
Sleep Monitoring Based on a Tri-Axial Accelerometer and a Pressure Sensor




Abstract
:1. Introduction
2. Sleep Quality Monitoring System
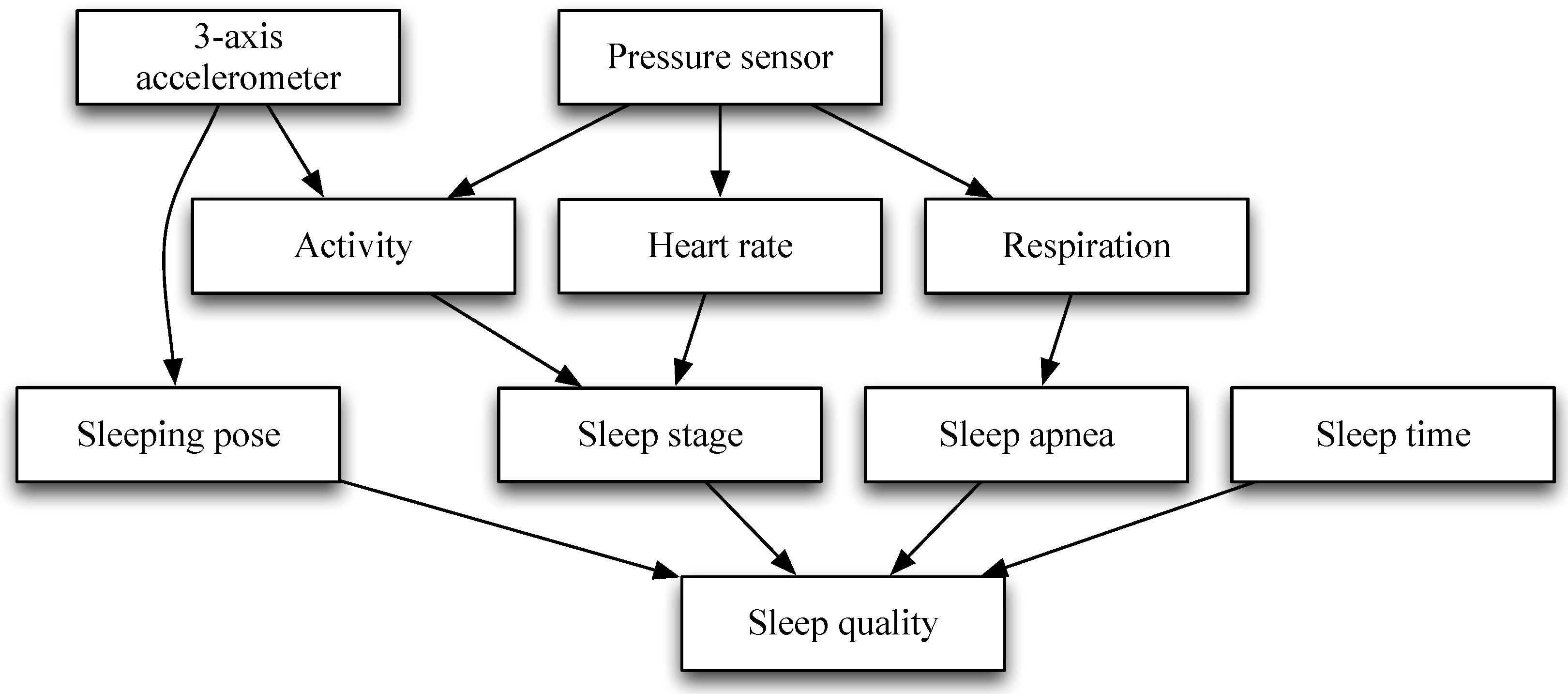
2.1. System Architecture
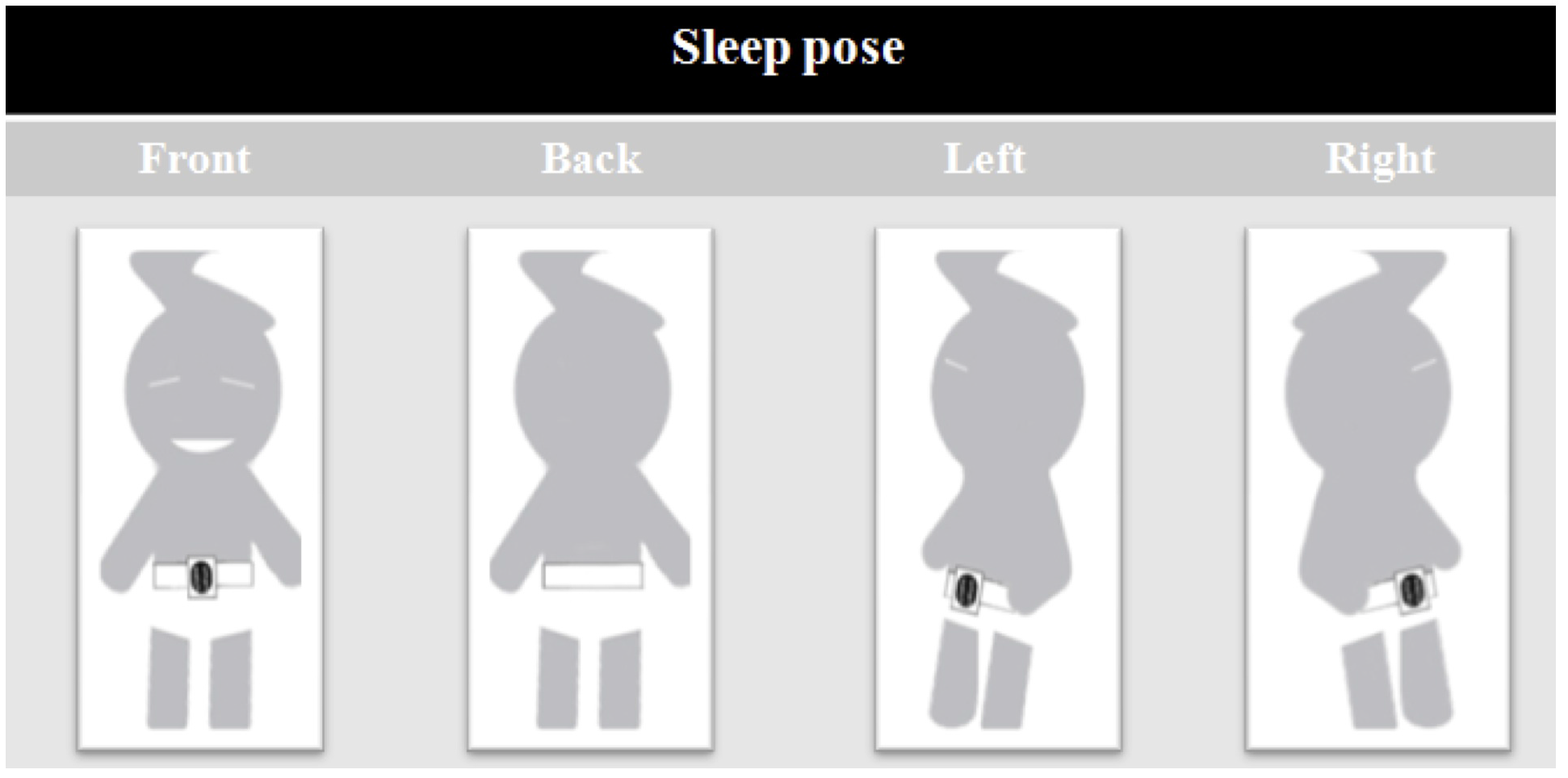
2.2. Feature Extraction and Data Analysis
3. Experimental Results
