Melioidosis in South America



Abstract
:1. Introduction
2. Review of Published Melioidosis Cases and the Presence of B. pseudomallei
2.1. Venezuela, Colombia and Peru
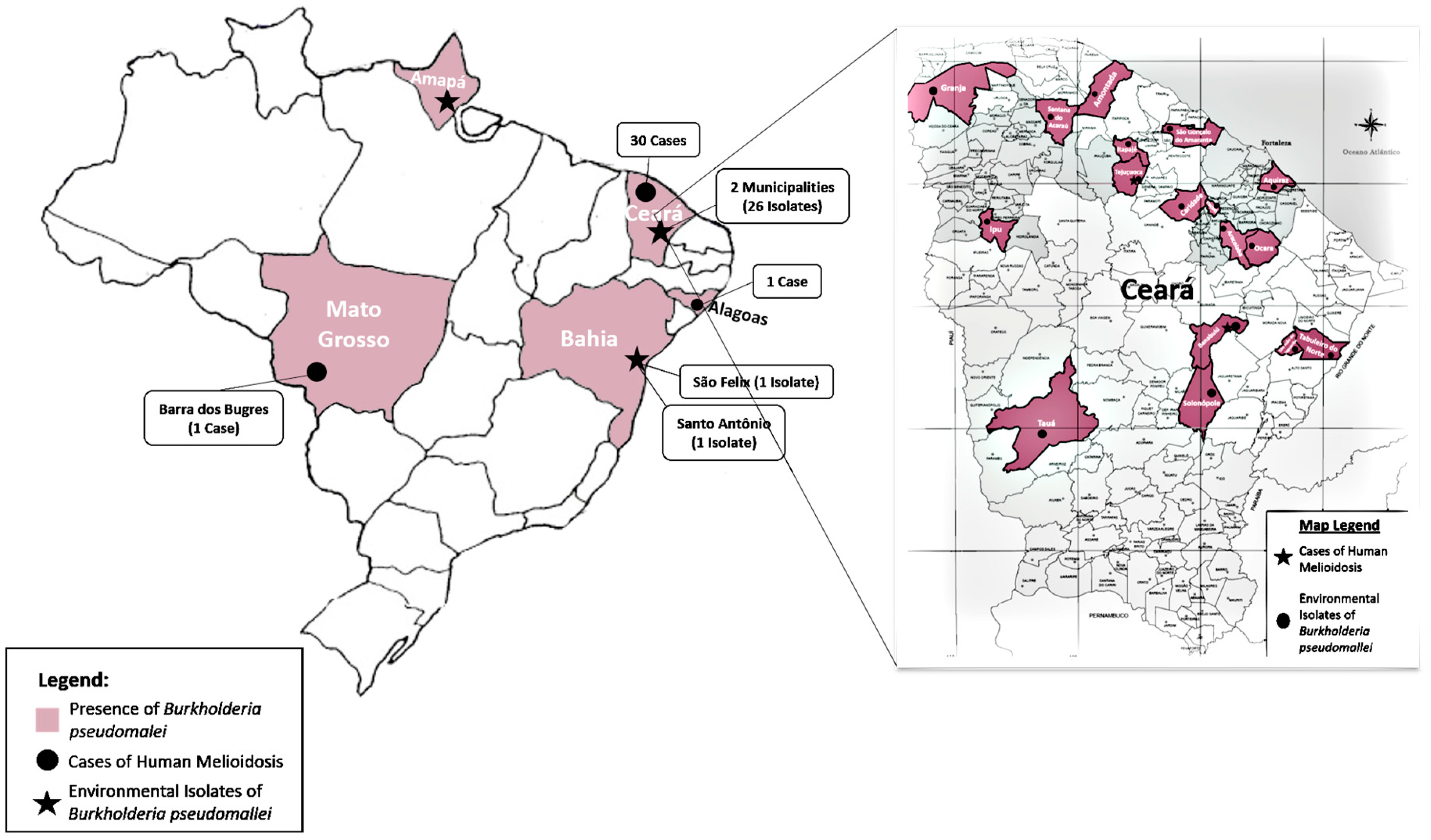
2.2. Brazil
2.3. Environmental Isolation
2.4. Animal Melioidosis
3. Surveillance and Public Policies in South America
4. Current Challenges and Perspective
- To raise professional and government awareness that this disease is present.
