease 3, no. 2: 48. https://doi.org/10.3390/tropicalmed3020048