
Double Diapering Ineffectiveness in Avoiding Adduction and Extension in Newborns Hips

Abstract
:1. Introduction
2. Materials and Methods
- (i)
- single pregnancy with cephalic presentation and physiological postnatal development
- (ii)
- no functional limitations of the hips at clinical examination, particularly those of abduction
- (iii)
- normal range weight
- (iv)
- infants younger than 3 months
- (v)
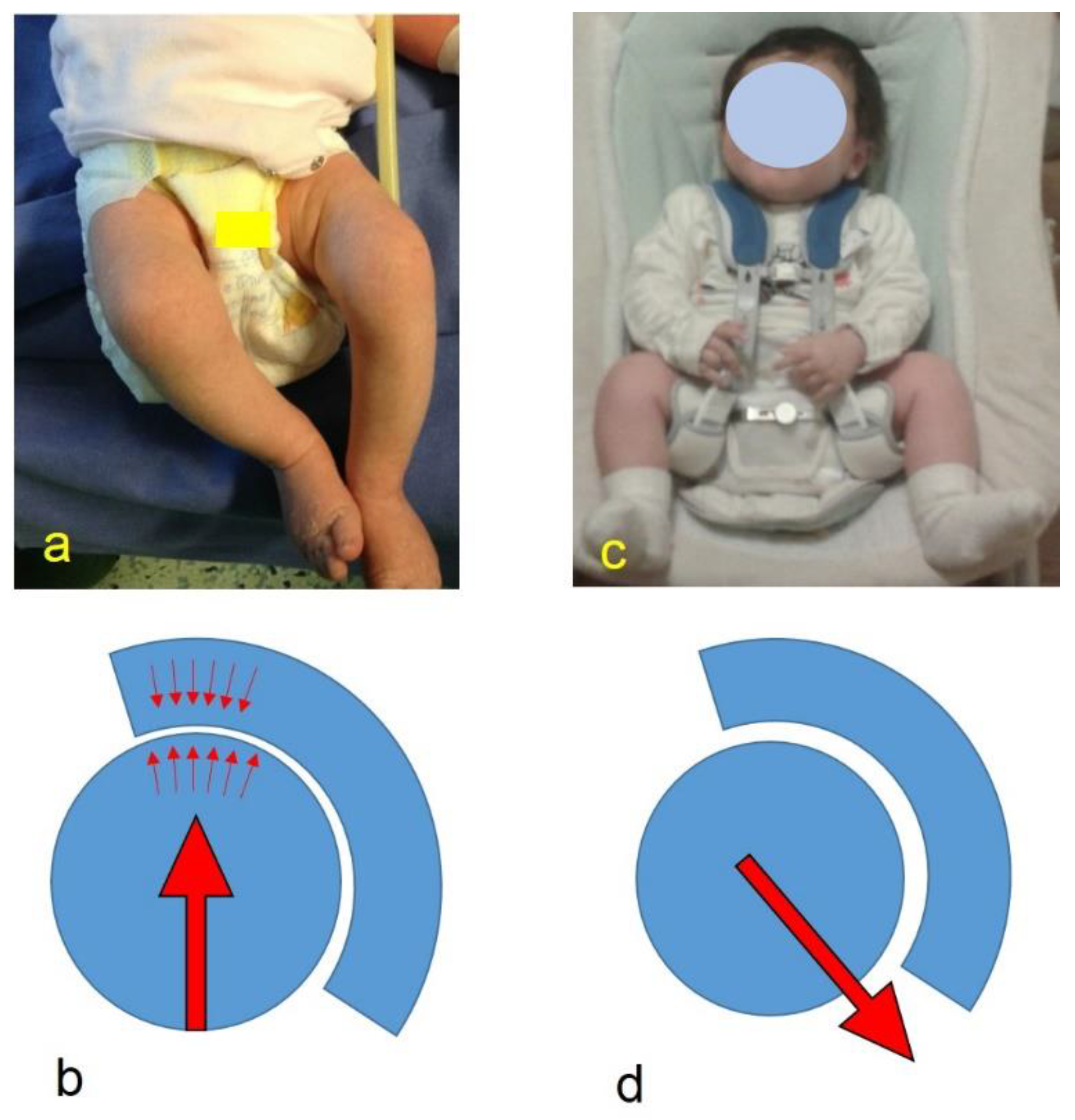
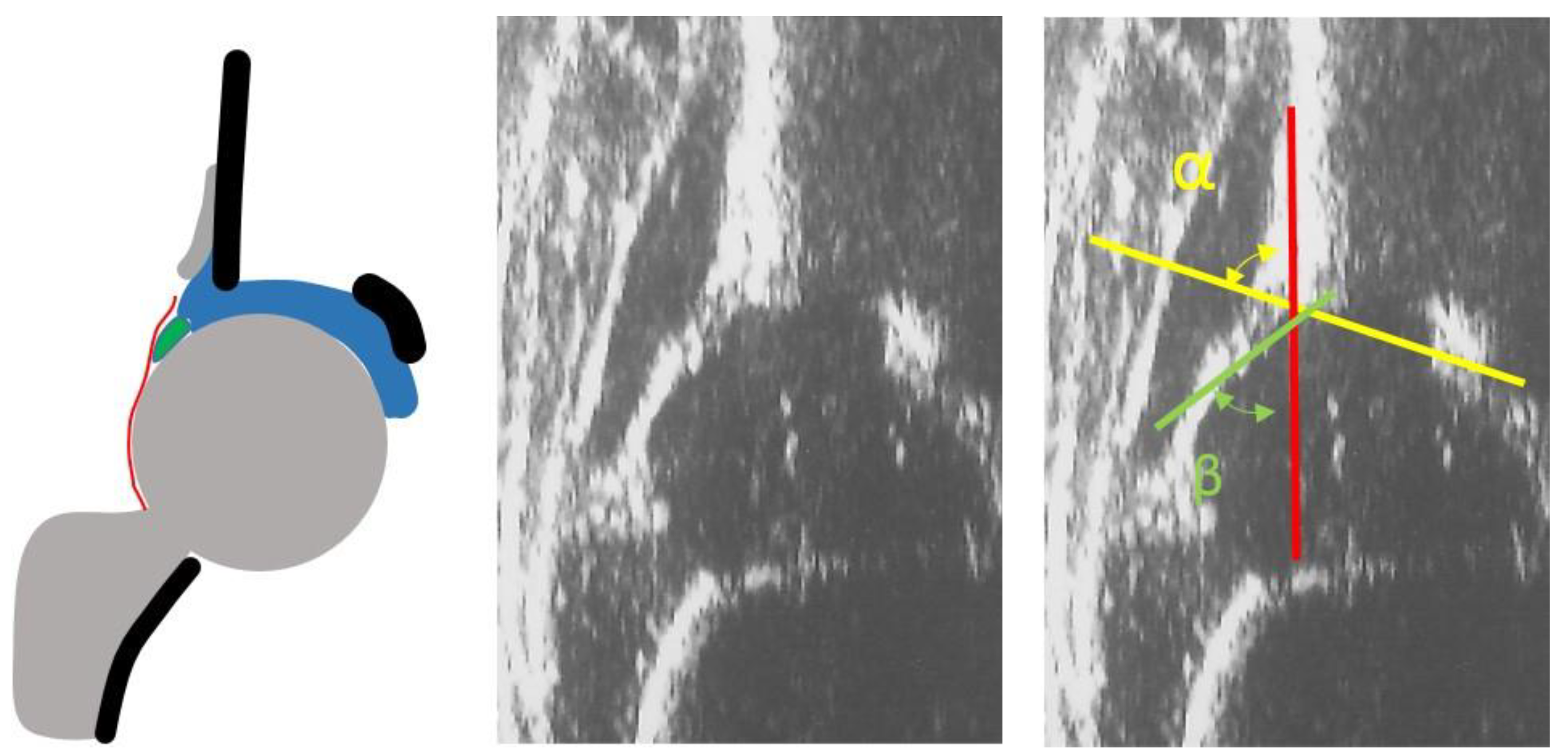
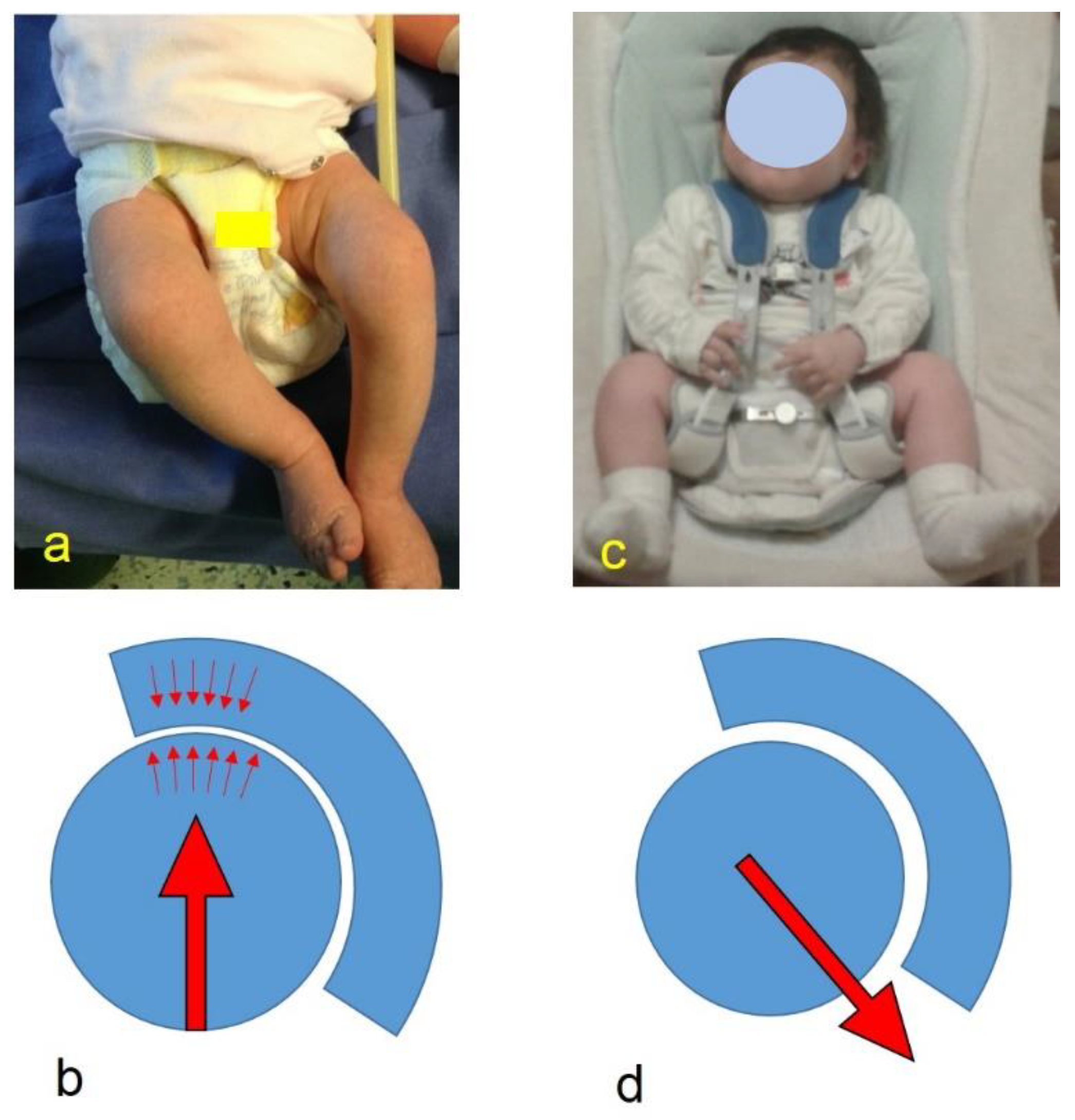
- infants with type I hips at the US examination according to Graf classification (Figure 1)
- (i)
- twins or non-cephalic presentation in pregnancy (breech, transverse) and abnormal postnatal development
- (ii)
- infants who presented with clinical signs of dysplasia or functional limitations of the hips, particularly abduction
- (iii)
- premature or non-normal weight newborns
- (iv)
- infants older than 3 months
- (v)
- infants with non-Type I hips at US examination according to Graf classification
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fettweis, E. Biomechanische Bedingungen der Hüftgelenksreifung. In Das Kindliche Hüftluxations-Leiden; Ecomed-Storck GmbH: Landsberg/Lech, Germany, 1992; pp. 52–62. [Google Scholar]
- Price, C.T.; Ramo, B.A. Prevention of Hip Dysplasia in Children and Adults. Orthop. Clin. North Am. 2012, 43, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Judet, J.; Gielis, L. Dépistage et traitement des luxation congénitales de la hanche. Acta Orthop. Belg. 1959, 25, 440–450. [Google Scholar] [PubMed]
