
Mid-Infrared Photoacoustic Detection of Glucose in Human Skin: Towards Non-Invasive Diagnostics

Abstract
:1. Introduction
2. Photoacoustic Detection: Theory
3. Experimental Arrangements
3.1. Setup with Fiber-Coupled EC-QCL
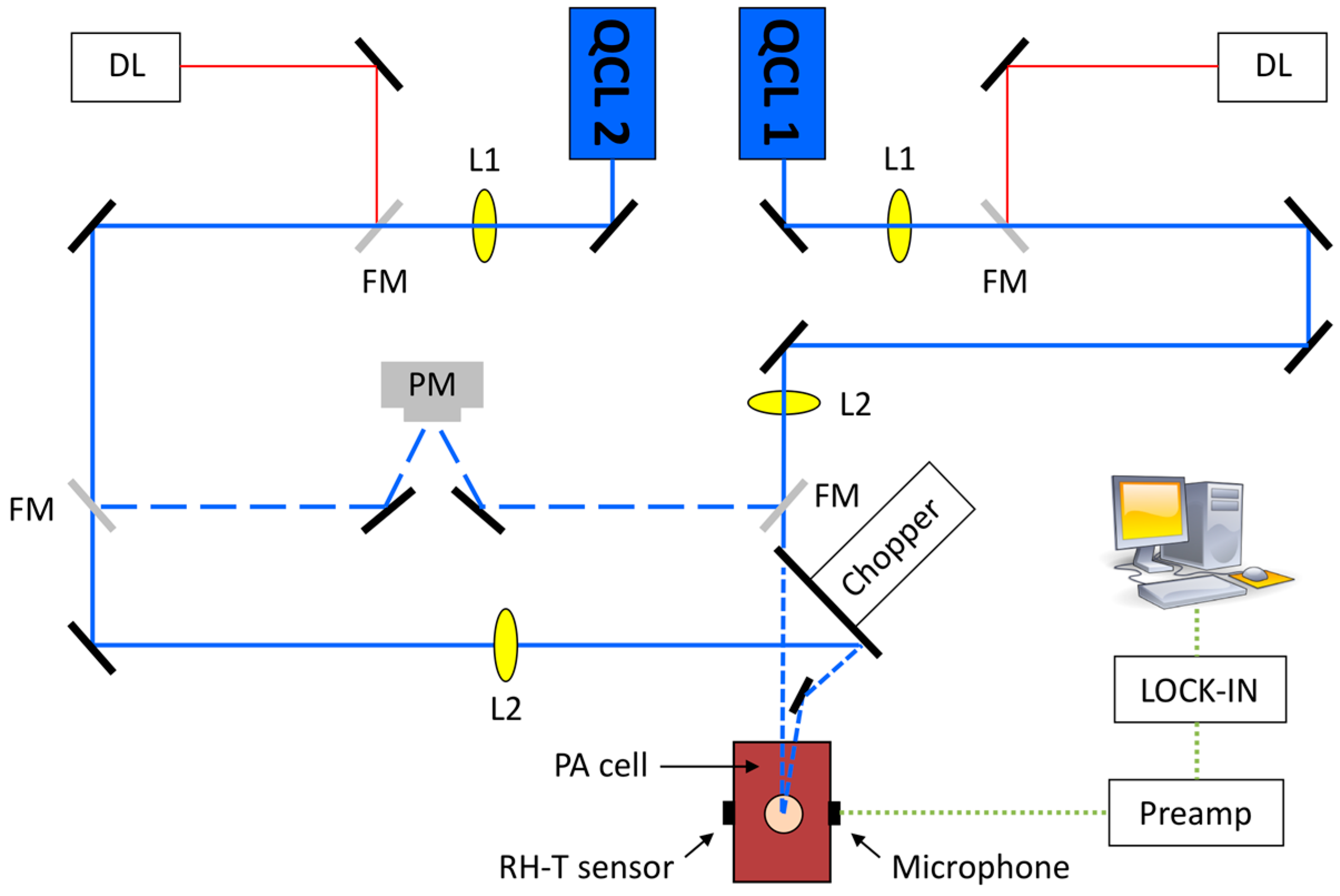