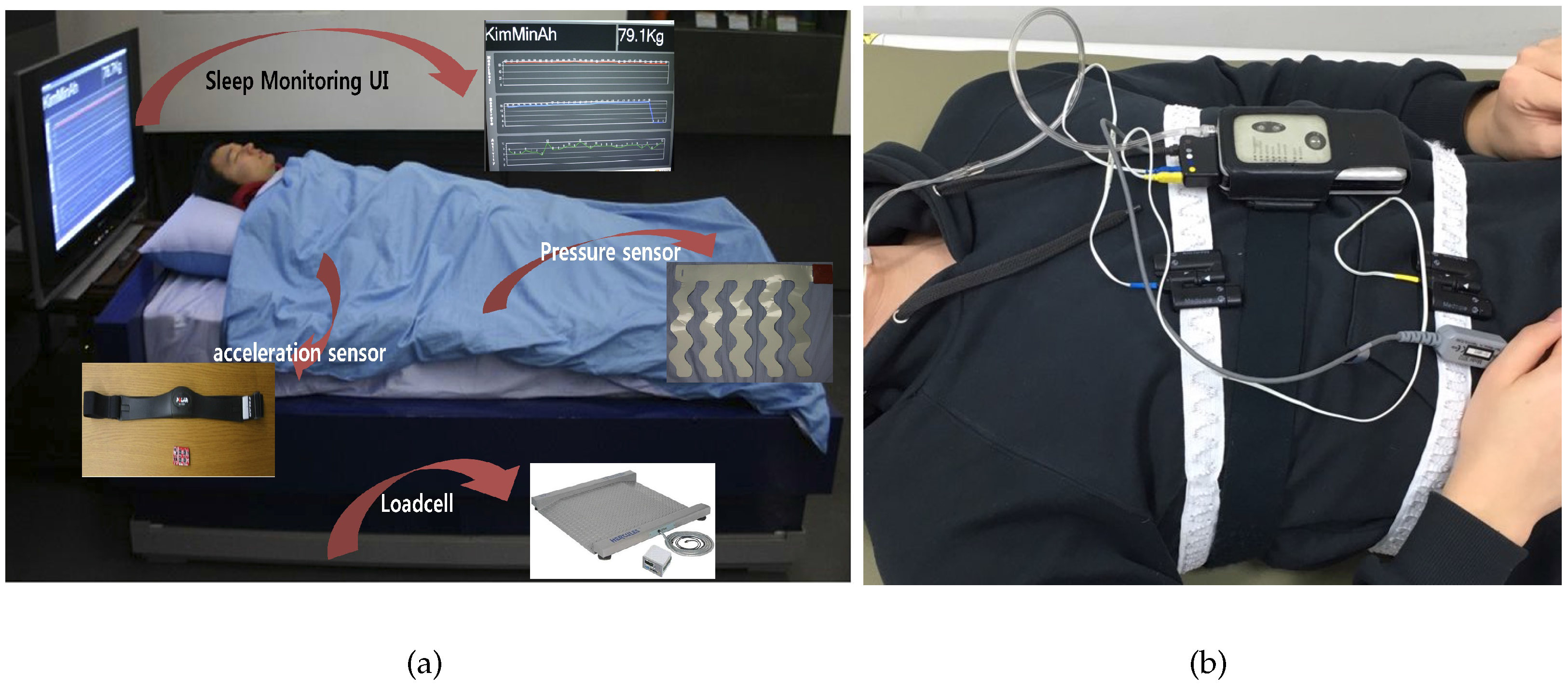
3.1. Experimental Environments
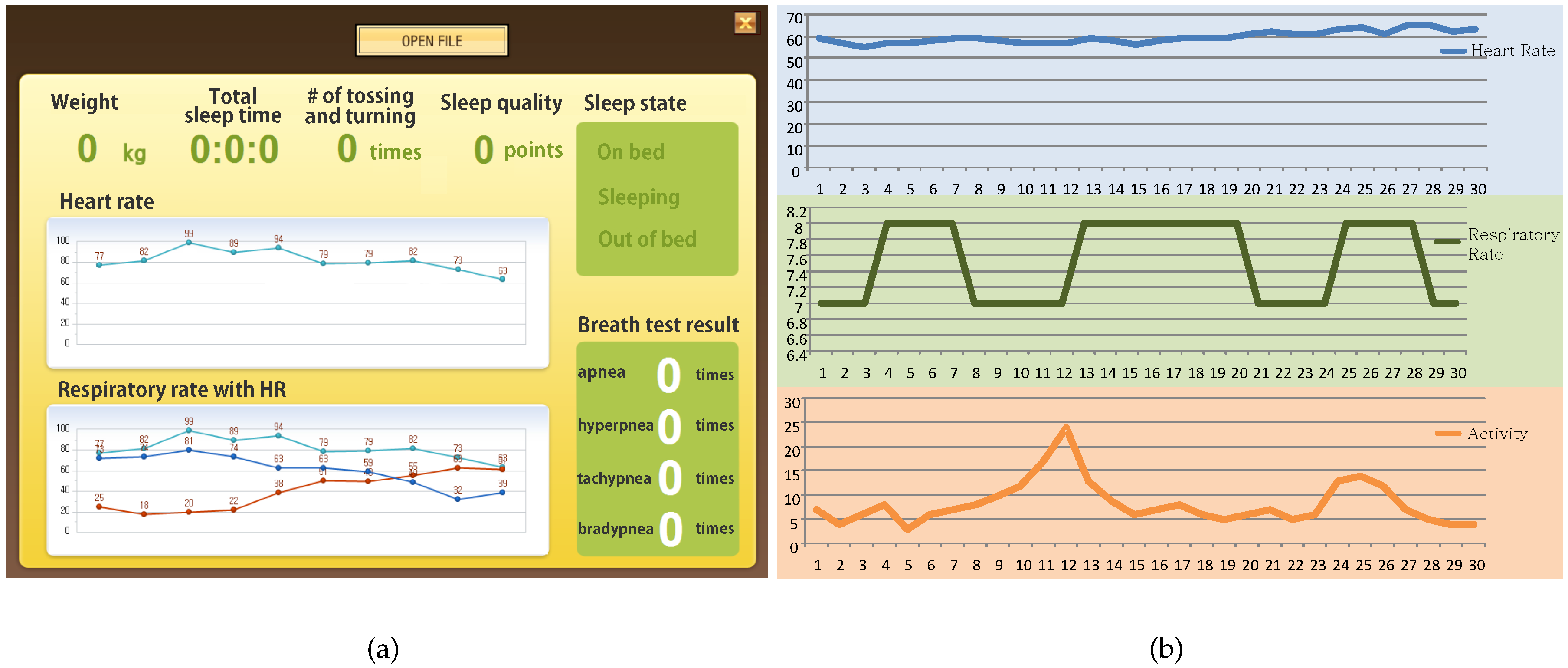
3.2. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Sadeh, A.; Sharkey, K.M.; Carskadon, M.A. Activity-based sleep—Wake identification: An empirical test of methodological issues. Sleep 1994, 17, 201–207. [Google Scholar] [PubMed]
- Salmi, T.; Leinonen, L. Automatic analysis of sleep records with static charge sensitive bed. Electroencephalogr. Clin. Neurophysiol. 1986, 64, 84–87. [Google Scholar] [CrossRef]
- Adami, A.; Hayes, T.; Pavel, M. Unobtrusive monitoring of sleep patterns. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Cancun, Mexico, 17–21 September 2003; Volume 2, pp. 1360–1363.
- Huang, R.S.; Kuo, C.J.; Tsai, L.L.; Chen, O.T. EEG pattern recognition-arousal states detection and classification. In Proceedings of the IEEE International Conference on Neural Networks, Washington, DC, USA, 3–6 June 1996; Volume 2, pp. 641–646.