- Omeroglu, H.; Kose, N.; Akceylan, A. Success of Pavlik Harness Treatment Decreases in Patients C 4 Months and in Ultrasonographically Dislocated Hips in Developmental Dysplasia of the Hip. Clin. Orthop. Relat. Res. 2016, 474, 1146–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavone, V.; Testa, G.; Riccioli, M.; Evola, F.R.; Avondo, S.; Sessa, G. Treatment of Developmental Dysplasia of Hip with Tubingen Hip Flexion Splint. J. Pediatr. Orthop. 2015, 35, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Klisic, P.; Zivanovic, V.; Brdar, R. Effects of triple prevention of CDH, stimulated by distribution of “baby packages”. J. Pediatr. Orthop. 1988, 8, 9–11. [Google Scholar] [CrossRef] [PubMed]
- Rosendahl, K.; Dezateux, C.; Aase, H.; Reigstad, H.; Alsaker, T.; Moster, D.; Markestad, T.; Fosse, K.R.; Aukland, S.M.; Lie, R.T. Immediate Treatment Versus Sonographic Surveillance for Mild Hip Dysplasia in Newborns. Pediatrics 2009, 125, e9–e16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teanby, D.N. Ultrasound screening for congenital dislocation of the hip: A limited targeted programm. Blackburn Royal Infirmary, Lancashire, England. J. Pediatr. Orthop. 1997, 17, 202–204. [Google Scholar] [CrossRef] [PubMed]