3.2. Setup with Two QCLs at Preselected Fixed Wavelengths
4. Results and Discussion
4.1. Fiber-Coupled EC-QCL
4.2. Two QCLs at Fixed Wavelengths
4.2.1. Glucose Measurement in Aqueous Solutions
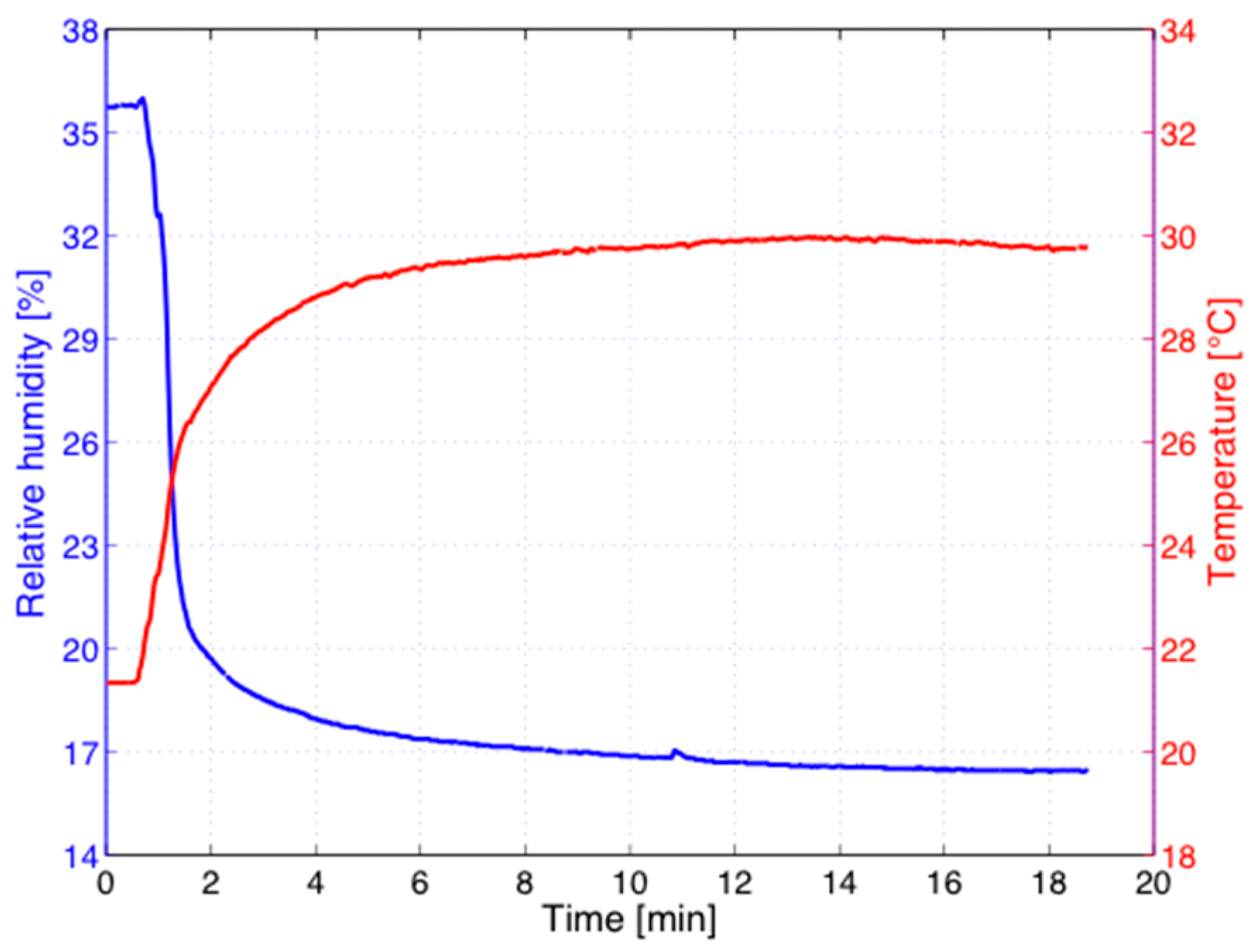
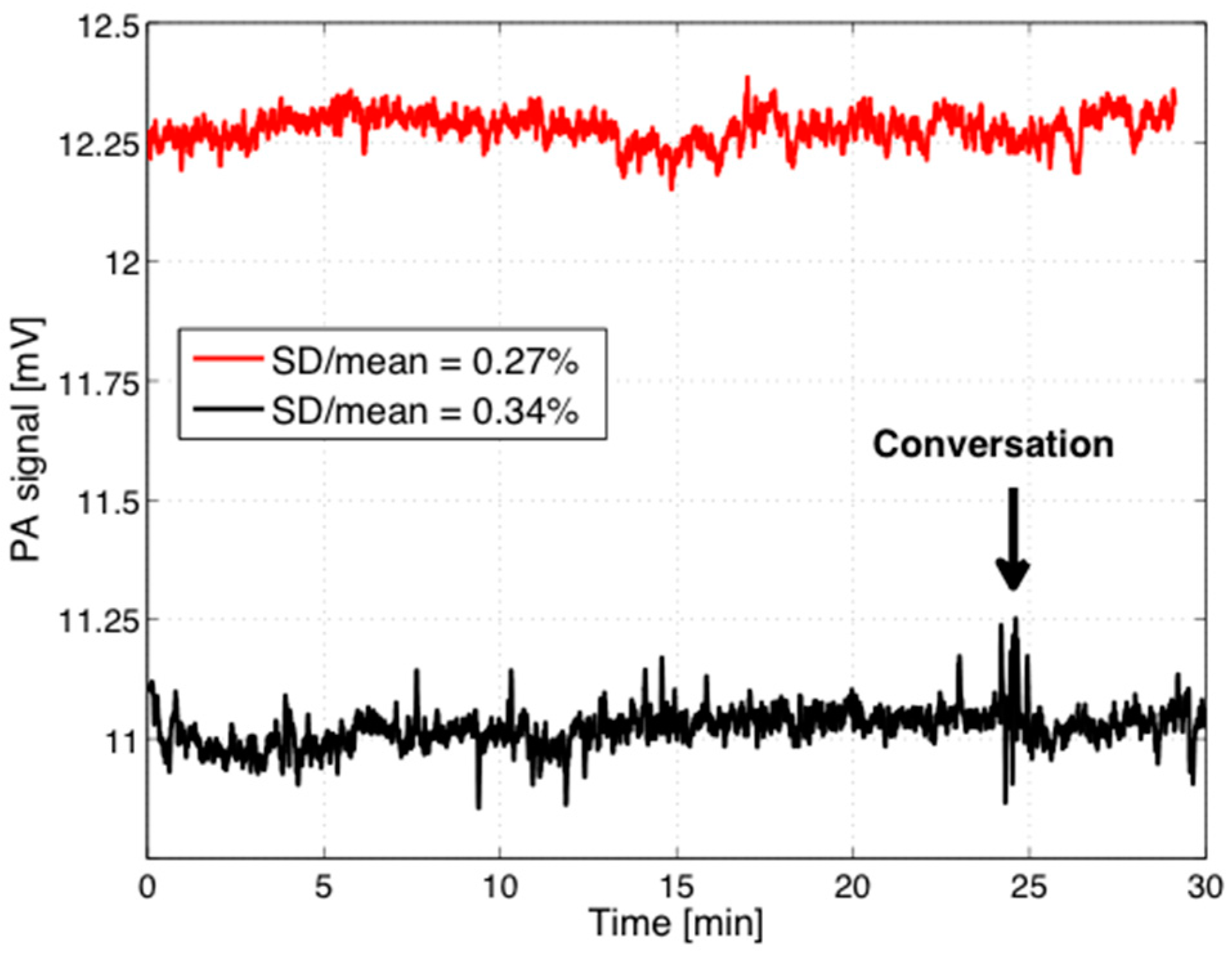
4.2.2. Stability Measurements
4.2.3. Oral Glucose Tolerance Test (OGTT)
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization (WHO). Global Report on Diabetes 2016. Available online: http://www.who.int/diabetes/global-report/en (accessed 31 July 2016).