- To alert clinicians to the fact that its early detection is critical if lives are to be saved.
Acknowledgments
Conflicts of Interest
References
- Limmathurotsakul, D.; Golding, N.; Dance, D.A.B.; Messina, J.P.; Pigott, D.M.; Moyes, C.L.; Rolim, D.B.; Bertherat, E.; Day, N.P.J.; Peacock, S.J.; et al. Predicted global distribution of Burkholderia pseudomallei and burden of melioidosis. Nat. Microbiol. 2016, 1, 15008. [Google Scholar] [CrossRef] [PubMed]
- Benoit, T.; Blaney, D.D.; Doker, T.J.; Gee, J.E.; Mindy, G.; Elrod, M.; Rolim, D.B.; Inglis, T.J.J.; Hoffmaster, A.R.; Bower, A.W.; et al. Review article: A review of melioidosis cases in the Americas. Am. J. Trop. Med. Hyg. 2015, 93, 1134–1139. [Google Scholar] [CrossRef] [PubMed]
- Biegeleisen, J.Z., Jr.; Mosquera, R.; Cherry, W.B. A case of human melioidosis: Clinical, epidemiological and laboratory findings. Am. J. Trop. Med. Hyg. 1964, 13, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Redondo, M.C.; Gómez, M.; Landaeta, M.E.; Ríos, H.; Khalil, R.; Guevara, R.N.; Palavecino, S.; Figuera, M.; Caldera, J.; Rivera, R.; et al. Melioidosis presenting as sepsis syndrome: A case report. Int. J. Infect. Dis. 2011, 15, E217–E218. [Google Scholar] [CrossRef] [PubMed]
- Montufar, F.E.; Ochoa, J.E.; Ortega, H.; Franco, L.; Montufar, M.C.; Monsalve, A.; Jaramillo, C.; Zapata, M. Melioidosis in Antioquia, Colombia: An emerging or endemic disease? A cases series. Int. J. Infect. Dis. 2015, 37, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Magalhaes, S.; Paiva, A.; Henrique, R.; Koch, A. Melioidose; diagnostico diferencial de tumor renal. Acta Urol. 2003, 2, 31. [Google Scholar]
- Miralles, I.S.; do Carmo Alves Maciel, M.; Angelo, M.R.F.; Gondini, M.M.; Frota, L.H.F.; dos Reis, C.M.F.; Hofer, E. Burkholderia pseudomallei: A case report of a human infection in Ceara, Brazil. Rev. Inst. Med. Trop. São Paulo 2004, 46, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Rolim, D.B.; Vilar, D.C.; Sousa, A.Q.; Miralles, I.S.; de Oliveira, D.; Harnett, G.; O’Reilly, L.; Howard, K.; Sampson, I.; Inglis, T.J.J. Melioidosis, northeastern Brazil. Emerg. Infect. Dis. 2005, 11, 1458–1460. [Google Scholar] [CrossRef] [PubMed]
- Braga, M.D.; Almeida, P.R. First description of an autopsied case of melioidosis in Ceara State. Rev. Soc. Bras. Med. Trop. 2005, 38, 58–60. [Google Scholar] [CrossRef] [PubMed]
- Virginio, C.G.; Teixeira, M.F.; Frota, C.C.; Café, V.S.; Rocha, M.F.; Sidrim, J.J. Phenotypic characterization of three clinical isolates of Burkholderia pseudomallei in Ceara, Brazil. Mem. Inst. Oswaldo Cruz 2006, 101, 95–97. [Google Scholar] [CrossRef] [PubMed]
- Aardema, H.; Luijnenburg, E.M.; Salm, E.F.; Bijlmer, H.A.; Visser, C.E.; Van’tWout, J.W. Changing epidemiology of melioidosis? A case of acute pulmonary melioidosis with fatal outcome imported from Brazil. Epidemiol. Infect. 2005, 133, 871–875. [Google Scholar] [CrossRef] [PubMed]
