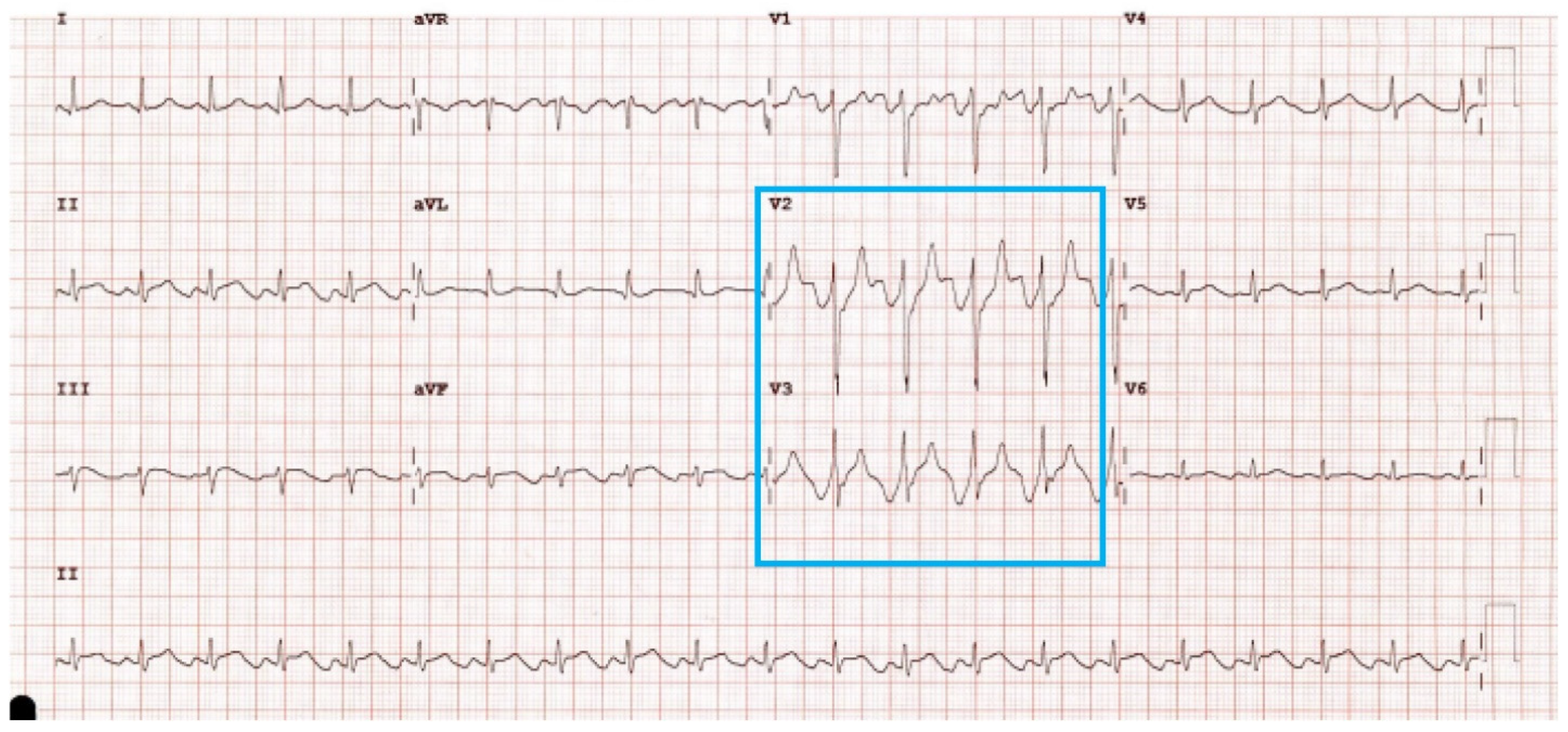
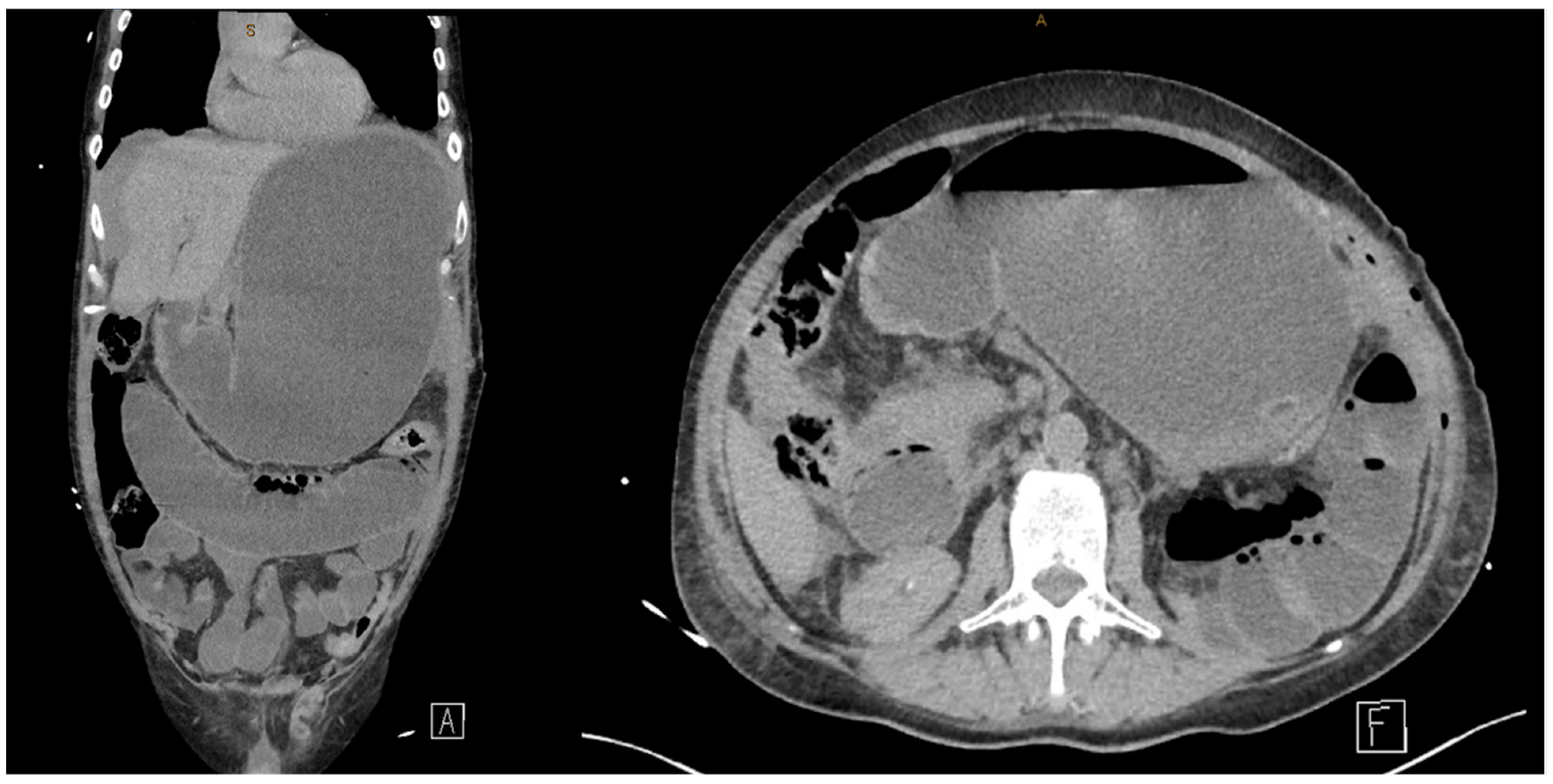
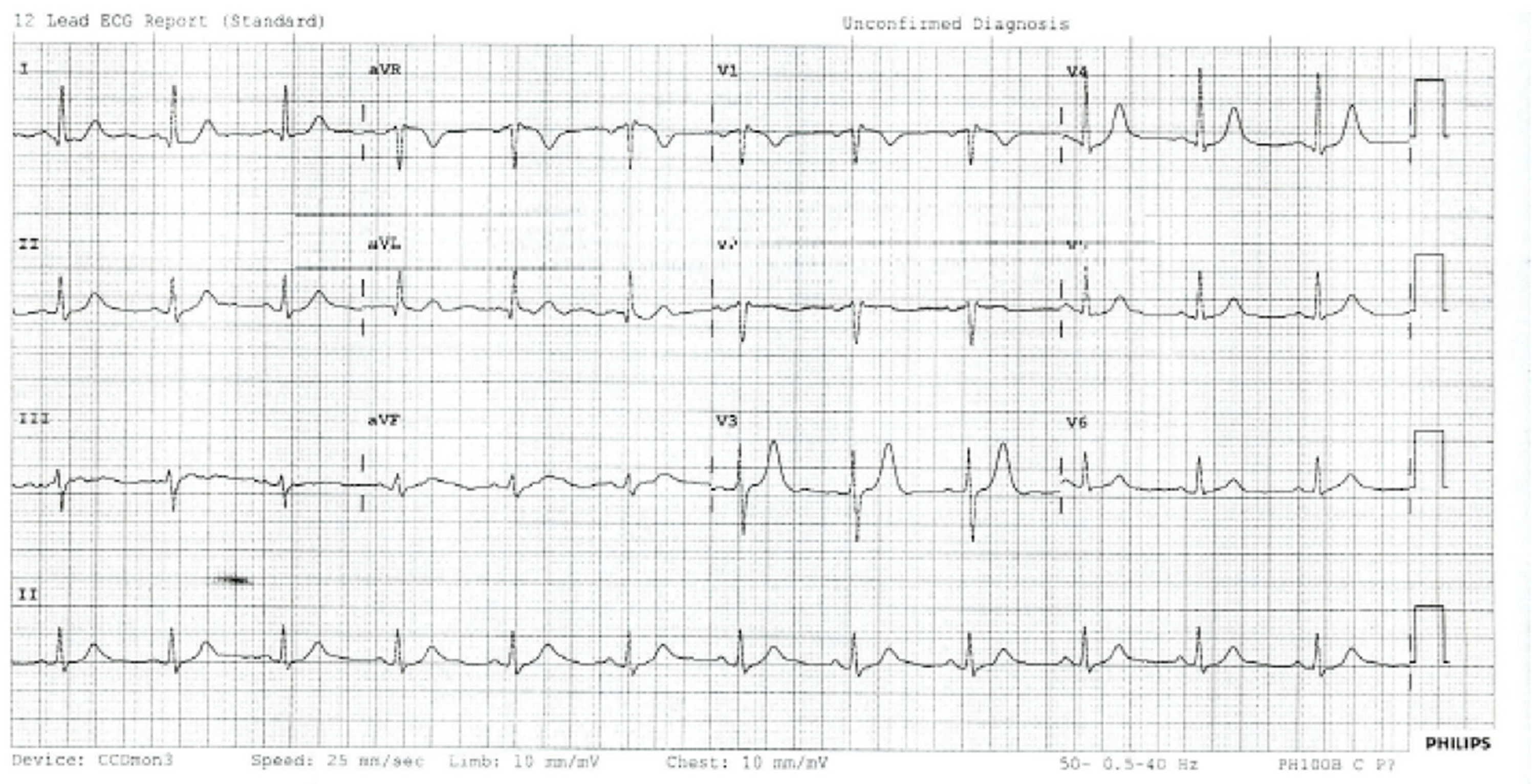
The “Spiked Helmet Sign”, a Mimic of ST-Elevation Myocardial Infarction in Post-Nephrectomy Ileus


{kind=link}
{kind=link}
{kind=link}
Abstract
:Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Littmann, L.; Monroe, M.H. The “spiked helmet” sign: A new electrocardiographic marker of critical illness and high risk of death. Mayo Clin. Proc. 2011, 86, 1245–1246. [Google Scholar] [CrossRef] [PubMed]
- De Bernardi, C.; Halasz, G.; Cattaneo, M. Spiked Helmet Electrocardiographic Sign in a Patient with a Diagnosis of Thoracoabdominal Aortic Dissection. JACC Case Rep. 2020, 2, 2353–2357. [Google Scholar] [CrossRef] [PubMed]