- Renard, E. Monitoring glycemic control: The importance of self-monitoring of blood glucose. Am. J. Med. 2005, 118, 12S–19S. [Google Scholar] [CrossRef] [PubMed]
- Kottmann, J.; Rey, J.M.; Luginbühl, J.; Reichmann, E.; Sigrist, M.W. Glucose sensing in human epidermis using mid-infrared photoacoustic detection. Biomed. Opt. Exp. 2012, 3, 667–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazen, K.H.; Arnold, M.A.; Small, G.W. Measurement of glucose in water with first-overtone near-infrared spectra. Appl. Spec. 1998, 52, 1597–1605. [Google Scholar] [CrossRef]
- Olesberg, J.T.; Arnold, M.A.; Mermelstein, C.; Schmitz, J. Tunable laser diode system for noninvasive blood glucose measurements. Appl. Spectrosc. 2005, 59, 1480–1484. [Google Scholar] [CrossRef] [PubMed]
- Burmeister, J.J.; Arnold, M.A. Evaluation of measurement sites for noninvasive blood glucose sensing with near-infrared transmission spectroscopy. Clin. Chem. 1999, 45, 1621–1627. [Google Scholar] [PubMed]
- Liu, J.; Rong, L.; Xu, K. Accuracy of Noninvasive Glucose Sensing Based on Near-Infrared Specroscopy. Appl. Spectrosc. 2015, 69, 1313–1318. [Google Scholar] [CrossRef] [PubMed]
- Von Lilienfeld-Toal, H.; Weidenmüller, M.; Xhelaj, A.; Mäntele, W. A novel approach to non-invasive glucose measurement by mid-infrared spectroscopy: The combination of quantum cascade lasers (QCL) and photoacoustic detection. Vibr. Spectrosc. 2005, 38, 209215. [Google Scholar] [CrossRef]
- Pleitez, M.A.; Lieblein, T.; Bauer, A.; Hertzberg, O.; von Lilienfeld-Toal, H.; Mäntele, W. Windowless ultrasound photoacoustic cell for in vivo mid-IR spectroscopy of human epidermis: Low interference by changes of air pressure, temperature, and humidity caused by skin contact opens the possibility for a non-invasive monitoring of glucose in the interstitial fluid. Rev. Sci. Instrum. 2013, 84, 084901. [Google Scholar] [PubMed]
- Pleitez, M.A.; Lieblein, T.; Bauer, A.; Hertzberg, O.; von Lilienfeld-Toal, H.; Mäntele, W. In Vivo Noninvasive Monitoring of Glucose Concentration in Human Epidermis by Mid-Infrared Pulsed Photoacoustic Spectroscopy. Anal. Chem. 2013, 85, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Pleitez, M.A.; Hertzberg, O.; Bauer, A.; Seeger, M.; Lieblein, T.; von Lilienfeld-Toal, H.; Mäntele, W. Photothermal deflectometry enhanced by total internal reflection enables non-invasive glucose monitoring in human epidermis. Analyst 2015, 140, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Mandelis, A.; Matvienko, A.; Sivagurunathan, K.; Zinman, B. Wavelength-modulated differential laser photothermal radiometry for blood glucose measurements. J. Phys. Conf. Ser. 2010, 214, 012025. [Google Scholar] [CrossRef]
- Guo, X.; Mandelis, A.; Zinman, B. Noninvasive glucose detection in human skin using wavelength modulated differential laser photothermal radiometry. Biomed. Opt. Express 2012, 3, 3012–3021. [Google Scholar] [CrossRef] [PubMed]