- Barth, A.L.; Silva, F.A.; Hoffmann, A.; Vieira, M.I.; Zavascki, A.P.; Ferreira, A.; da Cunha, L.G., Jr.; Albano, R.M.; de Andrade Marques, E. Cystic fibrosis patient with Burkholderia pseudomallei infection acquired in Brazil. J. Clin. Microbiol. 2007, 45, 4077–4080. [Google Scholar] [CrossRef] [PubMed]
- Inglis, T.J.; Rolim, D.B.; Sousa, AQ. Melioidosis in the Americas. Am. J. Trop. Med. Hyg. 2006, 75, 947–954. [Google Scholar] [PubMed]
- Gonzalez, G.; Mantilla, W.A.; Rada, R. Neumonía y osteomielitis por Burkholderia pseudomallei, reporte de un casoclínico. Rev. Med. 2009, 17, 146–149. [Google Scholar]
- Couto, M.S.; de AguiarCordeiro, R.; Rocha, M.F.; Grangeiro, T.B.; Leitao Junior, N.P.; de Jesus Pinheiro Gomes Bandeira, T.; Sidrim, J.J.C.; Brilhante, R.S.N. A diagnosis of Burkholderia pseudomallei directly in a bronchoalveolar lavage by polymerase chain reaction. Diagn. Microbiol. Infect. Dis. 2009, 65, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Sidrim, J.J.; Rocha, M.F.; Bandeira, T.J.; Cordeiro, R.A.; Carvalho, B.M.; Grangeiro, T.B.; Holanda, M.A.; Valente, L.G.; Costa, A.K.; Brilhante, R.S. Mycotic aneurysm caused by Burkholderia pseudomallei: Report of a Brazilian strain genetically related to Thai strains. Clin. Microbiol. Infect. 2011, 17, 719–721. [Google Scholar] [CrossRef] [PubMed]
- Brilhante, R.S.; Bandeira, T.J.; Cordeiro, R.A.; Grangeiro, T.B.; Lima, R.A.; Ribeiro, J.F.; Castelo-Branco, D.S.; Rodrigues, J.; Coelho, I.C.; Magalhães, F.G.; et al. Clinical-epidemiological features of 13 cases of melioidosis in Brazil. J. Clin. Microbiol. 2012, 50, 3349–3352. [Google Scholar] [CrossRef] [PubMed]
- Macedo, R.N.; Rocha, F.A.; Rolim, D.B.; Vilar, D.C.; Araújo, F.M.; Vieira, N.N.; Teixeira, J.R.; Carvalho, M.C.; Oliveira, F.G.; Cavalcanti, L.P. Severe coinfection of melioidosis and dengue fever in northeastern Brazil: First case report. Rev. Soc. Bras. Med. Trop. 2012, 45, 132–133. [Google Scholar] [CrossRef] [PubMed]
- Arellano, C.H.R.; Gómez, G.; Sanjuán, O.I.G. Cough and dyspnea during six years in a young adult with chronic pulmonary melioidosis: Case report. Med. Lab. 2013, 19, 1–8. [Google Scholar]
- Nasner-Posso, K.M.; Cruz-Calderon, S.; Rodriguez-Morales, A.J.; Montufar-Andrade, F.E. Melioidosis: A sporadic or an emerging disease in Colombia? Enferm. Infecc. Microbiol. Clin. 2015, 33, 206–207. [Google Scholar] [CrossRef] [PubMed]
- ProMEDmail. Melioidosis—Peru. 2016. Available online: http://www.promedmail.org/post/4624371 (accessed on 15 February 2018).
- Carmona, H.E.O.; Duran, L.F. Melioidosis: A case report in the department of Huila—Colombia. RFS Rev. Fac. Salud Univ. Surcolomb. 2014, 6, 56–59. [Google Scholar] [CrossRef]
- Rolim, D.B.; Rodrigues, J.L.N.; Vilar, D.C.F.L.; Ribeiro, A.K.C.; Castelo-Branco, D.S.; Bandeira, T.J.; Cordeiro, R.A.; Brilhante, R.S.; Gonçalves, A.L.M.; Cavalcanti, V.; et al. The epidemiology and clinical spectrum of melioidosis in Brazil: A fifteen-year review. (manuscript in preparation).