- Staheli, L. Management of Congenital Hip Dysplasia. Pediatric Ann. Health Res. Prem. Collect. 1989, 18, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Kotlarsky, P.; Haber, R.; Bialik, V.; Eidelman, M. Developmental dysplasia of the hip: What has changed in the last 20 years? World J. Orthop. 2015, 6, 886–901. [Google Scholar] [CrossRef] [PubMed]
- Ergen, E.; Turkmen, E.; Ceylan, M.; Aslan, M.; Felek, S. Evaluating the effectiveness of the national hip dysplasia early diagnosis and treatment program. Med. Sci. Int. Med. J. 2020, 9, 1023. [Google Scholar] [CrossRef]
- Graf, R. Classification of hip joint dysplasia by means of sonography. Arch. Orthop. Trauma Surg. 1984, 102, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Gripp, K.W.; Slavotinek, A.M.; Hall, J.G.; Allanson, J.E. Handbook of Physical Measurements. In Handbook of Physical Measurements; Oxford University Press (OUP): Oxford, UK, 2013; pp. 197–261. [Google Scholar]
- Ramsey, P.; Lasser, S.; MacEwen, G. Congenital dislocation of the hip. Use of the Pavlik harness in the child during the first six months of life. J. Bone Jt. Surg. Am. Vol. 1976, 58, 1000–1004. [Google Scholar] [CrossRef]
- American Academy of Pediatrics Clinical Practice Guideline: Early Detection of Developmental Dysplasia of the Hip. Pediatrics 2000, 105, 896–905. [CrossRef] [PubMed] [Green Version]
- Patel, H.; The Canadian Task Force on Preventive Health Care. Preventive health care, 2001 update: Screening and management of developmental dysplasia of the hip in newborns. CMAJ 2001, 164, 1669–1677. [Google Scholar] [PubMed]