- Salvador-Casabón, J.; Escota-Villanueva, J.; Casanova-Esteban, P.; Ortiz-Giménez, R.; Cantero-Lozano, D.; Pelegrín-Diaz, J. Cardiac extrinsic compression due to abdominal distension as a cause of electrocardiographic abnormality in a critically ill patient. J. Mol. Clin. Med. 2020, 3, 87. [Google Scholar] [CrossRef]
- Cisewski, D.H.; Madias, J.E.; Wong, L. Utilization of the Electrocardiographic “Spiked Helmet” Sign in the Diagnosis of Intra-Abdominal Pathology Within the Emergency Setting. J. Emerg. Med. 2019, 57, 390–394. [Google Scholar] [CrossRef] [PubMed]
- Herath, H.M.; Thushara Matthias, A.; Keragala, B.S.; Udeshika, W.A.; Kulatunga, A. Gastric dilatation and intestinal obstruction mimicking acute coronary syndrome with dynamic electrocardiographic changes. BMC Cardiovasc. Disord. 2016, 16, 245. [Google Scholar] [CrossRef] [PubMed]
- Reddy, M.J.R.; Johnson, B.; Garg, J. Spiked Helmet Sign. Am. J. Med. 2021, 134, 60–62. [Google Scholar] [CrossRef] [PubMed]
- Tomcsanyi, J.; Fresz, T.; Proctor, P.; Littmann, L. Emergence and resolution of the electrocardiographic spiked helmet sign in acute noncardiac conditions. Am. J. Emerg. Med. 2015, 33, 127.e5–127.e7. [Google Scholar] [CrossRef] [PubMed]
- Littmann, L.; Proctor, P. Real time recognition of the electrocardiographic “spiked helmet” sign in a critically ill patient with pneumothorax. Int. J. Cardiol. 2014, 173, e51–e52. [Google Scholar] [CrossRef] [PubMed]
- Tomcsanyi, J.; Fresz, T.; Bozsik, B. ST elevation anterior “spiked helmet” sign. Mayo Clin. Proc. 2012, 87, 309, author reply. [Google Scholar] [CrossRef] [PubMed]
- Laundon, R.K.; Littmann, L. Spiked helmet pattern ST elevation in subarachnoid hemorrhage. J. Electrocardiol. 2019, 52, 96–98. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wynn, J.; McCafferty, J.; Forsyth, R. The “Spiked Helmet Sign”, a Mimic of ST-Elevation Myocardial Infarction in Post-Nephrectomy Ileus. Soc. Int. Urol. J. 2024, 5, 93-96. https://doi.org/10.3390/siuj5020015
Wynn J, McCafferty J, Forsyth R. The “Spiked Helmet Sign”, a Mimic of ST-Elevation Myocardial Infarction in Post-Nephrectomy Ileus. Société Internationale d’Urologie Journal. 2024; 5(2):93-96. https://doi.org/10.3390/siuj5020015
Chicago/Turabian StyleWynn, Jessica, Jonathan McCafferty, and Robert Forsyth. 2024. "The “Spiked Helmet Sign”, a Mimic of ST-Elevation Myocardial Infarction in Post-Nephrectomy Ileus" Société Internationale d’Urologie Journal 5, no. 2: 93-96. https://doi.org/10.3390/siuj5020015