- Galimand, M.; Dodin, A. Le point sur la mélioïdose dans le monde. Bull. Soc. Path. 1982, 75, 375–383. [Google Scholar]
- Dance, D.A. Melioidosis: The tip of the iceberg? Clin. Microbiol. Rev. 1991, 4, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Chewapreecha, C.; Holden, M.T.; Vehkala, M.; Valimaki, N.; Yang, Z.; Harris, S.R.; Mather, A.E.; Tuanyok, A.; De Smet, B.; Le Hello, S.; et al. Global and regional dissemination and evolution of Burkholderia pseudomallei. Nat. Microbiol. 2017, 2, 16263. [Google Scholar] [CrossRef] [PubMed]
- Severiche, D. Pseudomonas pseudomallei community acquired pneumonia. Rev. Colomb. Neumol. 1998, 10, 188–192. [Google Scholar]
- Montufar, F.E.; Acosta, J.O.; Ortega, H.; Franco, L. Melioidosis in Colombia. An emerging disease. Chest 2011, 140, 753A. [Google Scholar] [CrossRef]
- Guzman-Gomez, L.; Agudo Bilbao, M.; Peiro-Callizo, E.; Salas, C. Melioidosis imported from Colombia to Spain. Enferm. Infecc. Microbiol. Clin. 2015, 33, 214–216. [Google Scholar] [CrossRef] [PubMed]
- Bandeira, T.D.J.P.G.; Castelo-Branco, D.D.S.C.M.; Rocha, M.F.G.; Cordeiro, R.D.A.; Ocadaque, C.J.; Paiva, M.D.A.N.; Brilhante, R.S.N.; Sidrim, J.J.C. Clinical and environmental isolates of Burkholderia pseudomallei from Brazil: Genotyping and detection of virulence gene. Asian Pac. J. Trop. Med. 2017, 10, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Rolim, D.B.; Rocha, M.F.G.; Brilhante, R.S.N.; Cordeiro, R.A.; Leitão-Junior, N.P.; Inglis, T.J.J.; Sidrim, J.J.C. Environmental Isolates of Burkholderia pseudomallei in Ceará State, Northeastern Brazil. Appl. Environ. Microbiol. 2009, 75, 215–1218. [Google Scholar] [CrossRef] [PubMed]
- Sousa, V.Y.K.; Segovia, J.F.O.; Martins Junior, P.O.; Bezerra, R.S.; Gonçalves, M.C.A.; Pereira, S.W.M.; Vallim, D.C.; Carvalho-Assef, A.P.D.; Hofer, E.; Kanzaki, L.I.B. Molecular studies of the first report of Burkholderia pseudomallei isolation from soil collected in the Amapá State, in Northern Brazil. Int. J. Biol. 2016, 8, 1. [Google Scholar] [CrossRef]
- De Castro, A.F.; Campedelli Filho, O.; Giorgi, W.; Rosa, C.A. Melioidosis and its causative agent: Pseudomonas pseudomallei. Rev. Inst. Med. Trop. São Paulo 1973, 15, 43–49. [Google Scholar] [PubMed]
- Rolim, D.B. Epidemiological study of first melioidosis outbreak in Brazil. Master’s Thesis, Universidade Federal do Ceará, Fortaleza, Brazil, 2004. [Google Scholar]
- Mendas, E.V. 25 anos do Sistema Único de Saúde: Resultados e desafios. Estud. Avançados 2013, 27, 27–34. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Case | Age | Gender | Year of Diagnosis | Country of Diagnosis | Country Where Infection Was Most Likely Acquired | Outcome | References |
|---|---|---|---|---|---|---|---|
| 1 | 30 | M | 1962 | Ecuador | Ecuador | Died | [3] |
| 2 | 50 | M | 1995 | Venezuela | Venezuela | Survived | [4] |
| 3 | 60 | M | 1998 | Colombia | Colombia | Survived | [5] |
| 4 | 65 | M | 1998 | Colombia | Colombia | Survived | [5] |
| 5 | 50 | M | 2000 | Venezuela | Venezuela | Survived | [4] |
| 6 | 66 | M | 2003 | Portugal | Venezuela | Survived | [6] |
| 7 | 10 | F | 2003 | Colombia | Colombia | Died | [5] |
| 8 | 40 | M | 2003 | Colombia | Colombia | Died | [5] |