- Storer, S.K.; Skaggs, D.L. Developmental dysplasia of the hip. Am. Fam. Physician 2006, 74, 1310–1316. [Google Scholar] [PubMed]
- Thallinger, C.; Pospischill, R.; Ganger, R.; Radler, C.; Krall, C.; Grill, F. Long-term results of a nationwide general ultrasound screening system for developmental disorders of the hip: The Austrian hip screening program. J. Child. Orthop. 2014, 8, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Beirne, J.G.; Chlapoutakis, K.; Alshryda, S.; Aydingoz, U.; Baumann, T.; Casini, C.; De Pellegrin, M.; Domos, G.; Dubs, B.; Hemmadi, S.; et al. International Interdisciplinary Consensus Meeting on the Evaluation of Developmental Dysplasia of the Hip. Ultraschall Med. Eur. J. Ultrasound 2019, 40, 454–464. [Google Scholar] [CrossRef] [Green Version]
- Agostiniani, R.; Atti, G.; Bonforte, S.; Casini, C.; Cirillo, M.; De Pellegrin, M.; Di Bello, D.; Esposito, F.; Galla, A.; Brunenghi, G.M.; et al. Recommendations for early diagnosis of Developmental Dysplasia of the Hip (DDH): Working group intersociety consensus document. Ital. J. Pediatr. 2020, 46, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Coon, V.; Donato, G.; Houser, C.; Bleck, E.E. Normal rages of hip motion in infant six weeks, three months, and six months of age. Clin. Orthop. Relat. Res. 1975, 110, 256–260. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hips Position | Without Diaper | Double Diapers | p * |