- Liakat, S.; Bors, K.A.; Xu, L.; Woods, M.C.; Doyle, J.; Gmachl, C.F. Noninvasive in vivo glucose sensing on human subjects using mid-infrared light. Biomed. Opt. Express 2014, 5, 2397–2404. [Google Scholar] [CrossRef] [PubMed]
- Kino, S.; Omori, S.; Katagiri, T.; Matsuura, Y. Hollow optical-fiber based infrared spectroscopy for measurements of blood glucose level by using multi-reflection prism. Biomed. Opt. Express 2016, 7, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Marbach, R.; Koschinsky, T.; Gries, F.A.; Heise, H.M. Noninvasive blood glucose assay by near-infrared diffuse reflectance spectroscopy of the human inner lip. Appl. Spectrosc. 1993, 47, 875–881. [Google Scholar] [CrossRef]
- Boyne, M.S.; Silver, D.M.; Kaplan, J.; Saudek, C.D. Timing of changes in interstitial and venous blood glucose measured with a continuous subcutaneous glucose sensor. Diabetes 2003, 52, 2790–2794. [Google Scholar] [CrossRef] [PubMed]
- Gebhart, S.; Faupel, M.; Fowler, R.; Kapsner, C.; Lincoln, D.; McGee, V.; Pasqua, J.; Steed, L.; Wangsness, M.; Xu, F.; Vanstory, M. Glucose sensing in transdermal body fluid collected under continuous vacuum pressure via micropores in the stratum corneum. Diabetes Technol. Ther. 2003, 5, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, F.; Meyerhoff, C.; Mennel, F.J.; Mayer, H.; Bischof, F.; Pfeiffer, E.F. Does fall in tissue glucose precede fall in blood glucose? Diabetologia 1996, 39, 609–612. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Fang, J.; Wu, P.; Chen, T.; Tsai, M.; Tsai, Y. Noninvasive glucose monitoring by back diffusion via skin: Chemical and physical enhancements. Biol. Pharm. Bull. 2003, 26, 983–987. [Google Scholar] [CrossRef] [PubMed]
- Vrančić, C.; Fomichova, A.; Gretz, N.; Herrmann, C.; Neudecker, S.; Pucci, A.; Petrich, W. Continuous glucose monitoring by means of mid-infrared transmission laser spectroscopy in vitro. Analyst 2011, 136, 1192–1198. [Google Scholar]
- Rosencwaig, A.; Gersho, A. Theory of photoacoustic effect with solids. J. Appl. Phys. 1976, 47, 64–69. [Google Scholar] [CrossRef]
- Kottmann, J.; Rey, J.M.; Sigrist, M.W. New photoacoustic cell design for studying aqueous solutions and gels. Rev. Sci. Instrum. 2011, 82, 084903. [Google Scholar] [CrossRef] [PubMed]
- Tam, A.C. Photoacoustics: Spectroscopy and other applications. In Ultrasensitive Laser Spectroscopy; Kliger, D.S., Ed.; Academic Press Inc.: New York, NY, USA, 1983; pp. 1–108. [Google Scholar]
- Zhao, Z. Pulsed Photoacoustic Techniques and Glucose Determination in Human Blood and Tissue. Ph.D. Thesis, University of Oulu, Oulu, Finland, 2002. [Google Scholar]
- Downing, H.D.; Williams, D. Optical constants of water in the infrared. J. Geophys. Res. 1975, 80, 1656–1661. [Google Scholar] [CrossRef]
- Duck, F.A. Physical Properties of Tissue: A Comprehensive Reference Book; Academic Press: London, UK, 1990. [Google Scholar]