| 9 | 15 | M | 2003 | Brazil | Brazil | Died | [7,8,9,10] |
| 10 | 14 | F | 2003 | Brazil | Brazil | Died | [7,8,9,10] |
| 11 | 10 | M | 2003 | Brazil | Brazil | Died | [7,8,9,10] |
| 12 | 12 | F | 2003 | Brazil | Brazil | Survived | [7,8,9,10] |
| 13 | 50 | M | 2003 | Netherlands | Brazil | Died | [11] |
| 14 | 46 | F | 2004 | Colombia | Colombia | Survived | [5] |
| 15 | 28 | M | 2005 | Spain | Colombia | Survived | [5] |
| 16 | 52 | M | 2005 | Colombia | Colombia | Survived | [5] |
| 17 | 17 | F | 2005 | Brazil | Brazil | Survived | [12] |
| 18 | 30 | M | 2005 | Brazil | Brazil | Died | [2,13] |
| 19 | 22 | M | 2008 | Colombia | Colombia | Survived | [14] |
| 20 | 17 | M | 2008 | Brazil | Brazil | Died | [15] |
| 21 | 69 | M | 2008 | Brazil | Brazil | Died | [16,17] |
| 22 | 48 | M | 2009 | Brazil | Brazil | Survived | [17] |
| 23 | 47 | M | 2010 | Brazil | Brazil | Survived | [17] |
| 24 | 28 | M | 2010 | Brazil | Brazil | Died | [18] |
| 25 | 29 | M | 2010 | Brazil | Brazil | Died | [2] |
| 26 | 56 | M | 2010 | Brazil | Brazil | Survived | [2] |
| 27 | 53 | M | 2011 | Brazil | Brazil | Survived | [2] |
| 28 | 3 | M | 2011 | Brazil | Brazil | Died | [2] |
| 29 | 56 | M | 2011 | Brazil | Brazil | Died | [2] |
| 30 | 7 | M | 2011 | Brazil | Brazil | Survived | [2] |
| 31 | 29 | M | 2011 | Brazil | Brazil | Survived | [2] |
| 32 | 21 | M | 2012 | Brazil | Brazil | Died | [2] |
| 33 | 82 | F | 2012 | Brazil | Brazil | Died | [2] |
| 34 | 31 | M | 2012 | Colombia | Colombia | Survived | [5] |
| 35 | 36 | M | 2013 | Colombia | Colombia | Survived | [19,20] |
| 36 | 19 | F | 2016 | Peru | Peru | Died | [21] |
| 37 | 68 | M | 2013 | Brazil | Brazil | Died | [2] |
| 38 | 57 | M | 2014 | Brazil | Brazil | Died | [2] |
| 39 | 42 | M | 2014 | Brazil | Brazil | Survived | [2] |
| 40 | 57 | M | 2014 | Brazil | Brazil | Survived | [2] |
| 41 | 50 | M | 2014 | Brazil | Brazil | Died | [2] |
| 41 | 72 | M | 2014? | Colombia | Colombia | Survived | [22] |
| 42 | 42 | M | 2015 | Brazil | Brazil | Survived | [2] |
| 43 | 13 | F | 2015 | Brazil | Brazil | Died | [23] |
| 44 | 64 | M | 2016 | Brazil | Brazil | Survived | [23] |
| 45 | 58 | M | 2016 | Brazil | Brazil | Died | [23] |
| 46 | 54 | M | 2016 | Brazil | Brazil | Survived | [23] |
| 47 | 100 | M | 2017 | Brazil | Brazil | Died | [23] |
| 48 | 4 | F | 2017 | Brazil | Brazil | Survived | [23] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rolim, D.B.; Lima, R.X.R.; Ribeiro, A.K.C.; Colares, R.M.; Lima, L.D.Q.; Rodríguez-Morales, A.J.; Montúfar, F.E.; Dance, D.A.B. Melioidosis in South America. Trop. Med. Infect. Dis. 2018, 3, 60. https://doi.org/10.3390/tropicalmed3020060
Rolim DB, Lima RXR, Ribeiro AKC, Colares RM, Lima LDQ, Rodríguez-Morales AJ, Montúfar FE, Dance DAB. Melioidosis in South America. Tropical Medicine and Infectious Disease. 2018; 3(2):60. https://doi.org/10.3390/tropicalmed3020060
Chicago/Turabian StyleRolim, Dionne B., Rachel Ximenes R. Lima, Ana Karoline C. Ribeiro, Rafael M. Colares, Leoniti D. Q. Lima, Alfonso J. Rodríguez-Morales, Franco E. Montúfar, and David A. B. Dance. 2018. "Melioidosis in South America" Tropical Medicine and Infectious Disease 3, no. 2: 60. https://doi.org/10.3390/tropicalmed3020060