|---|---|---|---|
| R Flexion Average (SD) | 25.25° (18.46°) | 27.5° (21.4°) | 0.33 |
| L Flexion Average (SD) | 25° (18.57°) | 28.64° (22.99°) | 0.34 |
| R Abduction Average (SD) | 24° (8.83°) | 35.06° (26.85°) | 0.87 |
| L Abduction Average (SD) | 23.5° (8.75°) | 34.39° (25.12°) | 0.87 |
| Hips Position | Double Diapers | Caretakers’ Side | p * |
|---|---|---|---|
| R Flexion Average (SD) | 27.5° (21.4°) | 90.74° (9.97°) | < 0.001 |
| L Flexion Average (SD) | 28.64° (22.99°) | 90° (10.38°) | < 0.001 |
| R Abduction Average (SD) | 35.06° (26.85°) | 54.44° (10.13°) | < 0.001 |
| L Abduction Average (SD) | 34.39° (25.12°) | 54.26° (9.87°) | < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Pellegrin, M.; Damia, C.M.; Marcucci, L.; Moharamzadeh, D. Double Diapering Ineffectiveness in Avoiding Adduction and Extension in Newborns Hips. Children 2021, 8, 179. https://doi.org/10.3390/children8030179
De Pellegrin M, Damia CM, Marcucci L, Moharamzadeh D. Double Diapering Ineffectiveness in Avoiding Adduction and Extension in Newborns Hips. Children. 2021; 8(3):179. https://doi.org/10.3390/children8030179
Chicago/Turabian StyleDe Pellegrin, Maurizio, Chiara Maria Damia, Lorenzo Marcucci, and Desiree Moharamzadeh. 2021. "Double Diapering Ineffectiveness in Avoiding Adduction and Extension in Newborns Hips" Children 8, no. 3: 179. https://doi.org/10.3390/children8030179