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Lu, L.; Tamura, T.; Togawa, T. Detection of body movements during sleep by monitoring of bed temperature. Physiol. Meas. 1999, 20, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Rechtschaffen, A.; Kales, A. A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages for Human Subjects; University of California at Los Angeles, Brain Research Institute: Los Angeles, CA, USA, 1968; pp. 1–52. [Google Scholar]
- Mendez, M.O.; Matteucci, M.; Castronovo, V.; Ferini-Strambi, L.; Cerutti, S.; Bianchi, A. Sleep staging from heart rate variability: Time-varying spectral features and hidden Markov models. Int. J. Biomed. Eng. Technol. 2010, 3, 246–263. [Google Scholar] [CrossRef]
- Hoddes, E.; Zarcone, V.; Smythe, H.; Phillips, R.; Dement, W. Quantification of sleepiness: A new approach. Psychophysiology 1973, 10, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Armon, C.; Roy, A.; Nowack, W. Polysomnography: Overview and Clinical Application. Available online: http://emedicine.medscape.com/article/1188764-overview (accessed on 19 May 2016).
- Shephard, J.W. Atlas of Sleep Medicine; Futura Publications Ltd.: London, UK, 1991. [Google Scholar]
- Kupfer, D.J.; Detre, T.P.; Foster, G.; Tucker, G.J.; Delgado, J. The application of Delgado’s telemetric mobility recorder for human studies. Behav. Biol. 1972, 7, 585–590. [Google Scholar] [CrossRef]
- Sadeh, A.; Hauri, P.J.; Kripke, D.F.; Lavie, P. The role of actigraphy in the evaluation of sleep disorders. Sleep 1995, 18, 288–302. [Google Scholar] [PubMed]
- Camm, A.J.; Malik, M.; Bigger, J.; Breithardt, G.; Cerutti, S.; Cohen, R.; Coumel, P.; Fallen, E.; Kennedy, H.; Kleiger, R.; et al. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [Google Scholar]
- Mack, D.; Kell, S.; Alwan, M.; Turner, B.; Felder, R. Non-invasive analysis of physiological signals (naps): A vibration sensor that passively detects heart and respiration rates as part of a sensor suite for medical monitoring. In Proceedings of the 2003 Summer Bioengineering Conference, Key Biscayne, FL, USA, 25–29 June 2003.
- Aittokallio, T.; Saaresranta, T.; Polo-Kantola, P.; Nevalainen, O.; Polo, O. Analysis of inspiratory flow shapes in patients with partial upper-airway obstruction during sleep. Chest 2001, 119, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Chen, B.; Zhou, J.; Lv, Z. A low-power and portable biomedical device for respiratory monitoring with a stable power source. Sensors 2015, 15, 19618–19632. [Google Scholar] [CrossRef] [PubMed]
- Pereira, C.B.; Yu, X.; Czaplik, M.; Rossaint, R.; Blazek, V.; Leonhardt, S. Remote monitoring of breathing dynamics using infrared thermography. Biomed. Opt. Express 2015, 6, 4378–4394. [Google Scholar] [CrossRef] [PubMed]
- Schena, E.; Massaroni, C.; Saccomandi, P.; Cecchini, S. Flow measurement in mechanical ventilation: A review. Med. Eng. Phys. 2015, 37, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Cikajlo, I.; Šprager, S.; Erjavec, T.; Zazula, D. Cardiac arrhythmia alarm from optical interferometric signals during resting or sleeping for early intervention. Biocybern. Biomed. Eng. 2016, 36, 267–275. [Google Scholar] [CrossRef]
- Dziuda, Ł.; Krej, M.; Skibniewski, F.W. Fiber bragg grating strain sensor incorporated to monitor patient vital signs during MRI. IEEE Sens. J. 2013, 13, 4986–4991. [Google Scholar] [CrossRef]