- Kottmann, J.; Grob, U.; Rey, J.M.; Sigrist, M.W. Mid-Infrared Fiber-Coupled Photoacoustic Sensor for Biomedical Applications. Sensors 2013, 13, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Kottmann, J.; Rey, J.M.; Sigrist, M.W. New photoacoustic cell with diamond window cover for mid-infrared investigations on biological sample. Proc. SPIE 2012, 8223, 82231A. [Google Scholar]
- DKE, D.V. Optische Strahlensicherheit und Laser 1 und 2; DIN Deutsches Institut für Normung e. V.: Berlin, Germany, 2007. [Google Scholar]
- Günzler, H.; Gremlich, H.U. IR-Spektroskopie: Eine Einführung; Wiley-VCH: Weinheim, Germany, 2003. [Google Scholar]
- Pleitez, M.; von Lilienfeld-Toal, H.; Mäntele, W. Infrared spectrosocpic analysis of human interstitial fluid in vitro and in vivo using FR-IR spectroscopy and pulsed quantum cascade lasers (QCL): Establishing a new approach to noninasive glucose measurement. Spectrochim Acta Part A 2012, 85, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Garidel, P. Mid-FTIR-Microspectroscopy of stratum corneum single cells and stratum corneum tissue. Phys. Chem. Chem. Phys. 2002, 4, 5671–5677. [Google Scholar] [CrossRef]
- Lucassen, G.W.; van Veen, G.N.A.; Jansen, J.A.J. Band analysis of hydrated human skin sratum corneum attenuated total reflectance fourier transform infrared spectra in vivo. J. Biomed. Opt. 1998, 3, 267–280. [Google Scholar] [CrossRef] [PubMed]
- Kottmann, J. Non-Invasive Photoacoustic Glucose Monitoring towards in Vivo Diagnostics. Ph.D. Thesis, ETH Zurich, Zurich, Switzerland, 2012. [Google Scholar]
- Deutsches Institut für Normung (DIN). EN ISO 15197: Testsysteme für die in-Vitro-Diagnostik—Anforderungen an Blutzuckermesssysteme zur Eigenanwendung Beim Diabetes Mellitus. Available online: https://www.beuth.de/de/norm/din-en-iso-15197/193588607 (accessed on 10 October 2016).











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medium | Density ρ (kg/m3) | Thermal Conductivity k (W/m·K) | Specific Heat C (J/kg·K) | αmax between 1000 and 1100 cm−1 (cm−1) |
|---|---|---|---|---|
| Water | 997 | 0.615 | 4181 | 651 |
| Epidermis | 1110–1190 | 0.293–0.393 | 3700 | ~ 0.6 · αwater |
| Stratum corneum | 1500 | 0.293–0.393 | 3700 | ~ 0.1 · αwater |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kottmann, J.; Rey, J.M.; Sigrist, M.W. Mid-Infrared Photoacoustic Detection of Glucose in Human Skin: Towards Non-Invasive Diagnostics. Sensors 2016, 16, 1663. https://doi.org/10.3390/s16101663
Kottmann J, Rey JM, Sigrist MW. Mid-Infrared Photoacoustic Detection of Glucose in Human Skin: Towards Non-Invasive Diagnostics. Sensors. 2016; 16(10):1663. https://doi.org/10.3390/s16101663
Chicago/Turabian StyleKottmann, Jonas, Julien M. Rey, and Markus W. Sigrist. 2016. "Mid-Infrared Photoacoustic Detection of Glucose in Human Skin: Towards Non-Invasive Diagnostics" Sensors 16, no. 10: 1663. https://doi.org/10.3390/s16101663
APA StyleKottmann, J., Rey, J. M., & Sigrist, M. W. (2016). Mid-Infrared Photoacoustic Detection of Glucose in Human Skin: Towards Non-Invasive Diagnostics. Sensors, 16(10), 1663. https://doi.org/10.3390/s16101663