- Dziuda, Ł. Fiber-optic sensors for monitoring patient physiological parameters: A review of applicable technologies and relevance to use during magnetic resonance imaging procedures. J. Biomed. Opt. 2015, 20, 010901. [Google Scholar] [CrossRef] [PubMed]
- Delaney, J.; Leong, K.S.; Watkins, A.; Brodie, D. The short-term effects of myofascial trigger point massage therapy on cardiac autonomic tone in healthy subjects. J. Adv. Nurs. 2002, 37, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Akselrod, S.; Gordon, D.; Ubel, F.A.; Shannon, D.C.; Berger, A.; Cohen, R.J. Power spectrum analysis of heart rate fluctuation: A quantitative probe of beat-to-beat cardiovascular control. Science 1981, 213, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Pomeranz, B.; Macaulay, R.; Caudill, M.A.; Kutz, I.; Adam, D.; Gordon, D.; Kilborn, K.M.; Barger, A.C.; Shannon, D.C.; Cohen, R.J.; et al. Assessment of autonomic function in humans by heart rate spectral analysis. Am. J. Physiol. Heart Circ. Physiol. 1985, 248, H151–H153. [Google Scholar]
- Kortelainen, J.M.; Mendez, M.O.; Bianchi, A.M.; Matteucci, M.; Cerutti, S. Sleep staging based on signals acquired through bed sensor. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 776–785. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Ouchi, K.; Kameyama, K.I.; Takahashi, M. Development of a sleep monitoring system with wearable vital sensor for home use. In BIODEVICES; Citeseer: Porto, Portugal, 2009; pp. 326–331. [Google Scholar]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sensor | Specifications | |
|---|---|---|
| three-axis accelerometer |  | Size: 5 cm, weight: 500 g, consumption current: 0.6 mA, resolution: 60 Hz, MSP430 micro controller for a micro controller (MCU): 16 bit reduced instruction set computer (RISC) |
| pressure |  | Size: 40 cm × 40 cm, weight: 300 g, sensor type: film, operating temp: from −40 C to +50 C, sensitivity: 25–250 pc/n, operating force range: >100 N/cm |
| Subject | Total Sleep Time (Hour) | The Number of Sleep Apnea (Ours) | The Number of Sleep Apnea (PSG) | The Number of Sleep State Change (Ours) | The Number of Sleep State Change (PSG) | Sleep Quality | Dominant Sleeping Pose |
|---|---|---|---|---|---|---|---|
| A | 7.1 | 16.3 | 16.6 | 5.6 | 5.8 | 75.77 | Right |
| B | 6.8 | 12.7 | 12.2 | 4.8 | 4.4 | 81.54 | Front |
| C | 7.6 | 13.6 | 13.2 | 5.2 | 5.6 | 77.57 | Right |
| D | 5.1 | 0 | 0 | 4 | 4 | 87.44 | Right |
| E | 10 | 0 | 0 | 3 | 3 | 120.3 | Front |
| F | 7 | 0 | 0 | 16 | 16 | 74.17 | Back |
| G | 7 | 5 | 5.2 | 6 | 6 | 77.66 | Right |
| H | 5.6 | 0 | 0 | 2 | 2 | 86.67 | Front |
| I | 7 | 2 | 2.2 | 3 | 3 | 104.75 | Front |
| J | 7 | 16 | 16.2 | 3 | 3 | 85.81 | Front |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, Y.; Kim, Y.; Lee, J. Sleep Monitoring Based on a Tri-Axial Accelerometer and a Pressure Sensor. Sensors 2016, 16, 750. https://doi.org/10.3390/s16050750
Nam Y, Kim Y, Lee J. Sleep Monitoring Based on a Tri-Axial Accelerometer and a Pressure Sensor. Sensors. 2016; 16(5):750. https://doi.org/10.3390/s16050750
Chicago/Turabian StyleNam, Yunyoung, Yeesock Kim, and Jinseok Lee. 2016. "Sleep Monitoring Based on a Tri-Axial Accelerometer and a Pressure Sensor" Sensors 16, no. 5: 750. https://doi.org/10.3390/s16050750
APA StyleNam, Y., Kim, Y., & Lee, J. (2016). Sleep Monitoring Based on a Tri-Axial Accelerometer and a Pressure Sensor. Sensors, 16(5), 750. https://doi.org/10.3390/s16050750